
Abstract
To analyze weight gain, metabolic hormones, and homocysteine (Hcys) levels in children and adolescents on antipsychotics (AP) during a year-long follow-up. 117 patients, AP-naïve or quasi-naïve (less than 30 days on AP), were included. Weight, body mass index (BMI), BMI z-score (z-BMI), and levels of leptin, insulin, insulin resistance (HOMA-IR), adiponectin, ghrelin, thyroid stimulating hormone (TSH), free thyroxine (FT4), and Hcys were measured at baseline, and at 3, 6, and 12 months, while patients remained on the same AP. Patients (mean age: 14.4 ± 3 years; 64.1 % male) were on risperidone (N = 84), olanzapine (N = 20) or quetiapine (N = 13) from baseline up to 1-year follow-up and significantly increased weight (5.8 ± 4.3 kg at 3-month, 8.1 ± 6.1 kg at 6-month, and 11.6 ± 7.0 kg at 1 year), BMI, and z-BMI. Leptin levels significantly increased from baseline to 3 and 6 months, as did TSH levels from baseline to 3 months, while FT4 levels decreased from baseline to 3 and 6 months. Patients with BMI >85th percentile at baseline (N = 16) significantly increased weight, BMI, and z-BMI, more than patients with normal BMI over time. Higher baseline levels of insulin, HOMA-IR, and leptin were associated with increased weight/BMI during follow-up, while higher baseline levels of FT4, adiponectin, and ghrelin were associated with lower weight/BMI during follow-up. All AP were associated with increased weight and BMI/z-BMI in all of the assessments; however, at 1-year assessment, this increase was significantly higher for patients on quetiapine. Both higher baseline levels of insulin, HOMA-IR, and leptin, as well as being overweight/obese at baseline were associated with increased weight/BMI during 1-year follow-up in children and adolescents on AP. Awareness of weight-related parameters in this population may help inform decisions regarding AP prescriptions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Prescribing antipsychotics (AP), essentially second-generation APs, has become a common practice in treating children and adolescents suffering from different psychiatric disorders [1], especially in the last decade [2–4].
Some studies suggest that the child and adolescent population has greater vulnerability to weight gain associated with medication intake [5–7]. Moreover, the younger the child, the greater the weight-gain risk [8]. Other medical problems, such as hyperglycemia, dyslipidemia, and high blood pressure, are associated with weight gain at the metabolic level [5]. All of this may have a negative physical and psychological impact on patients, increasing morbimortality [9], decreasing the quality of life, and lowering adherence to treatment [10].
There are several possible mechanisms to explain the metabolic abnormalities associated with APs. The main one is the direct effect of the drug antagonizing different brain receptors (H1 and H3 hystaminergic [11], 5HT2A and 2C serotonergic and alpha1 and alpha2 adrenergic receptors [12]), but there is also the effect of various peptide hormones originating in the peripheral system which send signals to the brain through different pathways. It is thought that all of these mechanisms act to increase weight through food intake, resting energy expenditure and physical activity [13]. The most important agents in the regulation of energetic homeostasis and body weight are insulin and leptin [14], although other hormones, such as ghrelin, adiponectin, thyroid hormones as well as the amino acid homocysteine (Hcys), are also involved. Leptin is a hormone that plays a key role in regulating appetite and body weight. It is mainly secreted by adipocytes. Its main function is to regulate energy balance through a negative feedback mechanism involving the hypothalamus and the ventral tegmental area [15]. The production of circulating leptin is related to adiposity. Peripheral administration of leptin reduces appetite and feeding [16]. Insulin is a hormone produced by beta pancreatic cells in the liver. It binds to receptors in the arcuate nucleus of the hypothalamus and, like leptin, provides information on energy status at the peripheral level. Moreover, insulin stimulates leptin’s secretion [17]. Ghrelin is a peptide hormone that appears to play a crucial role in regulating energy in the short term. It is secreted by the stomach and binds the growth hormone secretagogue receptor [18]. Ghrelin acts in a manner that is the opposite of leptin and insulin, as its orexygenic effect controls energy balance by increasing fat deposits and food intake [18]. Levels of circulating ghrelin increase before meals and decrease after meals [19]. Insulin seems to decrease ghrelin levels [16]. Adiponectin is a hormone secreted only by fatty cells involved in weight regulation processes by increasing fatty acid oxidation and glucose use [20]. In humans, adiponectin levels are negatively correlated to body weight and insulin levels. Serum adiponectin levels decrease with obesity, insulin resistance, and type II diabetes [21]. Thyroid hormones regulate basal and total energy consumption and could influence body composition [22]. Increases in thyroid stimulating hormone (TSH) levels have been described in obese children and adolescents [23, 24], and leptin might play a role in the relationship between thyroid hormone levels and body composition [25, 26]. As such, an increase of leptin could mediate an increase in thyrotropin-releasing hormone levels (TRH), resulting in an increase of TSH [23]. Hcys is a sulfur-containing amino acid formed during the metabolism of the essential amino acid methionine (one-carbon metabolism, OCM). High levels of Hcys have been consistently associated with cardiovascular risk [27]. Its relationship with being overweight and obesity is controversial in adult studies [28, 29], although higher BMI has recently been associated with higher Hcys levels in children [30].
Studies focusing on the relationship between AP-induced weight gain and the hormones involved in energetic homeostasis mechanisms have considerably increased in recent years. One review [31] states that leptin increases during AP treatment as a consequence of weight gain rather than as a direct effect of AP on leptin levels. Weight gain is also related to increased levels of ghrelin in most [32, 33], but not all [34] studies. It has been reported that ghrelin levels decrease during the first few weeks after beginning AP treatment and increase over time [16]. However, adiponectin has only been associated with weight gain in patients on olanzapine [33, 35].
