
Abstract
Background
Prosthetic mesh reinforcement is standard practice for inguinal hernia repair but can cause considerable pain and stiffness around the groin and affect physical functioning. This has led to various types of mesh being engineered, with a growing interest in a lighter weight mesh. The aim of this prospective study was to compare the outcome after laparoscopic totally extra-peritoneal (TEP) inguinal repair using new lightweight or traditional heavyweight mesh performed in a single specialist centre.
Methods
Between November 2004 and July 2005, 250 patients underwent laparoscopic TEP inguinal repair using either lightweight (Ultrapro®, 30 g/m2) or heavyweight (Prolene®, 100 g/m2) mesh. Follow-up data was obtained using case note review and telephone-based questionnaire. Patients were followed up within the early and late post-operative periods to assess any changes in outcome.
Results
Follow-up information was obtained for 188 (75%) out of 250 patients. There was no difference between lightweight and heavyweight groups in the incidence or severity of pain/discomfort at mean 4 and 15 months follow-up. There was significantly less interference with physical activity at short and long term follow-up in the lightweight group, in particular lifting (9% vs 21% at mean 4 months, Mann–Whitney U, P = 0.024), walking (1% vs 11% at mean 15 months, Mann–Whitney U, P = 0.006) and vigorous activities (7% vs 19% at mean 15 months, Mann–Whitney-U, P = 0.012). There was no significant difference in awareness of mesh or stiffness in the groin.
Conclusions
Laparoscopic TEP inguinal hernia repair with a lightweight mesh improves functional outcome in the short and long term. There was significantly less interference with all aspects of physical activity with the lightweight mesh. Pain in both groups was very mild, highlighting the benefits of laparoscopic surgery.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Inguinal hernia is becoming increasingly common in an ageing population, with a peak incidence in the sixth decade [1]. The lifetime risk of acquiring an inguinal hernia is 27% in men and 3% in women [2]. As such, there are over 80,000 operations performed per year in the United Kingdom for inguinal hernia [2]. Inguinal hernia repair is one of the commonest operations in general surgery, with increasing adoption of the laparoscopic totally extra-peritoneal (TEP) approach by surgeons as recommended by the National Institute for Health and Clinical Excellence (NICE) [3]. The laparoscopic TEP repair is associated with significantly less post-operative pain, faster recovery and return to normal activity, and equivalent recurrence rates to open techniques [4, 5].
Prosthetic reinforcement is routine in the management of inguinal hernia as it significantly reduces the risk of recurrence [4, 5]. In addition to tissue and nerve injury, the mesh may contribute to the problems encountered after surgical mesh repair. The standard polypropylene mesh may be associated with pain, discomfort and ultimately restricts physical activities. This may be due to the generation of a profound inflammatory response that results in scar formation, increased rigidity and stiffness of the abdominal wall, and shrinkage of the biomaterial with time [6, 7]. This can result in considerable morbidity and reduced quality of life.
Reducing the amount of polypropylene should induce less foreign body response and scar formation and is predicted to achieve better results [6, 7]. The introduction of “lightweight” meshes for inguinal hernia repair is promising [8–12]. However, there is little data regarding efficacy with the increasingly popular laparoscopic TEP procedure at long term follow-up. The aim of this study was to compare the outcome after laparoscopic TEP inguinal repair using lightweight or standard heavyweight mesh performed at a single specialist centre.
Patients and methods
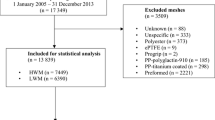
Patients undergoing elective laparoscopic TEP inguinal repair using either lightweight or heavyweight mesh between November 2004 and July 2005 were studied. Patients who had open repairs, non-inguinal hernias or had a mesh not being investigated in this study were excluded. A total of 250 consecutive patients were identified from the prospectively collected Lothian Surgical Audit Database with validation by case note review. Data collected from the database included patient demographic information, operative factors and date of discharge. Single blinded researchers using a telephone-based questionnaire obtained follow-up data. Patients were followed up once during the early post-operative period and again at a later date for long term follow-up. We attempted to follow up all 250 patients at early and late follow-up periods. However, not all patients were contactable or had correct contact details. Patients who could not be reached during the early period but were subsequently contacted later were included in the long-term follow-up.
