
Abstract
Background
There is increasing evidence that catatonia is an important source of impairment in adolescents and adults with autism.
Aim
Review of the evaluation, diagnosis, differential diagnosis, and treatment of catatonia in autism.
Method
Presentation and discussion of a case-vignette spanning early childhood to adulthood.
Results
Autistic and catatonic symptoms overlap, yet catatonia is diagnosable in about one of seven adolescents and young adults with autism. Case-reports suggest that benzodiazepines and electroconvulsive therapy are effective treatments in the acute and maintenance phase for people with autism who develop catatonia.
Conclusions
Catatonia should be assessed in people with autism when there is an obvious and marked deterioration in movement, vocalizations, pattern of activities, self-care, and practical skills. Benzodiazepines and electroconvulsive therapy are favored options for acute and maintenance treatment in these cases. Further studies on the possible biological-genetic overlap between autism and catatonia would be helpful.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
More effective treatments are needed in autism, an early-onset neurodevelopmental disorder, diagnosed on the basis of enduring deficits in social interaction, impaired language and communication, and presence of stereotyped and repetitive behavior [2]. Affected people show great clinical and functional heterogeneity. Autism is associated at times with a medical or neurological condition. Most cases are idiopathic although an important genetic component is suspected. Mainstay treatments for autism and its complicating conditions rely on classic methods such as behavioral therapies, speech therapy, parent education, stimulants, antipsychotics, and other psychotropic medications. Alternative treatments of questionable value and safety are common. Early identification of at-risk toddlers and intensive early intervention have received recent emphasis. However, there is no definitive cure or prevention.
There is increased recognition of catatonia as a comorbid syndrome of autism. Catatonia is characterized by abnormalities of movement, speech and behavior, and is most commonly associated with mood and psychotic disorders in the general psychiatric population [24]. Although psychotic symptoms such as hallucinations and delusions are relatively rare in people with autism [35], alternate psychotic manifestations like disorganized behavior and catatonic symptoms are prominent in many patients with autism. Examples of shared symptoms between autism and catatonia are mutism, stereotypic speech, echolalia, stereotypic or repetitive behaviors, posturing, grimacing (Fig. 1), rigidity (Fig. 2), mannerisms, and purposeless agitation.

Catatonic grimacing. From reference [9], p 267

Catatonic rigidity. From reference [9], p 269
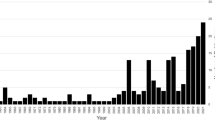
In some autistic people, these individual symptoms worsen to the point of full-blown catatonia. So far, there are two systematic studies of catatonia in autism [7, 58] that show that catatonia occurs in 12–17% of adolescents and young adults with autism. In the study of Wing and Shah [58], 17% of a large referred sample of adolescents and young adults with autism satisfied modern criteria for catatonia. Thirty individuals with autism aged 15 or older met criteria for catatonia. Classic Autistic Disorder was diagnosed in 11 (37%), atypical autism in 5 (17%), and Asperger Disorder in 14 (47%). Under age 15, no child demonstrated the full syndrome although isolated catatonic symptoms were often observed. In the majority of cases, catatonic symptoms started between 10 and 19 years of age. Five individuals had brief episodes of slowness and freezing during childhood, before age 10. Obsessive-compulsive and aggressive behaviors preceded catatonia in some cases. Visual hallucinations or paranoid ideas were occasionally reported, but no diagnosis of schizophrenia could be made.
In the second study [7], 13 (12%) of 120 autistic individuals between ages 17 and 40 years (mean age 25.5 years) had clinically diagnosed catatonia with severe motor initiation problems. Another four individuals had several catatonic symptoms but not the full syndrome. Eight of the 13 individuals with catatonia suffered from Autistic Disorder; the remaining five were diagnosed with atypical autism. The proportion of those with Autistic Disorder that were diagnosed with catatonia was 11% (8/73). Fourteen percent (5/35) of those with atypical autism had catatonia. An increasing number of cases of catatonia in autism [4, 8, 13, 14, 17, 26, 28, 30, 43, 47–49, 56, 60] have been reported throughout the world over the last 15 years. Several patients responded to benzodiazepines or electroconvulsive therapy (ECT) after other treatments failed [4, 26, 28, 56, 60].
A case-vignette of an autistic adolescent who develops catatonia ensues. The material is based on the cumulative clinical experience of the authors and illustrates the vicissitudes of appropriate evaluation, diagnosis, and treatment of catatonia in autism.
