
Abstract
Hoarding, common in pediatric obsessive–compulsive disorder (OCD), has specific clinical correlates and is associated with poor prognosis. However, there are few studies of hoarding in pediatric OCD. This study estimates the occurrence of hoarding symptoms in a sample of children and adolescents with OCD, investigating possible differences in demographic and clinical variables between pediatric OCD with and without hoarding symptoms. Furthermore, the study investigates whether hoarding symptoms predict poorer treatment outcomes after cognitive behavioral therapy (CBT). The study sample comprised 269 children and adolescents with OCD, aged 7–17 years, from Denmark, Sweden, and Norway, who were all included in the Nordic long-term obsessive–compulsive disorder Treatment Study. All had an OCD diagnosis according to the DSM-IV and were treated with 14 weekly sessions of manualized, exposure-based CBT. Hoarding symptoms and OCD severity were assessed with the Children’s Yale–Brown Obsessive–Compulsive Scale and group differences in treatment outcome were analyzed using linear mixed-effect modelling. Seventy-two patients (26.8%) had one or more symptoms of hoarding. Comorbid tic disorders (p = 0.005) and indecision (p = 0.024) were more prevalent among those with hoarding symptoms than those without hoarding symptoms. In addition, youth with hoarding symptoms had a different OCD symptom profile. Having symptoms of hoarding did not affect CBT outcome (p = 0.933). Results from the study suggest that CBT is equally effective for those with and without hoarding-related OCD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obsessive–compulsive disorder (OCD) is a debilitating psychiatric disorder with a prevalence rate between 0.25% and 4% [1,2,3,4]. Left untreated, OCD often continues into adulthood, significantly impairing daily functioning and reducing quality of life [5, 6]. Cognitive behavioral therapy (CBT) is recommended as first-line treatment for OCD in children and adolescents [7,8,9,10,11].
The classification of hoarding as a sub-category of OCD was recently revised. In the fifth edition of the DSM [12], hoarding is classified as a disorder in its own right, based on research showing that hoarding can present independently from OCD or any other neurological or psychiatric disorder. According to the DSM-5, the cardinal feature of hoarding disorder is persistent difficulty discarding or parting with possessions, regardless of their actual value. However, when symptoms are attributed, as a direct consequence, to typical obsessions or compulsions, such as avoidance of harm or feelings of incompleteness, hoarding is considered OCD-related and should not be diagnosed as hoarding disorder [12]. The prevalence rate of hoarding disorder in children is not established but has been found to be 2% in an adolescent population [13], and 2–5% in adults [14, 15]. Hoarding disorder usually begins before the age of 20 [16].
Hoarding symptoms are usually mild during childhood and become more severe with age [16, 17] Compared to other types of OCD symptoms, hoarding symptoms are less likely to follow an episodic course and more likely to be constant or worsening [18]. Some previous studies have investigated symptoms of hoarding in children and adolescents with OCD, finding them present in 19–30% of cases [19,20,21]. Hoarding is traditionally considered difficult to treat [22]. Therefore, the study of hoarding in OCD and especially examination of the treatment of hoarding in children and adolescents with OCD are crucial to prevent the symptoms from escalating and becoming severely debilitating [23].
Clinical correlates of OCD-related hoarding
Hoarding symptoms in children and adolescents with OCD have been associated with reduced insight [19, 24]. A recent mega-analysis that also included the sample used in this study, found 11.1% of youth with OCD to have poor or absent insight [25]. Hoarding symptoms have also been associated with indecision [20, 24, 26], and earlier OCD onset [20, 26]. Furthermore, hoarding symptoms in children and adolescents with OCD are associated with more comorbidities compared to children and adolescents with non-hoarding symptoms, such as anxiety [19, 20, 24, 26, 27], Tourette and Tic disorders [20], and symptoms of ADHD [19, 26, 28], although inconsistent. Symptoms of hoarding also correlate with ADHD independent of OCD [28]. Some studies have linked hoarding symptoms to autism spectrum disorders [27, 29], but one study found that patients in an OCD control group without autism symptoms were just as likely to endorse hoarding or repeating and ordering symptoms as were patients with OCD and comorbid autism symptoms [30].
A study consisting of a mixed sample of children and adults with OCD reported that across all ages, patients’ highest Y-BOCS severity score was almost two points higher in the hoarding group compared to those without hoarding symptoms [24]. Another study found that hoarding symptoms in children and adolescents with OCD predicted higher lifetime severity of OCD symptoms [20].
Hoarding symptoms in pediatric and adult OCD have been shown to correlate with OCD symptoms such as symmetry, repeating, counting, and ordering [19, 20, 24, 31]; however, it is unclear whether this correlation is independent of comorbidities, such as tics.