Laparoscopic TEP repair was performed under general anaesthesia and without fixing the mesh in the pre-peritoneal space. Laparoscopic TEP hernia repair has been performed in Edinburgh since 1992 and our surgical technique has been described [13]. In brief, access to the pre-peritoneal space was gained using a sub umbilical port and two further ports inserted in the lower midline. A pneumo-extro-peritoneum was created with carbon dioxide, and the hernia sac and contents reduced back into the abdominal cavity. A prosthetic mesh was then placed over the myopectineal orifice. The procedure was performed or directly supervised by an experienced consultant, who had the choice of mesh. There was a period of approximately 8 months prior to the study for those using the new mesh to familiarise themselves with the handling of the mesh. The chosen mesh was used consistently, ensuring that no particular selection criteria were applied to the use of one mesh over another for a given case. Predominantly one surgeon was the main user of the heavyweight mesh in this study.
The lightweight mesh used in this study is made up of a monocryl-prolene-composite material that has a large pore, thin filament size construction with residual component weighing approximately 30 g/m2 (Ultrapro®, Ethicon Products, Edinburgh, UK). The heavyweight mesh used was standard polypropylene and weighed approximately 100 g/m2 (Prolene®, Ethicon Products).
The questionnaire included: a pain severity score that ranged from 0 (no pain) to 10 (unbearable pain); quality of life scores based on patients’ pre-operative baseline (walking, lifting, sports, vigorous activities) from the modified Short Form 36 (SF-36) questionnaire [14]; questions enquiring about stiffness, numbness around the groin or down the thigh, awareness of the mesh and overall success of the operation. The questionnaire also asked about satisfaction with the appearances of the scars, whether recovery was faster than expected, and whether the patient would recommend the procedure that they had undergone.
Statistical analysis
All statistical tests were interpreted at the 5% significance level. Differences were considered significant at P < 0.050 (2-sided). Pain severity scores were compared by the t-test. Equal variances were not assumed for t-tests. The Mann–Whitney U test was used to compare ordered categorical data. Proportions were analysed using χ 2 test. No adjustment for multiple testing was made.
Analyses were completed using SPSS (version 10; SPSS, Chicago, IL).
Results
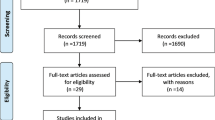
Overall, follow-up information was obtained for 188 (75%) out of 250 patients. From the cohort of 250 patients, 150 patients had early follow-up and 160 patients had long term follow-up (Table 1). Moreover, 122 (49%) out of 250 patients were followed up both during the early and late post-operative periods.
There were no significant differences between the groups in terms of mean follow-up time; early follow-up was at mean 4 months (t-test, P = 0.115) and late follow-up was at mean 15 months (t-test, P = 0.40). There were no differences in patient characteristics between the two mesh groups (Table 1). There were no intra-operative or major post-operative complications. At mean 15 months follow-up, 2 (2%) patients with lightweight mesh and 3 (4%) patients with heavyweight mesh had a recurrence of hernia; although there was no significant difference in the recurrence rates between the two groups in this study.
Pain and discomfort
There was no difference between lightweight and heavyweight groups in the incidence or severity of pain/discomfort at mean 4 months follow-up (combined total 31% vs 35%, Mann–Whitney U, P = 0.661) or at mean 15 months follow-up (combined total 25% vs 26%, Mann–Whitney U, P = 0.592; Table 2). Of note, 19% with lightweight mesh and 20% with heavyweight mesh reported pain at mean 4 months follow-up. At mean 15 months follow-up, only 8% with lightweight mesh and 11% with heavyweight mesh reported pain. However, there was greater use of analgesia within the heavyweight mesh group at long term follow-up, although this did not reach statistical significance (1% vs 8%, χ 2 test, P = 0.063).