Case-vignette
Autism in early childhood
Z was born after 9 months of normal pregnancy and initially met developmental milestones. In the second year, the parents noticed delays in speech and communication. Deafness was suspected but a medical examination showed that Z was healthy and had excellent hearing and a normal 46 XY karyotype. His motor skills improved with developmental services, yet Z was diagnosed as autistic at age three owing to ongoing language, communication, and interpersonal impairments. Testing showed an IQ of 86.
As early as age five, Z showed sporadic “freezing” episodes in which his arm would suddenly stretch out and remain immobile for several seconds. He also developed both vocal and motor tics and was additionally diagnosed with Tourette’s syndrome. Trials of alpha-2 agonists and antipsychotics did not alleviate the tics, and led to further behavioral deterioration. During the following years, Z attended specialized classes at school and his verbal skills improved. His social function remained atypical. His behavior was characterized by “insistence on sameness” and he developed intense but varying interests like collecting miniature cars, trains, and airplanes.
Catatonia in adolescence
At age 16, Z showed a decline in function when he stopped speaking except to family members. His posture deteriorated with slumping and complaints of back pain. At school, he refused to enter classrooms and would slowly walk head down through corridors. He was unable to retain food in his mouth and lost about £20 within the next half year. He showed poor fine and gross motor skills, with difficulty holding and using implements. Eventually, he required support to even stand. At home, his speech slowed excessively and he would not engage in activities other than those related to his specific interest in transport, mostly aircraft. By age 17, it was very difficult to get him to leave the family home. He required assistance washing and dressing and stopped using the toilet. The psychiatrist considered a diagnosis of catatonia but demurred due to the seemingly selective occurrence of symptoms. During medical examinations, he would often not cooperate and become unresponsive. Routine lab work and brain CT scan were negative. Patient refused to take the diazepam and fluoxetine that were prescribed for anxiety and depression. With intensive behavioral intervention, using the framework set out by Shah and Wing for the treatment of catatonia in people with autism [49], he showed moderate improvement. Despite the progress made, there were various motility problems across all circumstances, mainly slowness of movement, clumsiness, inability to control movement, poor coordination, freezing of movement, and awkward posture for which risperidone was prescribed without improvement.
One year later, Z was hospitalized due to dehydration and dramatic weight loss. He was fed with a nasogastral tube and diagnosed with depression and catatonia for which a selective serotonin reuptake inhibitor and an atypical antipsychotic were prescribed. He started to regain his appetite and gradually developed interests in other activities. His slowness and body rigidity improved. After a few months, his function decreased again, with decreased oral intake, urinary incontinence, compulsive behaviors, refusal to go outside the house and noncompliance with routine activities. During the next year and a half, his condition waxed and waned, unresponsive to different medication trials that included anticholinergics, alpha-2 agonists, selective serotonin reuptake inhibitors, and various atypical antipsychotics.
About a year later, Z was placed in a residential program for young adults with autism where he did well for a few months. However, psychomotor symptoms returned and a neurological work-up to rule out seizures was negative. Trials of anticonvulsants and alpha-2 agonists failed to alleviate symptoms. His diagnoses at this time were Pervasive Developmental Disorder Not Otherwise Specified (PDD NOS), Tic Disorder, Depressive Disorder with Catatonia, Anxiety Disorder, and mild mental retardation. As he seemed refractory to multiple medication trials, and developed continuous tics with explosive behavioral outbursts, the parents decided to pursue further treatment for catatonia.
Acute treatment of catatonia
At the inpatient psychiatric unit at a university center in another part of the country, Z now 20 years old, was diagnosed with catatonia. Lorazepam was started and titrated up to 18 mg total daily without sedation or respiratory depression, while tapering and stopping all other psychotropics. There was mild to moderate improvement but no return to baseline. The treating physicians recommended a course of bilateral ECT as the next step to which the parents consented. Lorazepam was continued throughout the course, but flumazenil was administered intravenously during the ECT procedure to allow seizure induction. Decreased tics, posturing, aggressive outbursts, and stereotypies were found after 3–4 sessions. He could eat again unassisted with spoon and forks, and was able to shower with minimal prompts. His baseline cognitive abilities returned. He received a total of 12 ECT sessions during the admission. After discharge, arrangements were made for outpatient continuation ECT near the home of the patient.
