
Abstract
Child maltreatment (CM) is associated with poor long-term health outcomes. However, knowledge about CM prevalence and related consequences is scarce among adults in South European countries. We examined the self-reported prevalence of five different forms of CM in a community sample of 1,200 Portuguese adults; we compared the results with similar samples from three other countries, using the same instrument. We also explored the relationship between CM and psychological symptoms. Cross-sectional data using the Childhood Trauma Questionnaire-Short Form and the Brief Symptom Inventory were analyzed. Moderate or severe CM exposure was self-reported by 14.7 % of the sample, and 67 % was exposed to more than one form of CM. Emotional neglect was the most endorsed experience, with women reporting greater emotional abuse and men reporting larger physical abuse. Physical and sexual abuse was less self-reported by Portuguese than by American or German subjects. CM exposure predicted 12.8 % of the psychological distress. Emotional abuse was the strongest predictor for psychological symptoms, namely for paranoid ideation, depression, and interpersonal sensitivity. Emotional abuse overlapped with the exposure to all other CM forms, and interacted with physical abuse, physical neglect, and emotional neglect to predict psychological distress. Low exposure to emotional abuse was directly associated with the effects of physical abuse, physical neglect, and emotional neglect to predict adult psychological distress. Verbal abuse experiences were frequently reported and had the highest correlations with adult psychological distress. Our results underline the potential hurtful effects of child emotional abuse among Portuguese adults in the community. They also highlight the need to improve prevention and intervention actions to reduce exposure and consequences of CM, particularly emotional abuse.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Childhood maltreatment
The World Health Organization (WHO) considers child maltreatment (CM) as a public health priority within the scope of violence prevention [1]. Despite the measures taken by European countries to protect children from violence and child abuse, effective prevention still demands strong improvements [2].
CM includes serious negative early experiences with caregivers that may harm, potentially harm or threat the physical, social and/or mental development of the child [3]. CM includes several forms of mistreatment. Emotional abuse refers to a persistent pattern of emotional ill-treatment that results in significant adverse effects to the emotional development. Physical abuse implies the use of physical force that results in harm or has the potential to harm. Sexual abuse consists of any completed or attempted sexual contact of a caregiver with a child. Neglect (physical and/or emotional) is the failure to provide adequate care to fulfill the child’s basic needs, such as adequate nutrition, hygiene, shelter and safety, education, medical care, and emotional needs [3].
CM experiences are repetitive and prolonged in time, and except for sexual abuse, usually perpetrated by parents or caregivers. Overlapping exposure to different forms of CM is also frequent [4]. Estimated prevalence rates for CM in Europe are 22.9 % for physical abuse, 29.1 % for emotional abuse, 9.6 % for sexual abuse (13.4 % girls and 5.7 % boys), 16.3 % for physical neglect, and 18.4 % for emotional neglect [5]. Exposure to emotional abuse was found to be the most prevalent and challenging form of CM, appearing often with other CM forms [6]. Yet, emotional abuse of a child is difficult to target, requiring improvement in detection and intervention tools [7].
It has been stated that officially ascertained CM accounts for less than one-tenth of the occurred cases [3]. Self-reported and retrospective assessment methods have been considered less effective, since results can be distorted by memory degradation or by mood congruent responses. However, they are necessary tools to identify the broader spectrum of CM [8]. In addition, studies have confirmed that CM self-reported data are stable across time [9] and are also good predictors of adult psychopathology in comparison with prospectively or officially ascertained CM [10].
CM prevalence studies in European community populations are scarce and mainly focused on sexual or physical abuse [3]. Because of the large differences in prevalence rates, comparison across countries should use ideally the same instruments in similar population and analyze diverse psychosocial outcomes [11].
Childhood maltreatment consequences
Consequences such as increased risk for depression, suicide attempts, substance use, and sexual risk behaviors have been found in CM-exposed adults, with emotional abuse having the larger effects [12]. CM has been associated with poor long-term physical health outcomes [13, 14] and psychopathology [15], independently of the assessment method [10].
Several psychological symptoms were linked to CM exposure. Physical abuse was related to aggressive behavior, social inhibition, and delinquency [16], while sexual abuse has been associated with anxiety, depression, maladaptive sexual behaviors, and sleep disturbances [17]. Neglect was associated with anxiety, depression, somatization, paranoia, and hostility and was also a significant predictor for general psychological problems [18]. Emotional abuse has been considered as a predictor for later psychological problems and poor health outcomes [19, 20]. Symptoms such as negative self-evaluation, anxiety, interpersonal sensitivity, and depression have been consistently associated with emotional abuse [17]. It has been suggested that negative consequences of other maltreatment forms (such as sexual and physical abuse) might be related with an overlapped exposure to emotional abuse [21]. Teicher and colleagues [22] found that parent verbal aggression has moderate to large associations with dissociation, limbic irritability, depression, and anger hostility in healthy community adults. They also verified that emotional maltreatment has stronger associations with psychiatric sequelae than physical maltreatment. Adult insecure attachment styles and maladaptive cognitive schemas were found to be mediating factors between CM and psychiatric disorders [23, 24].
There is growing evidence showing that CM-related clinical conditions have specific therapeutic demands [25]. Therapeutic interventions have been developed for children, adolescent, and adults [26, 27]. Phase-oriented interventions including psycho-education and affect regulation are suggested as effective in reducing symptoms among CM-exposed subjects suffering from post-traumatic stress disorder [26, 27]. However, there is a paucity of knowledge about what can be done to prevent disturbances in CM-exposed subjects. Therefore, data on CM prevalence and associated impairment may inform public health services about the most harmful forms of CM and specific programs to foster resilience among CM-exposed adults.