Interference with physical activities
Patients with lightweight mesh experienced significantly less interference with physical activity at both short and long term follow-up (Table 3). At mean 4 months follow-up, 9% with lightweight mesh reported problems with lifting/carrying groceries compared to 21% within HW group (Mann–Whitney U, P = 0.024). Moreover, only 3% with lightweight mesh but 12% with heavyweight mesh reported similar problems at mean 15 months (Mann–Whitney U, P = 0.053.
Difficulties with walking (1% LW vs 11% HW, Mann–Whitney U, P = 0.006) and sporting activities (2% LW vs 14% HW, Mann–Whitney U, P = 0.005) were significantly less in the lightweight group at mean 15 months follow-up (Fig. 1). These significant differences were not evident at early follow-up (Table 3), perhaps because early post-operative factors played a larger role in this period. Nevertheless, significantly fewer patients in the lightweight mesh group reported vigorous activities to be limiting both in the short term (20% vs 33%, Mann–Whitney-U, P = 0.038) and at long-term follow-up (7% vs 19%, Mann–Whitney-U, P = 0.012).

Problems with physical activity after repair at mean 15 months follow-up were significantly reduced with lightweight mesh
Numbness, prosthetic mesh and success of operation
Fewer patients with the lightweight mesh reported numbness around the groin or down the thigh after surgery compared to the heavyweight mesh group at mean 4 months follow-up, but this did not represent a significant difference (5% LW vs 13% HW, Mann–Whitney U, P = 0.113). Interestingly, the severity of numbness was less in the lightweight group at early follow-up (Mann–Whitney U, P = 0.088). As expected, numbness was reduced at later follow-up for both groups (2% LW vs 4% HW, Mann–Whitney U, P = 0.487).
There was no significant difference between the groups in awareness of mesh (16% LW vs 14% HW, χ 2, P = 0.947) or stiffness in the groin (4% LW vs 6% HW, χ 2, P = 1.00) at mean 15 months follow-up. Overall, 48 (54%) patients with lightweight mesh and 40 (56%) patients with heavyweight mesh reported a faster recovery than they had expected. Moreover, 83 (93%) patients with lightweight mesh and 61 (86%) patients with heavyweight mesh would recommend the laparoscopic procedure to others, thus highlighting patient satisfaction.
Discussion
Quality of life after hernia repair may be a more important outcome than recurrence [10, 15] as it influences patients’ ability to resume daily life activity and work. Whilst the focus of hernia surgery has been recurrence rates in the past, the tremendous advances made in laparoscopic and open hernia repair has diminished these rates. This has also allowed alternative options to repair such recurrent hernias with relative ease such that we should now be directing our attention towards maintaining quality of life. Our findings determine that laparoscopic TEP inguinal hernia repair with lightweight mesh allow better physical functioning at long term follow-up when compared with traditional heavyweight mesh. There was significantly less interference with all aspects of physical activity with the lightweight mesh.
Our pilot study suggested a faster recovery with the lightweight mesh [8]. This is in accordance with a recent randomised controlled trial, which reported a significantly shorter convalescence period after open repair with a titanium-coated lightweight mesh than standard polypropylene mesh [16]. Another small trial using laparoscopic TEP repair show significantly better pain scores, patient comfort and sexual function with lightweight mesh at early follow-up [17]. An earlier study in laparoscopic TEP repair for recurrent hernias found comparable results and significantly better general health scores with lightweight mesh at 2 months follow-up [18]. At short term follow-up, we show significantly less interference with lifting and vigorous activities in the lightweight group. This significant early difference may suggest a faster recovery with lightweight mesh owing to less mesh-induced inflammation. However, the other activities did not reach statistical significance at mean 4 months follow-up but did later on, perhaps because other early post-operative factors contribute to physical wellbeing and quality of life.
Whilst our present study suggests that the advantages of lightweight mesh persist in the long term, the incidence and severity of pain and the impact this has on physical activity is decreased with time in both lightweight and heavyweight groups. This is to be expected with lengthening time following surgery, with an approximately 50% reduction in pain experienced in both groups in this study. The fact that fewer patients with lightweight mesh required analgesia at mean 15 months further lends to the benefits of using a lightweight mesh. The severity of pain in both groups was very mild, highlighting the success of laparoscopic surgery. However, our data continues to reflect a cohort of patients who continue to suffer from chronic groin pain regardless of mesh type, and this is a well-recognised problem in modern hernia surgery [19–21].
