
Abstract
Objectives
This study aimed to compare the efficacy of silver nanoparticles (AgNPs) irrigating solution alone and following activation with photon-induced photoacoustic streaming (PIPS), photodynamic therapy (PDT) with indocyanine green (ICG), passive ultrasonic irrigation (PUI), and manual dynamic activation (MDA) method for elimination of Enterococcus faecalis (E. faecalis) from the root canal system.
Materials and methods
A total of 59 extracted human single-rooted teeth were collected and prepared. E. faecalis was inoculated into the root canals and incubated for 4 weeks. The teeth were then randomly divided into five experimental groups (n = 10): the AN group, irrigation with AgNPs alone; the AN/ICG/DL group, irrigation with AgNPs and ICG, then activation with diode laser; the AN/PIPS group, irrigation with AgNPs and activation with 0.3 W Er: YAG laser; the AN/MDA group, irrigation with AgNPs and activation with tapered gutta-percha; and the AN/PUI group, irrigation with AgNPs and activation with ultrasonic. Also, two control groups of irrigation with 2.5% sodium hypochlorite (n = 5) and no intervention (n = 4) were also used. Samples were collected from the dentinal chips before and after the intervention, and the percentage of reduction in colony count was calculated.
Results
A significant reduction in E. faecalis colony count was noted in all groups (P < 0.05). Maximum reduction in colony count was noted in AN/PIPS and AN/PUI groups by 91.03 and 91.29%, respectively. Minimum reduction was noted in the AN group alone.
Conclusion
Activation with PUI and PIPS enhanced the efficacy of AgNPs irrigating solution for elimination of E. faecalis from the root canal system.
Clinical relevance
AgNPs activated by ultrasound or PIPS can be used as an adjunct for disinfection of the root canal system in endodontic treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The success of root canal treatment is largely dependent on the elimination of harmful microorganisms and primarily bacteria from the root canal system [1]. However, the conventional method of chemo-mechanical root canal preparation cannot completely eliminate the bacteria from the root canal system [2,3,4]. The reason includes the complex anatomy and morphology of the root canal system due to the presence of isthmuses, accessory canals, and deltas. The bacteria, debris, and necrotic tissues in these inaccessible areas are hard to be treated. Furthermore, mechanical instrumentation of the root canal system has some shortcomings such as the formation of smear layer and dentinal debris, risk of iatrogenic accidents, and weakening of the root canal dentinal walls [2, 4,5,6].
Enterococcus faecalis (E. faecalis) is among the most commonly isolated bacteria from the root canals which failed endodontic treatment. This Gram-positive coccus is a facultative anaerobe that can survive in anaerobic conditions [5]. E. faecalis in the form of biofilm produces an extracellular polysaccharide matrix, which is much more resistant than the planktonic bacteria when exposed to disinfecting agents and other antimicrobial modalities [7]. The bacterial biofilm can also resist the host immune system and provide nutrients for the bacteria. In the form of biofilm, the bacteria can remain viable and even proliferate for a long time at low pH and high temperature and in endodontically treated teeth [5, 8, 9].
Sodium hypochlorite (NaOCl) is the most popular irrigating solution due to its optimal disinfecting property and dissolution of necrotic debris. However, its main shortcomings include cytotoxicity and metal corrosion. Other drawbacks include bad taste and odor; risk of injury to the eye, skin, and mucosa; airway sensitivity and obstruction; and risk of NaOCl accident. Also, the elastic modulus and flexural strength of dentin depend on the concentration and duration of exposure to NaOCl [6, 10, 11]. Therefore, new antimicrobial agents and novel anti-biofilm strategies are required to increase the success rate of root canal treatment [7, 9]. Among different nano-materials, nano-silver is more commonly used in the dental market [12]. Nano-silver is highly toxic for bacteria, while it is safe for human cells and tissues, except in very high concentrations [10, 12, 13]. It is also used for root canal disinfection in endodontic treatment to prevent microbial growth and infection in the root canal system. It can eliminate 650 pathogenic microorganisms including E. faecalis [5, 12]. Considering the suboptimal efficacy of the conventional root canal irrigation methods, some techniques are employed to activate the irrigating solution in the root canal system and increase its disinfection efficacy.