However, commencement of ECT locally was delayed because of state regulations restricting the use of ECT in people with developmental disorders. While the parents waited for approval of the local courts to start outpatient ECT, the patient relapsed. When he became agitated, aggressive and dehydrated, he was transferred to the emergency mental health treatment center where he was briefly prescribed high-dosage haloperidol. After rehydration, the parents decided to seek treatment at another facility where ECT would be readily available.
Maintenance treatment of catatonia
A second acute course of 20 bilateral ECT treatments on the inpatient unit of the local university hospital again improved Zs condition to a level close to overall baseline functioning. Lorazepam was successfully weaned and no other psychotropics were prescribed. An outpatient maintenance treatment schedule was started consisting of once weekly ECT for the first 3 months followed by once every other week for another 3 months. Z returned to live with his parents and attend an activity center in a local health center. After 6 months, ECT was stopped without immediate recurrence of catatonia. However, during a follow-up visit 4 months later, the parents reported that Z had stopped going to the activity center after an altercation with another patient, had lost weight, and that his speech had slowed considerably. For the next month, ECT was restarted twice a week on an outpatient basis with good results. Over the next six years, similar episodes occurred about once or twice yearly, usually after stressful events. These relapses were aborted each time with outpatient ECT courses of varying frequency and duration. The parents believe that ECT has been essential in allowing Z, now in his late twenties, to continue to live at home, and to maintain an adequate, albeit socially restricted, level of function.
Diagnostic considerations
A diagnosis of catatonia in Z is likely. From the age of 15, Z showed various catatonic symptoms including mutism, stupor, and posturing. The effects of catatonia on activities of daily living, occupational activities, and physiological necessities (eating, drinking, and excretion) varied widely throughout Zs life. At his worst, Z was stuporous, immobile for most of the day, and in need of assistance with food intake, constituting a medical emergency. Indeed, catatonia carries the potential for serious medical morbidity and mortality. This is particularly salient for patients with features of malignant catatonia (fever, altered consciousness, stupor, and autonomic instability as evidenced by lability of blood pressure, tachy- or bradycardia, cardiac arrhythmias, vasoconstriction causing acrocyanosis and diaphoresis) who demand immediate treatment.
Zs symptoms satisfy the criteria for catatonia in autism shown in Table 1, which are modeled after criteria for catatonia in patients without developmental disorders [24]. However, as autistic patients are often mute or have baseline symptoms like echophenomena, stereotypy, negativism, or other psychomotor abnormalities [53], diagnostic criteria specific for catatonia in autism have been proposed in which drastically decreased speech replaces mutism and the duration of symptoms is longer [20]. A rating scale or checklist may aid the quantification of catatonia. Several scales have been published during the last ten years and have been discussed elsewhere [10, 24]. However, these scales have not yet been applied to autistic populations.
Evaluation of catatonia
Possible catatonia should prompt a thorough clinical assessment in any patient, whether typically developing or autistic. Physical examination, laboratory and imaging investigations are dictated by clinical findings. Infectious, metabolic, endocrinological, neurological, and autoimmune diseases have been associated with catatonia and must therefore be ruled out [11, 24]. In one case-report, obsessive-compulsive behaviors and catatonia developed in a child after a streptococcal infection [22] with elevation of Antistreptolysin O and DNAse B antibody titers. The child improved rapidly with lorazepam treatment followed by plasmapheresis. The authors suggest that catatonia, like OCD and tics, may be another manifestation of pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS). The motor manifestations of hypocalcemia, tetanus, strychnine toxicity, and rabies can also mimic catatonia.
All prescribed medications should be evaluated for their potential to induce catatonic symptoms since many medical and psychiatric medications can cause catatonia or catatonia-like conditions [24, 39]. Antipsychotic agents should be promptly discontinued as they are contraindicated in patients who exhibit signs of catatonia because of the reported increased incidence of malignant catatonia or neuroleptic malignant syndrome (NMS) in patients with incipient signs of catatonia. When the catatonia is resolved, antipsychotics, antidepressants, or other psychotropics may be useful for select additional psychiatric diagnoses, but any re-emergence of catatonic symptoms should prompt discontinuation.
Recreational drugs (PCP, mescaline, psilocybin, cocaine, ecstasy, opiates and opioids), disulfiram, steroids, antibiotic agents (ciprofloxacin), baclofen and bupropion have also been associated with the emergence of catatonia in case-reports. Withdrawal of benzodiazepines, gabapentin, and dopaminergic drugs, especially if done rapidly, has precipitated catatonia in some patients [24].
