
Abstract
Purpose
Successful endodontic therapy relies on chemomechanical debridement. Laser-assisted irrigation techniques are available for debridement. However, there are limited studies demonstrating the effectiveness of dual lasers for root canal disinfection. Hence, the aim of the present study is to determine if laser activation irrigation using the Er,Cr:YSGG and 940-nm diode laser is as effective as positive pressure needle irrigation using sodium hypochlorite (NaOCl) and ethylenediamine tetraacetic acid (EDTA).
Methods
Fifty-two caries-free premolars were divided into six groups: G1, sterile water via positive pressure irrigation; G2, EDTA and NaOCl via positive pressure irrigation; G3, sterile water and the Er,Cr:YSGG cleaning and disinfection step; G4, sterile water and the Er,Cr:YSGG cleaning and disinfection step followed by disinfection with the 940-nm diode; G5, sterile water and the Er,Cr:YSGG cleaning step followed by a disinfection step with the Er,Cr:YSGG and diode laser together; and G6, negative controls. S1 samples were validated in both negative and positive control groups via culturing. All teeth, except the negative controls, were inoculated with Enterococcus faecalis. S2 sampling after treatments was completed and tested for bacterial presence via culturing and SEM and CLSM analysis.
Results
The data demonstrated that the traditional irrigation group (G2) and the dual laser group (G5) showed the greatest percentage decrease in bacterial counts from the S1 to the S2 group.
Conclusions
The data demonstrates that the combination of the Er,Cr:YSGG and 940-nm diode laser wavelengths is safe and more effective than either laser alone and is comparable to needle irrigation with sodium hypochlorite and EDTA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Successful endodontic therapy relies on adequate disinfection of the root canal system. Complex canal anatomy can harbor viable bacteria in areas such as isthmuses, ramifications, and dentinal tubules. Furthermore, these bacteria aggregate to form multispecies biofilms, which are resistant to chemomechanical preparation. Hence, mechanical debridement alone cannot effectively and efficiently clean these areas [1]. As a result, antimicrobial irrigants are used to clean and disinfect the root canal system. An ideal irrigant has many different properties, some of which include long-term antibacterial effects, ability to remove the smear layer, nontoxic, and noncarcinogenic [2]. Common irrigants used in endodontics include sodium hypochlorite (NaOCl) and chlorhexidine and ethylenediamine tetraacetic acid (EDTA) among others. Sodium hypochlorite has been the gold standard for irrigation for some time because of its ability to dissolve organic matter and its effective antibacterial activity. However, there are certain drawbacks associated with the use of sodium hypochlorite, which include its toxicity and inability to remove the smear layer, as well as in its ability to reduce the elastic modulus and flexural strength of dentin [3]. There are similar concerns with other irrigants used in endodontics. Hence, to date, there is no irrigant that satisfies all the criteria of an ideal irrigant.
Traditionally, positive pressure needle irrigation has been used to deliver irrigant into the canal system. Previous studies have shown that simple placement of irrigant into the canal does not sufficiently disinfect the canal system; therefore, activation of the irrigant is necessary in order to provide effective disinfection [4]. Over time, numerous techniques have been employed in order to facilitate adequate disinfection by activating the chosen irrigant in the root canal system. These techniques include, but are not limited to, sonic activation, ultrasonic activation, and photon-induced photoacoustic streaming (PIPS) [5,6,7]. These techniques have been shown to be superior to positive pressure irrigation. However, these techniques also have limitations and are unable completely sterilize the canals [8]. Irrigation with a laser has been proposed as an alternative method to effectively clean the root canal system. Lasers have established their presence in dentistry for decades and are being used for various purposes, which include the management of dentin hypersensitivity, pulpal diagnosis, pulp capping and pulpotomy procedures, root canal irrigation, endodontic surgery, gingival depigmentation, treatment of periimplantitis, and peripheral somatosensory neuropathy [9,10,11,12,13]. Moreover, previous studies have used lasers for smear layer removal, removal of filling remnants, and calcium hydroxide removal in addition to testing its antibacterial activity [14,15,16]. However, most published studies have utilized a single-wavelength laser for irrigation of the root canal system. More recently, a laser system (Waterlase, BIOLASE, Irvine, CA) has been developed which utilizes two laser wavelengths, 2780-nm Er,Cr:YSGG and 940-nm diode, simultaneously that are delivered through a radially firing tip in an effort to more effectively disinfect the root canal system [17]. This dual laser system has previously been successfully applied in treatment of periodontitis and alveolar osteitis and may also prove more effective in the treatment of root canal systems than either laser wavelength alone [18]. Another study has demonstrated that the use of these two wavelengths was effective to remove the smear layer and to achieve deep dentin disinfection. This study also discussed the rationale for using a double-wavelength laser in endodontics and case reports related to the same [19]. It is hypothesized that the activation of the dual laser within the canal system creates cavitation that destroys bacteria and biofilm [20,21,22]. However, no studies to date have shown the effectiveness of using a dual laser in human teeth as compared with a single laser system or conventional positive pressure irrigation. Hence, the aim of the present study is to determine if laser activation of sterile water using the 2780-nm Er,Cr:YSGG and 940-nm diode laser is as effective as the single laser system and the conventional positive pressure needle irrigation with sodium hypochlorite and EDTA.