Treatment outcome in OCD-related hoarding
In general, effective treatments for OCD, namely CBT and SSRIs, seem to be less effective in addressing the symptoms of obsessive–compulsive hoarding [32, 33]. However, some modifications to CBT specifically to address hoarding disorder in adults seem promising (which includes graded exposure to non-acquiring behavior and training in sorting, discarding, and cognitive restructuring) [33], but this has not been documented in younger samples. In younger children, hoarding with neither OCD nor another comorbid disorder may not lead parents to seek treatment, possibly because parents can influence a child’s hoarding behavior to some degree and because children have limited means to acquire certain items [34].
A 2014 meta-analysis showed a 50% poorer treatment response rate in OCD patients with hoarding symptoms compared to OCD patients without hoarding symptoms, independent of age and treatment type [22]. However, this meta-analysis included four OCD treatment studies of children and adolescents, all with small sample sizes, and only two of these evaluated behavioral interventions [22], and the remaining two were based on combined intervention [35] and pharmacotherapy [36]. A study that assessed 45 children 9 years after treatment showed that for those with hoarding as the primary symptom, OCD tended to persist into early adulthood [37]. Studies with larger samples are needed to evaluate the effect of hoarding symptoms on treatment outcome in children and adolescents.
The present study aimed: (1) to estimate the occurrence of hoarding symptoms in a sample of children and adolescents with OCD, (2) to investigate possible differences in demographic and clinical variables between those children and adolescents with and without symptoms of hoarding, and (3) to estimate whether the presence of hoarding symptoms affected the treatment outcome of manualized CBT.
We expected hoarding symptoms to occur frequently in children and adolescents with OCD [19,20,21], further expecting that patients with hoarding symptoms would be characterized by reduced insight [19, 24], higher levels of indecision [20, 24, 26], earlier onset [20, 26], more severe OCD symptoms [20, 24], and more OCD symptoms related to symmetry, repeating, counting, and ordering [19, 20, 24, 31]. Regarding comorbidity, we expected patients with OCD and hoarding symptoms to have higher levels of anxiety [19, 20, 24, 26, 27], tics [20], and ADHD symptoms [19, 26, 28]. As earlier research has been inconclusive regarding autism spectrum disorder and hoarding symptoms [27, 29, 30], no hypothesis was generated in that respect. Finally, we expected that patients with OCD and hoarding symptoms would have less favorable treatment outcomes [22].
Methods
Participants
A total of 269 children and adolescents aged 7–17 years, recruited from Denmark, Sweden, and Norway between September 2008 and June 2012, were included in the Nordic long-term obsessive–compulsive disorder treatment study (NordLOTS) [38]. They were eligible for inclusion from a total of 767 children and adolescents that were originally screened for participation where of 491 met the inclusion criteria for assessment [38]. Included patients were referred from community health centers, general practitioners and in many cases by parents contacting the clinics directly. Inclusion criteria were an OCD diagnosis based on DSM-IV criteria as assessed with the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS-PL), a CY-BOCS total severity score ≥ 16, and no treatment with CBT or effective doses of SSRIs (> 50 mg) six months prior to the start of the study. Exclusion criteria were kept to a minimum. However, patients with an autism spectrum disorder (except Pervasive Developmental Disorder, Not Otherwise Specified (PDD-NOS) or suffering from another psychiatric disorder with higher treatment priority than OCD (for example serious depression with suicidality or psychosis) were excluded. Patients with ADHD were allowed if pharmacological treatment for ADHD had been stabilized at least 3 months prior to inclusion. Study rationale [39] and inclusion procedures [38] for the NordLOTS are described in detail elsewhere.
Informed consent was obtained from all participants and their parents, and the trial was approved by the Norwegian, Swedish, and Danish Committees for Medical and Health Research Ethics and the Medical Products Agencies.
Measures
Children’s Yale–Brown obsessive–compulsive scale (CY-BOCS)
The CY-BOCS is a semi-structured interview used in the present study by an independent evaluator to evaluate OCD severity and symptom presentation. The scale comprises two parts. The first part is a 74-item symptom checklist assessing a broad range of current and past obsessions and compulsions. The second part, a severity scale, consists of 10 questions (five concerning obsessions and five concerning compulsions) that measures severity on a five-point scale, with a total score ranging from 0 to 40 [40]. The CY-BOCS symptom checklist includes one item regarding hoarding obsessions and one item regarding hoarding compulsions as well as two additional items where the clinician can report symptoms of hoarding obsessions and compulsions other than those defined in the checklist. If patients currently had any of these symptoms, they were classified as having hoarding symptoms in this study.
A score of < 16 on the CY-BOCS was used to define a treatment response as this was used in the NordLOTS. This score was originally chosen as it represents a severity level of mild OCD that has been used in several previous studies [41].
Indecision was measured with one item on the CY-BOCS (item 13), based on a Likert scale from 0 = no indecision to 4 = very indecisive. We measured insight by item no. 11 on the CY-BOCS (item no. 11). Insight is measured on a four-point scale (0 = excellent insight, 1 = good insight, 2 = fair insight, 3 = poor insight, = absent insight).”