A wide range of psychological problems have been identified in CM-exposed adults. As suggested by Belsky [28], CM exposure occurs in a context that will influence its potential consequences. In addition, CM forms may occur simultaneously, making it difficult to disentangle their independent consequences. Nevertheless, knowledge about CM prevalence and its psychological correlates among adults in the community is required to tailor preventive and intervention programs.
Portuguese context
In 2003, Portugal was one of the countries in the industrialized world with the worst levels of child protection because of the death rate of 3.7 from maltreatment and 17.8 from all injuries per 100,000 children [29]. Countries with similar cultures such as Spain (1/100,000), Italy or Greece (2/100,000) reported lower rates. Risk factors were identified in the Portuguese population, namely poverty and low education levels, comparing with other European countries [30]. Mental health disorders were also found in 23 % of the adult community population [31], while only 1.7 % was found looking for treatment [32].
Nevertheless, studies using the Childhood History Questionnaire (Milner 1990) concluded that Portugal registered lower rates for sexual abuse (2.6 vs 12.2 % for Spain, 10 % for the United States) and for physical abuse with injury (9.5 vs 15.2 % for Spain, 20.5 % for the United States) [33]. It was also found that 25.9 % of North Portuguese parents reported abusive behaviors toward their children (22.4 % emotionally and 12.3 % physically) [34].
Official CM prevalence rates for children are made available in Portugal by the agencies for youth protection (National Commission of Protection of Children and Youth at Risk). In 2012, 69,007 cases were followed, a number that represents about 2.3 % of the total number of children aged between 0 and 18 years. Exposure to neglect was detected in 30 %, physical abuse in 6.3 %, emotional abuse in 5.3 %, and sexual abuse in 2.2 % of the registered cases. Remaining cases were followed because of school dropouts, risk behaviors or abandonment of children [35]. However, these rates might underrepresent the true scale of the problem because of the clandestine nature of CM and the difficulties in detecting it. Thus, the extent of the problem can be better captured through the study of past CM reported by adults. To our knowledge, no data are available about CM rates and its potential consequences in adults from the community in Portugal.
Research goals
Considering the lack of CM studies within South European countries and bearing in mind the Portuguese social and economic context, we are in need of knowledge about CM prevalence and its potential consequences among community adults. Our study has three main goals: (1) to analyze the self-reported CM prevalence in a sample of Portuguese community adults, (2) to compare it with other countries using the same instrument, and (3) to study the relationship between CM and psychological symptoms in the Portuguese sample.
Method
Participants
A sample of 1,213 subjects, aged between 18 and 65 years, participated in the study. Data were collected between 2008 and 2010 within the larger project “Children of Colonial War: Post Memory and Representations”, developed at the Centre for Social Studies, Coimbra University, Portugal. Subjects were recruited using the snowball technique in three different parts of the country: Oporto University (17.75 %), Centre for Social Studies (36.25 %) and Santa Margarida Military Camp (46 %). Subjects agreed to participate after explanation about the research purposes exposed in the informed consent. Two inclusion criteria were considered: Portuguese nationality and 18 years or older. No data are available on no-response rates.
Sample demographics are detailed in Table 1. The proportion of men and women is equivalent to the Portuguese population (χ 21200,1 = 2,043, p = 0.1529). The sample differs from the Portuguese population in terms of age, education, marital status, and job status. The respondents are younger (χ 21200,3 = 118,427, p = 0.001; more subjects are aged between 18 and 24 years, and fewer subjects are older than 65 years), more frequently single (χ 21200,2 = 6,469, p = 0.0394), with more years of education (χ 21200,3 = 95,806, p = 0.001, with fewer subjects with 4 years or less of education and more subjects with higher education), and more employed (χ 21200,3 = 51,404, p = 0.0001, with fewer unemployed people, students, and pensioners). Portuguese community characteristics were obtained at the National Institute of Statistics [36].
Design and materials
This is a cross-sectional study using self-reported retrospective instruments. We used the Childhood Trauma Questionnaire-Short Form (CTQ-SF) [37] to assess CM exposure and the Brief Symptom Inventory (BSI) [38] to measure psychological symptoms and distress. In addition, the research protocol included the informed consent and a short interview with sociodemographic questions such as age, marital status, living area, and employment. Data collection was approved by the Ethical Commission of the Military Hospital of Coimbra and also by the Portuguese Commission for the Data Protection.
The Childhood Trauma Questionnaire-Short Form
The CTQ, developed by Bernstein and colleagues [37], is one of the most utilized CM assessment instruments across different cultures [39]. It is considered a gold standard instrument to assess self-reported CM because it is user-friendly and non-intrusive, assesses different forms of CM exposure and is sensitive to the severity of CM [40].
