
Abstract
Although fluoxetine is useful in the treatment of major depression, 30–40 % of the patients do not respond to therapy. The response seems to be influenced by certain genes which are involved in the drug’s pharmacodynamics and pharmacokinetics. The present study reviews the literature on genetic contributions to fluoxetine response in children and adults, and concludes that the different polymorphisms of CYP2D6 and CYP2C9 may influence the blood concentrations of fluoxetine. If the childhood dose is adjusted for weight, differences between children and adults are unlikely. As regards the genes that influence the drug’s pharmacodynamics, polymorphisms of SLC6A4, HTR1A and MAO-A seem to be involved in the response to fluoxetine, while the genes COMT, CRHR1, PDEA1, PDEA11 GSK3B and serpin-1 also seem to play a role. Comparison of different studies reveals that the results are not always consistent, probably due to methodological differences. Other factors such as gender or ethnicity may also influence treatment response.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In most countries, fluoxetine was the first selective serotonin reuptake inhibitor (SSRI) to become available for clinical use [1]. It is currently the only SSRI approved by the European Medicines Agency for the treatment of major depression in children above the age of eight, and in whom psychological treatment has not been effective [2]. Although SSRIs are the first-line treatment for major depression, 30–40 % of the patients do not show a significant response [3]. Differences in fluoxetine response may be influenced by certain genes that are involved in the drug’s pharmacokinetics and pharmacodynamics. Most pharmacogenetic studies have focused on investigating genes related to pharmacokinetics [4]. In psychiatry the focus has been placed on cytochrome p450 and its isoforms, since cytochrome P450 is the principal enzyme involved in antidepressant metabolism [5]. Fluoxetine is a racemic mixture of two equally potent enantiomers, (S)- and (R)-fluoxetine [6]. The difference between the enantiomers is that their metabolite, called norfluoxetine, has two enantiomers of different potency ((S)- and (R)-norfluoxetine). (S)-norfluoxetine is twenty times more potent in blocking serotonin reuptake than the (R)- form [1, 7–9].
Numerous studies indicate that cytochrome P450 (particularly the CYP2D6 isoenzyme) is involved in the N-demethylation of fluoxetine to norfluoxetine, while the enzymes CYP2C9, CYP2C19 and CYP3A4 also play a role [7, 9–11]. It has been postulated that the large inter-individual variation in fluoxetine blood concentrations could be due to differences in CYP2D6 and CYP2C9 activity [11, 12]. The present study reviews the literature on the genetic polymorphisms of CYP2D6 and CYP2C9, which may contribute to inter-individual variations in fluoxetine response.
Genetic factors affecting the pharmacodynamics of fluoxetine also influence the response to the drug. Pharmacodynamics is the study of the biochemical and physiological effects of drugs on the body and the mechanisms of drug action [4]. Fluoxetine specifically inhibits neuronal re-uptake of serotonin, thus increasing the concentration of serotonin at the synapse and reinforcing serotonergic neuronal transmission. Therefore, genes associated with serotonin transport, synthesis, modulation and degradation, as well as others that will be mentioned in the results section, have been proposed as pharmacogenetic targets. Fluoxetine also has slight effects on other neurotransmitters that have been proposed as pharmacogenetic targets.
With respect to the pediatric population, studies of the pharmacogenetics of fluoxetine are scarce. The current pharmacokinetic data on fluoxetine in children are similar to those published in adults [13]. Most studies of the pharmacodynamics of antidepressants have been performed in adults. In children, we found one study of serotonin transporters and citalopram [2], and two studies of genes associated with serotonin synthesis and degradation [2, 14].
This study reviews the literature on genetic contributions to the pharmacodynamics and pharmacokinetics of fluoxetine in adults and children. The aim of research in this field is to discover new therapeutic targets and to develop personalized treatments.
Method
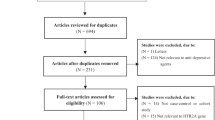
A literature search was conducted in the PubMed database (http://www.pubmed.gov) using the search terms “Fluoxetine pharmacogenetics”, “Fluoxetine pharmacokinetics”, “Fluoxetine pharmacodynamics”, “CYP2D6”, “CYP2C9”, “CYP219”, “serotonin transporter”, “serotonin receptors”, “serotonin synthesis”, “serotonin degradation”, and “other genes related to fluoxetine pharmacodynamics”. All the publications available up to July 2011 were included. The data obtained were used to identify the genes involved in fluoxetine response.
Results
Pharmacokinetics
Adults
After oral administration, fluoxetine is almost completely absorbed. Due to first-pass hepatic metabolism, oral bioavailability is below 90 %, after which the drug is distributed. Fluoxetine is the SSRI with the greatest distribution volume. Its excretion is mainly renal [1, 6] and it has a long half-life (t1/2) of 2–4 days. For norfluoxetine the t1/2 ranges from 7 to 15 days. Because of the long t1/2 the cytochrome inhibitory effect remains for weeks after treatment discontinuation [9]. Fluoxetine exhibits nonlinear kinetics, indicated by a disproportionate increase in its blood concentration after dose escalation. Blood concentration is not related to adverse effects or clinical improvement [1, 6, 15].
CYP2D6
The CYP2D6 gene has been mapped to chromosome 22 (at position 22q13.1) [10, 16]. To date, 74 allelic variants and a series of sub-variants of the CYP2D6 gene have been reported, and the number of alleles is still growing [16, 17]. They comprise are fully functional alleles, alleles with reduced function and null (non-functional) alleles whose enzyme activity ranges from zero to ultrarapid metabolism. Consequently, the application of standard doses may lead to adverse effects, or alternatively may have no effect at all. Phenotypically, patients are classified as ultrarapid metabolizers (UMs), extensive metabolizers (EMs), intermediate metabolizers (IMs) and poor metabolizers (PMs) [8, 10, 16–18]. The percentages of each phenotype in the Caucasian population are summarized in Table 1 [11, 16, 17, 19, 20]. PMs may present a prolonged therapeutic effect or drug-related toxicity after normal doses, reflecting a genetic predisposition to drug-induced effect. By contrast, UMs may not achieve therapeutic levels of the drug given at standard dose, so their main problem is a lack of treatment response [8, 10, 21]. Under steady-state conditions the contribution of CYP2D6 is diminished due to saturation and inhibition by both fluoxetine and norfluoxetine, and the difference between EMs and PMs is reduced [11]. It is suggested that the initial dose of CYP2D6 for PMs may be 50–70 % and for EMs 110–120 % of the average dose [19, 22]. Poor metabolizers are uncommon in the Asian population (1–2 %), whereas UMs are commonly found among Ethiopians and North Africans (16–29 %). There are also differences in (S)- and (R)-fluoxetine clearance. The distribution of different mutated alleles varies according to the ethnic group [10, 11, 16, 18]. Table 1 summarizes the mutated alleles found in the Caucasian population.