The CY-BOCS has demonstrated reliability and validity in samples of children with OCD [42, 43]. In the NordLOTS, the intra-class correlation coefficients (ICC) of inter-rater agreement were as follows: obsessions ICC = 0.94 (95% CI 0.85–0.97), compulsions ICC = 0.87 (95% CI 0.67–0.93), and total score ICC = 0.92 (95% CI 0.78–0.97) [41].
Kiddie schedule for affective disorders and schizophrenia (K-SADS-PL)
K-SADS-PL is a diagnostic, semi-structured interview designed to assess a broad range of child and adolescent mental disorders according to DSM-IV criteria. The interview comprises an introductory interview, a screening interview, and a diagnostic part. Symptoms are scored as one of “not present,” “possible,” “in remission,” or “certain” [44]. K-SADS-PL has been shown to possess good inter-rater reliability (98%) and has a 1–5 week test–retest kappa of 0.80 for all included anxiety diagnoses [44]. The interview has been shown to have good convergent and divergent validity [45, 46]. This study used present diagnoses classified as “certain.”
The child obsessive–compulsive impact scale-revised (COIS-R)
COIS-R is a 33-item, self-reported questionnaire designed to assess the psychosocial functioning of children and adolescents in home, school, and social settings and to assess how OCD affects such functioning. Parent and child rating versions are available. Scale items are scored on a four-point Likert scale (0 = not at all, 1 = just a little, 2 = pretty much, and 3 = very much). The scale has moderate to high internal consistency of α = 0.92–0.94 and α = 0.78–0.92, respectively, for the parent and child versions [47, 48].
Child behavior checklist (CBCL)
The CBCL is used to evaluate child behavioral and emotional problems, as well as social competence. The scale, rated by parents, has 113 items on a three-point scale (0 = not true, 1 = somewhat or sometimes true, and 2 = very or often true). It has been shown to have good psychometric properties across different populations, mean test–retest reliability between 0.95–1.00, and internal consistency from α = 0.78 to α = 0.97 [49, 50].
The mood and feelings questionnaire (MFQ)
The MFQ is a questionnaire for both parents and children that is used to assess symptoms of depression based on the DSM-III-R. The scale comprises 13 items, scored in total from 0 to 26 [51]. The assessment has sound psychometric properties, and the scale’s total score has demonstrated internal consistency of α = 0.75 to α = 0.90 [50, 52, 53].
Autism spectrum screening questionnaire (ASSQ)
The ASSQ is a parent questionnaire, used to measure symptoms of autism, consists of 27 items rated on a three-point scale (0 = no, 1 = somewhat, and 2 = yes). The scale’s total score ranges from 0 to 54 and has an internal consistency of α = 0.86 [54]. The instrument has been proven a reliable and valid tool for screening in both clinical and general populations [55, 56]. Good internal consistency has been found for the versions in different languages this study used [57].
Screen for child-anxiety-related emotional disorders (SCARED)
The SCARED is a parent and child questionnaire used to measure symptoms of anxiety based on the DSM-IV, scored from 0 to 82. Its total score has demonstrated internal consistency of α = 0.92 for both child- and parent-rated versions [50].
Treatment
The treatment protocol included 14 weekly sessions of exposure-based CBT, with each session lasting approximately 75 min. In eight sessions, individual therapy was given to the child for 45 min, while the remaining time was used with the parents, either alone or with the child. Depending on the child’s age or preference, parents could also join for the whole session. In the remaining six sessions, the child and parents were seen together for the full session. Hoarding symptoms were treated according to the same principles as other OCD symptoms. Therapists in the study were child and adolescent psychiatrists, clinical psychologists, or certified psychotherapists with at least five years of clinical experience. Assessments with CY-BOCS and K-SADS-PL were conducted by independent raters which were appropriately trained clinical psychologists, psychiatrists, psychiatric nurse or social worker, to ensure their reliability [38]. Parent-rated assessments were scored by either one or two parents together. Therapy adherence and fidelity were found to be excellent but independent raters were used to assess all outcome measures [38]. The sample and treatment procedure have been described elsewhere [38, 41].
Analysis
The sample was split into two groups based on the presence of hoarding symptoms from the CY-BOCS checklist. Differences in age and OCD severity between the groups were estimated using independent sample t tests. The Mann–Whitney U test was used to compare non-normally distributed data. Group differences in comorbid diagnoses, gender, and national origin were evaluated using Pearson’s Chi-square tests.
A linear mixed-effect model (LME) was used to estimate group differences in CBT outcome [58]. CY-BOCS score, measured at baseline, week seven, and week 14, were set as the dependent variable over continuous time, with weeks from baseline, the presence or absence of hoarding symptoms, and interaction of hoarding symptoms with time as fixed effects. The model included a random intercept and linear slope. Whether hoarding symptoms affected response to CBT was estimated by multiple logistic regression, with response defined as CY-BOCS severity score < 16. Age, gender, and hoarding symptom status were included in the logistic regression model.