There is scarce information about the relationship between weight gain and regulating hormones in children and adolescents on AP. It has been reported that body mass index (BMI) and leptin levels increased after 6 weeks on clozapine [36]. Moreover, in an 8-week observational study, despite a mean weight increase of approximately 4 kg, only insignificantly higher leptin levels were found in children and adolescents with psychotic disorders on AP [37]. In a 6-month follow-up study, serum leptin changes were not associated with weight gain in a sample of children with autism on risperidone [38]. In a study of children and adolescents with a mean of 2.9 years on risperidone, it was found that overweight or obese patients had higher insulin levels and insulin resistance than those with normal BMI [39]. To our knowledge, there have been no prospective longer follow-up studies addressing the relationship between weight and hormones in AP-naive or quasi-naive children and adolescents beginning AP treatment.
The main purpose of our study was to analyze weight gain, its relationship to hormones and amino acids associated with weight, and examine their evolution during a 1-year follow-up in a sample of naïve or quasi-naïve children and adolescents on AP treatment.
We hypothesized that patients’ weight, BMI, and BMI z-score (z-BMI) would increase from baseline to the different assessments of the follow-up. We also expected that weight gain would be associated with an increase in leptin, insulin, ghrelin, TSH, and Hcys, and a decrease in adiponectin levels.
Method
Subjects
Subjects were recruited from four child and adolescent Psychiatry departments at university hospitals in Spain. Both inpatients and outpatients visiting at these facilities between May 2005 and April 2007 who met the inclusion criteria were invited to participate in the study (for a full description of the study design, see [40]). Inclusion criteria were: age between 4 and 17 years at the time of first evaluation, with any psychiatric diagnoses according to DSM-IV criteria except for eating disorders; and being AP-naïve (prescribed an AP drug for the first time at baseline) or quasi-naïve (having begun any first AP treatment up to 30 days before baseline). Patients who did not have at least two assessments during the follow-up were not included in the study. There were no exclusion criteria.
For this study, from the whole sample, only patients whose baseline serum leptin levels had been measured were included (only two centers: Hospital Gregorio Marañón, Madrid, and Hospital Clínic, Barcelona, could perform this measurement). Moreover, only patients who continued their AP treatment during the whole follow-up period with the same single AP were included in this analysis. If a patient switched to a different AP or another was added, only the visits prior to that change were included. Additionally, since most patients were on risperidone, olanzapine or quetiapine, three patients who were on different AP were removed from the analysis (Fig. 1). The final sample included 117 subjects.

Participants flow chart
The study was approved by the ethical committees of all participating clinical centers. Parents or legal guardians of all patients gave written informed consent, and all patients older than 12 years agreed to participate.
Procedure
Patients were followed up during 1 year, with assessments at baseline, 3, 6, and 12 months, while they were on the same AP. In each evaluation, a blood analysis was performed; weight and height were measured, and AP and other pharmacological treatments were registered (drugs, dosage). AP doses were converted to chlorpromazine equivalents [41].
Assessment
Hormones
Serum leptin, insulin, adiponectin, TSH, and FT4 levels were measured in both centers. Ghrelin and Hcys levels were only measured in patients included in one of the centers (Hospital Clínic, Barcelona).
Leptin was measured with enzyme-linked immunosorbent assay (ELISA) (BioVendor, ref: RD191001100) in one center and by radioimmunoassay (Linco Research, St. Charles, MO, USA) in another. Insulin was measured in both places using a solid-phase, 2-site chemiluminescent immunometric assay (IMMULITE 2000 Insulin, CPS). Insulin resistance was determined using the homeostatic model assessment [HOMA-IR: fasting insulin (µIU/mL) × glucose (mg/dL)/405] [42]. Adiponectin levels were obtained using enzyme-linked immunosorbent assay (ELISA) (BioVendor, ref: RD195023100 and by radioimmunoassay (Linco Research, St. Charles, MO, USA), depending on the center. Both TSH and FT4 were measured using radioimmunoassay (Diagnostic Product Corporation, Los Angeles, CA, USA) at both sites. Ghrelin levels were measured by radioimmunoassay (Ghrelin-Total RIA Kit; Linco Research). Hcys levels were assessed by electrochemiluminiscence immunoassay in an Advia Centaur® analyzer (Siemens Healthcare, Barcelona, Spain).
Height and weight
Weight and height were measured with the same sliding-weight scale at both centers. Height was measured in meters to the nearest 0.1 cm, using a SECA 220 stadiometer. Body weight was measured in kilograms (kg) to the nearest 0.2 kg, wearing light clothes and no shoes, using platform scales. BMI and z-BMI (standardized BMI adjusted for age and gender) were also calculated, in agreement with standard Spanish tables [43].
Diagnoses
Psychiatric diagnoses were made by child and adolescent psychiatrists in each center, according to DSM-IV-TR criteria, at baseline. Diagnoses were grouped into the following categories: schizophrenia spectrum disorders, bipolar disorders, depressive disorders, disruptive behavior disorders, pervasive developmental disorder, and tic spectrum disorders (for a full description of diagnostic categories and use of AP associated, see [1]).
Data analysis
For descriptive purposes, continuous variables were expressed as means, standard deviations (SD), and ranges, and categorical variables were expressed as frequencies and/or percentages. MANOVA for repeated measures was used to compare the parameters in the different assessments. Student’s t test was used to compare assessments one by one when MANOVA for repeated measures was significant.
To assess differences between patients that were overweight/obese (with a BMI ≥85th percentile [44]) at baseline and those who were not, we used Student’s t test.