Fluoxetine and norfluoxetine are potent CYP2D6 inhibitors [8, 15]. In one fluoxetine study conducted in a population of 78 Caucasian patients, no differences were found between different CYP2D6 phenotypes (UM, EM, IM, PM) in relation to either the dose-normalized plasma concentrations of any of the enantiomers or the active moiety (which means, for example, the sum of (S)-fluoxetine, (R)-fluoxetine and (S)-norfluoxetine). However, the authors reported that the plasma concentration of (S)-norfluoxetine was very low in PMs, and that the (S)-norfluoxetine/(R)-norfluoxetine ratio was higher in homozygous than in heterozygous EM patients (P < 0.05). These results suggest that CYP2D6 polymorphisms may contribute to inter-individual variability in fluoxetine pharmacokinetics at the steady state. One limitation of this study was that only one PM patient was included [11].
A study by Llerena et al. [12] of 64 Caucasian patients obtained different results regarding the relationship between CYP2D6 polymorphisms and plasma concentrations of fluoxetine. The authors showed that dose-corrected plasma concentrations of fluoxetine were related to the number of active genes of CYP2D6 (p < 0.01). In a study of 278 patients treated with different SSRIs (42 with fluoxetine), Serretti et al. [23] found no relationship between treatment response and CYP2D6. Interestingly, the doses were not adjusted in this study, and treatment response was measured as clinical improvement on the Hamilton Rating Scale for Depression.
CYP2C9
CYP2C9 has been reported to catalyze the metabolism of antidepressants, and it is involved in the N-demethylation of fluoxetine in the liver [1, 24]. As in the case of CYP2D6, fluoxetine also inhibits CYP2C9 activity [25]. The gene is located on chromosome 10 and several allelic variants causing decreased activity have been identified. The most common allele is *1, and the combination with normal activity is called *1/*1. Research has so far identified two allelic variants with different activities, called *2 and *3 [20, 26]. In the Caucasian population, the percentage of *2 carriers varies from 8 to 12 %, while the range is 3–8 % for *3 carriers [10, 20, 26]. In Asian and African populations the rates of *2 and *3 carriers remain low. The least common combination is *3/*3, which seems to be related to pharmacokinetic alterations. Carriers of the *3 allele show less enzymatic activity (5 % less than the *1 allele), while *2 allele carriers present intermediate enzymatic activity (12 % compared to the *1 allele) [10, 11, 20, 27]. Llerena et al.’s fluoxetine study sought to determine the relationship between CYP2C9 polymorphisms and treatment response. Only patients with two active CYP2D6 genes were selected to avoid bias, and the authors also adjusted doses. They observed that the dose-corrected plasma concentrations of fluoxetine and active moiety (fluoxetine plus norfluoxetine) were higher in patients with the combinations *1/*2 and *1/*3 than in those with *1/*1 (p < 0.05) [12]. These results were confirmed by another study which, to avoid bias, selected only EM patients who were homozygous for CYP2D6. The authors found that (R)-fluoxetine concentrations were lower in CYP2C9*1 homozygous patients than in the other participants (p < 0.05) [11]. This study also found that CYP2C9*3 carriers had higher blood concentrations of (R)-fluoxetine, (S)-fluoxetine and (R)- + (S)-fluoxetine than the other phenotypes. The authors concluded that the *3 allele was the one with least activity.
Other CYP
CYP2C19: This cytochrome has a role in antidepressant metabolism. The percentage of PMs varies according to ethnicity, from 2–5 % among Caucasians to approximately 15–25 % in the Asian population [10, 11, 19, 20]. The alleles associated with PM are *2 and *3. In Caucasians, it is usual to find *2 associated with less enzymatic activity. In studies with the Asian population an association between CYP2C19 and antidepressant response has been reported [24], in particular in N-demethylation [28]. In one study in Caucasians, a significantly lower level of depressive symptoms in PMs of CYP2C19 was found [29], although no dose correction seems to be necessary in people treated with fluoxetine [19].
Children and adolescents
Previously it was thought that pharmacokinetics of children and adolescents was very different from that of adults. This affirmation is true for some drugs in the first years of life. Fluoxetine is recommended for children aged 8, and we found no differences in absorption, distribution or excretion compared with adults.
Drug absorption
In newborns, gastric pH is high (2.3–3.6) and falls to adult levels (1.4–2.0) by the age of 2 years. By contrast, gastric emptying is slow in infants and reaches adult levels later in childhood [30, 31]. Drug bioavailability is influenced by gastric pH, gastric emptying, and intestinal metabolism, and by the age of 5 years it is similar to adults for most drugs [31, 32]. During childhood, therefore, the effect of administered drugs may be delayed [33].
Distribution
After absorption a drug is distributed. Distribution depends on molecular weight, the ionization constant, and on aqueous and lipid solubility. Children under 2 years have a larger distribution volume due to an increased water volume (60 %). It should be noted, therefore, that the distribution volume of newborns is larger for hydrophilic drugs and smaller for lypophilic drugs than it is in adults, although the adult level is reached by the age of 3–5 years [30, 31, 33]. Drug binding to proteins such as albumin reaches adult levels by the age of 1 year [31, 32].