All analyses were conducted using SPSS version 22 [59], except for the LME model, which was fit using STATA [60]. All tests were two-tailed, and p < 0.05 was considered to indicate statistical significance.
Results
According to the CY-BOCS symptom checklist, 72 patients (26.8%) in the sample had one or more symptoms of hoarding, while the remaining 197 had no hoarding symptoms. Twelve patients reported having symptoms of hoarding in the past but reported no current symptoms of hoarding. Hoarding symptoms had no effect on completing CBT (p = 0.985). Of the 72 patients with hoarding symptoms, 15 had only compulsions and 12 had only obsessions concerning hoarding; most (n = 45) presented with both. Table 1 presents basic demographics, clinical group descriptive statistics, and group differences. Comorbid tic disorders and indecision were more prevalent among those with hoarding symptoms compared to those without hoarding symptoms (p = 0.005 and p = 0.024, respectively). In addition, those with hoarding symptoms scored significantly higher on the ASSQ motor/tics subscale (p = 0.013). No other measures differed significantly between the two groups although ADHD and anxiety disorder showed a trend toward significance (p = 0.084 and p = 0.076, respectively). OCD patients with hoarding symptoms had significantly more OCD symptoms in all CY-BOCS checklist categories except contamination obsessions, sexual obsessions, magical obsessions, and mental compulsions (Table 2).
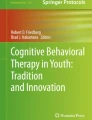
The observed mean reduction in OCD severity after treatment, measured with CY-BOCS, was 13.01 (SD= 8.44) for the non-hoarding group and 13.50 (SD= 7.87) for the hoarding group. LME analysis (χ2 (5) = 641.66, p < 0.001) did not show a significant difference in OCD severity reduction at posttreatment between groups (p = 0.933), indicating that having hoarding symptoms did not affect CBT outcome (Fig. 1). However, there was a significant within-group difference in both groups (13.19 points (p < 0.001) and 13.29 points (p < 0.001) for the non-hoarding and hoarding groups, respectively).

Estimated reduction in OCD severity for hoarding and non-hoarding OCD groups during 14 weeks of cognitive behavioral therapy, with 95% confidence intervals
When measuring outcome as a treatment response (CY-BOCS < 16), the logistic regression model (χ2 [3] = 8.16, p = 0.043), which also included age and gender, suggested that hoarding did not predict outcome [OR (CI) 0.64 (0.33–1.27), p = 0.204]. In the same model, age predicted treatment response [OR (CI) 0.90 (0.80–1.00), p = 0.048], while gender did not [OR (CI) 1.57 (0.88–2.81), p = 0.125].
Discussion
As expected, hoarding symptoms were frequently present (26.8%, n = 72) in the sample, supporting previous pediatric OCD studies that found rates of hoarding symptoms between 19% and 30% [19,20,21]. Hoarding symptoms may therefore develop at an early age and should be addressed in pediatric OCD populations.
Contrary to our hypothesis, the present study did not support earlier findings indicating lower insight in hoarding-related OCD compared to OCD without hoarding symptoms [19, 24]. Why remains unclear; one possibility is that insight may worsen with age in those patients whose hoarding symptoms continue to progress and become more severe, but the mean age of the sample in the study by Storch et al. [19], was slightly higher than in the present study. Consistent with previous studies [20, 24, 26], our study suggest that children and adolescents with hoarding symptoms have significantly higher levels of indecision. Unlike insight, indecision may precede hoarding symptoms, as indecision is thought to contribute to the development of hoarding [24]. Although the hoarding group in our sample tended to have earlier OCD onset, this difference was not the significant result some previous studies have reported [20, 26].
The results confirmed neither significantly elevated levels of anxiety disorders nor significantly elevated levels of ADHD among children and adolescents with OCD and hoarding symptoms, although a trend in that direction may be seen (p = 0.076 and p = 0.084 for anxiety disorders and ADHD, respectively). These comorbid disorders were found at relatively low rates in our sample, perhaps explaining these null findings. The fact that we analyzed anxiety disorders as a single group rather than individual diagnoses may also have an effect on the outcome as previous studies have not found differences for all types of anxiety [20]. Regarding ADHD, results from previous studies are inconsistent. One study found symptoms, but not diagnoses of ADHD to be higher in hoarding-related OCD [28], one found no difference in ADHD diagnoses between groups [19]. The study finding a significant difference in ADHD diagnoses between samples was based on relatively small sample sizes that could have affected the results [26]. Additionally, there were no group differences found regarding the CBCL internalizing/externalizing scales and the SCARED, indicating that anxiety and externalizing (i.e., ADHD) behavioral differences were also absent at the symptom level, which strengthens the null-difference findings regarding treatment outcome. On the other hand, and in support of previous findings [20], tic disorders were more common among the group with OCD and hoarding symptoms. Regarding autism, those with OCD and hoarding did not have a higher ASSQ total score and autistic style subscale, but patients with hoarding symptoms scored higher on the ASSQ subscale of motor/tics/OCD. This may be related to the items concerning tics on this scale and could indicate a higher rate of tics in this group.