The CTQ-SF assesses five different forms of CM described by 25 items—emotional abuse, sexual abuse, physical abuse, emotional neglect, and physical neglect. Each subscale includes five items, classified into a 5-point Likert scale (1 = never true, 2 = rarely true, 3 = sometimes true, 4 = often true, 5 = very often true). CTQ-SF presented Cronbach’s alpha values varying between 0.61 for physical neglect and 0.95 for sexual abuse in clinical populations [37] and between 0.58 for physical neglect and 0.94 for sexual abuse [41] in community samples. Results on time stability, convergence, and discriminant validity were considered good [42]. The CTQ-SF psychometric properties were studied in Portuguese community subjects [43]. The original five-factor model for the instrument was confirmed in a sample of 746 subjects. Cronbach’s alpha varied between 0.47 for physical neglect, 0.71 for emotional abuse, 0.72 for sexual abuse, 0.78 for physical abuse, 0.79 for emotional neglect, and 0.84 for the overall scale. Time stability, discriminant, and convergent validity were also tested and considered acceptable.
Two different strategies were used to summarize the CTQ-SF results: CM endorsement, identified by item scores larger than 1, and moderate or severe CM exposure, classified by scores above moderate or severe in each subscale, accordingly with the cutoff points suggested by the CTQ authors [44]: emotional abuse ≥13, physical abuse ≥10, sexual abuse ≥8, emotional neglect ≥15, and physical neglect ≥10. For the overall CTQ-SF score, we used the value of the average summed to one standard deviation to identify subjects moderately or severely exposed to CM.
The brief symptom inventory
The BSI is a self-reported measure for psychological symptoms. It includes 53 items, grouped in nine clinical scales (somatization, obsession, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychosis) and three global indices that suggest a generic level of mental health suffering (global severity index, positive symptom total, and positive symptom index). Symptoms can be classified accordingly with the frequency they occur (never, rarely, sometimes, many times, and often). Global severity index (GSI) represents a measure of general psychological distress. Thus we used it as an overall score for psychological distress. Psychometric studies suggested good internal validity, with Cronbach’s alpha values varying between 0.71 and 0.85 and test–retest validity values ranging between 0.68 and 0.91 [38]. Psychometric properties of the BSI in the Portuguese population were examined in a sample of 404 subjects, including clinical and non-clinical population [45]. Reliability and construct validity were analyzed through the study of the internal consistency and correlations between items and scales, showing good results in both fields. Correlations between items and scales presented values between 0.29 and 0.78. Cronbach’s alpha values varied between 0.62 for psychosis and 0.80 for somatization. The BSI is generally considered an excellent tool to assess psychopathology [46].
Self-reported CM in different countries
To explore differences in CM prevalence among countries, we searched for studies analyzing similar samples and using the same assessment tool. Studies were found for the United States [41], The Netherlands [47], and Germany [48]. Data from USA were collected in the metropolitan area of Memphis through telephonic interviews. Subjects aged between 18 and 65 years were selected using a random digit dialing with balanced proportions of men and women. For the Netherlands, results were found for a non-clinical sample of adults, aged between 18 and 70 years. Subjects were recruited through personal contacts of researchers and by public advertisements. For Germany, data were collected in a representative sample of subjects aged between 14 and 90 years old. Data were obtained by personal visits to previous selected households. Sample size, mean age, and results of CTQ-SF subscales for the different countries are described in Table 4.
Statistical analysis
Data were analyzed using the SPSS (version 17) and Mplus (version 6.11). CM prevalence was analyzed through the study of the CTQ-SF score frequencies. T test was applied to compare male and female scores. ANOVA was used for the CTQ-SF subscale comparisons among countries. Spearman correlations were calculated to study the relationship between CM items and psychological distress. Effects of CM on psychological distress and symptoms were tested using simple and stepwise regression and path analyses.
Results
Data analyses
Data were inspected for missing values, outliers, multivariate normality, and multicollinearity. Of the 1,213 subjects who participated in the study, 13 were removed because they filled less than 90 % of the protocol, 1,044 completed all questions, and the remaining missing values were imputed with the average score for the corresponding variable in the overall group; there were no variables with more than 1 % of missing values. Outliers were detected using the Mahalanobis distance, which indicated the existence of 38 multivariate outliers; however, they were admitted as part of the sample considering that among community subjects the existence of a set of subjects with high CM exposure is expected [49].
Adult CM prevalence in the Portuguese sample
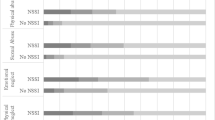
Figure 1 shows that 14.7 % of the sample reported moderate or severe CM exposure while 88.7 % self-reported some CM endorsement, as indicated in the Fig. 1a. About 11 % of subjects were not exposed to any CM experience and 67 % have been exposed to more than one form of CM (Fig. 1b). Items assessing positive experiences, which are scored with reversed rates, such as “There was someone in my family who helped me feel important or special” and “People in my family looked out for one another.” were the most self-reported. Looking into the group of items with direct scoring, 47.7 % of the sample self-reported insults by family members (“People in my family said hurtful things or insulting…”), which also has the highest correlation with GSI (r = 0.304 with p < 0.01). The items “I believe that I was emotionally abused” and “Family members called me things like ‘stupid’…” have also the highest significant correlations with the global severity index (r = 0.281 and r = 0.241, with p < 0.01). All CTQ-SF items are significantly correlated with distress, except two items of physical abuse (“I got hit so hard by someone in my family that I had to see a doctor or go to the hospital” and “I got hit or beaten so badly that it was noticed by someone like a teacher…”). For a detailed view of the results, see Table 2.