In passive ultrasonic activation (PUI), a file is used to induce high-frequency (25–40 KHz) and low-spectrum vibrations in the root canal system and create bubbles in the irrigating solution in the root canal system with negative and positive pressure. These bubbles are unstable and eventually rupture and then create a stream in the liquid. Evidences show that ultrasonic (US) activation of NaOCl increases its solubility, disinfection efficacy, and elimination of organic and inorganic debris [3, 14, 15].
Photodynamic therapy (PDT) is a novel technique [15] that involves the use of a photosensitizer attached to the bacteria in the root canals and its reaction with light in the presence of oxygen. The photosensitizer is activated by light and releases its energy via production of oxygen. The released oxygen becomes activated and damages the bacterial cell wall. This method is capable of eliminating bacteria, viruses, fungi, and protozoa, while it is safe for the host tissue. However, direct use of NaOCl and antibiotic therapy is toxic for the host. The infrared wavelength has higher penetration into tissues when compared with other wavelengths. Moreover, lasers at this wavelength have the greatest capability for elimination of E. faecalis [5, 15, 16]. Indocyanine green (ICG) is a new photosensitizer used in PDT. It has advantages such as low toxicity for the host tissue, greater penetration than infrared radiation, optimal efficacy for elimination of bacteria and fungi, and powerful photosensitized cellular damage [5, 15, 16].
In another technique known as photo-induced photoacoustic streaming (PIPS), Er/YAG laser with low level of energy and short duration is irradiated with a tapered and stripped tip. In this technique, the PIPS tip is placed in the pulp chamber at the orifice and Er/YAG laser is irradiated. The primarily generated heat is absorbed by the water molecules and increases their temperature to the boiling point. The molecules are then converted to vapor. When ruptured, the energy of bubbles is converted to mechanical energy in the liquid medium. In other words, the energy of a bubble that ruptures concentrates at a point and causes cavitation. Each impulse causes serial shock waves that eventually create a strong stream in the irrigating solution in the root canal. Since the tip is positioned at the orifice, there is no need to flare the canal to allow introduction of instrument to the apical region. This technique eliminates the viable and necrotic tissues and bacteria from the root canal system and disinfects the dentinal tubules [6, 15,16,17]. This method is more effective than the conventional irrigation of the root canal for elimination of the smear layer, debris, intracanal medicaments, and bacteria from the root canal walls. In addition, it increases the bond strength of resin cement and sealer to the root canal walls [6, 16,17,18]. The main advantage of this method is that heat is not generated in the root canal dentin. Also, the laser tip is positioned at the canal orifice in the pulp chamber and does not require introduction into the root canal system [16,17,18].
Mechanical activation is among the simplest techniques for manual activation of root canal irrigating solutions. This is done by the use of gutta-percha (GP), hand files, or endodontic brushes. Manual activation of irrigating solution can be helpful for the elimination of the smear layer [15, 19].
To the best of the authors’ knowledge, no previous study has compared the efficacy of these different systems for activation of silver nanoparticles (AgNPs) for elimination of E. faecalis. Thus, the present study aimed to assess the effect of ultrasound, PIPS, PDT, and manual activation of AgNPs disinfecting solution on its antibacterial efficacy against E. faecalis.
Materials and methods
Preparation of teeth
The study protocol was approved by the ethics committee of the Tehran University of Medical Sciences (REC.1396.4358). A total of 59 single-rooted, single-canal human permanent teeth that had been extracted due to periodontal disease or orthodontic treatment and did not have open apex, resoprtion, fracture, caries, or previous endodontic treatment were evaluated in this study. Having one single canal was ensured by taking radiographs in mesiodistal and buccolignual directions. For the purpose of standardization, the roots were cut at 16 mm from the apex using a fissure diamond bur perpendicular to the longitudinal axis of the tooth. Working length was considered 1-mm short of the apical foramen. All teeth were instrumented using rotary ProTaper system (Dentsply Maillefer, Ballaigues, Switzerland). S1, S2, F1, F2, and F3 files were used in an orderly fashion, along with the use of RC-Prep (DiaDent, Almere, Netherlands). In between the use of rotary files, the root canals were rinsed with 1 mL of 2.5% NaOCl using a 30-gauge needle (Luerlock, Avapezeshk, Tehran, Iran). After root canal preparation with files, the smear layer was eliminated by using 1 mL of 17% EDTA (Master-Dent, Bristol, UK), 5 mL of saline, and 1 mL of 2.5% NaOCl, each for 3 min using a 30-gauge needle 1 mm short of the working length. Next, all canals were rinsed with 5 mL of saline solution.