Materials and methods
Preparation of the teeth
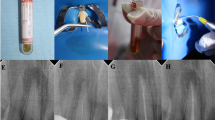
Fifty-two caries-free premolar teeth were selected. The teeth were radiographed mesiodistally to confirm a Weine’s type one canal morphology. The teeth were accessed, and working length was determined using a size 10 K file (Maillefer, Ballaigues, Switzerland) until the tip of the file was just visible at the apical foramen. Working length was determined by subtracting 1 mm. The teeth were then standardized to 18 mm working length by decoronating the occlusal aspect of the tooth perpendicular to the long axis of the root. Coronal flaring was completed using a size 2 Gates Glidden (Dentsply Maillefer, Ballaigues, Switzerland). A glide path was established with a size #15 K file. The apical constriction was gauged with hand files, and teeth larger than #30 were discarded. The teeth were prepared using slight modifications to a previously established protocol [23]. The teeth were then prepared using a crown down technique to a size #30/0.04 using Vortex Blue files (Dentsply/Tulsa Dental, York, PA). During instrumentation, the teeth were irrigated with sterile saline using a Max-I-Probe (Dentsply/Tulsa Dental, York, PA).
The teeth were then rinsed with sterile saline, and excess moisture was removed from the canal using paper points. Finally, all teeth were placed in an ultrasonic bath of 17% EDTA, 6% NaOCl, and 5% sodium thiosulfate for 5 min each, to ensure the removal of debris and smear layer and autoclaved at 121 °C and 15 lb./in.2 for 20 min.
Cultivation of Enterococcus faecalis and specimen inoculation
E. faecalis (American Type Culture Collection 19433) grown on brain heart infusion (BHI) agar plates for 24 h were used for these experiments. Isolated colonies were inoculated into 20 ml sterile BHI broth and grown for 8 h, after which 4 drops of these cultures were subcultured into new 20 ml sterile BHI broth and grown for an additional 4 h. Working cultures were adjusted to 1.5 × 108 colony forming units/ml (CFUs/ml) (equivalent to 0.5 McFarland standard), of which 20 ml was added to vials containing teeth suspended in sterile medium. All vials containing teeth were sealed and kept at 37 °C for 45 days in aerobic conditions to ensure adequate penetration of bacteria into dentinal tubules [24]. Every 5th day, 20 ml BHI broth was replaced with fresh medium to avoid culture saturation. The turbidity of the culture during the incubation indicated bacterial growth, and purity was confirmed by Gram staining after 45 days.
Preparation for bacteria sampling
The teeth were removed from broth and rinsed with sterile saline, and the outside of each tooth was wiped with 70% isopropyl alcohol. A sterile cotton pellet was placed into the chamber, and the access cavity sealed with Cavit (3 M ESPE, St. Paul, MN). The apical foramen was sealed with flowable composite to resemble a closed system (35% phosphoric acid (Ultra-Etch), Prime & Bond NT, PermaFlo Purple, Ultradent, South Jordan, UT). The outer surface of each tooth was disinfected with 30% hydrogen peroxide (H2O2) until no further bubbling of the peroxide occurred. All surfaces were coated with a 10% povidone–iodine solution (Aplicare, Meriden, CT) and allowed to dry. The tooth surface was swabbed with a 5% sodium thiosulfate solution to inactivate the iodine [23].
Initial sample (S1)
The Cavit and cotton pellet were removed with an air-cooled carbide bur, and the canal flushed with 2 ml sterile water and dried with sterile paper points. With a sterile syringe, sterile BHI broth was inserted into the canals, removed with four consecutive sterile paper points, which was then cultured onto a BHI agar plate. A second round of sterile BHI broth was reinserted and again removed with four sterile paper points (Fine) and ultimately cultured into Eppendorf tubes containing 1 ml sterile BHI broth. The 1 ml broth cultures were then serially diluted 1:10 and plated onto BHI agar plates in aliquots of 0.1 ml. CFUs were counted after 48 h growth at 37 °C aerobically. This procedure was verified in both negative control and positive control groups.
Treatment groups
-
G1: 10 teeth were irrigated with 5 ml sterile water via positive pressure irrigation with 30-gauge Max-I-Probe within 1 mm of working length (positive control).
-
G2: 10 teeth were irrigated with 3 ml 17% EDTA and 5 ml 5.25% NaOCl via positive pressure irrigation with 30-gauge Max-I-Probe within 1 mm of working length.