In line with hypotheses and confirming results from previous studies [19, 20, 24, 31], in the present study OCD patients with hoarding symptoms had significantly more symptoms of OCD (based on the CY-BOCS checklist), especially symptoms of symmetry/ordering, repeating, counting. Hoarding has been associated with these symptoms in several previous factor analyses [61]. Only four symptom dimensions were less frequent: (1) contamination obsessions, (2) sexual obsessions, (3) magical obsessions; and (4) mental compulsion. It is unclear why those with hoarding show a trend to have more symptoms of the remaining dimensions.
Contrary to hypothesis, OCD severity and OCD-related impairment were not greater in the OCD group with hoarding symptoms. In addition, the between-group differences in the reduction of OCD severity during treatment was non-significant (p = 0.933). Hoarding symptoms also did not predict CBT response. In short, the presence of hoarding symptoms seemed to influence neither OCD severity nor CBT outcome in our sample. Possible explanations for these differences between the results of the present and previous studies could be due to the use of different diagnostic instruments. The K-SADS-PL was used to assess comorbidity in this study while the anxiety disorders interview schedule (ADIS) is commonly used in other studies. In addition, hoarding symptoms were rated with the CY-BOCS rather than with a separate instrument that could have provided more detail about the hoarding symptoms and their severity.
Insight has previously been identified as a predictor of treatment outcome [62] and correlated with low age and ADHD [25], and finding no difference in outcome, age and ADHD between groups in this study seems to support these results. The results presented here therefore suggest that CBT is also a helpful treatment for OCD with hoarding symptoms, in addition to OCD in general. Further studies should focus on how patient level of insight may affect treatment outcome independent of hoarding symptoms.
This study has several strengths. The sample size is large, the sample was well-defined by a comprehensive assessment of both OCD and comorbidity, treatment was manualized, and the sample received no medication for OCD during CBT. Limitations of this study include that the CY-BOCS was used to assess hoarding symptoms, and CY-BOCS includes relatively few hoarding-related items and cannot distinguish between mild and severe hoarding symptoms. It is possible that those with severe hoarding might respond differently to treatment compared to those with less severe hoarding or another explanation. Our sample consisted of children and adolescents with OCD and therefore our results cannot extend to children with hoarding disorder without OCD. Finally, the homogeneity of the Scandinavian sample limits the generalizability of its results to other, more diverse populations.
Conclusion
More than a fourth of children and adolescents with OCD included in the NordLOTS had one or more symptoms of hoarding. Those with hoarding symptoms more often had comorbid tic disorders, more often had problems with decision making, and had a different OCD symptom profile. In contrast to previous studies, findings of the present study suggest that OCD severity and CBT outcome are not affected by the presence of hoarding symptoms, confirming that the treatment response is similar in OCD with and without hoarding symptoms.
References
Heyman I, Fombonne E, Simmons H et al (2001) Prevalence of obsessive-compulsive disorder in the British nationwide survey of child mental health. Br J Psychiatry 179:324–329. https://doi.org/10.1097/00004583-200107000-00017
Thomsen PH (1993) Obsessive-compulsive disorder in children and adolescents. Self-reported obsessive-compulsive behaviour in pupils in Denmark. Acta Psychiatry Scand 88:212–217. https://doi.org/10.1111/j.1600-0447.1993.tb03441.x
Flament MF, Whitaker A, Rapoport JL et al (1988) Obsessive compulsive disorder in adolescence: an epidemiological study. J Am Acad Child Adolesc Psychiatry 27:764–771. https://doi.org/10.1097/00004583-198811000-00018
Canals J, Hernández-Martínez C, Cosi S, Voltas N (2012) The epidemiology of obsessive–compulsive disorder in Spanish school children. J Anxiety Disord 26:746–752. https://doi.org/10.1016/j.janxdis.2012.06.003
Huppert JD, Simpson HB, Nissenson KJ et al (2009) Quality of life and functional impairment in obsessive–compulsive disorder: a comparison of patients with and without comorbidity, patients in remission, and healthy controls. Depress Anxiety 26:39–45. https://doi.org/10.1002/da.20506