Differential diagnosis
A detailed history, clinical examination, and application of diagnostic criteria must differentiate catatonia from other conditions, syndromes, or disorders featuring psychomotor abnormalities that may overlap with the manifestations of catatonia. Making an adequate differential diagnosis of catatonia is compounded by the fact that there is no diagnostic biological marker of catatonia. The differential of catatonia among other hypokinetic or hyperkinetic conditions is listed in Table 2.
Among the hyperkinetic states, acute dystonia, tardive dyskinesia, withdrawal-emergent dyskinesia, and akathisia are medication-induced conditions that may be mistaken for catatonia. Typical antipsychotics are the medications that are usually associated with these movement disorders, but atypical antipsychotics, tricyclic and tetracyclic antidepressants, selective serotonin-uptake inhibitors, monoamine oxidase inhibitors, antiemetics, calcium-antagonists, anticonvulsants, stimulants, and a variety of other psychotropics have also been implicated through alterations in central dopamine metabolism [34]. As mentioned, antipsychotics may additionally be a risk factor for the development of catatonia itself. Tic disorder, Gilles de la Tourette syndrome, elective mutism, conversion disorder, and compulsions in Obsessive-Compulsive Disorder may also overlap with catatonia [33, 36, 55].
Among the hypokinetic states, parkinsonism is the medication-induced form of Morbus Parkinson both resembling catatonia. Typical antipsychotics are especially prone to cause parkinsonism in dose-dependent fashion, usually within the first month of administration [3].
Malignant Hyperthermia, NMS, toxic serotonin syndrome, delirium, stiff-person syndrome and locked-in syndrome constitute another group of disorders characterized by varying levels of hypokinesis and muscle stiffness, in combination with altered levels of consciousness, that should be included in the differential diagnosis. For example, there is discussion in the literature if NMS and toxic serotonin truly differ in key aspects with catatonia, or alternatively, if they should be regarded as medication-induced forms of catatonia [23, 25]. The fact that NMS and toxic serotonin syndrome seem to respond to the same treatments as catatonia strengthens the argument of relatedness.
Diagnostic rules in DSM-IV state that catatonia should not be diagnosed if occurring exclusively during the course of a delirium while acknowledging that similar medical conditions of infectious, metabolic, endocrine and neurological etiologies are associated with both catatonia and delirium [2]. The validity of this provision is uncertain given the lack of studies in the literature that have assessed the importance of catatonia during delirium. The issue has crucial therapeutic consequences, as anti-catatonic and anti-delirium treatments are different, albeit with overlap. While delirium is typically treated with (typical or atypical) antipsychotics, the emergence of catatonia in delirium may caution against the use of antipsychotic medications due to the aforementioned risk of worsening catatonia with antipsychotics medications [25].
Another unresolved classification issue is whether catatonia should be included in the differential diagnosis in patients with coma (complete unresponsiveness) [32], and, in a similar vein, if stupor or profound unresponsiveness can be the sole presenting symptom of catatonia [6, 27, 32]. Recent case-reports have shown that patients with levels of unresponsiveness similar as in coma, and without other catatonic symptoms (except resistance to eye-opening) responded to ECT [5] and intravenous benzodiazepines [27].
Treatment considerations
Frequently, catatonia in autistic patients becomes chronic [43], like in Zs case, and proves to be largely refractory to most behavioral and psychopharmacological approaches. Recent cases like Z that were treated by the authors suggest that only lorazepam may have consistent positive effects and that both acute and maintenance ECT may be crucial treatments for autistic patients with catatonia. Acute ECT may be imperative to abort lethal catatonia and preserve life, with ongoing usage of ECT necessary to bring the patient closer to his baseline status. There are no large studies on maintenance ECT in catatonia in any psychiatric population. ECT also does seem to have acute, and possibly prophylactic, effects in refractory patients with schizophrenia [54], depressive disorders [44], bipolar disorder [51], Morbus Parkinson [61], and other conditions [46].