One recent randomised study using laparoscopic trans-abdominal pre-peritoneal repair reports no advantage of lightweight mesh in terms of pain or physical function beyond 3 months [21]. They do state a significant slower convalescence and more post-operative complications with the standard heavyweight polypropylene mesh in the short term [21].
A previous randomised controlled trial reported less groin pain after open Lichtenstein repair with lightweight mesh compared to heavyweight mesh at 12 months follow-up [10]. There were no such differences in pain at 1 and 3 months follow-up, suggesting that the benefits of lightweight mesh may not necessarily be immediate but more important in the long term. Yet, another study found no differences in pain scores at 12 months follow-up despite a shorter convalescence with lightweight mesh, but describe a tendency for less pain in the lightweight group after open repair [16]. A 3-year follow-up study reports less pain and discomfort with lightweight mesh after Lichtenstein repair [22].
A previous study comparing lightweight and heavyweight mesh following open inguinal hernia repair showed less pain on exercise and “feeling of a foreign body” in the lightweight group at 6 months follow-up [9]. However, rates of patients reporting an awareness of mesh in both groups were considerably higher in their trial compared to our results. Moreover, problems with numbness following repair are minimal in laparoscopic surgery when compared to studies of open repair [23]. It has been postulated that the lightweight mesh causes less fibroblastic ingrowth and shrinkage of mesh and thus less entrapment of nerves and stiffness. This could imply that a combination of laparoscopic TEP approach with minimal tissue trauma and lightweight mesh is required to minimise awareness of foreign material and stiffness.
The most commonly used polypropylene mesh is associated with a strong foreign body reaction and is a major contributor to pain. The lightweight Ultrapro® mesh used in this study is thought to minimise the inflammatory response and scar formation compared to the conventional heavyweight mesh [6, 7]. This should result in less restriction of abdominal wall movement and increased elasticity of the abdominal wall without undermining its ability to resist mechanical strain. This appears to be consistent with the results of this study with lightweight mesh translating to better functional outcomes, particularly in an ageing population. One study comparing type of mesh and type of repair (open vs laparoscopic) found that a lightweight mesh causes significantly less pain independent of the technique and thus the prosthesis is the major determinant [24].
Fixation of the prosthetic mesh can contribute to pain and discomfort experienced by some patients months or years after repair. Fixation of the mesh in laparoscopic TEP hernia repair is currently not performed in our unit [25]. Placement of staples or sutures may induce specific complications such as nerve entrapment and haematoma. There have been concerns with early recurrence with lightweight mesh and some surgeons are actively using fixation or placing extra sutures, especially for larger hernias. A combination of the laparoscopic TEP approach and use of lightweight mesh without fixation may have advantages over a heavyweight mesh in improving quality of life outcomes after groin hernia repair.
In conclusion, laparoscopic TEP inguinal hernia repair with a lightweight mesh yields significantly better functional results than a heavyweight mesh in the long term.