The apical foramen of all teeth was sealed with glass ionomer (Willmann & Pein GmbH, Hamburg, Germany) in order to inhibit the passage of irrigating solution and bacteria through it. The entire tooth surface, except for the orifice, was coated with two layers of nail varnish, and the teeth were autoclave-sterilized at 121 °C for 15 min.
Bacterial culture
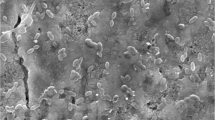
Standard-strain E. faecalis (American Type Culture Collection 29212) was added to 5 mL of brain heart infusion (BHI) broth (33 g/L; Merck, Darmstadt, Germany) and incubated at 37 °C for 24 h. Next, 100 μL of sterile BHI and 30 μL of culture medium containing 109 colony forming units (CFUs) of E. faecalis were added to sterile root canals in the microtubes. The teeth were incubated at 37 °C for 4 weeks, and every 3 days, 30 μL of the BHI suspension containing bacteria was aspirated and replaced with fresh BHI under sterile conditions. To confirm biofilm formation under these experimental conditions, one root was selected randomly and was prepared and analyzed by scanning electron microscopy (SEM).
Primary sampling
The teeth were removed from the microtube using a sterile gauze, and BHI broth was aspirated from the root canal system using a sterile 30-gauge needle. The root canal was then rinsed with 3 mL of sterile saline for 30 s. The teeth were then vortexed for 30 s. Next, a #40 paper point (DiaDent, Almere, Netherlands) was placed in the root canal for 30 s and was then transferred to a microtube containing 1 mL of saline and vortexed for 30 s.
Next, 10-fold serial dilution up to 1:100 was prepared, and 100 μL of each dilute was cultured on blood agar plate (30 g/L distilled water in 50 mL of sheep blood). After 24 h, the number of colonies was counted and converted to actual value using the dilution factor. The mean of actual number of colonies between 1:10 and 1:100 dilutions was calculated.
Experiment
The samples were randomly divided into five experimental (n = 10) and two control groups as follows:
-
1.
Group AN: The root canals were rinsed with 5 mL of AgNPs for 1 min and it remained in the canal for 4 min.
-
2.
Group AN/ICG/DL: The root canals were rinsed with 5 mL of AgNPs suspension plus 1 mL of ICG (1 mg/mL) (Green +I, Novateb Pars, Iran) in 1:1 ratio for 1 min. It remained in the canal for 3 min and was then irradiated with diode laser (Konftec, Taiwan) with 250 mW power and 808 nm wavelength in continuous-wave mode for 60 s.
-
3.
Group AN/PIPS: The crown was reconstructed with a thin layer of Filtek Z250 composite (3 M, Bracknell, UK) for all teeth in this group. The root canals were rinsed with 5 mL of AgNPs for 1 min, and then the tip of the Er/YAG (LightWalker AT, Fotona, Ljubljana-Slovenia) (20 mJ, 15 Hz, 0.3 w, 50 microseconds) was located in the pulp chamber space and radiated for 30 s, and AgNPs were remained in the canal for 3 min and 30 s.
-
4.
Group AN/MDA: The root canals were rinsed with 5 mL of AgNPs for 1 min, which was then agitated by the pull and push motions of F2 GP to the working length for 4 min (around 60 times).
-
5.
Group AN/PUI: The root canals were rinsed with 1 mL of AgNPs for 30 s, which was then activated with size 20 ultrasonic file with power 4 to 1 mm short of the working length for 30 s. This was repeated for five cycles.
*Root canal irrigation in all groups was performed using a 30-gauge needle to 1 mm short of the working length. AgNPs (Mehreganchem, Tehran, Iran) used in the groups had 100 ppm concentration, and the mean diameter of its particles was 30 nm.
Control groups
-
6.