Hepatic metabolism
Most drugs are metabolized by cytochrome P450 (CYPs), and as noted above both CYP2D6 and CYP2C9 are involved in fluoxetine metabolism [33]. No phenotypic differences between adult and children have been reported to date, and therefore one finds similar percentages of PM, IM, EM and UM individuals in children and in adults. Enzymatic activity differences are responsible for inter-individual variation in plasma concentrations of psychotropic medication [33].
Some years ago it was believed that children have an increased metabolism for all drugs, but it is now known that this depends on the enzyme involved. In the case of CYPs, the total liver content is lower at birth (50–70 % compared to adult levels) and reaches adult levels by the age of 1 year. CYP2C9 activity is high at birth and reaches adult levels by puberty, whereas CYP2C19 activity is low at birth and reaches adult levels by the age of 5 years. The differences between adults and children are not important if adjustments are made for liver weight. The activity of CYP2D6 is considerably lower at birth, but reaches adult levels by the age of 2–3 years [30, 31].
Fluoxetine is a well-tolerated drug. The literature contains only one study about fluoxetine pharmacokinetics in children. This study, by Wilens et al., was based on a sample of ten children (6–12 years old) treated with 20 mg of fluoxetine daily and were compared with 11 adolescents. The results showed that children have twofold higher maximum concentrations than adolescents, while the concentration of norfluoxetine was 1.7 times higher than in adolescents. When the authors took into account the children’s weight they found no differences between children and adolescents and recommended that treatment begins at 10 mg daily in pre-pubertal children and 20 mg daily in adolescents [13–34].
Excretion
Glomerular filtration, tubular absorption, urine pH and tubular secretion reach adult values by the age of 6–12 months [30, 32].
Pharmacodynamics
Serotonergic system
Serotonin transporter
The human gene encoding the serotonin transporter (SLC6A4) has been one of the most widely studied genes in relation to antidepressant response. This gene is located on chromosome 17, at position 17q11.1-q12, and it is involved in serotonin transport to the presynaptic neuron. The gene’s expression could be altered by a polymorphism which is involved in gene transcription. This polymorphism is called 5-HTTLPR and is an insertion/deletion located in the promoter region of SLC6A4 [17, 35]. 5-HTTLPR has two different alleles, known as s and l [3, 36]. The s allele has half the transcriptional activity of the l allele, and is present in 49 % of Caucasians [3, 37]. Two studies in Caucasian [36, 37] populations concluded that fluoxetine response is influenced by the 5-HTTLPR polymorphism. Individuals who are homozygous for the l allele are believed to respond better to fluoxetine treatment, and also have fewer side effects (Table 2). Another study which divided the sample according to age (under/over 25 years) concluded that the ss genotype was associated with worse response to fluoxetine. In depressed patients under the age of 25 genotype was not a significant predictor of outcome, whereas in the over-25 s the ss genotype was a significant predictor of a lower likelihood of response [38]. In studies in Chinese, among whom 79 % of the population carries the s allele, the results are similar to those for Caucasians (i.e. l carriers respond better to treatment) [39, 40]. One study conducted with a Korean population found that individuals who were homozygous for the s allele responded better to fluoxetine than l carriers [41] (Table 2). These results were confirmed in another study by Kim et al. [42]. The reason for this ethnic difference remains unclear. One explanation could be differences in allelic frequencies: in the Korean and Japanese populations only 25 % carried the l variant of 5-HTTLPR. Another explanation could be that 5-HTTLPR is linked to unknown functional variants. It may be an associated marker in linkage disequilibrium with a functional site, rather than a functional polymorphism itself [42] (Table 2). With respect to the pediatric population it has been postulated that the s allele is related to stress [43, 44]. In the presence of adverse life events, female carriers of the s allele appear to have a higher risk of developing depression [14]. Fluoxetine use in children has not been assessed, although there is one study involving citalopram in the Caucasian population, in which the authors concluded that s homozygous individuals responded worse to treatment and showed less symptomatic remission [2] (Table 3).
The SLC6A4 transcription may also be altered by another polymorphism called STin2 [45]. STin2 consists of a variable number of tandem repeats within intron 2, and it could alter the role of SLC64A in brain development and synaptic plasticity. It has two alleles, a short allele called 10 and the long one called 12. A relationship between this polymorphism and antidepressant response has been hypothesized. One study of fluoxetine or paroxetine found a better response to antidepressants among individuals who were 12 homozygous [41]. STin2 also exerts a synergistic effect with 5-HTTLPR [3], but research has been unable to find an association between treatment response and STin2 [40, 46, 47] (Table 2). A study in children with various antidepressants in doses corresponding to fluoxetine 40 mg/day also found no association between STin2 and treatment response [48].
There is another polymorphism called rs25531, just upstream of the HTTLPR in the gene’s promoter region, which showed evidence of affect transcription activity. The rs25531 has two alleles called G and A. An association with non-response to fluoxetine and G allele has been observed. Experiments showed that this polymorphism altered the binding of nuclear extracts to a consensus sequence for the activator protein 2 transcription factor, which is believed to be a critical factor in regulating neural gene expression in mammals [17, 49].
Serotonin receptors
Serotonin receptors are the most important candidates for modulation of antidepressant response, and most antidepressants increase the concentration of serotonin present in the synaptic cleft [3]. The serotonin 1A receptor (HTR1A) is located on chromosome 5, at position 5q11.2-13. The polymorphism 1019C/G (rs6295) regulates HTR1A transcription, and it has two alleles called C and G. Fluoxetine studies in Caucasian populations have failed to find a relationship between fluoxetine response and this polymorphism [17, 36, 50]. By contrast, one study with Asians reported a better response to fluoxetine among individuals who were homozygous for the G allele [40] (Table 4). The serotonin 2A receptor (HTR2A) is located on chromosome 13, at position 13q-14-q21, and it has two polymorphisms that may alter its transcription: 102T/C (rs6313), where the C allele would express less mRNA than would the T form, and 1438A/G (rs6311), where the G allele would express less mRNA than the A form. There is considerable discrepancy among HTR2A studies. Some studies have found no relationship between antidepressant response and HTR2A [40, 51], whereas others have reported an association [36, 49]. In children, HTR2A has not been associated with antidepressant response [44] or major depression [52].