-
The machine used for this study was a prototype from BIOLASE (Irvine, CA), which delivers both wavelengths simultaneously through the same fiber delivery system and through the same radial firing tip. It can be operated in YSGG-only mode, 940 nm-only mode, and in synergy mode, which were used in the different experimental groups described below. In synergy mode, the 2780-nm and 940-nm pulses are intermixed—each 2780-nm pulse is followed by a 940-nm pulse, which in turn is followed by a 2780-nm pulse and so on. A gold handpiece was used with the RFT3 tip, which the diameter of the RFT3 tip was 320 μm, and delivered energy in a radial pattern 360° around the tip. The tip was changed after the cleaning step, as per the manufacturer’s protocol. No changes in the tip-aiming beam were observed throughout the study.
-
G3: 10 teeth: sterile water inserted into canals followed by Er,Cr:YSGG cleaning step (63 mJ, 20 Hz, 1.25 W) RFT3 fiber placed to within 1 mm of working length (17 mm) activated and withdrawn at 1 mm/s a total of 8 times per tooth under 5 ml sterile water irrigation. This cleaning step has been shown to remove smear layer [25]. Samples were then treated with the Er,Cr:YSGG disinfection step (50 mJ, 5 Hz, 0.25 W) RFT3 fiber placed to within 1 mm of working length (17 mm) activated and withdrawn at 1 mm/s a total of 8 times per tooth under 5 ml sterile water irrigation. Previous data has reported using a speed of 2 mm/s till the most coronal part of the canal [19] while others have used 1 mm/s [26]. This speed is an approximation, and we followed the manufacturer’s recommendation for the same for this study.
-
G4: 10 teeth: sterile water inserted into canals followed by Er,Cr:YSGG cleaning step (63 mJ, 20 Hz, 1.25 W) RFT3 fiber placed to within 1 mm of working length (17 mm) activated and withdrawn at 1 mm/s a total of 8 times per tooth under 5 ml sterile water irrigation. ER,CR:YSGG disinfection step (50 mJ, 5 Hz, 0.25 W) RFT3 fiber placed to within 1 mm of working length (17 mm) activated and withdrawn at 1 mm/s a total of 8 times per tooth under 5 ml sterile water irrigation. Each sample was allowed to rest for 3 min. The samples were then treated with the 940-nm diode disinfection step (1 W avg., 5 W peak 40-ms pulse duration, 160-ms interval) RFT3 fiber placed to within 1 mm of working length (17 mm) activated and withdrawn at 1 mm/s a total of 8 times per tooth under 5 ml sterile water irrigation.
-
G5: 10 teeth: sterile water inserted into canals followed by Er,Cr:YSGG cleaning step (63 mJ, 20 Hz, 1.25 W) RFT3 fiber placed to within 1 mm of working length (17 mm) activated and withdrawn at 1 mm/s a total of 8 times per tooth under 5 ml sterile water irrigation. Dual-wavelength disinfection. Er,Cr:YSGG (50 mJ, 5 Hz, 0.25 W) + 940-nm diode (1 W avg., 5 W peak, 0 ms delay, 40-ms pulse duration) RFT3 fiber placed to within 1 mm of working length (17 mm) activated and withdrawn at 1 mm/s a total of 8 times per tooth under 5 ml sterile water irrigation.
-
G6: 2 teeth were prepared for bacterial sampling as mentioned above, and S1 and S2 sampling performed without any treatment in between (negative control).
The teeth in the laser group were treated as suggested by the manufacturer’s recommendations. The laser tip was withdrawn straight while still being in contact with the canal walls. This has been the method of choice in other studies [26].
The pulse duration for the YSGG was 60 μs and pulse duration for the 940 nm was 40 ms. The power output from the tip and the power output from the trunk fiber delivery system were measured. Transmission through the tip was calculated. The powers written in the “Materials and methods” section above reflect the true power output measured from the RFT3 tips (not settings on the laser display). Another important factor to consider is the duty cycle which is one of the factors that determines the average power when the diode laser is operating in pulse mode. The duty cycle is a periodic phenomenon in a given period to the period (reciprocal value of the current frequency setting—number of pulses per second) [27]. The duty cycle here was calculated at 20%.
Final sample (S2)
After completion of treatment based on the assigned group protocol, the root canal of each tooth was dried with sterile paper points and filled with sterile BHI broth. Four consecutive paper points were introduced into the canal to absorb the BHI broth and cultured on a BHI agar plate. The canal was then refilled with sterile BHI broth, and a #15 K file was placed into the canal within 1 mm of working length, and the canal was circumferentially filed for 20 s. Four consecutive paper points (Fine) were inserted into the canal and then placed into an Eppendorf tube containing 1.0 ml of sterile BHI broth. The 1 ml tube was vortexed, and 1:10 serially diluted aliquots of 0.1 ml suspensions were plated onto BHI agar plates. The plates were then incubated aerobically for 48 h at 37 °C after which the CFUs were counted.