Group control (+) (n = 5): The root canals were rinsed with 5% NaOCl for 1 min. It was remained in the canal for 4 min and then 1 mL of 5% sodium thiosulfate was used for 30 s using a 30-gauge needle to neutralize the hypochlroite.
-
7.
Group control (−) (n = 4): No intervention was performed in this group.
Final sampling
For the purpose of standardization of the groups, the root canals were rinsed with 3 mL of sterile saline for 30 s. Next, a #40 Hedstrom file (Mani Inc., Tochigi, Japan) was used to file all canal walls circumferentially to the working length. A #40 paper point was placed in the canal for 30 s and then the Hedstrom file along with the paperpoint were placed in a microtube containing 1 mL of saline and vortexed for 30 s. The rest of the procedures were conducted in the same way as those described for primary sampling.
Statistical analysis
Data were analyzed using SPSS version 25 (SPSS Inc., IL, USA). The percentage of change in CFUs in each group was calculated and reported descriptively as the mean and standard deviation values. For inferential analysis, the percentage of reduction in CFUs was compared among the five study groups using one-way ANOVA. Since the result was significant, pairwise comparisons were performed using the Games-Howell test. Level of significance was set at 0.05.
Results
One-way ANOVA showed a significant reduction in colony count after the intervention when compared with baseline in all experimental groups (P < 0.05). Table 1 shows the colony count before and after the intervention and the percentage of reduction (RCC%). The maximum percentage of reduction in colony count among experimental groups was noted in AN/PIPS and AN/PUI with very close values, and the minimum was noted in AN group. A significant difference was noted between AN/PUI and AN/PIPS groups versus AN group (P < 0.05), but no other significant differences were noted in experimental groups (P > 0.05). Among the control groups, control (+) group showed the maximum percentage of reduction (100%), and control (−) not only did not have any reduction in result but also showed biofilm proliferation after the procedure. Thus, all the experimental groups had significant differences with both of the control groups (Table 1).
Discussion
E. faecalis is among the most common bacteria present in the root canal system. It is resistant to antibacterial agents, phagocytosis, and antibodies due to its ability to form biofilm [5]. The incubation time of E. faecalis has a direct effect on the structure and resistance of its biofilm. In the first 1 h after incubation, it mainly has a planktonic state and then starts to form a biofilm. It is sensitive to antibacterial agents such as 1% NaOCl, 2% chlorhexidine, and 0.2 and 0.4% iodine at 2 weeks. However, it becomes highly resistant to these agents after 3 weeks. Thus, we considered a 4-week incubation time for E. faecalis in this study [6].
In the current study, 5% NaOCl was used as a positive control group and demonstrated a powerful antibiofilm effect against E.faecalis biofilm. It is in agreement with the results reported earlier where NaOCl was recognized as the most efficient irrigating solution in various concentration in order to biofilm destruction [20,21,22].
At present, AgNPs are extensively used as antibacterial agents for the treatment of root canal infections and due to their very small size, such nano-materials can enter into dentinal tubules with 2.4–2.9 μm diameter. Evidences show that the antibacterial efficacy of AgNPs against E. faecalis and Staphylococcus aureus is comparable to that of 5.25% NaOCl and can help control bacterial growth in the root canal system [23, 24]. These particles have a positive charge, and their mechanism of action is via reaction with sulfonyl groups present in proteins and DNA. They open the DNA sequence and thus prevent its transcription and expression of ribosomes and by doing so interfere in the energy transfer cycle and cell mitosis. They also cause permeability of bacterial membrane and leakage of cell contents and its subsequent lysis and destruction [5, 24]. Evidence shows that silver has antibacterial properties against a wide spectrum of bacteria and even mature biofilms [10]. Afkhami et al. [5] used 5 mL of 100 ppm AgNPs for 5 min and reported results similar to the use of 2.5% NaOCl in reduction of E. faecalis in the root canal system. Hirashi et al. [25] used 3.8% Ag (Na3)2F and 5.25% NaOCl in the root canal for 60 min and reported similar results. Bo et al. [26] used the methyl thiazolyl tetrazolium assay and confocal laser scanning microscopy and showed that 0.1 and 0.2% nanosilver gel can be much more effective than camphorated phenol and chlorhexidine against E. faecalis. Such promising results call for further studies on this material to achieve maximum root canal disinfection by AgNPs.