The linear mixed-effects model for longitudinal data (R) was used to analyze the relationship between hormone and Hcys levels at baseline and weight/BMI during the follow-up. We also used linear mixed models to analyze the weight/BMI/z-BMI change at the different assessments according to AP.
Pearson/Spearman correlations were used to assess continuous variables or categorical ones.
All tests were two-tailed. Statistical analyses were carried out with the SPSS 18.0 (Statistical Package for the Social Sciences, Chicago, USA) and R statistics version 3.2.1 (http://www.r-project.org) using linear mixed models with package lme4 (version 1.1-8). Differences of p < 0.05 were considered significant.
Results
Sociodemographic characteristics, diagnoses, and treatment at baseline
Table 1 shows the sociodemographic data, diagnoses, and treatment at baseline of the sample. When patients entered the study, 57 (48.7 %) were AP-naïve, and those already on AP had a previous mean exposure of 6.8 ± 6.9 days on medication. The AP dose of quasi-naïve patients at baseline is shown in Table 2.
From baseline to the different assessments, there was a decrease in the patient sample (Fig. 1). Five (3.4 %) patients were excluded from the study during the follow-up because of AP switch, 2 (1.7 %) for adding a new AP, and 8 (6.8 %) for not having blood analysis results due to technical reasons. Moreover, 36 (30.8 %) patients left the study for medical reasons (mainly, clinical improvements which led to stopping AP treatment), and 27 (23.1 %) for other reasons, such as noncompliance and failure to continue follow-up. The same decrease was found in the subsample for which ghrelin and Hcys were measured (from 33 subjects at baseline to 17 at 3 months, 13 at 6 months, and 8 at 1 year). No differences in age, gender, diagnosis, and baseline hospitalization were found between patients who were excluded or left the study and those who completed it (data not shown).
Evolution of weight, BMI, z-BMI, and levels of laboratory parameters associated with weight
Mean weight, BMI, and z-BMI score significantly increased from baseline to all the posterior assessments (p < 0.001 for all the assesments) (Table 3). No differences were found on any BMI and z-BMI assessment when we compared patients who at baseline were using stimulants (n = 5) vs. those not using them (N = 112), or between patients who were taking any concomitant psychotropic medication (N = 47) vs. those not taking any (N = 70) (data not shown). AP dose and its chlorpromazine equivalents at all of the assessments are shown in Table 2.
Mean leptin levels increased from baseline to 3- and 6-month visits with statistical significance (F = 3.233, p = 0.047). Mean TSH levels significantly increased from baseline to 3- and 6-month assessments (F = 3.424, p = 0.034), while FT4 levels significantly decreased from baseline to 3-month evaluation (F = 3.000, p = 0.025) (Table 3 shows the complete comparison data). The other mean levels of laboratory parameters measured did not significantly change across the assessments (Table 3).
When we divided the sample by gender, mean leptin levels were significantly higher in female than in male subjects at baseline (15.4 ± 14.4 vs. 7 ± 11.4 ng/mL, t = 3.459, p = 0.001), 3-month (42.4 ± 25.3 vs. 17.4 ± 8.2 ng/mL, t = 2.900, p = 0.014) and 12-month assessments (20.9 ± 12.7 vs. 6.8 ± 7 ng/mL, t = 3.969, p < 0.001). No other differences were found among the other parameters.
Differences in weight gain and BMI/z-BMI increase depending on the AP prescribed
Weight gain and BMI/z-BMI increase from baseline to 3-, 6-, and 12-month assessments varied according to the AP prescribed, as shown in Table 4. Patients on different AP showed different degrees of weight gain and BMI/z-BMI increase at all of the assessments. However, only from baseline to the 12-month assessment was there statistically significant data, with patients on quetiapine gaining a mean of 9.5 kg more than those on risperidone, and 7.7 kg more than those on olanzapine (t = 2.403, p = 0.0217) (Table 4).
In patients on quetiapine, a relationship was detected between weight gain and BMI/z-BMI increase from baseline to 12-month and mean daily dose at 12-month assessment (R = 0.975, p = 0.005 for all the analyses). No such relationship was found for risperidone or olanzapine.
Evolution of parameters in baseline overweight/obese subjects compared to normal BMI subjects
In overweight/obese subjects (n = 16, 13.7 % from the whole sample, at baseline; n = 14, 16.9 %, at 3-month; n = 11, 17.5 %, at 6-month; and n = 7, 17.9 %, at 12-month visits), mean levels of leptin and HOMA-IR were significantly higher in all of the assessments compared to normal BMI subjects. Moreover, mean levels of insulin were significantly higher at 3 and 12-month visits in overweight/obese subjects compared to those with normal BMI (Table 5).
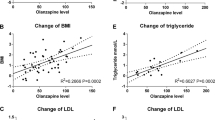
From baseline to 3, 6, and 12 months, overweight/obese as well as normal BMI patients increased in weight, BMI, and z-BMI, with a significant interaction of time by group (weight, F = 31.261, df = 3.31, p < 0.001; BMI, F = 26.268, df = 3.31, p < 0.001 and z-BMI, F = 24.816, df = 3.31, p < 0.001). Thus, overweight/obese patients at baseline had a significantly higher increase in weight/BMI and z-BMI than normal BMI subjects during the follow-up (Fig. 2).

Change over time of mean BMI z-scores in normal BMI (BMI < 85th percentile) and overweight/obese (BMI ≥ 85th percentile) patients at baseline. Axis: x = assessment visits; y = BMI z-scores. Time: F(3, 31) = 55.501, p < 0.001. Group × Time interaction: F(3,31) = 8.131, p < 0.001
Regarding laboratory parameters, only insulin (F = 5.289, df = 3.17, p = 0.009) and HOMA-IR (F = 5.434, df = 3.17, p = 0.008) increased in each of the assessments with a significant interaction of time by group (Fig. 2). Baseline overweight/obese patients had significantly higher levels of insulin and HOMA-IR than did normal BMI subjects during the follow-up.