Confocal laser scanning microscope examination and image analysis
After treatment, half of the samples from each group were used for SEM analysis, and the other half were used for confocal laser scanning microscope (CLSM) analysis. Staining and confocal imaging were performed as previously described, with slight modifications [28, 29]. Fluorescent stains SYTO®9 and propidium iodide (PI) (Life Technologies Corp, Grand Island, NY) were diluted together in sterile saline to a final concentration of 20 and 120 μmol/L, respectively, and filled into the canals of prerinsed teeth in an Eppendorf tube. Samples were maintained at room temperature in the dark for 15 min after which the staining solution and wax were removed. The teeth were sectioned across the lower and middle apical third areas of the sample. These sections were rinsed with sterile saline, sanded, rinsed again to remove excess debris, transferred into tubes containing the staining solution, and maintained again at room temperature in the dark for 15 min. The samples were taken out and rinsed with saline three times and then examined using a confocal microscope.
Samples were examined by CLSM with the Leica SP8X confocal microscope (Leica Microsystems, Germany) at × 400 magnification. The thresholds of the red and green fluorescence were manually adjusted, and images of the apical and middle thirds starting from the lumen surface of the root canal were taken. Live bacteria with intact membranes were stained green by SYTO®9, and dead bacteria with damaged membranes were stained red by propidium iodide uptake. Image analysis was performed using the ImageJ 1.5b Java 1.8.0 (64 bit) software (National Institutes of Health, USA) with the Bio-Formats version 5.5.1 plugin package.
Scanning electron microscopy examination
The teeth were longitudinally grooved, sectioned, and rinsed in phosphate-buffered saline, soaked in glutaraldehyde for 1 h, and then fixed with osmium tetroxide for 30 min [30]. Samples were then dehydrated, mounted on SEM discs, and sputter coated with 5 nm of gold–palladium for conductivity, and examined with a scanning electron microscope (JEOL Model JSM 6010Plus). Representative images were taken of the middle and apical thirds at magnifications of × 500, × 1000, × 5000, and × 10,000.
Statistical analysis
The required sample size was calculated to be 10 samples per group. This gave the study at least 90% power to detect a difference between groups. The differences in bacterial colonies were assessed at S1 and S2. Viable counts were transformed to their log10 values. The Wilcoxon signed-rank test was used for intragroup analysis comparing the reduction in the number of CFU counts from S1 to S2. The Kruskal-Wallis test was used to test for differences in CFUs across groups. The significance level was set at p < 0.05 for all tests.
Results
The dual laser group performed as well as the traditional irrigation group
All groups except the negative control (G6) showed bacterial growth on the BHI plates at the S1 sample (data not shown). The mean log10 viable counts at the S1 sample showed no statistical differences between the groups prior to starting the irrigation protocols (Table 1). The positive control (G1) group showed an increase in the bacterial CFUs at the S2 sample. Overall, the other groups showed significant reductions in bacterial counts from the S1 to the S2 sample. However, the traditional irrigation group (G2) and the dual laser group (G5) showed the greatest percentage decrease in bacterial counts from the S1 to the S2 group (Table 1). There were no statistically significant differences between the G2 and G5 groups (Fig. 1).

Bacterial CFU counts before and after laser treatment. Mean (± standard deviation) CFU counts in viable bacterial counts of before (S1) and after (S2) treatments. Groups 2, 3, 4, and 5 showed a significant reduction in bacterial counts as compared with group 1 where teeth were irrigated with sterile water
Scanning electron microscopy analysis
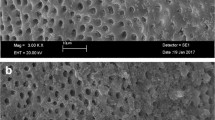
SEM examination shows the presence of bacteria in the dentin tubules in group 1. No bacteria could be visualized in groups 2–5 (Fig. 2). These results may be due to the lower numbers of bacteria in the treatment groups and the limitations of SEM, which include processing of the samples.

The radicular dentin using SEM imaging. The radicular dentin samples were washed and fixed (as stated in the “Materials and methods” section), and then their surface topography was analyzed using scanning electron microscopy (SEM). Bar = 5 μm and × 5000 magnification. Bacteria could be visualized only in group 1, which was the positive control group
Confocal laser scanning microscopy
CLSM images show viable bacteria in group 1 approximating the canal lumen. In groups 2–5, nonviable bacteria are seen approximating the canal lumen and extending into the dentine tubules at varying distances. Group 5 appears to have the deepest depth of nonviable bacteria extending into the dentin tubules (Fig. 3). This is consistent with the microbiological findings. The depth of nonviable bacteria staining was different between groups 2 and 5 (Fig. 4). This correlates to the depth of irrigant or laser penetration into the dentinal tubules.