Weidle B, Ivarsson T, Thomsen PH et al (2015) Quality of life in children with OCD before and after treatment. Eur Child Adolesc Psychiatry 24:1061–1074. https://doi.org/10.1007/s00787-014-0659-z
Geller DA, March J (2012) Practice parameter for the assessment and treatment of children and adolescents with obsessive–compulsive disorder. J Am Acad Child Adolesc Psychiatry 51:98–113. https://doi.org/10.1016/j.jaac.2011.09.019
National Institute for Health and Clinical Excellence (2005) Obsessive–compulsive disorder: core interventions in the treatment of obsessive–compulsive disorder and body dysmorphic disorder. NICE, London
Skapinakis P, Caldwell D, Hollingworth W et al (2016) A systematic review of the clinical effectiveness and cost-effectiveness of pharmacological and psychological interventions for the management of obsessive-compulsive disorder in children/adolescents and adults. Health Technol Assess 20:1–392. https://doi.org/10.3310/hta20430
Storch EA, Bussing R, Small BJ et al (2013) Randomized, placebo-controlled trial of cognitive-behavioral therapy alone or combined with sertraline in the treatment of pediatric obsessive–compulsive disorder. Behav Res Ther 51:823–829. https://doi.org/10.1016/j.brat.2013.09.007
Ivarsson T, Skarphedinsson G, Kornør H et al (2015) The place of and evidence for serotonin reuptake inhibitors (SRIs) for obsessive compulsive disorder (OCD) in children and adolescents: views based on a systematic review and meta-analysis. Psychiatry Res 227:93–103. https://doi.org/10.1016/j.psychres.2015.01.015
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Publishing, Arlington
Ivanov VZ, Mataix-Cols D, Serlachius E et al (2013) Prevalence, comorbidity and heritability of hoarding symptoms in adolescence: a population based twin study in 15-year olds. PLoS one 8:e69140. https://doi.org/10.1371/journal.pone.0069140
Iervolino AC, Perroud N, Fullana MA et al (2009) Prevalence and heritability of compulsive hoarding: a twin study. Am J Psychiatry 166:1156–1161. https://doi.org/10.1176/appi.ajp.2009.08121789
Samuels JF, Bienvenu OJ, Grados MA et al (2008) Prevalence and correlates of hoarding behavior in a community-based sample. Behav Res Ther 46:836–844. https://doi.org/10.1016/j.brat.2008.04.004
Tolin DF, Meunier SA, Frost RO, Steketee G (2010) Course of compulsive hoarding and its relationship to life events. Depress Anxiety 27:829–838. https://doi.org/10.1002/da.20684
Cath DC, Nizar K, Boomsma D, Mathews CA (2017) Age-specific prevalence of hoarding and obsessive compulsive disorder: a population-based study. Am J Geriatr Psychiatry 25:245–255. https://doi.org/10.1016/j.jagp.2016.11.006
Kichuk SA, Torres AR, Fontenelle LF et al (2013) Symptom dimensions are associated with age of onset and clinical course of obsessive-compulsive disorder. Prog Neuropsychopharmacol Biol Psychiatry 44:233–239. https://doi.org/10.1016/j.pnpbp.2013.02.003
Storch EA, Lack CW, Merlo LJ et al (2007) Clinical features of children and adolescents with obsessive–compulsive disorder and hoarding symptoms. Compr Psychiatry 48:313–318. https://doi.org/10.1016/j.comppsych.2007.03.001
Samuels JF, Grados MA, Riddle MA et al (2014) Hoarding in children and adolescents with obsessive–compulsive disorder. J Obsessive Compuls Relat Disord 3:325–331. https://doi.org/10.1016/j.jocrd.2014.08.001
Sheppard B, Chavira D, Azzam A et al (2010) ADHD prevalence and association with hoarding behaviors in childhood-onset OCD. Depress Anxiety 27:667–674. https://doi.org/10.1002/da.20691
Bloch MH, Bartley CA, Zipperer L et al (2014) Meta-analysis: hoarding symptoms associated with poor treatment outcome in obsessive–compulsive disorder. Mol Psychiatry 19:1025–1030. https://doi.org/10.1038/mp.2014.50
Burton CL, Arnold PD, Soreni N (2015) Three reasons why studying hoarding in children and adolescents is important. J Can Acad Child Adolesc Psychiatry 24:128–130
Samuels JF, Bienvenu OJ, Pinto A et al (2007) Hoarding in obsessive–compulsive disorder: results from the OCD collaborative genetics study. Behav Res Ther 45:673–686. https://doi.org/10.1016/j.brat.2006.05.008
Selles RR, Højgaard DRMA, Ivarsson T et al (2018) Symptom insight in pediatric obsessive–compulsive disorder: outcomes of an international aggregated cross-sectional sample. J Am Acad Child Adolesc Psychiatry 57:615–619.e5. https://doi.org/10.1016/j.jaac.2018.04.012