Baseline parameters and weight and BMI at follow-up
Some laboratory parameters at baseline were associated with an increase in weight at follow-up. Baseline insulin levels (t = 2.41, p = 0.01) and HOMA-IR (t = 3.31, p = 0.001) were associated with weight, with an increase of one insulin unit being associated with a mean increase of 1.16 kg. Baseline leptin levels (t = 4.22, p = 0.0001) were also linked to an increase in weight (an increase of one leptin unit being associated with a mean increase of 0.19 kg). The same baseline parameters were associated with BMI at follow-up (insulin levels: t = 3.40, p < 0.001; HOMA-IR: t = 4.45, p < 0.001 and leptin levels: 6.02, p < 0.001).
The same statistical test showed that other baseline laboratory parameters were associated with lower weight at follow-up. Higher FT4 (t = −7.194, p < 0.001), adiponectin (t = −3.77, p < 0.001), and ghrelin levels (t = −3.849 p < 0.001) were all linked to a decrease in weight at follow-up.
Pearson/Spearman correlations showed no direct link between cumulative doses of AP at each assessment and the increase in weight and BMI from baseline to 3-, 6- or 12-month assessments. First or second degree family background of obesity also did not correlate with the increased weight or BMI in the different visits (data not shown).
Discussion
Our study found that higher baseline levels of insulin, HOMA-IR, and leptin were significantly associated with higher weight/BMI during the 1-year follow-up; while higher baseline levels of FT4, adiponectin, and ghrelin were linked to lower weight/BMI during the follow-up in children and adolescents on treatment with the same single AP (risperidone, olanzapine or quetiapine). Weight, BMI, and z-BMI increased from baseline to 3, 6, and 12 months, and at the same time, leptin levels significantly increased from baseline to 3 and 6-month assessments. TSH levels significantly increased from baseline to 3 and 6-month visits, and FT4 levels significantly decreased from baseline to 3-month assessment. Moreover, different degrees of weight gain and BMI/z-BMI increase were found for each of the prescribed AP at all of the assessments. However, only at 1-year follow-up were these differences significant, with quetiapine being associated with significantly greater increases than risperidone or olanzapine.
Weight significantly increased in our sample from baseline to the follow-up assessments (5.8 ± 4.3 kg at 3 months, 8.1 ± 6.1 kg at 6 months, and 11.6 ± 7.0 kg at 1 year). Weight gain in children and adolescents on AP has been consistently reported [8, 45] in studies with follow-up periods ranging from 4 weeks to 2 years. Nevertheless, few studies have had a 1-year or longer follow-up [7]. Additionally, our study was unique in that it focused on patients who were on the same single AP during the entire follow-up. As a result, our findings do not exactly confirm those of other studies, because AP polypharmacy seems to confer a higher risk for weight gain in children and adolescents [46].
Concomitant treatment in addition to AP could also play a role in weight gain, and exposure to two or more medications appears to be a predictor of being overweight [8]. However, in our study, we did not find that patients with concomitant psychotropic drugs had different BMI or z-BMI than those without them. Moreover, among patients with concomitant treatment with only stimulants (which could decrease appetite and produce weight loss [47]), no differences were observed in BMI or z-BMI compared to the rest of the sample in any of the assessments. The fact that only 5/117 (4.3 %) patients were on stimulants in our sample does not allow this finding to have sufficient statistical power, but other authors have also reported similar results [48].
In our study, leptin levels increased during the first 6 months of treatment. A significant increase was found between baseline and 3 and 6 months, while a decrease was found from 6- to- 12-month assessments. We also found a relationship between baseline leptin levels and the mean increase in weight/BMI during follow-up. In child and adolescent samples, shorter follow-up studies have not found a relationship between increased weight and serum leptin levels [37, 38], except for one study [34] where BMI and serum leptin levels increased from baseline to week 6 of treatment with clozapine. However, the association between weight and leptin levels is consistently observed in adult studies [32]. Increases in leptin levels during AP treatment could be a result of weight gain rather than a direct effect of atypical AP on leptin physiology [32]. Increased leptin levels in healthy subjects imply that fat stores are sufficient, and that the subject should decrease food intake. However, in patients on AP, it is possible that the ability of hyperleptinemia to decrease food intake is lost [36]. AP could interfere with the neural processing of leptin by blocking 5-HT2C, which modifies appetite and feeding behavior [49]. In fact, most obese subjects are resistant to the effects of endogenous leptin [16], and AP treatment could cause a similar resistance.
Moreover, we found that female patients had higher leptin levels in almost all of the assessments (baseline, 3, and 12 months), which is consistent with other studies in children and adolescents not on AP [50, 51]. It has been reported that higher levels of leptin in adolescent girls are associated with an increase of fat mass during puberty, compared to the increase of lean mass in boys [52]. No studies are found in the literature, which examine AP use in this population and the possible gender-specific effects of leptin levels.
Thyroid hormones significantly changed in the short-term follow-up. TSH levels increased from baseline to 3- and 6-month assessments, although this could be explained as a consequence of weight gain rather than a cause of it [23]. FT4 levels significantly decreased from baseline to 3-month visits, but not in later assessments. This could be explained by the decreasing sample size over time. The decrease in FT4 levels could be associated with the increased TSH levels as a possible adaptive process [22]. Moreover, baseline FTA levels were associated with a decrease in mean weight/BMI. Thyroid hormones have been related to the mechanism of weight gain [22], and this has been widely described in obese children and adolescents [23]. In our study, only FT4 and not TSH levels were related to the increase of weight/BMI, although this may be due to the linear correlation described for TSH with FT3 levels, but not with FT4 in pediatric subjects [53]. Other authors [54] have studied the relationship between TSH and weight in children with obesity, and reported a positive correlation between TSH and FT3 levels and z-BMI, but not FT4. Margari et al. [55] described an increase in FT3 levels in children and adolescents after 6 months on risperidone, but they did not study the possible association with increased weight and BMI. Unfortunately, we did not measure FT3 in our study.