Percentage of subjects: a Reporting any CM experience/endorsement (gray) and moderate or severe CM exposure (black); b reporting exposure to different amounts of CM forms (from not exposed until exposed to all assessed forms)
Emotional neglect and emotional abuse were the most self-reported CM experiences, while sexual abuse was the least one (Table 3). Spearman correlations between CTQ-SF subscales were all statistically significant, varying between 0.494 for emotional neglect and physical neglect, and 0.133 for sexual abuse and physical abuse/physical neglect. The larger correlations were found between emotional neglect and physical neglect, emotional abuse and emotional neglect (r = 0.479), and between physical abuse and emotional abuse (r = 0.356). About 52 % of subjects were exposed to emotional neglect and cumulatively to emotional abuse. Exposure to emotional abuse also overlapped with exposure to physical abuse, sexual abuse, and physical neglect (Fig. 2). Significant differences between men and women were found for emotional and physical abuse: women self-reported more emotional abuse (t = 4.266 with p < 0.000) and men self-reported greater physical abuse (t = −2.537 with p < 0.011).

Venn diagram for percentages of overlapped exposure with emotional abuse. EA Emotional abuse, EN emotional neglect, PA physical abuse, PN physical neglect, SA sexual abuse. a 52.1 % (EA, EN); b 29.8 % (EA, PN); c 29 % (EA, PN, EN); d 20.3 % (EN, PN); e 17.5 % (EA, PA); f 17.1 % (EA, PA, EN); g 6.7 % (EA, SA, PN); h 5.2 % (PN, SA)
Comparison of self-reported CM among countries
Comparing the results among countries, lower sexual and physical abuse was reported in Portugal than in the USA or Germany. However, Portugal and USA registered the largest scores for emotional abuse. No significant differences were found between Portugal and the Netherlands for emotional, sexual, and physical abuse as well as emotional neglect. Portugal and the Netherlands only differed in physical neglect, with Portuguese subjects self-reporting less physical neglect than Dutch. Accordingly with the CTQ-SF results, German subjects scored higher for emotional and physical neglect, comparing with Portuguese, Dutch, and American subjects. For emotional neglect, Portuguese and Dutch scored higher than American but lower than German subjects. For physical neglect, Portuguese subjects scored lower than German and higher than Dutch and American subjects. Table 4 shows detailed results for the four above-mentioned countries.
Relations between CM and psychological symptoms
Spearman correlations between CM forms and psychological symptoms were all statistically significant, varying between 0.348 for emotional abuse and paranoid ideation, and 0.074 for sexual abuse and obsession. Correlations were larger between emotional abuse and psychological symptoms than for other forms of CM.
A stepwise multiple regression was conducted to identify the best group of CM predictors for psychological suffering (GSI). At step one, GSI was predicted by emotional abuse, explaining 11.3 % of variance [F (1,1198) = 152.10, p ≤ 0.000]. At step 2, physical neglect was included in the model, with a contribution of 0.9 % of explained variance [R 2 change = 0.009; F (1,1197) = 12.854, p ≤ 0.000]. At step three, sexual abuse contributed with 4 % of explained variance [R 2 change = 0.004, F (1,1196) = 4.953, p ≤ 0.026]. Together, emotional abuse, physical neglect, and sexual abuse explained 12.6 % of psychological distress [F (3, 1196) = 57.323, p ≤ 0.000]. Interaction effects between emotional abuse and other CM forms were studied using regression analysis of centered values for CM forms and its cross products. Significant interactions were found for physical neglect (t = −3.187, p ≤ 0.001, β = −0.099), physical abuse (t = −3.232, p ≤ 0.001, β = −0.129), and emotional neglect (t = −3.064, p ≤ 0.002, β = −0.110), but not for sexual abuse (t = −0.588, p ≤ 0.557). Scatter plots were produced to study the interaction effects in two levels of emotional abuse: low exposure (sum for subscale item scores ≤13) and moderate or severe exposure (sum for subscale item scores >13). Different patterns of relation were found: for low exposure to emotional abuse, the effects of emotional neglect, physical neglect, and physical abuse were directly related with adult psychological distress; for moderate or severe exposure, an inverse relation was found between the severity of these CM forms and psychological distress, as it is shown in Fig. 3.

Scatter plots of psychological distress (Y) and child maltreatment subtypes (X) including regression lines for low (solid line) and moderate/severe (dashed line) emotional abuse. Significant interactions were found for physical abuse, physical neglect and emotional neglect with emotional abuse. Low emotional abuse exposure was found to mediate the effects of physical abuse, physical neglect and emotional neglect on psychological distress, while moderate or severe emotional abuse moderated these relations. *Centered variables
Regression analysis indicated that 12.8 % of psychological distress (measured by the GSI of the BSI) was predicted by CM exposure (p < 0.000) (Table 5). Emotional abuse, physical neglect, and sexual abuse were significant predictors, with emotional abuse having the larger standardized regression weight (β = 0.324, with p < 0.000). Despite sexual abuse being found a significant predictor for psychological distress (GSI), it had a small regression weight (β = 0.061 with p < 0.028).