Frank H, Stewart E, Walther M et al (2014) Hoarding behavior among young children with obsessive–compulsive disorder. J Obsessive Compuls Relat Disord 3:6–11. https://doi.org/10.1016/j.jocrd.2013.11.001
Storch EA, Nadeau JM, Johnco C et al (2016) Hoarding in youth with autism spectrum disorders and anxiety: incidence, clinical correlates, and behavioral treatment response. J Autism Dev Disord 46:1602–1612. https://doi.org/10.1007/s10803-015-2687-z
Park JM, Samuels JF, Grados MA et al (2016) ADHD and executive functioning deficits in OCD youths who hoard. J Psychiatr Res 82:141–148. https://doi.org/10.1016/j.jpsychires.2016.07.024
Ruta L, Mugno D, D’Arrigo VG et al (2010) Obsessive–compulsive traits in children and adolescents with Asperger syndrome. Eur Child Adolesc Psychiatry 19:17–24. https://doi.org/10.1007/s00787-009-0035-6
Lewin AB, Wood JJ, Gunderson S et al (2011) Phenomenology of comorbid autism spectrum and obsessive–compulsive disorders among children. J Dev Phys Disabil 23:543–553. https://doi.org/10.1007/s10882-011-9247-z
Højgaard DRMA, Mortensen EL, Ivarsson T et al (2017) Structure and clinical correlates of obsessive–compulsive symptoms in a large sample of children and adolescents: a factor analytic study across five nations. Eur Child Adolesc Psychiatry. https://doi.org/10.1007/s00787-016-0887-5
Mataix-Cols D, Rauch SL, Manzo PA et al (1999) Use of factor-analyzed symptom dimensions to predict outcome with serotonin reuptake inhibitors and placebo in the treatment of obsessive–compulsive disorder. Am J Psychiatry 156:1409–1416
Tolin DF, Frost RO, Steketee G, Muroff J (2015) Cognitive behavioral therapy for hoarding disorder: a meta-analysis. Depress Anxiety 32:158–166. https://doi.org/10.1002/da.22327
Storch EA, Rahman O, Park JM et al (2011) Compulsive hoarding in children. J Clin Psychol 67:507–516. https://doi.org/10.1002/jclp.20794
Storch EA, Merlo LJ, Larson MJ et al (2008) Symptom dimensions and cognitive-behavioural therapy outcome for pediatric obsessive–compulsive disorder. Acta Psychiatr Scand 117:67–75. https://doi.org/10.1111/j.1600-0447.2007.01113.x
Masi G, Millepiedi S, Perugi G et al (2009) Pharmacotherapy in paediatric obsessive-compulsive disorder: a naturalistic, retrospective study. CNS Drugs 23:241–252. https://doi.org/10.2165/00023210-200923030-00005
Bloch MH, Craiglow BG, Landeros-Weisenberger A et al (2009) Predictors of early adult outcomes in pediatric-onset obsessive–compulsive disorder. Pediatrics 124:1085–1093. https://doi.org/10.1542/peds.2009-0015
Torp NC, Dahl K, Skarphedinsson G et al (2015) Effectiveness of cognitive behavior treatment for pediatric obsessive–compulsive disorder: acute outcomes from the Nordic long-term ocd treatment study (NordLOTS). Behav Res Ther 64:15–23. https://doi.org/10.1016/j.brat.2014.11.005
Ivarsson T, Thomsen PH, Dahl K et al (2010) The rationale and some features of the Nordic long-term OCD treatment study (NordLOTS) in childhood and adolescence. Child Youth Care Forum 39:91–99. https://doi.org/10.1007/s10566-010-9097-3
Scahill L, Riddle MA, McSwiggin-Hardin M et al (1997) Children’s Yale–Brown obsessive compulsive scale: reliability and validity. J Am Acad Child Adolesc Psychiatry 36:844–852. https://doi.org/10.1097/00004583-199706000-00023
Thomsen PH, Torp NC, Dahl K et al (2013) The Nordic long-term OCD treatment study (NordLOTS): rationale, design, and methods. Child Adolesc Psychiatry Ment Health 7:41. https://doi.org/10.1186/1753-2000-7-41
Storch EA, Murphy TK, Geffken GR et al (2004) Psychometric evaluation of the children’s Yale–Brown obsessive–compulsive scale. Psychiatry Res 129:91–98. https://doi.org/10.1016/j.psychres.2004.06.009
Scahill L, Dimitropoulos A, McDougle CJ et al (2014) Children’s Yale–Brown obsessive compulsive scale in autism spectrum disorder: component structure and correlates of symptom checklist. J Am Acad Child Adolesc Psychiatry 53:97–107.e1. https://doi.org/10.1016/j.jaac.2013.09.018
Kaufman J, Birmaher B, Brent D et al (1997) Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 36:980–988. https://doi.org/10.1097/00004583-199707000-00021
Lauth B, Arnkelsson GB, Magnússon P et al (2010) Validity of K-SADS-PL (schedule for affective disorders and schizophrenia for school-age children-present and lifetime version) depression diagnoses in an adolescent clinical population. Nord J Psychiatry 64:409–420. https://doi.org/10.3109/08039481003777484