The radicular dentin using the CLSM examination. CLSM of the radicular dentin and infected dentinal tubules after exposure to the different disinfecting agents and viability staining. The green staining indicated viable bacteria, whereas the red–orange–yellow staining represents dead bacteria. The images for groups 1–4 were taken at × 400 magnification and 40 μm and at × 400 magnification and 100 μm for group 5

Depth of irrigant and laser penetration into the dentinal tubules. The staining with the live/dead stain corroborates with the depth of the laser penetration into the dentinal tubules. The depth of laser penetration correlated to the red staining in the dentinal tubules and was calculated accordingly. The dual laser, group 5, demonstrated the best results in the apical third
Discussion
Previous research has shown that elimination of bacteria from the root canal system is important for both pulpal and periapical healing [31]. Effective chemomechanical debridement is essential to achieve elimination of bacteria. Sodium hypochlorite (NaOCl) has been considered the gold standard for irrigation for many decades and continues to be used in routine endodontic practice as the irrigant of choice [32]. However, the use of NaOCl has its drawbacks, which include high cytotoxicity, lack of substantivity, its inability to remove the smear layer, and inability to be combined with other irrigants like chlorhexidine [32].
More recent research has focused on alternative irrigation techniques which include the use of Er,Cr:YSGG lasers. Among several laser devices, the Er:YAG laser has shown to be effective, because its 2940-nm wavelength coincides with the highest absorption band of water [22]. Furthermore, it has the ability to interact with aqueous solutions and produce cavitation that is capable penetrating into the dentinal tubules and achieving significant disinfection while also removing the smear layer and dentin debris [19]. It is thought that the cleaning mechanism of an Er:YAG laser is mainly based on collapse shock waves and high-speed streaming of fluid, which are caused by rapid expansion and implosion of laser-induced bubbles [22]. Another important aspect related to the success of this technique is the use of a radial firing tip. Radial firing tips have played a significant role in improving the efficacy of lasers in endodontics with its ability to reduce emission in the forward direction towards the apical tissues and instead deliver homogenous distribution of energy along the root canal walls thereby resulting in more effective debridement [19, 26]. Previous published data demonstrates that the 2780-nm Er,Cr:YSGG and 940-nm diode lasers used with a radial firing tip have been effective in disinfecting root canal systems of bovine teeth [33] and have been reported to be safe and effective [19]. Some other studies have demonstrated that these two lasers can effectively eliminate the smear layer inside the root canal [34]. However, there is limited data related to the disinfection properties of these laser wavelengths in extracted human teeth inoculated with a mature biofilm and their comparison with positive pressure irrigation. Hence, this study evaluated the effects of these lasers on human teeth inoculated with E. faecalis.
E. faecalis was chosen because this bacterium is resistant to traditional chemomechanical preparation and has several virulence factors that make it difficult to eradicate from the root canal system [24, 35]. The teeth were cultured in an E. faecalis broth for 45 days to create a mature biofilm and to recreate the microbial conditions within the root canal system of a necrotic tooth [30]. Sterile water was used in conjunction with the laser treatment to show the effectiveness of the laser in killing bacteria without the effects of a chemical irrigant. By separating the chemical irrigant from the laser treatment, we could demonstrate that the laser energy alone is responsible for the reduction in the bacteria within the root canal system [36, 37]. Furthermore, previous data has demonstrated that there is no difference in reduction of bacteria when the Er,Cr:YSGG was in a dry canal or in a canal that had water [26].
During the irrigation procedure, the tip used in the teeth was withdrawn straight. Previous studies have described using circular motions when withdrawing the tip which is well accepted clinically [19], but for this study, we followed the manufacturer’s recommendations which also mentioned that the tip movement was less important than the fact that the tip is always in contact with the canal walls [38].
Another important difference in this study from previous published studies is that the 940-nm laser was used in pulsed mode versus a CW mode [19]. CW mode has already been shown to be effective, so this study used the pulsed mode to check if this could be an alternative. This pulsed mode worked equally well thus proving it could be a viable option to the CW mode.
The log values of the CFUs demonstrated that groups 2–5 showed a statistically significant difference between the S1 and S2 counts (Table 1). This demonstrates that the laser when used either separately or together was effective in lowering the bacterial counts. The data further demonstrates that the dual laser group (G5) performed as well as the traditional irrigation group (G2). There were no statistically significant differences between the S2 counts for both groups, and the percentage reductions were similar (Fig. 1).
The laser groups (G3–G5) used sterile water as an irrigant and demonstrated low CFU counts in their S2 groups as compared with the S1 groups. Sterile water is not an intracanal irrigant in endodontics because it lacks antibacterial activity, thereby indicating that the effects of the laser treatments were solely due to the laser/lasers alone. Moreover, sterile water lacks cytotoxicity, demonstrating the significance of a potential combined therapy using dual laser treatment in conjunction with a nontoxic irrigant. This could be of notable importance in teeth with open apices as lasers could prove to be an effective way of irrigating immature teeth without the fear of a hypochlorite accident. Another advantage of this potential laser therapy is advantage of treatment without the potential to damage stem cells. Preliminary studies investigating the effects of the dual laser system on stem cells of the apical papilla (SCAP) have shown no deleterious effects (ongoing study).