Activation of irrigating solution enhances its efficacy and dynamic flow and improves its antibacterial property [27].
The simplest method for activation of irrigating solution is the manual technique that increases the longitudinal (corono-apical) and lateral penetration of liquid into the root dentinal tubules [27]. A previous study [28] reported that during activation of irrigating solutions with the manual dynamic agitation (MDA) technique, GP should have a size and taper similar to the size and taper of the root canal. When the GP is introduced into the canal to the working length, agitation of air bubbles in the apical third of the canal can be ensured. Hence, increased liquid flow at the apical third increases the penetration depth of irrigating solution and its refreshment. This would result in enhanced debridement of the root canal system [15, 27]. A previous study [27] used tapered GP in the canal and concluded that the distance between the GP cone and the canal wall (reflux space) is effective for activation of irrigating solution and its penetration. This suggests that the smaller this distance, and the thinner the liquid that flows between these two surfaces, the higher the hydrodynamic effect would be. In contrast, other studies [29, 30] stated that when GP adapts to the root canal wall, it prevents the flow of the irrigating solution. When GP is removed from the canal, debris remains in the root canal system. A previous study showed that MDA and sonic activation techniques were more effective than the RinseEndo technique in elimination of smear layer from the apical third of curved canals [31]. A recent study evaluating different irrigation activation methods showed that the groups of Er/YAG and PUI had the most bacterial elimination fallowed by PDT, while the standard needle irrigation had the lowest performance among the tested methods [32]. In contrast, another study [33] reported that the MDA was more effective for smear layer removal than the PUI and needle irrigation methods. Similarly, in the present study, significant reduction in bacterial count of the canal (71.94% reduction in bacterial count) was noted after the use of F2 GP.
Previous studies have shown that US is an adjunct that causes cavitation and acoustic streaming in the root canal irrigating solution which increases both the flushing action of the irrigant and increases its efficacy for elimination of organic and inorganic debris [15, 34, 35]. Accordingly, several studies have reported a reduction in the number of viable colonies after the use of US activation. The hydrodynamic effect increases the efficacy of activation of irrigating solution and has a heating effect that can increase the root canal temperature to 45 °C [15, 34, 35]. Cameron [36] and Al-Jadaa et al. [37] demonstrated that PUI increases the temperature of root canal and also increases the effectiveness of NaOCl as an irrigant. Our results reported greater reduction in bacterial count in AN/PUI group when compared with AN/MDA group (92 and 71%, respectively). Ahmad et al. [38] showed that PUI creates continuous flow of the irrigating solution in the canal around the file, which causes shear stress and damages the biological cells in the root canal. Macedo et al. [39] further showed that activation with US and laser increases the efficacy of NaOCl. Caputa et al. [40] in their review study demonstrated that almost all clinical and in vitro studies have reported higher efficacy of US activation when compared with irrigation with syringe alone. Our results were in line with their findings and indicated the higher efficacy of PUI than all other methods for the elimination of E. faecalis biofilm from the root canal system.
PDT is another activation technique that can be used along with the conventional method. ICG has gained special attention as a new photosensitizer, which is activated by 810 nm wavelength infrared [5]. Beltes et al. [41] evaluated the efficacy of PDT with 1 W and 0.5 W diode laser with 808 nm wavelength and 60 s irradiation time for each sample (3 cycles, 20 s each) and 100 μg/mL ICG for elimination of planktonic E. faecalis. A significant reduction in bacterial count was noted in the PDT group. Moreover, complete elimination of bacteria was noted when NaOCl was used either alone or along with PDT. Pourhajibagher et al. [42] evaluated the effect of PDT with curcumin (40 mA) and 100 μg/mL ICG as photosensitizers for the elimination of E. faecalis when compared with the conventional endodontic irrigating solutions (chlorhexidine and NaOCl). They reported that maximum percentage of reduction in bacterial count was noted in ICG/PDT and curcumin/PDT groups which were further rinsed with NaOCl and chlorhexidine. They found no significant difference between these groups and irrigation with NaOCl and chlorhexidine alone. Afkhami et al. [5] evaluated the effect of PDT with 810 nm diode laser and 1 mg/mL ICG and 100 ppm AgNPs for the elimination of E. faecalis. They reported a significant reduction in bacterial count in diode laser/ICG/AgNPs group, while minimum reduction was noted in diode laser/ICG group without AgNPs. In our study, 70.77% reduction in bacterial biofilm of the root canal system was noted in AN/ICG/DL group. The efficacy of AN/ICG/DL group in the present study was lower than that of AN/PIPS and AN/PUI groups, but it was more effective than the AN/MDA group or AN group, although these differences were not statistically significant.