The other parameters analyzed (insulin, HOMA-IR, adiponectin, ghrelin, and Hcys) were not significantly different from baseline to the other assessments in the whole sample. However, higher baseline insulin levels/HOMA-IR were linked to an increase of mean weight/BMI at follow-up. This is consistent with higher insulin levels/HOMA-IR described in children and adolescents on AP at 6-month follow-up [45] and insulin levels in longer follow-up [39]. Moreover, higher baseline adiponectin and ghrelin levels were associated with a mean decrease in weight/BMI at follow-up. Among adults, adiponectin has been associated with weight gain in patients on olanzapine in some studies [33, 35], but not others [31]. Studies of ghrelin have also shown controversial results in studies ranging from 1 week to 1 year of follow-up [31]. All previous studies have been conducted with adult patients only.
We found no changes in Hcys levels during the assessment and no relationship between baseline Hcys and weight/BMI at follow-up. Nevertheless, Yakub et al. [30] described a relationship in children between high Hcys levels and increased weight. Moreover, in adults with a first episode of psychosis, increased BMI and higher levels of Hcys after 12 weeks on AP have been described, and changes in Hcys levels were associated with changes in BMI [56]. In our study, it is possible that the negative results relate to the fact that Hcys measures were obtained for only a limited number of subjects.
We also found that different AP had a different impact on weight gain and BMI increase, with patients on quetiapine showing greater gains at 1-year assessment than those on risperidone or olanzapine. Supporting our results, Correll et al. [5] described, in a naturalistic 12-week study, that patients on quetiapine increased more weight than those on aripiprazole or risperidone; However, no patients in that study were on olanzapine. A review of weight gain in children and adolescents on AP [8] reported that olanzapine appears to cause the most significant weight gain, with quetiapine being associated with lower weight gain than olanzapine or risperidone treatment [8]. In a comprehensive review of controlled or prospective studies of AP treatment in children and adolescents with psychotic or bipolar spectrum disorders [3], olanzapine has also been associated with the highest increased weight. The authors suggested a ranking for SGA-induced weight in the pediatric population of olanzapine ≥ clozapine > risperidone ≥ quetiapine > aripiprazole = ziprasidone. Our group has also previously reported a follow-up study in children and adolescents where risperidone, olanzapine, and quetiapine were all associated with a 7 % increase in patients’ weight at 6 months, although both risperidone and olanzapine were associated with a higher proportion of patients showing this 7 % gain than was quetiapine. Moreover, patients on quetiapine had reached their maximum weight after the first 3 months of treatment, while those on risperidone and olanzapine continued to gain weight up to end point [45]. Olanzapine and quetiapine have a similar receptor-binding profile [57], and this could play a role in their potential to produce weight gain.
In our sample, baseline overweight/obese patients showed greater increases in weight, BMI, and z-BMI than patients with normal BMI. This is contrary to previous adult studies which report that patients with lower baseline BMI are at increased risk of weight gain [48]. In children and adolescents, controversial data on this issue have been reported [8]. We also observed differences in leptin and insulin levels as well as HOMA-IR between overweight/obese and normal BMI patients. Other authors have observed higher levels of leptin [58] and of insulin and HOMA-IR [59] in obese children. In fact, insulin and leptin are interrelated, since insulin stimulates the secretion of leptin [17]. We did not find differences in TSH levels between overweight/obese and normal BMI subjects, in contrast to the increased TSH in obese patients that has been widely reported [23]. Because changes in TSH seem to be more a consequence than a cause of obesity [23], it is possible that obese/overweight patients on AP have a different pattern of adaptive response to weight gain. Other laboratory parameters showed no differences between overweight/obese and normal BMI patients.
In our study, we did not find any correlation between family background of obesity and increased weight, BMI or z-BMI over time. This differs from one adolescent study which reports a correlation between paternal BMI and weight gain after 12 weeks on AP [60]. We also found no correlation between weight gain and the other parameters studied. This contrasts with Sporn et al. [36] who found in children and adolescents with schizophrenia correlations between an increased BMI and a decrease in ghrelin and adiponectin levels after 6 weeks on clozapine, stating that these changes, also seen in obese subjects, probably represent secondary compensatory changes resulting from weight gain.
Limitations and strengths
Several limitations to our study deserve mention: the sample size was reduced during the follow-up; we did not measure FT3 levels or other OCM markers, such as folic acid and vitamin B12; we did not have a single laboratory to perform all of the necessary measurements, and leptin and adiponectin levels were analyzed using two different methods; and we did not register the dietary habits or physical activity of patients. Moreover, it is a naturalistic study where AP was prescribed by clinical criteria, and our results cannot be compared to randomized or controlled studies.
However, among its strengths are the prospective design, with 12 months of follow-up; the homogeneity of the sample, with AP-naïve or quasi-naïve children and adolescents; the repeated measurements of laboratory parameters (not only at baseline and end point); and its naturalistic design, which can offer more generalizable results, similar to clinical practice.
To sum up, we found an increase from baseline to 1 year in weight, BMI, and z-BMI in a sample of children and adolescents treated with a single AP. Increases in leptin and TSH and decreases in FT4 levels were observed. Higher baseline levels of insulin, HOMA-IR, and leptin, were all associated with increased weight/BMI during the follow-up, as was being overweight/obese at baseline. Higher baseline levels of FT4, adiponectin, and ghrelin were associated with lower weight/BMI during the follow-up. Additionally, weight gain and BMI/z-BMI increase at 1-year assessment were significantly higher for patients on quetiapine.