Microbiological results were verified with SEM, which showed presence of bacteria in the positive control group but absence of bacteria in the other groups (Fig. 2). Groups G3 and G4 showed positive cultures, but the SEM images did not show the presence of bacteria which could be related to the way these teeth were sectioned and processed and is one of the known drawbacks of SEM imaging [39]. SEM imaging does not help determine the viability of the bacteria and is another drawback of this technique. Hence, CLSM imaging was performed to visualize the presence of live/dead bacteria in the dentinal tubules (Fig. 3).
The CLSM data demonstrated that the positive control (G1) had viable bacteria in the dentinal tubules, which appeared green. The green color corresponds to viable bacteria, and any color other than green corresponds to dead bacteria [40]. The treatment G2–5 showed nonviable bacteria adjacent to the canal lumen and extending varying depths into the dentin (stained red–orange) (Fig. 3). The CLSM data show that the traditional irrigation group (G2) was effective in killing bacteria up to a few micrometers into the dentinal tubules. However, the laser treatment groups (G3–5) were more effective when compared with group 2 (Fig. 4). It is important to note that groups 4 and 5 received the same laser treatment except that the 940-nm diode laser was used after a 3-min rest in group 4 versus being used simultaneously with the Er,Cr:YSGG laser in group 5. However, the results for these two groups varied. Group 5 demonstrated less viable bacteria, which is evident from the microbiology results and the CLSM staining. This could be better appreciated with the 100-μm section taken for group 5 as compared with the 40-μm sections taken for all other groups. Other studies have demonstrated the effectiveness of the dual laser reaching a depth of 1000 μm of bovine dentin [33]. This study did not analyze the dentin beyond 300 μm, but based on previous evidence, deeper penetration be possible. This suggests that using both laser wavelengths simultaneously could prove more effective and possibly increase the depth of penetration into the dentinal tubules up to 300 μm (Fig. 4). This is especially important since some bacteria, like E. faecalis, have the ability to penetrate from 250 to 1500 μm into the dentinal tubules [41]. Irrigants, such as NaOCl, cannot disperse into this depth within the dentinal tubules, which is another explanation for why the G2 group shows presence of viable bacteria a few micrometers away from the canal [42] (Fig. 3).
The staining with the live/dead stain corroborates with the depth of the laser penetration into the dentinal tubules. The depth of laser penetration correlated to the red staining in the dentinal tubules and was calculated accordingly. The dual laser demonstrated the best results in the apical third. This could be due to the radial firing tip, which helps the cavitation energy to travel laterally versus apically. Alternatively, as the apical third of the root canal system is more constricted than the middle third, it is possible that the tip is closer to the canal walls in the apical third as compared with the middle third. Hence, the apical third could be exposed to more expansion and implosion of the dual laser-induced bubbles, which is why the depth of penetration for these groups (G4 and G5) was higher than the other groups (Fig. 4). This may be particularly helpful in narrow-curved canals where a radial tip might be able to clean the root canal efficiently and might improve the success rates of root canal treatments. Another important aspect to consider is the apical third of the root canal system that usually remains unprepared in about 18% of cases and could attribute to endodontic failures [43].
Visual inspection of the root prior to sectioning and after sectioning demonstrated no damage to any portion of the root surface. We believe this is important as some previous studies have demonstrated damage to the root after laser irradiation [44]. This corresponds to data from previous studies that demonstrated no ultrastructural changes in the root canal walls [34]. Furthermore, the dual laser has been shown to be safe when used for root canal disinfection as it did not result in adverse thermal changes on the external root surface. This is important as increases in the root surface temperature could cause detrimental effects on the periodontal ligament and surrounding bone [45]. Altogether, our data combined with the evidence from previous studies demonstrate that this dual laser system appears to be safe, efficient, and effective in debriding the root canal system, especially the apical third, which could potentially lead to fewer failures. Randomized clinical trials with the Er,Cr:YSGG laser have shown no statistically significant differences between the laser and the sodium hypochlorite group [46]. However, this in vitro study demonstrates encouraging results with the dual laser, and studies are ongoing to determine if these results have the potential to be extrapolated into an in vivo system.
Conclusions
Our data demonstrates that the combination of 2780-nm Er,Cr:YSGG and 940-nm diode laser wavelengths is safe and more effective than either laser alone when considering microbial disinfection and is comparable to the gold standard of needle irrigation with sodium hypochlorite and EDTA. However, the depth of dentin tubule disinfection was superior in the dual laser group compared with the traditional irrigation.