To our knowledge, there is only the anecdotal annotation on ECT in autism from O’Gorman in the 1970s [42]: “Electric Shock Treatment does seem to have a definite place in our armamentarium, particularly as a means of cutting short an acutely disturbed episode…Time is short and we must try to avoid the rapid deterioration which tends to occur if such an episode is prolonged. It appears that, in some hands, electric shock treatment is very helpful, but the course of the treatment will often have to be intensive and prolonged. Four or five treatments a week for four or even five weeks may be necessary. It is of course essential that psychotherapeutic measures and individual attention to the child should be increased rather than decreased while electric shock treatment is given. The present writers practice is to employ this treatment only during acutely disturbed phases in older (adolescent) patients”. It is unclear if these adolescents were diagnosed with catatonia or suffered from other comorbid conditions.
Unfortunately, a significant treatment barrier in the usage of ECT in autism concerns the reluctance of parents/family and clinicians to consider ECT as a treatment option in autistic patients once catatonia is diagnosed. Concerns often include fear of “brain damage” and social stigma associated with ECT. Indeed, since Italian psychiatrists Cerletti and Bini conceived ECT in 1938 after von Meduna demonstrated the therapeutic effect of chemically induced seizures in 1934, historical research shows that ECT won wide acceptance until the turbulent 1960s, then started to be cast aside for reasons having more to do with cultural prejudice and urban legends than with safety and efficacy [50]. Misconceptions regarding ECT are rampant in both the medical professional and lay publics. Even with critically ill children, the authors have been frequently asked by parents of autistic children requiring ECT if their children will “become zombies”, suffer intense pain or have further cognitive decline and loss of functional skills.
Legal stipulations may factor into the ease of access to ECT for children, adolescents and adults with autism and other developmental disorders. For example, a few US states have severe restrictions on ECT, often precluding or severely restricting prompt access [31, 59] even in the case of medical emergencies. The authors have worked with patients whose families literally had to cross state lines in order to access life-saving ECT treatment, at considerable expense as well as risk to an ill child not necessarily fit for travel. These legal barriers are often amplified in the case of juveniles or patients with cognitive impairment, particularly as related to concerns of informed consent. ECT providers themselves may be reluctant to assume perceived medico-legal risks associated with providing ECT to minors and adults with developmental disabilities, despite literature supporting safety and efficacy of ECT in the mentally retarded population.
Diagnostic implications
Catatonia should be considered in any autistic patient, of any age, when there is an obvious and marked deterioration in movement, vocalizations, pattern of activities, self-care, and practical skills. Autistic, developmental, and psychiatric disorders associated with catatonia are listed in Table 3.
It follows that autism should also be considered as the underlying condition in patients presenting with catatonia, especially in those with histories of developmental problems. Psychiatrists working with adults are usually much more familiar with schizophrenia and other psychotic disorders than autism. Therefore, catatonia may be misdiagnosed as a feature of schizophrenia, and any underlying diagnosis of autism may be missed leading to possible suboptimal treatment of both catatonia and autism.
Timely diagnosis is paramount to avoid catatonia remaining undiagnosed or untreated for extended periods. Delay typically results in sluggish treatment responses, as well as potential for serious medical complications such as deep vein thrombosis, pulmonary emboli [37, 41], dehydration, malnutrition and physical exhaustion.
Treatment implications
An example of a medical treatment algorithm for severe catatonia based on the cumulative experience in autism [21, 24] is shown in Fig. 3. The lack of controlled studies must be emphasized, as well as the limited number of published cases of catatonia in people with developmental disorders.

Medical treatment algorithm for catatonia in autism
The algorithm features the lorazepam challenge test that consists of intravenous administration of 1 mg of lorazepam, and if no changes occur within the next two to five minutes, repeating the procedure with another 1 mg lorazepam bolus.
If improvement is seen after the challenge test, treatment with increasing doses of lorazepam as high as 24 mg per day is recommended. Improvement should be observed at least after 3 days before considering bilateral ECT. Once the efficacy of lorazepam is demonstrated, a 6–12 months continuation phase starts. Although the usual dose range of 6–24 mg per day is considered “high” in conventional psychopharmacology, such higher doses are necessary (and well tolerated without sedation) in many cases with catatonia. Lorazepam should be slowly tapered after the continuation phase to avoid withdrawal symptoms due to tolerance.
ECT is indicated in severe catatonia when the Lorazepam Challenge Test fails or increased dosages do not bring rapid relief. In such circumstances, ECT may be life saving, and should be promptly considered. A few technical issues concerning electrode placement and concurrent medication use need to be considered to maximize the effect of ECT. Bilateral (bitemporal or bifrontal) electrode placement is more efficacious than unilateral placement, and the use of bilateral placement in catatonia is therefore recommended [24]. All psychiatric medications should be stopped before initiation of ECT, as well as any other non-psychiatric medications, if possible.