Serotonin synthesis
Tryptophan hydroxylase 1 (TPH1) is an enzyme encoded by the TPH1 gene, located on chromosome 11 at position 11p15.3-p14, and it is expressed in peripheral organs. TPH1 has great affinity for tryptophan, and also shows high enzymatic activity. It has two polymorphisms, called 218A/C and 799A/C (it is not known whether 799A/C alters TPH1 activity). Most studies have found no association between fluoxetine response and the 218A/C (rs1800532) polymorphism [17, 40, 52], although there is one exception to this [36] (Table 4). Tryptophan hydroxylase 2 (TPH2) is located on chromosome 12, at position 12q21.1, and is more commonly found in brain tissue. TPH2 has several polymorphisms which have been associated with major depression, suicidal behavior and fluoxetine response [36, 54]; some of them, such as G1463A (Arg441His) can alter its transcription. Poor treatment response has been observed in depressed patients carrying 1463A [55]. Another polymorphism that has been studied is G703T (rs4570625). One study with citalopram found that children who are homozygous for the G allele responded better to treatment [2] (Table 3).
Serotonin degradation
Monoamine oxidase A (MAO-A) is encoded by the MAO-A gene, located on chromosome X at position XP11.23, and its transcription can be altered by the VNTR polymorphism. VNTR has two alleles: 3R and 4R. The 4R allele, considered to be a long allele, has more transcription activity than the short one (3R). MAO-A plays an important role in the metabolism and regulation of central serotonin and norepinephrine, which in turn play a part in the pathogenesis of major depression disorder. MAO-A is associated with depression through its involvement with serotonin and norepinephrine [17, 56]. Several studies have found an association between MAO-A VNTR polymorphism and antidepressant response [36] or depression [56] (Table 4). However, this association has not been found in children [14]. One study reported that females who were homozygous for 3R responded faster to fluoxetine than those who were 4R carriers [56] (Table 4).
Catechol-O-methyltransferase (COMT)
COMT is located on chromosome 22, at position 22q11.1-q11.2, and its activity can be altered by the polymorphism 158Val/Met (rs4680). Met has lower transcriptional activity than Val. The 158Val/Met polymorphism has been associated with suicidal behavior and personality traits, and it is also involved in dopamine degradation [17, 57]. One fluoxetine study in an Asian population found that individuals who were homozygous for Val showed a worse treatment response than Met carriers, and that men were also more influenced by genotype [57] (Table 5). In the Caucasian population, Met carriers have been reported to show a poorer response to treatment [58]. No association between COMT and anxiety or depression has been found in children [59].
Other genes related to fluoxetine pharmacodynamics
Brain-derived neurotrophic factor (BDNF)
BDNF is a small protein involved in neuronal growth and synaptic and neuronal plasticity. It is encoded by the BDNF gene, which is located on chromosome 11 at position 11p13. The polymorphism 196G/A (rs6265) is a valine substitution by methionine in exon 1 (Val66Met) [60]. Antidepressants seem to influence BDNF synthesis [61]. Fluoxetine studies have found no association between BDNF and antidepressant response, although depression was observed to remit more quickly in individuals who were Met/Val heterozygous for 196G/A as compared to homozygous patients [60, 62] (Table 5). One study of obsessive–compulsive disorder found an association between BDNF and antidepressant response [63]. BDNF levels have also been reported to be decreased in depressed children and adolescents [64].
Corticotropin-releasing hormone receptor 1 (CRHR1)
Hypothalamic–pituitary–adrenal dysfunction is present in most depressed patients, and therefore CRHR1 is probably involved in antidepressant response. It is located on chromosome 17, at position 17q12-q22 [17, 65]. Two studies in Caucasian and Asian populations associated three polymorphisms (rs1876828, rs242939, rs242941) and one haplotype (GAG) with antidepressant response [66] (Table 5). Another study concluded that the relationship between polymorphisms and depression depends on anxiety levels [67].
Binding protein 5 (FKBP5)
FKBP5 is a co-chaperone member of the immunophilin protein family. It plays a role in immunoregulation and in basic cellular processes involving protein folding and trafficking. Its polymorphisms have been associated with psychiatric disorders [68], and the rs1360780 polymorphism seems to be involved in general antidepressant response [69, 70] (Table 5). Although one study of children and several antidepressants reported an association between suicide and FKBP5 (p = 0.025), no association was found between FKBP5 and antidepressant response [48] (Table 3).
Glucocorticoid receptor (NR3C1 or GR)
This is the receptor to which cortisol and other glucocorticoids bind. NR3C1 regulates genes that control development, metabolism and immune response. In humans the GR protein is encoded by the NR3C1 gene, which is located on chromosome 5 (5q31). Numerous genetic polymorphisms within the GR gene have been described. Research has yet to demonstrate that NCR31 plays a role in depression, despite the fact that antidepressants stimulate NCR31 action [71, 72]. There are no published studies with fluoxetine, but one study with escitalopram and nortriptyline reported an association between NR3C1 and antidepressant response [72].
CAMP responsive element binding protein 1 (CREB1)
CREB1 is a protein which, in humans, is encoded by the CREB1 gene. This protein binds the cAMP response element and it is a member of the leucine zipper family of DNA-binding proteins. It is phosphorylated by several protein kinases and induces gene transcription in response to hormonal stimulation of the cAMP pathway. Alternative splicing of the CREB1 gene results in two transcript variants encoding different isoforms [67]. CREB1 is located on chromosome 2, at position 2q32.3-q34. It has been associated with antidepressant response and depression, and also plays a role in neuronal plasticity and long-term memory. Specifically, increased CREB levels in rodent models result in antidepressant-like behaviors and studies in both humans and rodents have shown that CREB is upregulated by chronic antidepressant treatment [67]. One study with a number of antidepressants (including fluoxetine) found no relationship between antidepressant response and CREB1 polymorphisms [73] (Table 5). Similarly, a study in children reported no association between childhood depression and CREB1 [74].