References
Peters OA, Peters CI, Schonenberger K, Barbakow F (2003) ProTaper rotary root canal preparation: effects of canal anatomy on final shape analysed by micro CT. Int Endod J 36(2):86–92
Torabinejad M, Handysides R, Khademi AA, Bakland LK (2002) Clinical implications of the smear layer in endodontics: a review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 94(6):658–666. https://doi.org/10.1067/moe.2002.128962
Mohammadi Z (2008) Sodium hypochlorite in endodontics: an update review. Int Dent J 58(6):329–341
Gutarts R, Nusstein J, Reader A, Beck M (2005) In vivo debridement efficacy of ultrasonic irrigation following hand-rotary instrumentation in human mandibular molars. J Endod 31(3):166–170
Sabins RA, Johnson JD, Hellstein JW (2003) A comparison of the cleaning efficacy of short-term sonic and ultrasonic passive irrigation after hand instrumentation in molar root canals. J Endod 29(10):674–678. https://doi.org/10.1097/00004770-200310000-00016
Akcay M, Arslan H, Mese M, Durmus N, Capar ID (2016) Effect of photon-initiated photoacoustic streaming, passive ultrasonic, and sonic irrigation techniques on dentinal tubule penetration of irrigation solution: a confocal microscopic study. Clin Oral Investig 21:2205–2212. https://doi.org/10.1007/s00784-016-2013-y
Ayranci LB, Arslan H, Akcay M, Capar ID, Gok T, Saygili G (2016) Effectiveness of laser-assisted irrigation and passive ultrasonic irrigation techniques on smear layer removal in middle and apical thirds. Scanning 38(2):121–127. https://doi.org/10.1002/sca.21247
Aminoshariae A, Kulild J (2015) Master apical file size—smaller or larger: a systematic review of microbial reduction. Int Endod J 48(11):1007–1022. https://doi.org/10.1111/iej.12410
Lan WH, Liu HC (1996) Treatment of dentin hypersensitivity by Nd:YAG laser. J Clin Laser Med Surg 14(2):89–92. https://doi.org/10.1089/clm.1996.14.89
Moritz A, Schoop U, Goharkhay K, Sperr W (1998) The CO2 laser as an aid in direct pulp capping. J Endod 24(4):248–251. https://doi.org/10.1016/S0099-2399(98)80106-4
Gholami L, Moghaddam SA, Rigi Ladiz MA, Molai Manesh Z, Hashemzehi H, Fallah A, Gutknecht N (2018) Comparison of gingival depigmentation with Er,Cr:YSGG laser and surgical stripping, a 12-month follow-up. Lasers Med Sci 33(8):1647–1656. https://doi.org/10.1007/s10103-018-2501-1
Birang E, Talebi Ardekani MR, Rajabzadeh M, Sarmadi G, Birang R, Gutknecht N (2017) Evaluation of effectiveness of photodynamic therapy with low-level diode laser in nonsurgical treatment of peri-implantitis. J Lasers Med Sci 8(3):136–142. https://doi.org/10.15171/jlms.2017.25
Fallah A, Mirzaei A, Gutknecht N, Demneh AS (2017) Clinical effectiveness of low-level laser treatment on peripheral somatosensory neuropathy. Lasers Med Sci 32(3):721–728. https://doi.org/10.1007/s10103-016-2137-y
Granevik Lindstrom M, Wolf E, Fransson H (2017) The antibacterial effect of Nd:YAG laser treatment of teeth with apical periodontitis: a randomized controlled trial. J Endod 43(6):857–863. https://doi.org/10.1016/j.joen.2017.01.013
Shahriari S, Kasraei S, Roshanaei G, Karkeabadi H, Davanloo H (2017) Efficacy of sodium hypochlorite activated with laser in intracanal smear layer removal: an SEM study. J Lasers Med Sci 8(1):36–41. https://doi.org/10.15171/jlms.2017.07
Suk M, Bago I, Katic M, Snjaric D, Munitic MS, Anic I (2017) The efficacy of photon-initiated photoacoustic streaming in the removal of calcium silicate-based filling remnants from the root canal after rotary retreatment. Lasers Med Sci 32(9):2055–2062. https://doi.org/10.1007/s10103-017-2325-4
Schulte-Lunzum R, Gutknecht N, Conrads G, Franzen R (2017) The impact of a 940 nm diode laser with radial firing tip and bare end fiber tip on Enterococcus faecalis in the root canal wall dentin of bovine teeth: an in vitro study. Photomed Laser Surg 35(7):357–363. https://doi.org/10.1089/pho.2016.4249
Ertugrul AS, Tekin Y, Talmac AC (2017) Comparing the efficiency of Er,Cr:YSGG laser and diode laser on human beta-defensin-1 and IL-1beta levels during the treatment of generalized aggressive periodontitis and chronic periodontitis. J Cosmet Laser Ther 19(7):409–417. https://doi.org/10.1080/14764172.2017.1334923