The PIPS technique is based on photo-acoustic shock wave and photo-mechanical principles [15]. Ordinola-Zapata et al. [18] evaluated the effect of PIPS along with 6% NaOCl with PUI, sonic and ultrasonic methods and the conventional method combined with 6% NaOCl. They observed significant elimination of bacterial biofilm from the infected dentin of the canal in the PIPS group. A review article of Mohammadi et al. [16] showed that cleaning and irrigating of the root canal with the conventional method after 20 min resulted in disinfection of 83% of the canal. In contrast, application of PIPS after 1 min of irrigation with the same solution caused 100% disinfection. Akcay et al. [17] evaluated the efficacy of conventional canal irrigation, Er/YAG-PIPS, ER/YAG-Preciso, PUI, and sonic techniques to assess the penetration depth of irrigating solutions into the dentinal tubules. They observed that Er/YAG-PIPS significantly enhanced the penetration of irrigating solution into the tubules. Ultrasound and sonic ranked second and third, respectively, in terms of efficacy. Also, this penetration in the coronal region was greater than that in the middle and apical regions. Most previous studies have confirmed the efficacy of PIPS for the elimination of microorganisms from the root canal system. The same result was obtained in the present study since AN/PIPS and AN/PUI groups in our study showed greater reduction in bacterial count compared with other groups. However, this difference was only significant when compared with the AN group.
Conclusion
Within the limitations of this in vitro study, the results showed that activation with PUI and PIPS enhanced the efficacy of AgNPs irrigating solution for elimination of E. faecalis from the root canal system. MDA and PDT showed superior antibacterial activity when compared with the use of AgNPs irrigating solution without activation, and also MDA group resulted better reduction than PDT, although these differences were not statistically significant. Clinical application of the results of this in vitro study requires their further confirmation by other in vitro as well as in vivo studies.
Change history
05 January 2022
A Correction to this paper has been published: https://doi.org/10.1007/s00784-021-04351-3
References
Javidi M, Zarei M, Afkhami F (2011) The antibacterial effect of calcium hydroxide on intraluminal and intratubular nterococcus faecalis. Iran Endod J 6(3):1036
de Gregorio C, Estevez R, Cisneros R, Heilborn C, Cohenca N (2009) Effect of EDTA, sonic, and ultrasonic activation on the penetration of sodium hypochlorite into simulated lateral canals: an in vitro study. J Endod 35(6):8915
Kanumuru PK, Sooraparaju SG, Konda KR, Nujella SK, Reddy BK, Penigalapati SR (2015) Comparison of penetration of irrigant activated by traditional methods with a novel technique. J Clin Diagn Res 9(11):ZC447
Neelakantan P, Cheng CQ, Mohanraj R, Sriraman P, Subbarao C, Sharma S (2015) Antibiofilm activity of three irrigation protocols activated by ultrasonic, diode laser or Er:YAG laser in vitro. Int Endod J 48(6):60210
Afkhami F, Akbari S, Chiniforush N (2017) Entrococcus faecalis elimination in root canals using silver nanoparticles, photodynamic therapy, diode laser, or laser-activated nanoparticles: an in vitro study. J Endod 43(2):27982
Golob BS, Olivi G, Vrabec M, El Feghali R, Parker S, Benedicenti S (2017) Efficacy of photon-induced photoacoustic streaming in the reduction of nterococcus faecalis within the root canal: different settings and different sodium hypochlorite concentrations. J Endod 43(10):17305
Wang D, Shen Y, Ma J, Hancock REW, Haapasalo M (2017) Antibiofilm ffect of D-enantiomeric eptide lone and ombined with EDTA n itro. J Endod 43(11):18627