Further studies, especially ones with different AP and longer follow-up periods, are needed to confirm these results. Increased awareness of the role of these biochemical parameters could help improve the management of weight gain in children and adolescents on AP, a problem with significant physical and emotional coonsequences in this population.
References
Baeza I, De la Serna E, Calvo-Escalona R, Morer A, Merchán-Naranjo J, Tapia C, Martínez-Cantarero MC, Andrés P, Alda JA, Sánchez B, Arango C, Castro-Fornieles J (2014) Antipsychotic use in children and adolescents. A 1-year follow-up study. J Clin Psychopharmacol 5:613–619
Olfson M, Blanco C, Liu SM, Wang S, Correll CU (2012) National trends in the office-based treatment of children, adolescents, and adults with antipsychotics. Arch Gen Psychiatry 69:1247–1256
Fraguas D, Correll CU, Merchán-Naranjo J, Rapado-Castro M, Parellada M, Moreno C, Arango C (2011) Efficacy and safety of second-generation antipsychotics in children and adolescents with psychotic and bipolar spectrum disorders: comprehensive review of prospective head-to-head and placebo-controlled comparisons. Eur Neuropsychopharmacol 21:621–645
Arango C (2015) Present and future of developmental neuropsychopharmacology. Eur Neuropsychopharmacol 25:703–712
Correll CU, Manu P, Olshanskiy V, Napolitano B, Kane JM, Malhotra AK (2009) Cardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescents. JAMA 302:1765–1773
Fleischhaker C, Heiser P, Hennighausen K, Herpertz-Dahlmann B, Holtkamp K, Mehler-Wex C, Rauh R, Remschmidt H, Schulz E, Warnke A (2006) Clinical drug monitoring in child and adolescent psychiatry: side effects of atypical neuroleptics. J Child Adolesc Psychopharmacol 16:308–316
Safer DJ (2004) A comparison of risperidone-induced weight gain across the age span. J Clin Psychopharmacol 24:429–436
Martínez-Ortega JM, Funes-Godoy S, Díaz-Atienza F, Gutiérrez-Rojas L, Pérez-Costillas L, Gurpegui M (2013) Weight gain and increase of body mass index among children and adolescents treated with antipsychotics: a critical review. Eur Child Adolesc Psychiatry 22:457–479
Cohn TA, Sernyak MJ (2006) Metabolic monitoring for patients treated with antipsychotic medications. Can J Psychiatry 51:492–501
Allison DB, Mentore JL, Heo M, Chandler LP, Cappelleri JC, Infante MC (1999) Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 156:1686–1696
Deng C, Weston-Green K, Huang X (2010) The role of histaminergic H1 and H3 receptors in food intake: a mechanism for atypical antipsychotic-induced weight gain? Prog Neuropsychopharmacol Biol Psychiatry 34:1–4
Baptista T (1999) Body weight gain induced by antipsychotic drugs: mechanisms and management. Acta Psychiatr Scand 100:3–16
Cuerda C, Velasco C, Merchán-Naranjo J, García-Peris P, Arango C (2014) The effects of second-generation antipsychotics on food intake, resting energy expenditure and physical activity. Eur J Clin Nutr 68:146–152
Havel PJ (2001) Peripheral signals conveying metabolic information to the brain: short-term and long-term regulation of food intake and energy homeostasis. Exp Biol Med (Maywood). 226:963–977
Friedman JM (2002) The function of leptin in nutrition, weight, and physiology. Nutr Rev 60:S1–14 (discussion S68–84, 85–87)
Sentissi O, Epelbaum J, Olié JP, Poirier MF (2008) Leptin and ghrelin levels in patients with schizophrenia during different antipsychotics treatment: a review. Schiz Bull 34:1189–1199
Barsh GS, Schwartz MW (2002) Genetic approaches to studying energy balance: perception and integration. Nat Rev Genet 3:589–600
Nakazato M, Murakami N, Date Y, Kojima M, Matsuo H, Kangawa K, Matsukura S (2001) A role for ghrelin in the central regulation of feeding. Nature 409:194–198
Lucidi P, Murdolo G, Di Loreto C, Parlanti N, De Cicco A, Ranchelli A, Fatone C, Taglioni C, Fanelli C, Santeusanio F, De Feo P (2004) Meal intake similarly reduces circulating concentrations of octanoyl and total ghrelin in humans. J Endocrinol Invest 27:RC12–5
Heilbronn LK, Smith SR, Ravussin E (2003) The insulin-sensitizing role of the fat derived hormone adiponectin. Curr Pharm Des 9:1411–1418
Weyer C, Funahashi T, Tanaka S, Hotta K, Matsuzawa Y, Pratley RE, Tataranni PA (2001) Hypoadiponectinemia in obesity and type 2 diabetes: close association with insulin resistance and hyperinsulinmia. J Clin Endocrinol Metab 86:1930–1935
Reinehr T (2010) Obesity and thyroid function. Mol Cel Endocrinol 316:165–171
Reinehr T (2011) Thyroid function in the nutritionally obese child and adolescent. Curr Opin Pediatrics 23:415–420
Aypak C, Türedi O, Yüce A, Görpelioğlu S (2013) Thyroid-stimulating hormone (TSH) level in nutritionally obese children and metabolic co-morbidity. J Pediatr Endocrinol Metab 26:703–708
Jacobellis G, Ribaudo MC, Zappaterreno A, Iannucci CV, Leonetti F (2005) Relationship of thyroid function with body mass index, leptin, insulin sensitivity and adiponectin in euthyroid obese women. Clin Endocrinol 62:487–491