Phosphodiesterases 1 and 11A (PDE1 and PDE11A)
Phosphodiesterases (PDEs) catalyze the hydrolysis of cAMP and cGMP to the corresponding 5’-monophosphates, and provide a mechanism to down-regulate cAMP and cGMP signalling. This gene encodes a member of the PDE protein superfamily. Multiple transcript variants encoding different isoforms have been found for the PDE11A gene [75]. One study with fluoxetine and desipramine found a relationship between PDE11A and depression, particularly with respect to the rs3770018 A/C polymorphism, with C-allele carriers being more susceptible to depression (p = 0.0005) [76, 77]. PDE1 and PDE11A have also been associated with fluoxetine response [76–78] (Table 5).
Glycogen synthase kinase 3 beta (GSK3B)
GSK3B is an enzyme which, in humans, is encoded by the GSK3B gene, located on chromosome 3 at position 3q13.33. It is involved in cellular functions including gene expression, cellular architecture and apoptosis, and it is mainly expressed in neuronal tissue during development. GSK3B inhibition seems to play a role in the therapeutic effect of antidepressants [79]. GSK3B levels are increased in depressed patients, and BDNF and CREB1 may interact with GSK3B in relation to antidepressant response [80]. One study with fluoxetine and citalopram reported no association between CSK3B polymorphisms and depression, although the authors did find an association between the rs334558, rs13321783, rs2319398 and rs6808874 polymorphisms and antidepressant response after 4 weeks of treatment. As for the different haplotypes of the four polymorphisms, TAGT carriers have been reported to show a poorer treatment response at 4 and 8 weeks [80] (Table 5).
Serpin-1
Serpin-1 is also known as PAI-1 and is located on chromosome 7, at position 7q21.3-q22. Several polymorphisms, such as 4G/5G (rs1799889), may alter its transcription. The 4G allele transcripts more actively than the 5G allele. Serpin regulates the plasminogen activator (tPA), which is involved in learning, memory, stress, neuronal degeneration and addictions. tPA is involved in the cleavage of proBDNF in the brain. Given that BDNF has a central role in major depression disorder pathogenesis and in antidepressant action, it is possible that tPA may also be involved in major depression disorder pathogenesis. One study with fluoxetine and citalopram reported a relationship between serpin-1 and both depression and antidepressant response [81] (Table 5).
Conclusions
This review systematically summarizes the available empirical evidence concerning the influence of pharmacogenetics on the response to fluoxetine treatment in patients diagnosed with major depressive disorder. The main limitations of this review are the low number of studies with antidepressants in children and adolescents and the methodological differences between the studies collected.
In children, only one pharmacokinetic study with fluoxetine was found [13]. The information suggests that there are no differences between adults and children (aged 8 years) in relation to the absorption, distribution, metabolism or excretion of fluoxetine, when children’s weight is taking into account. Currently, given the lack of a clear relationship between fluoxetine dose and response to treatment, dosage adjustments in pediatric patients should continue to be based on observed efficacy and tolerability.
Similarly, very few studies of pharmacodynamics in children have been performed. With regard to SCL6A4 and TPH2 one study in children with citalopram was found [2]. The results suggest that the polymorphisms 5HTTLPR of SCL6A4 and G703T of THP2 are involved in response to treatment. Although the study was not done performed with fluoxetine, the results are similar to the ones obtained in adults with fluoxetine. The studies in children suggest that age may not influence the pharmacogenetics of fluoxetine, but further studies are required to confirm these results.
In relation to the methodologies used in the studies, differences were found regarding the study period, the number of subjects, the fluoxetine dose (from 10 to 80 mg/day) and the use of specific scales to measure clinical improvement. These methodological differences may explain the disparity in results. Further studies based on stricter criteria are required to confirm the results obtained so far, and to identify new therapeutic targets for improving antidepressant treatment.
Another point to take into account is ethnicity. In the case of polymorphism 5HTTLPR of SLC6A4 the response seemed less favorable for Caucasian patients with s/s genotype than for l/l genotype [34, 35], while in Asians effects in both directions were observed. In Chinese populations better response to treatment was related to l/l genotype [37, 38], while in Korean and Japanese populations the s/s genotype was associated with favorable response [39]. For other polymorphisms of the genes HTR1A, COMT, PDEA1, PDEA11, GSK3B and serpin-1 an association between these polymorphisms and fluoxetine response was found in Asian population. Studies in Caucasian population are needed to establish whether these polymorphisms are involved in the fluoxetine response.
On the basis of our review we conclude that fluoxetine response may be influenced by certain genes which are involved in its pharmacodynamics and pharmacokinetics. As regards pharmacokinetics, different genetic polymorphisms of CYP2D6 and CYP2C9 influence the blood concentrations of fluoxetine. Research has yet to demonstrate a correlation between plasma concentrations and clinical improvement, so the benefit of knowing the patient’s phenotype would be to avoid adverse reactions or a lack of drug effect. Further fluoxetine studies are required to confirm the results obtained by Llerena et al. [12], who reported that poor metabolizers of CYPs have higher plasma concentrations of fluoxetine.
With respect to pharmacodynamics, some genes are related to fluoxetine response, while others appear to have no mediating effect. Those genes for which there are still no conclusive results as regards their role in relation to fluoxetine response include SLC6A4 (STin2), HTR2A, TPH1, TPH2, BDNF, FKBP5, NR3C1 and CREB1. Pharmacogenetic studies indicate some candidate genes that may be involved in fluoxetine response. This area of research has great potential, particularly in psychiatry, given the lack of biologically based treatment guidelines. There is great hope that it will soon be possible to personalize psychiatric treatments based on genetic profiles.