Betancourt P, Merlos A, Sierra JM, Camps-Font O, Arnabat-Dominguez J, Vinas M (2019) Effectiveness of low concentration of sodium hypochlorite activated by Er,Cr:YSGG laser against Enterococcus faecalis biofilm. Int Endod J 34(2):24754
Ghorbanzadeh A, Fekrazad R, Bahador A, Ayar R, Tabatabai S, Asefi S (2018) Evaluation of the antibacterial efficacy of various root canal disinfection methods against nterococcus faecalis biofilm. An ex-vivo study. Photodiagnosis Photodyn Ther 24:4451
Gomes-Filho JE, Silva FO, Watanabe S, Cintra LTA, Tendoro KV, Dalto LG et al (2010) Tissue reaction to silver nanoparticles dispersion as an alternative irrigating solution. J Endod 36(10):1698702
Spencer HR, Ike V, Brennan PA (2007) Review: the use of sodium hypochlorite in endodontics—potential complications and their management. Br Dent J 202(9):555
Takamiya AS, Monteiro DR, Bernabé DG, Gorup LF, Camargo ER, Gomes-Filho JE (2016) In vitro and in vivo toxicity evaluation of colloidal silver nanoparticles used in endodontic treatments. J Endod 42(6):95360
Farshad M, Abbaszadegan A, Ghahramani Y, Jamshidzadeh A (2017) Effect of Imidazolium-based silver nanoparticles on root dentin roughness in comparison with three common root anal irrigants. Iran Endod J 12(1):836
Merino A, Estevez R, de Gregorio C, Cohenca N (2013) The effect of different taper preparations on the ability of sonic and passive ultrasonic irrigation to reach the working length in curved canals. Int Endod J 46(5):42733
Plotino G, Cortese T, Grande NM, Leonardi DP, Di Giorgio G, Testarelli L et al (2016) New technologies to improve root canal disinfection. Braz Dent J 27(1):38
Mohammadi Z, Jafarzadeh H, Shalavi S, Palazzi F (2017) Recent advances in oot anal disinfection: review. Iran Endod J 12(4):4026
Akcay M, Arslan H, Mese M, Durmus N, Capar ID (2017) Effect of photon-initiated photoacoustic streaming, passive ultrasonic, and sonic irrigation techniques on dentinal tubule penetration of irrigation solution: a confocal microscopic study. Clin Oral Investig 21(7):220512
Ordinola-Zapata R, Bramante CM, Aprecio RM, Handysides R, Jaramillo DE (2014) Biofilm removal by 6% sodium hypochlorite activated by different irrigation techniques. Int Endod J 47(7):65966
Andrabi SM, Kumar A, Zia A, Iftekhar H, Alam S, Siddiqui S (2014) Effect of passive ultrasonic irrigation and manual dynamic irrigation on smear layer removal from root canals in a closed apex in vitro model. J Investig Clin Dent 5(3):18893
Del Carpio-Perochena AE, Bramante CM, Duarte MA, Cavenago BC, Villas-Boas MH, Graeff MS et al (2011) Biofilm dissolution and cleaning ability of different irrigant solutions on intraorally infected dentin. J Endod 37(8):11348
Rodrigues CT, de Andrade FB, de Vasconcelos LRSM, Midena RZ, Pereira TC, Kuga MC et al (2018) Antibacterial properties of silver nanoparticles as a root canal irrigant against Enterococcus faecalis biofilm and infected dentinal tubules. Int Endod J 51(8):90111
Wu D, Fan W, Kishen A, Gutmann JL, Fan B (2014) Evaluation of the antibacterial efficacy of silver nanoparticles against enterococcus faecalis biofilm. J Endod 40(2):28590
Bukhari S, Kim D, Liu Y, Karabucak B, Koo H (2018) Novel endodontic disinfection approach using catalytic nanoparticles. J Endod 44(5):80612
Shrestha A, Kishen A (2016) Antibacterial nanoparticles in Endodontics: review. J Endod 42(10):141726
Hiraishi N, Yiu CK, King NM, Tagami J, Tay FR (2010) Antimicrobial efficacy of 3.8% silver diamine fluoride and its effect on root dentin. J Endod 36(6):10269
Bo D, Kayombo CM (2014) Effect of Nanosilver el, Chlorhexidine Gluconate, and amphorated phenol on enterococcus faecalis biofilm. Int Sch Res Notices 2014:380278
Jiang LM, Lak B, Eijsvogels LM, Wesselink P, van der Sluis LW (2012) Comparison of the cleaning efficacy of different final irrigation techniques. J Endod 38(6):83841