Roef G, Lapauw B, Goemaere S, Zmierczak HG, Toye K, Kaufman JM, Taes Y (2012) Body composition and metabolic parameters are associated with variation in thyroid hormone levels among euthyroid young men. Eur J Endocrinol 167:719–726
Martí-Carvajal AJ, Solà I, Lathyris D, Karakitsiou DE, Simancas-Racines D (2013) Homocysteine-lowering interventions for preventing cardiovascular events. Cochrane Database Syst Rev 1:CD006612. doi:10.1002/14651858.CD006612.pub3
Karatela RA, Sainani GS (2009) Plasma homocysteine in obese, overweight and hypertensive subjects in Mumbai. Indian Heart 61:156–159
Vayá A, Carmona P, Badia N, Pérez R, Hernandez Mijares A, Corella D (2011) Homocysteine levels and the metabolic syndrome in a Mediterranean population: a case-control study. Clin Hemorheol Microcirc 47:59–66
Yakub M, Schulze KJ, Khatry SK, Stewart CP, Christian P, West KP Jr (2014) High Plasma Homocysteine increases risk of metabolic syndrome in 6–8 year old children in rural Nepal. Nutrients 6:1649–1661
Jin H, Meyer JM, Mudaliar S, Jeste DV (2008) Impact of atypical antipsychotic therapy on leptin, ghrelin and adiponectin. Schiz Res 100:70–85
Palik E, Birkas KD, Faludi G, Karádi I, Cseh K (2005) Correlation of serum ghrelin levels with body mass index and carbohydrate metabolism in patients treated with atypical antipsychotics. Diabetes Res Clin Pract 68(suppl 1):S60–S64
Perez-Iglesias R, Vazquez-Barquero JL, Amado JA, Berja A, Garcia-Unzueta MT, Pelayo-Terán JM, Carrasco-Marín E, Mata I, Crespo-Facorro B (2008) Effect of antipsychotics on peptides involved in energy balance in drug-naive psychotic patients after 1 year of treatment. J Clin Psychopharmacol 28:289–295
Basoglu C, Oner O, Gunes C, Semiz UB, Ates AM, Algul A, Ebrinc S, Cetin M, Ozcan O, Ipcioglu O (2010) Plasma orexin A, ghrelin, cholecistokinin, visfasin, leptin and agouti-related protein levels during 6-week olanzapine treatment in first-episode male patients with psychosis. Int Clin Psychopharmacol 25:165–171
Richards AA, Hickman IJ, Wang AY, Jones AL, Newell F, Mowry BJ, Whitehead JP, Prins JB, Macdonald GA (2006) Olanzapine treatment is associated with reduced high molecular weight adiponectin in serum: a potential mechanism for olanzapine-induced insulin resistance in patients with schizophrenia. J Clin Psychopharmacol 26:232–237
Sporn AL, Bobb AJ, Gogtay N, Stevens H, Greenstein DK, Clasen LS, Tossell JW, Nugent T, Gochman PA, Sharp WS, Mattai A, Lenane MC, Yanovski JA, Rapoport JL (2005) Hormonal correlates of clozapine-induced weight gain in psychotic children: an exploratory study. J Am Acad Child Adolesc Psychiatry 44:925–933
Maayan LA, Vakhrusheva J (2010) Risperidone associated weight, leptin, and anthropometric changes in children and adolescents with psychotic disorders in early treatment. Human Psychopharmacol 25:133–138
Martin A, Scahill L, Anderson G, Aman M, Arnold LE, McCracken J, McDougle CJ, Tierney E, Chuang S, Vitiello B (2004) Weight and leptin changes among risperidone-treated youths with autism: 6-month prospective data. Am J Psychiatry 161:1125–1127
Calarge CA, Acion L, Kuperman S, Tansey M, Schlechte JA (2009) Weight gain and metabolic abnormalities during extended risperidone treatment in children and adolescents. J Child Adol Psychopharmacol 19:101–109
Merchan-Naranjo J, Tapia C, Bailón C, Moreno C, Baeza I, Calvo-Escalona R, Morer A, Martínez-Cantarero C, Nestares PA, Alda JÁ, Muñoz D, Arango C (2012) Secondary effects of antipsychotic treatment in naïve or quasi-naïve children and adolescents: design of a follow-up protocol and baseline results. Rev Psiquiatr Salud Ment 5:217–228
Andreasen NC, Pressler M, Nopoulos P, Miller D, Ho BC (2010) Antipsychotic dose equivalents and dose-years: a standardized method for comparing exposure to different drugs. Biol Psychiatry 67:255–262
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
Sobradillo B, Aguirre A, Aresti U, Bilbao C, Fernández-Ramos A, Lizarraga H, Lorenzo L, Madariaga I, Rica I, Ruiz E, Sánchez C Santamaría, Serrano JM, Zabala A, Zurimendi B, Hernández M (2004) Curvas y tablas de crecimiento: estudios longitudinal y transversal. Fundación Faustino Orbegozo Eizaguirre, Bilbao
Flodmark CE, Lissau I, Moreno LA, Pietrobelli A, Widhalm K (2004) New insights into the field of children and adolescents’ obesity: the European perspective. Int J Obes Relat Metab Disord 28:1189–1196
Arango C, Giráldez M, Merchán-Naranjo J, Baeza I, Castro-Fornieles J, Alda JA, Martínez-Cantarero C, Moreno C, de Andrés P, Cuerda C, de la Serna E, Correll CU, Fraguas D, Parellada M (2014) Second-generation antipsychotic use in children and adolescents; a 6-month prospective cohort study in drug-naïve patients. J Am Acad Child Adol Psychiatry 53:1179–1190
McIntyre RS, Jerrell JM (2008) Metabolic and cardiovascular adverse events associated with antipsychotic treatment in children and adolescents. Arch Pediatr Adolesc Med 162:929–935