References
Hiemke C, Härtter S (2000) Pharmacokinetics of selective serotonin reuptake inhibitors. Pharmacol Ther 85(1):11–28
Kronenberg S, Frisch A, Rotberg B, Carmel M, Apter A, Weizman A (2008) Pharmacogenetics of selective serotonin reuptake inhibitors in paediatric depression and anxiety. Pharmacogenomics 9(11):1725–1736
Kato M, Serretti A (2010) Review and meta-analysis of antidepressant pharmacogenetic findings in major depressive disorder. Mol Psychiatry 15:473–500
Porcelli S, Drago A, Fabbri C, Gibiino S, Calati R, Serretti A (2011) Pharmacogenetics of antidepressant response. J Psychiatry Neurosci 36(2):87–113
Steimer W, Müller B, Leucht S, Kissling W (2001) Pharmacogenetics: a new diagnostic tool in the management of antidepressive drug therapy. Clin Chim Acta 308:33–41
DeVane CL (1999) Metabolism and pharmacokinetics of selective serotonin reuptake inhibitors. Cell Mol Neurobiol 19(4):443–466
Ring BJ, Eckstein JA, Gillespie JS, Binkley SN, Vandenbranden M, Wrighton SA (2001) Identification of the human cytochromes P450 responsibles for in vitro formation of R- and S-Norfluoxetine. J Pharmacol Exp Ther 297:1044–1050
Charlier C, Broly F, Lhermitte M, Pinto E, Ansseau M, Plomteaux G (2003) Polymorphisms in the CYP2D6 gene: association with plasma concentrations of fluoxetine and paroxetine. Ther Drug Monit 25:738–742
Spina E, Santoro V, D’Arrigo C (2008) Clinically relevant pharmacokinetic drug interactions with second-generation antidepressants: an update. Clin Ther 30(7):1206–1227
Scordo MG, Caputi AP, D’Arrigo C, Fava G, Spina E (2004) Allele and genotype frequencies of CYP2C9, CYP2C19 and CYP2D6 in an Italian population. Pharmacol Res 50:195–200
Scordo MG, Spina E, Dahl M-L, Gatti G, Perucca E (2005) Influence of CYP2C9, 2C19 and D6 Genetic polymorphisms on the steady-state plasma concentrations of the enantiomers of fluoxetine and norfluoxetine. Basic Clin Pharmacol Toxicol 97:296–301
Llerena A, Dorado P, Berecz R, González AP, Peñas-Lledó EM (2004) Effect of CYP2D6 and CYP2C9 genotypes on fluoxetine and norfluoxetine plasma concentrations during steady-state conditions. Eur J Clin Pharmacol 59:869–873
Wilens TE, Cohen L, Biederman J, Abrams A, Neft D, Faird N et al (2002) Fluoxetine pharmacokinetics in pediatric patients. J Clin Psychopharmacol 22(6):568–575
Eley TC, Sugden K, Corsico A, Gregory AM, Sham P, McGuffin P et al (2004) Gene-environment interaction analisis of serotonin system markers with adolescent depression. Mol Psychiatry 9:908–915
Zhou SF (2009) Polymorphism of human cytochrome P450 2D6 and its clinical significance: part II. Clin Pharmacokinet 48(12):761–804
Zhou SF (2009) Polymorphism of human cytochrome P450 2D6 and its clinical significance: part I. Clin Pharmacokinet 48(11):689–723
Keers R, Aitchison KJ (2011) Pharmacogenetics of antidepressant response. Expert Rev Neurother 11(1):101–125
Hinrichs JW, Loovers HM, Scholten B, van der Weide J (2008) Semi-quantitative CYP2D6 gene doses in relation to metabolic ratios of psychotropics. Eur J Clin Pharmacol 64:979–986
Kirchheiner J, Nickchen K, Bauer M, Wong ML, Licinio J, Roots I et al (2004) Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic variations to the phenotype of drug response. Mol Psychiatry 9:442–473
Porcelli S, Fabbri C, Spina E, Serretti A, De Ronchi D (2011) Genetic polymorphisms of cytochrome P450 enzymes and antidepressant metabolism. Expert Opin Drug Metab Toxicol 7(9):1101–1115
Parker G, Rowe M, Mehta F, Kumar S (2010) Will a new genotyping test help the clinician predict response to antidepressant drugs? Australas Psychiatry 18(5):413–416
Kirchheiner J, Brøsen K, Dahl ML, Gram LF, Kasper S, Roots I et al (2001) CYP2D6 and CYP2C19 genotype-based dose recommendations for antidepressants: a first step towards subpopulation-specific dosages. Acta Psychiatr Scand 104:173–192
Serretti A, Calati R, Massat I, Linotte S, Kasper S, Lecubrier Y et al (2009) Cytochrome P450, CYP1A2, CYP2C9, CYP2C19 and CYP2D6 genes are not associated with the response and remission in a sample of depressive patients. Int Clin Psycopharmacol 24:250–256
Liu Z-H, Shu Y, Huang S-L, Wang L-S, He N, Zhou H–H (2001) Effects of CYP2C19 genotype and CYP2C9 on fluoxetine N-demethylation in human liver microsomes. Acta Pharmacol Sin 22(1):85–90
Schmider J, Greenblatt DJ, von Moltke LL, Karsov D, Shader RI (1997) Inhibition of CYP2C9 by selective serotonin reuptake inhibitors in vitro: studies of phenytoin p-hydroxylation. Br J Clin Pharmacol 44:495–498
Dorado P, Berecz R, Norberto MJ, Yasar Ü, Dahl ML, Llerena A (2003) CYP2C9 genotypes and diclofenaco metabolism in Spanish healthy volunteers. Eur J Clin Pharmacol 59:221–225
Dorne JL (2004) Impact of interindividual differences in drug metabolism and pharmacokinetics on safety evaluation. Fundam Clin Pharmacol 18:609–620
Liu ZQ, Cheng ZN, Huang SL, Chen XP, Ou-Yang DS, Jiang CH et al (2001) Effect of the CYP2C19 oxidation polymorphism on fluoxetine metabolism in Chinese healthy subjects. Br J Clin Pharmacol 52:96–99
Sim SC, Nordin L, Andersson TM-L, Virding S, Olsson M, Pedersen NL et al (2010) Association between CYP2C19 polymorphism and depressive symptoms. Am J Med Genet Part B 153B:1160–1166
Yokoi T (2009) Essentials for starting a pediatric clinical study (1): pharmacokinetics in children. J Toxicol Sci 34 Suppl 2:SP307–12