The concurrent use of lorazepam and ECT is a useful treatment variant when lorazepam treatment brings benefits but no complete remission or return to baseline function. Intravenous administration of flumazenil, a benzodiazepine antagonist with quick onset of action and short-lived effect, just before the seizure induction temporarily suspends the anti-seizure effects of lorazepam, obviating the tapering or stopping of lorazepam. It is recommended to wait until the patient shows outward signs of agitation after flumazenil administration to guarantee benzodiazepine reversal before delivering the electrical stimulus. In a case-series, synergy of lorazepam and ECT treatment using flumazenil was observed [45].
The relief of catatonia often seems to require more frequent seizures than does the relief of depressive illness. In severe or malignant catatonia, daily ECT treatment for 3–5 days may be needed. The number of sessions that will be needed before substantial improvement or remission occur cannot be predicted, and the authors have worked with some patients requiring several dozen ECT treatments. It seems reasonable to assess the patients overall response after the first five or six treatments, and then again after ten or 12 treatments. The cognitive and non-cognitive side effects of ECT are known and manageable, and typically time-limited [1].
Options for continuation treatment after an effective ECT course may include continuation of lorazepam or ECT on an outpatient basis. Although the optimal duration of treatments to prevent relapse of catatonia is unknown, weekly and bi-weekly ECT treatments may be needed for 6 months or longer to ensure a stabilized response. Like in other conditions, wide differences in treatment needs between patients are to be expected. Fortunately, continued ECT is safe with ongoing monitoring.
Research implications
Findings that catatonia is diagnosable in about one of seven patients diagnosed with autism [7, 58], a proportion similar as in those with affective and psychotic disorders [24] is contrary to earlier claims that catatonia is restricted to schizophrenia, and soon to be extinct [40], and beg the question of clinical and biological overlap between these disorders.
Clinical boundaries between the autistic spectrum disorders and other disorders, particularly early-onset psychotic disorders [29, 52, 57] are not always clear. About 40% of children with onset of schizophrenia before age ten had symptoms of autism during infancy and early childhood [57]. In another study of children with childhood-onset schizophrenia (COS) (before their 13th birthday), 19 of 75 (25%) of children with COS had a lifetime diagnosis of PDD [52]. Two siblings of children with COS were diagnosed with classic autism. This suggests a familial link between certain types of autism and childhood-onset schizophrenia.
Recent studies suggest overlap in genetic causes for autism and major psychiatric syndromes such as affective disorders [15] and schizophrenia [38], and catatonia [12, 18]. Admittedly, genes for any of the autistic, catatonic, affective, or psychotic disorders are yet to be identified. Further studies on the possible biological-genetic overlap between these conditions would be helpful.
References
Abrams R (2002) Electroconvulsive therapy, 4th edn. Oxford University Press, New York
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, 4th edn. American Psychiatric Association, Washington, DC
Ayd F (1961) A survey of drug-induced extrapyramidal reactions. JAMA 175:102–108
Bailine S, Petraviciute S (2007) Catatonia in autistic twins: role of electroconvulsive therapy. J ECT 23:21–22
Bender K, Feutrill J (2000) Comatoid catatonia. Aust NZ J Psychiatry 34:169–170
Benegal V, Hingorani S, Khanna S (1993) Idiopathic catatonia: validity of the concept. Psychopathology 26:41–46
Billstedt E, Gilberg C, Gilberg C (2005) Autism after adolescence: population-based 13- to 22-year follow-up study of 120 individuals with autism diagnosed in childhood. J Autism Dev Disord 35:351–360