Faraone SV, Biederman J, Morley CP, Spencer TJ (2008) Effect of stimulants on height and weight: a review of the literature. J Am Acad Child Adolesc Psychiatry 47:994–1009
Penzner JB, Dudas M, Saito E, Olshanskiy V, Parikh UH, Kapoor S, Chekuri R, Gadaleta D, Avedon J, Sheridan EM, Randell J, Malhotra AK, Kane JM, Correll CU (2009) Lack of effect of stimulant combination with second-generation antipsychotics on weight gain, metabolic changes, prolactin levels, and sedation in youth with clinically relevant aggression or oppositionality. J Child Adolesc Psychopharmacol. 19:563–573
Gentile S (2009) Contributing factors to weight gain during long-term treatment with second-generation antipsychotics. A systematic appraisal and clinical implications. Obes Rev 10:527–542
Gonzaga NC, Medeiros CC, de Carvalho DF, Alves JG (2014) Leptin and cardiometabolic risk factors in obese children and adolescents. J Paediatr Child Health 50:707–712
Poveda E, Callas NE, Baracaldo CM, Castillo C, Hernández P (2007) Leptin levels in school age children associated with antropometric measurements and lipid profiles. Biomedica 27:505–514
Venner AA, Lyon ME, Doyle-Baker PK (2006) Leptin: a potencial biomarker for childhood obesity? Clin. Biochem 39:1047–1056
Karavani G, Strich D, Edri S, Gillis D (2014) Increases in thyrotropin within the near-normal range are associated with increased triiodothyronine but not increased thyroxine in the pediatric age. J Clin Endocrinol Metab 99(8):E1471–5. doi:10.1210/jc.2014-1441 (Epub 2014 May 30)
Marras V, Casini MR, Pilia S, Carta D, Civolani P, Porcu M, Uccheddu AP, Loche S (2010) Thyroid function in obese children and adolescents. Horm Res Paediatr 73:193–197
Margari L, Matera E, Craig F, Petruzzelli MG, Palmieri VO, Pastore A, Margari F (2013) Tolerability and safety profile of risperidone in a sample of children and adolescents. Int Clin Psychopharmacol 28:177–183
Misiak B, Frydecka D, Laczmanski L, Slezak R, Kiejna A (2014) Effects of second-generation antipsychotics on selected markers of one-carbon metabolism and metabolic syndrome components in first-episode schizophrenia patients. Eur J Clin Pharmacol. doi:10.1007/s00228-014-1762-2
Nasrallah HA (2008) Atypical antipsychotic-induced metabolic side effects: insights from receptor-binding profiles. Mol Psychiatry. 13:27–35
Catli G, Anik A, Tuhan HÜ, Kume T, Bober E, Abaci A (2014) The relation of leptin and soluble leptin receptor levels with metabolic and clinical parameters in obese and healthy children. Peptides 56:72–76
Friedemann C, Heneghan C, Mahtani K, Thompson M, Perera R, Ward AM (2012) Cardiovascular disease risk in healthy children and its association with body mass index: systematic review and meta-analysis. BMJ 345:e4759. doi:10.1136/bmj.e4759
Ratzoni G, Gothelf D, Brand-Gothelf A, Reidman J, Kikinzon L, Gal G, Phillip M, Apter A, Weizman R (2002) Weight gain associated with olanzapine and risperidone in adolescent patients: a comparative prospective study. J Am Acad Child Adol Psychiatry 41:337–343
Acknowledgments
We would like to thank the Center for Biomedical Research in the Mental Health Network (CIBERSAM), Madrid (Spain); for partial funding, the following: the Spanish Ministry of Health, Instituto de Salud Carlos III ≪Health Research Fund≫ (F.I.S.-PI04/0455); Madrid Mental Health Association (≪Miguel Angel Martín≫ Research Grant); ≪NARSAD 2005: Independent Investigator Award≫; Alicia Koplowitz and Mutua Madrileña foundations; and the Ministries of Science and Innovation, Community of Madrid, Biomedical R&D funding S2010/BMD-2422 AGES (Madrid) for their support. FP7-HEALTH-F4-2010-241959 (Project PERS—Pediatric European Risperidone Studies). The authors thank Mr. A.D.Pierce for his English editorial assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
IB has received honoraria and travel support from Otsuka and Janssen, research support from Fundación Alicia Koplowitz and grants from the Spanish Ministry of Health, Instituto de Salud Carlos III. RCE has a grant from the Spanish Ministry of Health, Instituto de Salud Carlos III, and has received travel support from Shire. CA is a consultant for AstraZeneca, Bristol Myers Squibb, Janssen-Cilag, Pfizer and Servier; has received grants/support from the Spanish Ministry of Health, Instituto de Salud Carlos III, the European Comission, Fundación Alicia Koplowitz, Astra-Zeneca, Bristol Myers Squibb. JCF has been a consultant for Eli Lilly and has received grants from the Spanish Ministry of Health, Instituto de Salud Carlos III, the European Comission and Fundació La Marató de TV3. LV, ES, JMN and PRL declare no conflicts of interest.
Rights and permissions
About this article

Cite this article
Baeza, I., Vigo, L., de la Serna, E. et al. The effects of antipsychotics on weight gain, weight-related hormones and homocysteine in children and adolescents: a 1-year follow-up study. Eur Child Adolesc Psychiatry 26, 35–46 (2017). https://doi.org/10.1007/s00787-016-0866-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-016-0866-x