Anderson GD (2010) Developmental pharmacokinetics. Semin Pediatr Neurol 17:208–213
Pichini S, Papaseit E, Joya X, Vall O, Farré M, García-Algar O et al (2009) Pharmacokinetics and therapeutic drugs monitoring of phychotropic drugs in pediatrics. Ther Drug Monit 31:283–318
Van den Anker JN (2010) Developmental Pharmacology. Dev Disabil Res Rev 16:233–238
Findling RL, McNamara NK, Stansbrey RJ, Feeny NC, Young CM, Peric FV et al (2006) The relevance of pharmacokinetic studies in designing efficacy trials in juvenile major depression. J Child Adolesc Psychopharmacol 16(1–2):131–145
Serreti A, Smeraldi E (2004) Neural network analysis in pharmacogenetics of mood disorders. BMC Med Genet 5:27
Peters EJ, Slager SL, McGrath PJ, Knowles JA, Hamilton SP (2004) Investigation of serotonin-related genes in antidepressant response. Mol Psychiatry 9:879–889
Perlis RH, Mischoulon D, Smoller JW, Wan YJ, Lamon-Fava S, Lin KM et al (2003) Serotonin transporter polymorphisms and adverse effects with fluoxetine treatment. Biol Psychiatry 54:879–883
Joyce PR, Mulder RT, Luty SE, McKenzie JM, Miller AL, Rogers GR et al (2003) Age-dependent antidepressant pharmacogenomics: polymorphisms of serotonin transporter and G protein beta3 subunit as predictors of response to fluoxetine and nortyptiline. Int J Neuropsychopharmacol 6:339–346
Yu YW-Y, Tsai S-J, Chen T-J, Lin C-H, Hong C-J (2002) Association study of serotonin transporter promoter polymorphism and symptomatology and antidepressant response in major depressive disorders. Mol Psychiatry 7:1115–1119
Hong C-J, Chen T-J, Yu YW-Y, Tsai S-J (2006) Response to fluoxetine and serotonin 1A receptor (C-1019G) polymorphism in Taiwan Chinese major depressive disorder. Pharmacogenomics J 6:27–33
Kim DK, Lim SW, Lee S, Sohn SE, Kim S, Hahn CG et al (2000) Serotonin transporter gene polymorphism and antidepressant response. NeuroReport 11:215–219
Kim H, Lim SW, Kim S, Kim JW, Chang YH, Carroll BJ, Kim DK (2006) Monoamine transporter gene polymorphisms and antidepressant response in Koreans with late-life depression. JAMA 296(13):1609–1618
Caspi A, Sugden K, Moffitt TE, Taylor A, Craig IW, Harrington H et al (2003) Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 301:386–389
Aslund C, Leppert J, Comasco E, Nordquist N, Oreland L, Nilsson KW (2009) Impact of the interaction between the 5HTTLPR polymorphism and maltreatment on adolescent depression. Popul Based Study 39:524–531
Ogilvie D, Battersby S, Bubb VJ, Fink G, Harmar AJ, Goodwim GM et al (1996) Polymorphism in serotonin transporter gene associated with susceptibility to major depression. Lancet 374(9003):731–733
Smits KM, Smits LJM, Schouten JSAG, Stelma FF, Nelemans P, Prins MH (2004) Influence of SERTPR and STin2 in the serotonin transporter gene on the effect of selective serotonin reuptake inhibitors in depression: a systematic review. Mol Psychiatry 9:433–441
Smits KM, Smits LJM, Peeters F, Schouten J, Janssen R, Smeets H et al (2008) The influence of 5-HTTLPR and STin2 polymorphisms in the serotonin transporter gene on treatment effect of selective reuptake inhibitors in depressive patients. Psychiatr Genet 18:184–190
Brent D, Melhem N, Ferrell R, Emslie G, Wagner KD, Ryan N et al (2010) Association of FKBP5 polymorphisms with suicidal events in the treatment of resistant depression in adolescents (TORDIA) Study. Am J Psychiatry 167(2):190–197
Kraft JB, Slager SL, McGrath PJ, Hamilton SP (2005) Sequence analysis of the serotonin transporter and associations with antidepressant response. Biol Psychiatry 58:374–381
Noro M, Antonijevic I, Forray C, Kasper S, Kocabas NA, Lecubrier Y et al (2010) 5HT1A and 5HT2A receptor genes in treatment response phenotypes in major depressive disorder. Int Clin Psycopharmacol 25:228–231
Illi A, Setälä-Soikkeli E, Viikki M, Poutanen O, Huhtala H, Mononen N et al (2009) 5-HTRA1, 5-HTR2A, 5-HTR6, TPH1 and TPH2 polymorphisms and major depression. NeuroReport 20:1125–1128
Shaikh SA, Strauss J, King N, Bulgin NL, Vetró A, Kiss E et al (2008) Association study of serotonin system genes in childhood-onset mood disorder. Psychiatr Genet 18:47–52
Wang HS, Yeh TL, Chang HH, Gean PW, Chi MH, Yang YK et al (2011) TPH1 is associated with major depressive disorder but not with SSRI/SNRI response in Taiwanese patients. Psycopharmacology (Berl) 213:773–779
Tsai SJ, Hong CJ, Liou YJ, Yu Y-W, Chen TJ, Hou SJ et al (2009) Tryptophan hydroxylase 2 gene is associated with major depression and antidepressant treatment response. Prog Neuropsychopharmacol Biol Psychiatry 33:637–641
Zhang X, Gainetdinov RR, Beaulieu JM, Sotnikova TD, Burch LH, Williams RB et al (2005) Loss-of-function mutation in tryptophan hydroxylase-2 identified in unipolar major depression. Neuron 45:11–16
Yu Y W-Y, Tsai S-J, Hong C-J, Chen T-JM, Chen M-C, Yang C-W (2005) Association study of monoamine oxidase A gene promoter polymorphism with major depressive disorder and antidepressant response. Neuropsycopharmacology 30(9):1719–1723
Tsai SJ, Gau Y-TA, Hong C-J, Liou Y-J, Yu YW-Y, Chen T-J (2009) Sexually dimorphic effect of catechol-O-methyltransferase val158met polymorphism on clinical response to fluoxetine in major depressive patients. J Affect Disord 113:183–187