Saber SE-D, Hashem AAR (2011) Efficacy of different final irrigation activation techniques on smear layer removal. J Endod 37(9):12725
Parente J, Loushine R, Susin L, Gu L, Looney SW, Weller R et al (2010) Root canal debridement using manual dynamic agitation or the EndoVac for final irrigation in a closed system and an open system. Int Endod J 43(11):100112
Susin L, Liu Y, Yoon JC, Parente JM, Loushine RJ, Ricucci D (2010) Canal and isthmus debridement efficacies of two irrigant agitation techniques in a closed system. Int Endod J 43(12):107790
Caron G, Nham K, Bronnec F, Machtou P (2010) Effectiveness of different final irrigant activation protocols on smear layer removal in curved canals. J Endod 36(8):13616
Aydin SA, Taşdemir T, Buruk CK, Çelik D (2020) Efficacy of Erbium, Chromium-doped Yttrium, Scandium, Gallium and Garnet Laser-activated Irrigation Compared with Passive Ultrasonic Irrigation, Conventional Irrigation, and Photodynamic Therapy against Enterococcus faecalis. J Contemp Dent Pract 21(1):12
Ahuja P, Nandini S, Ballal S, Velmurugan N (2014) Effectiveness of four different final irrigation activation techniques on smear layer removal in curved root canals: a scanning electron microscopy study. J Dent (Tehran) 11(1):19
Neuhaus KW, Liebi M, Stauffacher S, Eick S, Lussi A (2016) Antibacterial efficacy of a new sonic irrigation device for oot anal disinfection. J Endod 42(12):1799803
Plotino G, Pameijer CH, Grande NM, Somma F (2007) Ultrasonics in endodontics: a review of the literature. J Endod 33(2):8195
Cameron JA (1988) The effect of ultrasonic endodontics on the temperature of the root canal wall. J Endod 14(11):5549
Al-Jadaa A, Paque F, Attin T, Zehnder M (2009) Necrotic pulp tissue dissolution by passive ultrasonic irrigation in simulated accessory canals: impact of canal location and angulation. Int Endod J 42(1):5965
Ahmad M (1989) Effect of ultrasonic instrumentation on Bacteroides intermedius. Endod Dent Traumatol 5(2):836
Macedo RG, Wesselink PR, Zaccheo F, Fanali D, Van Der Sluis LW (2010) Reaction rate of NaOCl in contact with bovine dentine: effect of activation, exposure time, concentration and pH. Int Endod J 43(12):110815
Căpută PE, Retsas A, Kuijk L, de Paz LEC, Boutsioukis C (2019) Ultrasonic irrigant activation during root canal treatment: a systematic review. J Endod 45(1):3144. e13
Beltes C, Sakkas H, Economides N, Papadopoulou C (2017) Antimicrobial photodynamic therapy using Indocyanine green and near-infrared diode laser in reducing Entrerococcus faecalis. Photodiagnosis Photodyn Ther 17:58
Pourhajibagher M, Chiniforush N, Shahabi S, Palizvani M, Bahador A (2018) Antibacterial and antibiofilm efficacy of antimicrobial photodynamic therapy against intracanal enterococcus faecalis: an in vitro comparative study with traditional endodontic irrigation solutions. J Dent (Tehran) 15(4):197204
Funding
This study was supported by Tehran University of Medical Sciences, International campus, Tehran, Iran.
SignificanceSilver nanoparticles activated by passive ultrasonic irrigation or photon-induced photo acoustic streaming can serve as a suitable adjunct for irrigation and disinfection of the root canals inoculated with Enterococcus faecalis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: This article was originally published with an incorrect author name.
Rights and permissions
About this article

Cite this article
Afkhami, F., Ahmadi, P., Chiniforush, N. et al. Effect of different activations of silver nanoparticle irrigants on the elimination of Enterococcus faecalis. Clin Oral Invest 25, 6893–6899 (2021). https://doi.org/10.1007/s00784-021-03979-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-021-03979-5