Brasic J, Zagzag D, Kowalik S, Prichep L, John E, Liang H, Klurchko B, Cancro R (1999) Progressive catatonia. Psychol Rep 84:239–246
Bumke O (1924) Lehrbuch der Geisterkrankheiten, 2nd edn. Bergmann, Munich
Caroff S, Mann S, Francis A, Fricchione G (2004) Catatonia. From psychopathology to neurobiology. American Psychiatric Publishing, Washington, DC
Carroll B, Goforth H (2004) Medical catatonia. In: Caroff S, Mann S, Francis A, Fricchione G (eds) Catatonia. From psychopathology to neurobiology. American Psychiatric Publishing, Washington DC
Chagnon Y (2006) Shared susceptibility region on chromosome 15 between autism and catatonia. Int Rev Neurobiol 72:165–178
Cohen D (2006) Towards a valid nosography and psychopathology of catatonia in children and adolescents. Int Rev Neurobiol 72:131–147
de Winter C, van Dijk F, Verhoeven W, Dhossche D, Stolker J (2007) Autism and catatonia: successful treatment using lorazepam. A case study. Tijdschr Psychiatr 49:257–261
DeLong R (2004) Autism and familial major mood disorders: are they related? J Neuropsychiatr Clin Neurosci 16:199–213
Dhossche D, Bouman N (1997) Catatonia in an adolescent with Prader–Willi Syndrome. Ann Clin Psychiatry 4:247–253
Dhossche D (1998) Catatonia in autistic disorders (brief report). J Autism Dev Disord 28:329–331
Dhossche D (2004) Autism as early expression of catatonia. Med Sci Monit 10:RA31–39
Dhossche D, Rout U (2006) Are autistic and catatonic regression related? A few working hypotheses involving GABA, Purkinje cell survival, neurogenesis, and ECT. Int Rev Neurobiol 72:55–79
Dhossche D, Shah A, Wing L (2006) Blueprints for the assessment, treatment, and future study of catatonia in autism spectrum disorders. Int Rev Neurobiol 72:267–284
Dhossche D, Wing L, Ohta M, Neumarker K-J (eds) (2006) Catatonia in Autism Spectrum Disorders. Elsevier, San Diego
Elia J, Dell M, Friedman D, Zimmerman R, Balamuth N, Ahmed A, Pati S (2005) PANDAS with catatonia: a case-report. Therapeutic response to lorazepam and plasmapheresis. J Am Acad Child Adolesc Psychiatry 44:1145–1150
Fink M (1995) Recognizing NMS as a type of catatonia. Neuropsychiatry Neuropsychol Behav Neurol 8:75–67
Fink M, Taylor M (2003) Catatonia. A clinician’s guide to diagnosis and treatment. Cambridge University Press, Cambridge
Fink M, Taylor M (2006) Neuroleptic malignant syndrome is malignant catatonia, warranting treatments efficacious for catatonia. Prog Neuropsychopharmacol Biol Psychiatry 30:1182–1183
Fink M, Taylor M, Ghaziuddin N (2006) Catatonia in autistic spectrum disorders: a medical treatment algorithm. Int Rev Neurobiol 72:233–244
Freudenreich O, McEvoy J, Goff D, Fricchione G (2007) Catatonic coma with profound bradycardia. Psychosomatics 48:74–78
Ghaziuddin M, Quinlan P, Ghaziuddin N (2005) Catatonia in autism: a distinct subtype? J Intellect Dis Res 49:102–105
Green W, Campbell M, Hardesty A, Grega D, Padron-Gayol M, Shell J, Erlenmeyer-Kimling L (1984) A comparison of schizophrenic and autistic children. J Am Acad Child Psychiatry 23:399–409
Hare D, Malone C (2004) Catatonia and autism spectrum disorders. Autism 8:183–195
Harris V (2006) Electroconvulsive therapy: administrative codes, legislation, and professional recommendations. J Am Acad Psychiatry Law 34:406–411
Hem E, Andreassen O, Robasse J-M, Vatnaland T, Opjodsoen S (2005) Should catatonia be part of the differential diagnosis of coma? Nord J Psychiatry 59:528–530
Hermesh H, Hoffnung R, Aizenberg D, Molcho A, Munitz H (1989) Catatonic signs in severe obsessive compulsive disorder. J Clin Psychiatry 50:303–305
Jimenez-Jimenez F, Garcia-Ruiz P, Molina J (1997) Drug-induced movement disorders. Drug Saf 16:180–204
Kakooza A, Stoppelbein L, Dhossche D (2006) Psychosis in autism. In: Fujii D, Ahmed I (eds) The spectrum of psychotic disorders: neurobiology, etiology & pathogenesis. Cambridge University Press, Cambridge, pp 233–246
Karadenizli D, Dilbar N, Bayam G (2005) Gilles de la Tourette Syndrome Response to Electroconvulsive Therapy. J ECT 21:246–248