Arias B, Serretti A, Lorenzi C, Gastó C, Catalán R, Fañanás L (2006) Analysis of COMT gene (Val 158 Met polymorphism) in the clinical response to SSRIs in depressive patients of European origin. J Affect Disord 90:251–256
Middeldorp CM, Slof-Op’T Landt MCT, Medland SE, Van Beijsterveldt CEM, Bartels M, Willemsen G et al (2010) Anxiety and depression in children and adults: influence of serotonergic and neurotrophic genes? Genes Brain Behav 9:808–816
Tsai SJ, Cheng CY, Yu YW, Chen TJ, Hong CJ (2003) Association study of a brain-derived neurotrophic-factor genetic polymorphism and major depressive disorders, symptomatology, and antidepressant response. Am J Med Genet B Neuropsychiatr Genet 123B(1):19–22
Allaman I, Fiurmelli H, Magistretti PJ, Martin JL (2011) Fluoxetine regulates the expression of neurotrophic/growth factors and glucose metabolism in astrocytes. Psychopharmacology (Berl) 216:75–84
Zou YF, Wang Y, Liu P, Feng XL, Wang BY, Zang TH et al (2010) Association of brain-derived neurotrophic factor genetic Val66Met polymorphism with severity of depression, efficacy of fluoxetine and its side effects in chinese major depressive patients. Neuropychobiology 61(2):71–78
Real E, Gratacòs M, Soria V, Escaramís G, Alonso P, Segalàs C et al (2009) A brain-derived neurotrophic factor haplotype is associated with therapeutic response in obsessive–compulsive disorder. Biol Psychiatry 66:674–680
Pandey GN, Dwivedi Y, Rizavi HS, Ren X, Zhang H, Pavuluri M (2010) Brain-derived neurotrophic factor gene and protein expression in pediatric and adult depressed subjects. Prog Neuropsychopharmacol Biol Psychiatry 34:645–651
Liu Z, Zhu F, Wang G, Xio Z, Tang J, Liu W et al (2007) Association study of corticotrophin-releasing hormone receptor1 gene polymorphisms and antidepressant response in major depressive disorders. Neurosci Lett 414:155–158
Licino J, O¡Kirwan F, Irizarry K, Merriman B, Thakur S, Jepson R et al (2004) Association of corticotrophin-releasing hormone receptor1 haplotype and antidepressant treatment response in Mexican–Americans. Mol Psychiatry 9:1075–1082
Dong C, Wonf M-L, Licino J (2009) Sequence variations of ABCB1, SLC6A2, SCL6A3, SLC6A4, CREB1, CRHR1 and NTRK2: association with major depression and antidepressant response in Mexican–Americans. Mol Psychiatry 14:1105–1118
Zobel A, Maier W (2010) Pharmacogenetics of antidepressive treatment. Eur Arch Psychiatry Clin Neurosci 260:407–417
Binder EB, Salyakina D, Lichtner P, Wochnik GM, Ising M, Pütz B et al (2004) Polymorphisms in FKBP5 are associated with increased recurrence of depressive episodes and rapid response to antidepressant treatment. Nat Genet 36(12):1319–1325
Horstmann S, Lucae S, Menke A, Hennings JM, Ising M, Roeske D, Müller-Myhsok B, Holsboer F, Binder EB (2010) Polymorphisms in GRIK4, HTR2A, and FKBP5 show interactive effects in predicting remission to antidepressant treatment. Neuropsychopharmacology 35(3):727–740
Claes S (2009) Glucocorticoid receptor polymorphisms in major depression. Ann N Y Acad Sci 1179:216–228
Uher R, Huezo-Díaz P, Perroud N, Smith R, Rietschel M, Mors O et al (2009) Genetic predictors of response to antidepressants in the GENDEP project. Pharmacogenomics J 9:225–233
Serretti A, Chiesa A, Calati R, Massat I, Linotte S, Kasper S et al (2011) A preliminary investigation of the influence of CREB1 gene on treatment resistance in major depression. J Affect Disord 128:56–63
Burcescu I, Wigg K, King N, Vetro A, Kiss E, Katay L et al (2005) Association study of CREB1 and childhood-onset mood disorders. Am J Med Genet B Neuropsychiatr Genet 137B:45–50
Hebb AL, Robertson HA (2007) Role of phosphodiesterases in neurological and psychiatric disease. Curr Opin Pharmacol 7:86–92
Wong M-L, Whelan F, Deloukas P, Whittaker P, Delgado M, Cantor RM et al (2006) Phosphodiesterase genes are associated with susceptibility to major depression and antidepressant treatment response. Proc Natl Acad Sci USA 103(41):15124–15129
Luo H-R, Wu G-S, Dong C, Arcos-Burgos M, Ribeiro L, Licino J et al (2009) Association of PDE11A global haplotype with major depression and antidepressant drug response. Neuropsychiatr Dis Treat 5:163–170
Esposito K, Reierson G, Luo HR, Wu GS, Licinio J, Wong M-L (2009) Phosphodiesterase genes and antidepressant treatment response: a review. Ann Med 41:177–185
Li X, Zhu W, Roh MS, Friedman AB, Rosborough K, Jope RS (2004) In vivo regulation of glycogen synthase kinase-3beta (GSK3beta) by serotonergic activity in mouse brain. Neuropsychopharmacology 29:1426–1431
Tsai S-J, Liou Y-J, Hong C-J, Yu YW-Y, Chen T-J (2008) Glycogen synthase kinase-3b gene is associated with antidepressant treatment response in Chinese major depressive disorder. Pharmacogenomics J 8:384–390
Tsai SJ, Hong CJ, Liou YJ, Yu YW, Chen TJ (2008) Plasminogen activator inhibitor-1 gene is associated with major depression and antidepressant treatment response. Pharmacogenet Genomics 18(10):869–875
Acknowledgments
This study was financially supported by Alicia Koplowitz Foundation and Centro de Investigación Biológica en Red de Salud Mental (CIBERSAM).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Blazquez, A., Mas, S., Plana, M.T. et al. Fluoxetine pharmacogenetics in child and adult populations. Eur Child Adolesc Psychiatry 21, 599–610 (2012). https://doi.org/10.1007/s00787-012-0305-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-012-0305-6