We confirmed that all psychological symptoms were predicted by CM exposure through path analysis, as shown in Table 5. Effect sizes varied between 0.14 for paranoid ideation and 0.058 for phobia, with p ≤ 0.000). The largest effect sizes were found for paranoid ideation, depression, interpersonal sensitivity, and psychosis. Emotional abuse significantly predicted all of the assessed psychological symptoms, with regression weights varying between 0.353 for paranoid ideation and 0.183 for phobic anxiety (with p ≤ 0.000). Excluding for psychosis, physical neglect was also a significant predictor, but with smaller regression weights (varying between 0.155 for somatization, p < 0.000, and 0.065 for psychosis, p < 0.046). Physical neglect effects were higher for somatization (β = 0.155), anxiety (β = 0.141), and phobic anxiety (β = 0.141). Although the regression weights for sexual abuse were lower than for emotional abuse and physical neglect, they were significant for depression, anxiety, paranoid ideation, psychosis, and phobic anxiety. Emotional neglect and physical abuse were no significant predictors. For a detailed view of results, see Table 5.
Discussion
CM prevalence in Portuguese adults
Our study analyzed the self-reported prevalence of CM in a community sample of Portuguese adults. Approximately 14.7 % reported moderate or severe CM exposure, while 67 % have been exposed to more than one CM form. Emotional neglect was the most endorsed CM form, but emotional abuse was also highly reported and showed the largest correlations with psychological symptoms. Exposure to emotional abuse occurred mainly together with emotional neglect, but also with physical neglect, sexual abuse, and physical abuse. These results are in line with previous studies stating that exposure to diverse CM forms occurs commonly together [4], and that emotional abuse frequently overlaps other CM forms [21]. They also underline the need to develop screening and intervention tools addressing simultaneously various CM forms, and integrating specific actions for the detection and management of emotional abuse.
Officially ascertained CM prevalence by the Portuguese agencies for children protection is considerably lower (2.3 %) compared with the rates in our sample of adults. Although prevalence differences might be explained by the use of different CM definitions and the comparison of different population cohorts (children versus adults), this finding is in line with the one reported by Gilbert and colleagues [3] about the high rates of unreported cases by agencies for children protection. Thus, plans for prevention and intervention need to consider additional information sources about CM detection, its prevalence and its effects, beyond the one provided by the agencies for children protection.
Comparison among countries
CM self-reported exposure among Portuguese community adults, as assessed by the CTQ-SF, was compared with findings from three other countries: USA, The Netherlands and Germany. We found that the prevalence for sexual and physical abuse in Portugal was lower than in the USA and Germany. These results confirm the previous findings of Figueiredo and colleagues [33], stating that Portugal has less incidence of physical and sexual abuse, when compared with USA and Spain. However, these results are incongruent with the UNICEF study that classified Portugal as one of the countries with worst levels of children protection. The low adult self-reported rates for physical abuse might be due to the social acceptance of physical punishment among Portuguese subjects. Adults often regard physical punishment as a needed resource to educate, thus not considering it as a CM experience [34]. Another reason may lie in the strong influence that Catholicism had in the Portuguese society. The Catholic Church used the physical punishment to control misbehavior, and has forbidden the disclosure of sexual themes. Those historical roots may still distort the individual meaning of past experiences of sexual or physical abuse, specifically in communities with low education levels.
Other CM prevalence differences were found among compared countries. Portugal and USA had higher rates for emotional abuse, comparing with Germany. On the other hand, Germany had higher scores for physical and emotional neglect. It is likely that these differences are due to the mean age of the samples: the German sample is older than the American or the Portuguese. Young adults might have lived with better life conditions, and were probably more protected against neglect. However, such differences may also be due to specific cultural characteristics.
Relations between CM and psychological symptoms
Childhood maltreatment exposure appeared to be significantly linked to psychological symptoms in the analyzed sample, as suggested by previous studies. We found that 12.8 % of psychological distress was explained by CM exposure. With regard to the prediction of psychological symptoms, the larger effect sizes were found for paranoid ideation, depression, interpersonal sensitivity, and psychosis, with values ranging between 0.14 and 0.10. The best set of predictors included emotional abuse, physical neglect, and sexual abuse, with emotional abuse having the strongest effect size, as we discuss further. Although these effect sizes are small according to Cohen’s classification [49], our results are important from a public health standpoint, since Portugal is registering a high prevalence of mental health disorders. Considering the multiple causes of psychological distress, such as genetic predisposition and exposure to relevant life events, the obtained effect sizes are meaningful, as we analyzed a community sample and not at-risk groups.
Emotional neglect did not predict psychological symptoms in our sample, only physical neglect. These results are different from the ones obtained by Gauthier and colleagues [18]. Emotional and physical neglect exposure during infancy can have different outcomes in adult functioning; thus, its consequences should be analyzed separately. Physical abuse was not found to be a significant predictor for psychological symptoms, results that are in line with Teicher’s and colleagues findings.
Physical neglect was a predictor for somatization, anxiety, and phobic anxiety. However, because of the low internal consistency of this subscale, these results need replication. Furthermore, sexual abuse was found to be a modest predictor for psychological symptoms, having the larger effect sizes for depression and anxiety.
Emotional abuse predicted all psychological symptoms, with larger effect sizes for interpersonal sensitivity, paranoid ideation, and depression. This finding confirms Teicher’s and colleagues’ standpoint [50] about the effects of emotional abuse in the development of adult psychiatric sequelae [22]. Emotional abuse is a potential risk factor for psychopathology among Portuguese community subjects, and it appears to be the most harmful CM form. It may disturb the development of cognitive structures for social interaction, providing a ground for the occurrence of symptoms having interpersonal components [23, 24].