References
Hair A, Duffy K, McLean J et al (2000) Groin hernia repair in Scotland. Br J Surg 87:1722–1726
Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362(9395):1561–1571
National Institute for Clinical Excellence (2004) Guidance on the use of laparoscopic surgery for inguinal hernia. Technological appraisal guidance no. 83. NICE, London
MRC Laparoscopic Groin Hernia Trial Group (1999) Laparoscopic versus open repair of groin hernia: a randomised comparison. Lancet 354:185–190
EU Hernia Trialist Collaboration (2002) Laparoscopic versus open groin hernia repair: meta-analysis of randomised trials based on individual patient data. Hernia 6:2–10
Cobb WS, Kercher KW, Heniford BT (2005) The argument for lightweight polypropylene mesh in hernia repair. Surg Innov 12:63–69
Junge K, Rosch R, Krones CJ, Klinge U, Mertens PR, Lynen P, Schumpelick V, Klosterhalfen B (2005) Influence of polyglecaprone 25 (Monocryl) supplementation on the biocompatibility of a polypropylene mesh for hernia repair. Hernia 9:212–217
Khan LR, Kumar S, Nixon SJ (2006) Early results for new lightweight mesh in laparoscopic totally extra-peritoneal inguinal hernia repair. Hernia 10:303–308
Post S, Weiss B, Willer M, Neufang T, Lorenz D (2004) Randomized clinical trial of lightweight composite mesh for lichtenstein inguinal hernia repair. Br J Surg 91:44–48
O’Dwyer PJ, Kingsnorth AN, Molloy RG, Small PK, Lammers B, Horeyseck G (2005) Randomized clinical trial assessing impact of a lightweight or heavyweight mesh on chronic pain after inguinal hernia repair. Br J Surg 92:166–170
Champault G, Barrat C (2005) Inguinal hernia repair with beta glucan-coated mesh: results at two-year follow up. Hernia 9:125–130
Bringman S, Wollert S, Osterberg J, Heikkinen T (2005) Early results of a randomized multicenter trial comparing Prolene and VyproII mesh in bilateral endoscopic extraperitoneal hernioplast (TEP). Surg Endosc 19:536–540
Nixon SJ, Kumar S (2005) The totally extraperitoneal approach (TEP) to inguinal hernia repair. Surgeon 3:281–7, 305
Ware JE Jr, Sherbourne CD (1992) The MOS 36-item-short-form health survey (SF36). 1. Conceptual framework and item selection. Med Care 30:473–483
Kurzer M, Kark AE, Hussain T (2008) Hernia repair: outcomes other than recurrence should be analysed. BMJ 336:1033
Koch A, Bringman S, Myrelid P, Smeds S, Kald A (2008) Randomized clinical trial of groin hernia repair with titanium-coated lightweight mesh compared with standard polypropylene mesh. Br J Surg 95:1226–1231
Agarwal BB, Agarwal KA, Mahajan KC (2009) Prospective double-blind randomized controlled study comparing heavy- and lightweight polypropylene mesh in totally extraperitoneal repair of inguinal hernia: early results. Surg Endosc 23: 242–247
Heikkinen T, Wollert S, Osterberg J, Smedberg S, Bringman S (2006) Early results of a randomised trial comparing Prolene and VyproII-mesh in endoscopic extraperitoneal inguinal hernia repair (TEP) of recurrent unilateral hernias. Hernia 10:34–40
Kumar S, Wilson RG, Nixon SJ, Macintyre IMC (2002) Chronic pain after laparoscopic and open mesh repair of groin hernia. Br J Surg 89:1476–1479
Courtney CA, Duffy K, Serpell MG, O’Dwyer PJ (2002) Outcome of patients with severe chronic pain following repair of groin hernia. Br J Surg 89:1310–1314
Langenbach MR, Schmidt J, Ubrig B, Zirngibl H (2008) Sixty-month follow-up after endoscopic inguinal hernia repair with three types of mesh: a prospective randomized trial. Surg Endosc 22:1790–1797
Bringman S, Wollert S, Osterberg J, Smedberg S, Granlund H, Heikkinen TJ (2006) Three-year results of a randomized clinical trial of lightweight or standard polypropylene mesh in lichtenstein repair of primary inguinal hernia. Br J Surg 93:1056–1059
Grant AM, Scott NW (2004) MRC laparoscopic groin hernia trial group. Five-year follow-up of a randomized trial to assess pain and numbness after laparoscopic or open repair of groin hernia. Br J Surg 91:1570–1574
Champault G, Bernard C, Rizk N, Polliand C (2007) Inguinal hernia repair: the choice of prosthesis outweighs that of technique. Hernia 11:125–128
Beattie GC, Kumar S, Nixon SJ (2000) Laparoscopic total extraperitoneal hernia repair: mesh fixation is unnecessary. J Laparoendosc Adv Surg Tech A 10:71–73
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khan, L.R., Liong, S., de Beaux, A.C. et al. Lightweight mesh improves functional outcome in laparoscopic totally extra-peritoneal inguinal hernia repair. Hernia 14, 39–45 (2010). https://doi.org/10.1007/s10029-009-0558-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-009-0558-2