Villabø MA, Oerbeck B, Skirbekk B et al (2016) Convergent and divergent validity of K-SADS-PL anxiety and attention deficit hyperactivity disorder diagnoses in a clinical sample of school-aged children. Nord J Psychiatry 70:358–364. https://doi.org/10.3109/08039488.2015.1125944
Piacentini J, Peris TS, Bergman RL et al (2007) BRIEF REPORT: functional impairment in childhood OCD: development and psychometrics properties of the child obsessive–compulsive impact scale-revised (COIS-R). J Clin Child Adolesc Psychol 36:645–653. https://doi.org/10.1080/15374410701662790
Skarphedinsson G, Melin KH, Valderhaug R et al (2015) Evaluation of the factor structure of the child obsessive–compulsive impact scale—revised (COIS-R) in Scandinavia with confirmatory factor analysis. J Obsessive Compuls Relat Disord 7:65–72. https://doi.org/10.1016/j.jocrd.2015.03.005
Achenbach TM, Thomas M (1999) The Child Behavior Checklist and related instruments. In: Maruish Mark E (ed) The use of psychological testing for treatment planning and outcomes assessment, 2nd edn. Lawrence Erlbaum Associates Inc, Mahwah, pp 429–466
Torp NC, Dahl K, Skarphedinsson G et al (2015) Predictors associated with improved cognitive-behavioral therapy outcome in pediatric obsessive–compulsive disorder. J Am Acad Child Adolesc Psychiatry 54:200–207.e1. https://doi.org/10.1016/j.jaac.2014.12.007
Angold A, Costello EJ, Messer SC et al (1995) Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. Int J Methods Psychiatr Res 5:237–249
Angold A, Costello J, Van Kämmen W, Stouthamer-Loeber M (1995) Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents: factor composition and structure across development. Int J Methods Psychiatr Res 5:251–262
Wood A, Kroll L, Moore A, Harrington R (1995) Properties of the mood and feelings questionnaire in adolescent psychiatric outpatients: a research note. J Child Psychol Psychiatry 36:327–334. https://doi.org/10.1111/j.1469-7610.1995.tb01828.x
Ehlers S, Gillberg C (1993) The epidemiology of asperger syndrome. J Child Psychol Psychiatry 34:1327–1350. https://doi.org/10.1111/j.1469-7610.1993.tb02094.x
Posserud MB, Lundervold AJ, Gillberg C (2006) Autistic features in a total population of 7–9-year-old children assessed by the ASSQ (autism spectrum screening questionnaire). J Child Psychol Psychiatry Allied Discip 47:167–175. https://doi.org/10.1111/j.1469-7610.2005.01462.x
Ehlers S, Gillberg C, Wing L (1999) A screening questionnaire for Asperger syndrome and other high-functioning autism spectrum disorders in school age children. J Autism Dev Disord 29:129–141
Arildskov TW, Højgaard DRMA, Skarphedinsson G et al (2016) Subclinical autism spectrum symptoms in pediatric obsessive–compulsive disorder. Eur Child Adolesc Psychiatry 25:711–723. https://doi.org/10.1007/s00787-015-0782-5
Gueorguieva R, Krystal JH (2004) Move over ANOVA: progress in analyzing repeated-measures data and its reflection in papers published in the archives of general psychiatry. Arch Gen Psychiatry 61:310–317. https://doi.org/10.1001/archpsyc.61.3.310
IBM Corp (2013) IBM SPSS statistics for windows, version 22.0. IBM Corp, Armonk, NY
StataCorp (2015) Stata statistical software: release 14. StataCorp LP, College Station, TX:
Bloch MH, Landeros-Weisenberger A, Rosario MC et al (2008) Meta-analysis of the symptom structure of obsessive–compulsive disorder. Am J Psychiatry 165:1532–1542. https://doi.org/10.1176/appi.ajp.2008.08020320
Mataix-Cols D, Marks IM, Greist JH et al (2002) Obsessive–compulsive symptom dimensions as predictors of compliance with and response to behaviour therapy: results from a controlled trial. Psychother Psychosom 71:255–262
Acknowledgements
The authors would like to thank TrygFonden, Lundbeck Foundation and Central Region Denmark’s Research Fund for supporting the research presented in this article through project Grants.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Ivarsson has served on the speaker’s bureau of Shire Sweden. All remaining authors report no biomedical financial interests or potential conflicts of interest.
Rights and permissions
About this article

Cite this article
Højgaard, D.R.M.A., Skarphedinsson, G., Ivarsson, T. et al. Hoarding in children and adolescents with obsessive–compulsive disorder: prevalence, clinical correlates, and cognitive behavioral therapy outcome. Eur Child Adolesc Psychiatry 28, 1097–1106 (2019). https://doi.org/10.1007/s00787-019-01276-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-019-01276-x