Significant interaction effects with emotional abuse were found for physical abuse, emotional and physical neglect, confirming previous findings by Briére and Runtz [17]. However, the interactions we found had divergent patterns: when there is a low exposure to emotional abuse, an increase in physical abuse, emotional neglect, and physical neglect directly increased psychological distress. Yet, for moderate or severe levels of emotional abuse, an increase on physical abuse, emotional neglect, and physical neglect is accompanied by a decrease of psychological distress. These results highlight the hurtful potential of low levels of emotional abuse when they are accompanied by exposure to other CM forms. Nevertheless, for moderate or severe emotional abuse exposure, other variables might have to be accounted to explain the obtained results. Subjects exposed to moderate or severe emotional abuse and simultaneously to other moderate or severe CM forms have a higher likelihood to being identified during their infancy. Marks of physical abuse and physical neglect are often more easy to detect by official agencies of children protection or by relatives and friends. Thus, this group of subjects might have had opportunities to stop CM exposure and restore their levels of functioning in a way to prevent adult psychological distress. But for emotional neglect, which is often an invisible CM form like emotional abuse, these mechanisms may not apply.
Considering the harmful potential of CM, public health interventions to prevent exposure in children and reduce potential consequences in adults should be reinforced. Although particularly child emotional abuse is difficult to identify, its potential hurtful effects make it a priority target in the scope of child maltreatment. Child and adolescent mental health services may have an important role to inform how to recognize early signs of child emotional abuse and how to prevent it. Glaser suggested that the combination of emotional abuse and neglect occurs when there are “persistent, non-physical, harmful interactions with the child by the caregiver, which include both commission and omission”, (p. 4). This author underlined that children’s needs must be accounted for, instead of solely consider the caregiver–child interactions. According to this perspective, the risk for emotional abuse and neglect may be detected in four layers: the social environment, caregiver risk factors, caregiver–child interactions and child functioning. Intervention opportunities are placed not only in the family, but also in the community, integrating knowledge about risk and protective factors for both caregivers and children. Such a framework (FRAMEA) might enlarge prevention possibilities for emotional abuse exposure and offer suitable interventions for at-risk children. Yet, whenever prevention and intervention actions fail during childhood, public health care systems may need to develop specific measures focused on adults to reduce the impact of CM on poor long-term physical and mental health.
Limitations and strengths
Our study aimed to explore the prevalence and potential consequences of CM among adults from a Portuguese community sample. Although we analyzed a large sample, it was not randomly selected and it was merely representative in terms of gender. The use of self-reported and retrospective CM assessment, the lack of control of variables such as socioeconomic status, and the cross-sectional assessment of psychological distress are characteristics that may reduce the ability to generalize our results. In addition, the recall of experiences of child abuse and neglect by disturbed adults might be less accurate. However, using self-reported methods may add information about the not-officially ascertained CM cases, namely those that were never disclosed because of social desirability or shame. Nevertheless, we recognize the importance of prospective studies and multiple information sources to assess CM and its related consequences.
The comparison of adult self-reported CM among countries is important, since it may elucidate about the efficacy of different prevention plans that are being implemented. Countries may learn from each other strategies to reduce the scope of CM. However, the differences in age and sociodemographic characteristics of samples we compared, and the different methods for data collection may also explain some of the founded variations.
Despite some of the aforementioned artifacts, our study adds knowledge about the impact of CM exposure in Portuguese adult community subjects and estimates adult CM prevalence rates, using a well-known and robust instrument. It also provides prevalence data on five CM forms and reveals information on the association between CM experiences and psychological distress among Portuguese adults. Moreover, it confirms the hypothesis that CM exposure is a risk factor for mental illness among community adults, identifying emotional abuse as the CM form with the largest associated harmful potential, in terms of psychological symptoms.
Future research should investigate the degrees of emotional abuse and/or verbal abuse that trigger clinical levels of psychological distress and psychopathology in both male and female subjects, as well as resilience factors among CM-exposed subjects. Longitudinal studies analyzing the independent and combined effects of emotional abuse will allow a better understanding of its hurtful potential. More information is also required about the cumulative effects of CM exposure with regard to different psychological symptoms, and about the effects of chronic versus occasional CM exposure among Portuguese subjects.
Conclusions
Moderate or severe levels of childhood maltreatment exposure were self-reported by 14.7 % of adults from a Portuguese community sample; 67 % of the sample identified exposure to more than one CM form. Estimated CM prevalence in adults was far beyond the one estimated by agencies for children and youth protection. Physical abuse and sexual abuse were less self-reported in Portugal than in other countries like United States or Germany, probably because of cultural specificities. Despite emotional neglect being the most self-reported form of child maltreatment, emotional abuse was found to be a significant predictor for psychological symptoms, with greater effect sizes for paranoid ideation, depression, interpersonal sensitivity and psychosis. Emotional abuse overlapped with exposure to other CM forms and significantly interacted with physical abuse, physical neglect and emotional neglect to predict the severity of adult psychological distress. Remarkably, low exposure to emotional abuse increased the effects of other forms of child maltreatment to predict adult psychological distress, which emphasizes its hurtful potential. Experiencing verbal abuse during childhood was frequently self-reported and it was significantly correlated with adult psychological distress. Based on our results and bearing in mind the previous studies, practical implications may be drawn: preventive actions to reduce emotional abuse during childhood are required; CM screening and intervention in children should target the emotional abuse additionally to other CM forms; adult community subjects may need specific public health interventions to mitigate childhood emotional abuse consequences.