Lachner C, Sandson N (2003) A case of catatonia-induced deep venous thrombosis. Psychosomatics 44:512–414
Larsson H, Eaton W, Madsen K, Vestergaard M, Olesen A, Agerbo E, Schendel D, Thorsen P, Mortensen P (2005) Risk factors for autism: perinatal factors, parental psychiatric history, and socioeconomic factors. Am J Epidemiol 161:1–10
Lopez-Canino A, Francis A (2004) Drug-induced catatonia. In: Caroff S, Mann S, Francis A, Fricchione G (eds) Catatonia. From psychopathology to neurobiology. American Psychiatric Publishing, Washington DC
Mahendra B (1981) Where have all the catatonics gone? (editorial). Psychol Med 11:669–671
McCall W, Mann S, Shelp F, Caroff S (1995) Fatal pulmonary embolism in the catatonic syndrome: two case reports and a literature review. J Clin Psychiatry 56:21–25
O’ Gorman G (1970) The nature of childhood autism, 2nd edn. Butterworths, London
Ohta M, Kano Y, Nagai Y (2006) Catatonia in individuals with autism spectrum disorders in adolescence and early adulthood: a long-term prospective study. Int Rev Neurobiol 72:41–54
Petrides G, Dhossche D, Fink M, Francis A (1994) Continuation ECT: relapse prevention in affective disorders. Convuls Ther 10:189–194
Petrides G, Divadeenam KM, Bush G, Francis A (1997) Synergism of lorazepam and electroconvulsive therapy in the treatment of catatonia. Biol Psychiatry 42:375–381
Rabheru K, Persad E (1997) A review of continuation and maintenance electroconvulsive therapy. Can J Psychiatry 42:476–484
Realmuto G, August G (1991) Catatonia in autistic disorder: a sign of comorbidity or variable expression. J Autism Dev Disord 21:517–528
Schieveld J (2006) Case reports with a child psychiatric exploration of catatonia, autism, and delirium. Int Rev Neurobiol 72:195–206
Shah A, Wing L (2006) Psychological approaches to chronic catatonia-like deterioration in autism spectrum disorders. Int Rev Neurobiol 72:245–264
Shorter E, Healy D (2007) Shock therapy: a history of electroconvulsive treatment in mental illness. Rutgers University Press/University of Toronto Press, Piscataway
Sienaert P, Peuskens J (2006) Electoconvulsive therapy: an effective therapy of medication-resistent bipolar disorder. Bipol Disord 8:304–306
Sporn A, Addington A, Gogtay N, Ordonez A, Gornick M, Clasen L, Greenstein D, Tossell J, Gochman P, Lenane M, Sharp W, Straub R, Rapaport J (2004) Pervasive developmental disorder and childhood-onset schizophrenia: comorbid disorder or a phenotypic variant of a very early onset illness? Biol Psychiatry 55:989–994
Stoppelbein L, Greening L, Kakooza A (2006) The importance of catatonia and stereotypies in autistic spectrum disorders. Int Rev Neurobiol 72:103–118
Suzuki K, Awata S, Takano T, Ebina Y, Iwasaki H, Matsuoka H (2005) Continuation electroconvulsive therapy for relapse prevention in middle-aged and elderly patients with intractable schizophrenia. Psychiatry Clin Neurosci 59:481–489
Trivedi H, Mendelowitz A, Fink M (2003) Gilles de la Tourette form of catatonia: response to ECT. J ECT 19:115–117
Wachtel L, Kahng S, Dhossche D, Cascella N, Reti I (2008) ECT for catatonia in an autistic girl. Am J Psychiatry 165:329–333
Watkins J, Asarnow R, Tanguay P (1988) Symptom development in childhood onset schizophrenia. J Child Psychol Psychiatry 29:865–878
Wing L, Shah A (2000) Catatonia in autistic spectrum disorders. Br J Psychiatry 176:357–362
Winslade W, Liston E, Ross J, Weber K (1984) Medical, Judicial, and Statuatory Regulations of ECT in the United States. Am J Psychiatry 141:1349–1355
Zaw F, Bates G, Murali V, Bentham P (1999) Catatonia, autism, and ECT. Dev Med Child Neurol 41:843–845
Zervas I, Fink M (1991) ECT for refractory Parkinson’s disease. Convuls Ther 7:222–223
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kakooza-Mwesige, A., Wachtel, L.E. & Dhossche, D.M. Catatonia in autism: implications across the life span. Eur Child Adolesc Psychiatry 17, 327–335 (2008). https://doi.org/10.1007/s00787-008-0676-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-008-0676-x