References
Krug E, Dahlberg L, Mercy JA et al (2002) World Report on Violence and Health. 346
Puras D (2011) Protection of children in European countries: analysis of the concluding observations of the UN Committee on the Rights of the Child. Eur Child Adolesc Psychiatry 20:S42–S43. doi:10.1007/s00787-011-0181-5
Gilbert R, Widom CS, Browne K et al (2009) Burden and consequences of child maltreatment in high-income countries. Lancet 373:68–81
Chiu RG, Lutfey KE, Litman HJ et al (2013) Prevalence and overlap of childhood and adult physical, sexual, and emotional abuse: a descriptive analysis of results from the Boston Area Community Health (BACH) Survey. Violence Vict 28:381–402
Sethi D, Bellis M, Hughes K et al (2013) European report on preventing child maltreatment. 116
Hibbard R, Barlow J, MacMillan H, The Committee on Child Abuse and Neglect and AMERICAN ACADEMY OF CHILD AND ADOLESCENT PSYCHIATRY CM and VC (2012) Psychological Maltreatment. Pediatr 130:372–378. doi:10.1542/peds.2012-1552
Glaser D (2011) How to deal with emotional abuse and neglect: further development of a conceptual framework (FRAMEA). Child Abuse Negl 35:866–875. doi:10.1016/j.chiabu.2011.08.002
Brewin CR, Andrews B, Gotlib IH (1993) Psychopathology and early experience: a reappraisal of retrospective reports. Psychol Bull 113:82–98
Pereira da Silva SS, da Costa Maia  (2013) The stability of self-reported adverse experiences in childhood: a longitudinal study on obesity. J Interpers Violence 28:1989–2004. doi:10.1177/0886260512471077
Scott KM, McLaughlin KA, Smith DAR, Ellis PM (2012) Childhood maltreatment and DSM-IV adult mental disorders: comparison of prospective and retrospective findings. Br J Psychiatry 200:469–475. doi:10.1192/bjp.bp.111.103267
Briere J, Jordan CE (2009) Childhood maltreatment, intervening variables, and adult psychological difficulties in women: an overview. Trauma Violence Abus 10:375–388. doi:10.1177/1524838009339757
Norman RE, Byambaa M, De R et al (2012) The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med 9:e1001349. doi:10.1371/journal.pmed.1001349
Springer KW, Sheridan J, Kuo D, Carnes M (2007) Long-term physical and mental health consequences of childhood physical abuse: results from a large population-based sample of men and women. Child Abus Negl 31:517–530
Wegman HL, Stetler C (2009) A meta-analytic review of the effects of childhood abuse on medical outcomes in adulthood. Psychosom Med 71:805–812
MacMillan HL, Fleming JE, Streiner DL et al (2001) Childhood abuse and lifetime psychopathology in a community sample. Am J Psychiatry 158:1878–1883
Kaplan SJ, Pelcovitz D, Labruna V (1999) Child and adolescent abuse and neglect research: a review of the past 10 years. Part I: physical and emotional abuse and neglect. J Am Acad Child Adolesc Psychiatry 38:1214–1222. doi:10.1097/00004583-199910000-00009
Briere J, Runtz M (1990) Differential adult symptomatology associated with three types of child abuse histories. Child Abus Negl 14:357–364
Gauthier L, Stollak G, Messé L, Aronoff J (1996) Recall of childhood neglect and physical abuse as differential predictors of current psychological functioning. Child Abuse Negl 20:549–559. doi:10.1016/0145-2134(96)00043-9
Irving SM, Ferraro KF (2006) Reports of abusive experiences during childhood and adult health ratings: personal control as a pathway?. J Aging Heal 18:458–485. doi:10.1177/0898264305280994
Spertus IL, Yehuda R, Wong CM et al (2003) Childhood emotional abuse and neglect as predictors of psychological and physical symptoms in women presenting to a primary care practice. Child Abus Negl 27:1247–1258
Riggs SA, Kaminski P (2010) Childhood emotional abuse, adult attachment, and depression as predictors of relational adjustment and psychological aggression. J Aggress Maltreat Trauma 19:75–104. doi:10.1080/10926770903475976
Teicher MH, Samson JA, Polcari A, McGreenery CE (2006) Sticks, stones, and hurtful words: relative effects of various forms of childhood maltreatment. Am J Psychiatry 163:993–1000
Bifulco A, Kwon J, Jacobs C et al (2006) Adult attachment style as mediator between childhood neglect/abuse and adult depression and anxiety. Soc Psychiatry Psychiatr Epidemiol 41:796–805. doi:10.1007/s00127-006-0101-z
Wright MO, Crawford E, Del Castillo D (2009) Childhood emotional maltreatment and later psychological distress among college students: The mediating role of maladaptive schemas. Child Abuse Negl 33:59–68. doi:10.1016/j.chiabu.2008.12.007
Teicher MH, Samson JA (2013) Childhood maltreatment and psychopathology: a case for ecophenotypic variants as clinically and neurobiologically distinct subtypes. Am J Psychiatry 170:1114–1133
Leenarts LW, Diehle J, Doreleijers TH et al (2013) Evidence-based treatments for children with trauma-related psychopathology as a result of childhood maltreatment: a systematic review. Eur Child Adolesc Psychiatry 22:269–283. doi:10.1007/s00787-012-0367-5
Dorrepaal E, Thomaes K, Smit JH et al (2010) Stabilizing group treatment for complex posttraumatic stress disorder related to childhood abuse based on psycho-education and cognitive behavioral therapy: a pilot study. Child Abuse Negl 34:284–288. doi:10.1016/j.chiabu.2009.07.003
Belsky J (1980) Child maltreatment: an ecological integration. Am Psychol 35:320–335
Unicef (2003) A league table of child maltreatment in rich nations. 36
Eurostat (2010) Europe in figures—Eurostat yearbook. 650
Paulo I (2010) Portugal é o país da Europa com mais doentes mentais. [Portugal is the European country with the highest rates of mental health problems]. Expresso
Caldas de Almeida JM (2009) Portuguese National Mental Health Plan (2007–2016) Executive Summary. Ment Health Fam Med 6:233–244
Figueiredo B, Bifulco A, Paiva C et al (2004) History of childhood abuse in Portuguese parents. Child Abus Negl 28:669–682
Machado C, Gonçalves M, Matos M, Dias AR (2007) Child and partner abuse: self-reported prevalence and attitudes in the north of Portugal. Child Abus Negl 31:657–670
Comissão Nacional de Protecção de Crianças e Jovens em Risco (2012) Relatório Anual de Avaliação da Atividade das Comissões de Proteção de Crianças e Jovens [Annual report of activities assessment of the Comissions for children and youth protection]. 184
Instituto Nacional de Estatistica (2011) Recenseamento da População Portuguesa—2011 (Census of the Portuguese Population). http://censos.ine.pt/xportal/xmain?xpid=CENSOS&xpgid=censos2011_apresentacao. Accessed 25 Mar 2014
Bernstein DP, Stein JA, Newcomb MD et al (2003) Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abus Negl 27:169–190
Derogatis LR, Melisaratos N (1983) The brief symptom inventory: an introductory report. Psychol Med 13:595–605
Baker AJL, Maiorino E (2010) Assessments of emotional abuse and neglect with the CTQ: issues and estimates. Child Youth Serv Rev 32:740–748. doi:10.1016/j.childyouth.2010.01.011
Hernandez A, Gallardo-Pujol D, Pereda N et al (2012) Initial validation of the spanish childhood trauma questionnaire-short form: factor structure, reliability and association with parenting. J Interpers Violence. doi:10.1177/0886260512468240
Scher CD, Stein MB, Asmundson GJ et al (2001) The childhood trauma questionnaire in a community sample: psychometric properties and normative data. J Trauma Stress 14:843–857
Roy CA, Perry JC (2004) Instruments for the assessment of childhood trauma in adults. J Nerv Ment Dis 192:343–351
Dias A, Sales L, Carvalho A et al (2013) Estudo de propriedades psicométricas do Questionário de Trauma de Infância—Versão breve numa amostra portuguesa não clínica (Study of psychometric properties of the Childhood Trauma Questionnaire-Short Version in a Portuguese community sample). Laboratório Psicol 11:103–120
Bernstein DP, Ahluvalia T, Pogge D, Handelsman L (1997) Validity of the Childhood Trauma Questionnaire in an adolescent psychiatric population. J Am Acad Child Adolesc Psychiatry 36:340–348
Canavarro MC (1999) Inventário de Sintomas Psicopatológicos—BSI. In: Simões MR, Gonçalves M, Almeida LS (eds) SHO-Apport, Braga, pp 87–109
De Beurs E, Zitman FG (2006) De Brief Symptom Inventory (BSI): De betrouwbaarheid en validiteit van een handzaam alternatief voor de SCL-90. Maandbl. Geestelijke Volksgezond. 61
Thombs BD, Bernstein DP, Lobbestael J, Arntz A (2009) A validation study of the Dutch Childhood Trauma Questionnaire-Short Form: factor structure, reliability, and known-groups validity. Child Abus Negl 33:518–523
Klinitzke G, Romppel M, Hauser W et al (2012) The German Version of the Childhood Trauma Questionnaire (CTQ): psychometric characteristics in a representative sample of the general population. Psychother Psychosom Med Psychol 62:47–51. doi:10.1055/s-0031-1295495
Tabachnick BG, Fidell LS (2007) Using multivariate statistics, 5th edn. p 980
Teicher MH, Samson JA, Sheu Y-S et al (2010) Hurtful words: association of exposure to peer verbal abuse with elevated psychiatric symptom scores and corpus callosum abnormalities. Am J Psychiatry 167:1464–1471
Acknowledgments
This research was financed by the Fundação para a Ciência e Tecnologia, Portugal through the Research Grant of Aida Dias, with reference SFRH/BD/68995/2010 (POSI 2010 and FSE). Data were collected within the project “Children of Colonial War: post memory and representations”, financed by the same organization, and with reference PTDC/ELT/65592/2006 FCOMP-01-0124-FEDER-007261. We would like to thank the Faculty of Social Sciences of Utrecht University for its hosting conditions; David Bernstein and Maria Cristina Canavarro by the permission to use the instruments; Margarida Calafate Ribeiro by the consent to use the data collected within the Project “Children of Colonial War: post memory and representations”.
Conflict of interest
There are no conflicts of interest in this work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dias, A., Sales, L., Hessen, D.J. et al. Child maltreatment and psychological symptoms in a Portuguese adult community sample: the harmful effects of emotional abuse. Eur Child Adolesc Psychiatry 24, 767–778 (2015). https://doi.org/10.1007/s00787-014-0621-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-014-0621-0