Martins MR, Franzen R, Depraet F, N. G (2018) Rationale for using a double-wavelength (940 nm + 2780 nm) laser in endodontics: literature overview and proof-of-concept. Lasers Dent Sci 2(1):29–41. https://doi.org/10.1007/s41547-017-0017-9
Blanken J, De Moor RJ, Meire M, Verdaasdonk R (2009) Laser induced explosive vapor and cavitation resulting in effective irrigation of the root canal. Part 1: a visualization study. Lasers Surg Med 41(7):514–519. https://doi.org/10.1002/lsm.20798
De Moor RJ, Blanken J, Meire M, Verdaasdonk R (2009) Laser induced explosive vapor and cavitation resulting in effective irrigation of the root canal. Part 2: evaluation of the efficacy. Lasers Surg Med 41(7):520–523. https://doi.org/10.1002/lsm.20797
Matsumoto H, Yoshimine Y, Akamine A (2011) Visualization of irrigant flow and cavitation induced by Er:YAG laser within a root canal model. J Endod 37(6):839–843. https://doi.org/10.1016/j.joen.2011.02.035
Hockett JL, Dommisch JK, Johnson JD, Cohenca N (2008) Antimicrobial efficacy of two irrigation techniques in tapered and nontapered canal preparations: an in vitro study. J Endod 34(11):1374–1377. https://doi.org/10.1016/j.joen.2008.07.022
Haapasalo M, Orstavik D (1987) In vitro infection and disinfection of dentinal tubules. J Dent Res 66(8):1375–1379. https://doi.org/10.1177/00220345870660081801
George R, Meyers IA, Walsh LJ (2008) Laser activation of endodontic irrigants with improved conical laser fiber tips for removing smear layer in the apical third of the root canal. J Endod 34(12):1524–1527. https://doi.org/10.1016/j.joen.2008.08.029
Gordon W, Atabakhsh VA, Meza F, Doms A, Nissan R, Rizoiu I, Stevens RH (2007) The antimicrobial efficacy of the erbium, chromium:yttrium-scandium-gallium-garnet laser with radial emitting tips on root canal dentin walls infected with Enterococcus faecalis. J Am Dent Assoc 138(7):992–1002
Pirnat S (2007) Versatility of an 810 nm diode laser in dentistry: an overview. Journal of Laser and Health Academy 2007(7):1–9
Linkert M, Rueden CT, Allan C, Burel JM, Moore W, Patterson A, Loranger B, Moore J, Neves C, Macdonald D, Tarkowska A, Sticco C, Hill E, Rossner M, Eliceiri KW, Swedlow JR (2010) Metadata matters: access to image data in the real world. J Cell Biol 189(5):777–782. https://doi.org/10.1083/jcb.201004104
Parmar D, Hauman CH, Leichter JW, McNaughton A, Tompkins GR (2011) Bacterial localization and viability assessment in human ex vivo dentinal tubules by fluorescence confocal laser scanning microscopy. Int Endod J 44(7):644–651. https://doi.org/10.1111/j.1365-2591.2011.01867.x
Latham J, Fong H, Jewett A, Johnson JD, Paranjpe A (2016) Disinfection efficacy of current regenerative endodontic protocols in simulated necrotic immature permanent teeth. J Endod 42(8):1218–1225. https://doi.org/10.1016/j.joen.2016.05.004
Kakehashi S, Stanley HR, Fitzgerald R (1969) The exposed germ-free pulp: effects of topical corticosteroid medication and restoration. Oral Surg Oral Med Oral Pathol 27(1):60–67
Mohammadi Z, Shalavi S, Moeintaghavi A, Jafarzadeh H (2017) A review over benefits and drawbacks of combining sodium hypochlorite with other endodontic materials. Open Dent J 11:661–669. https://doi.org/10.2174/1874210601711010661
Gutknecht N, Al-Karadaghi TS, Al-Maliky MA, Conrads G, Franzen R (2016) The bactericidal effect of 2780 and 940 nm laser irradiation on Enterococcus faecalis in bovine root dentin slices of different thicknesses. Photomed Laser Surg 34(1):11–16. https://doi.org/10.1089/pho.2015.3960
Al-Karadaghi TS, Franzen R, Jawad HA, Gutknecht N (2015) Investigations of radicular dentin permeability and ultrastructural changes after irradiation with Er,Cr:YSGG laser and dual wavelength (2780 and 940 nm) laser. Lasers Med Sci 30(8):2115–2121. https://doi.org/10.1007/s10103-015-1757-y
Yang Y, Shen Y, Wang Z, Huang X, Maezono H, Ma J, Cao Y, Haapasalo M (2016) Evaluation of the susceptibility of multispecies biofilms in dentinal tubules to disinfecting solutions. J Endod 42(8):1246–1250. https://doi.org/10.1016/j.joen.2016.05.011
Wang QQ, Zhang CF, Yin XZ (2007) Evaluation of the bactericidal effect of Er,Cr:YSGG, and Nd:YAG lasers in experimentally infected root canals. J Endod 33(7):830–832. https://doi.org/10.1016/j.joen.2007.03.017
Yavari HR, Rahimi S, Shahi S, Lotfi M, Barhaghi MH, Fatemi A, Abdolrahimi M (2010) Effect of Er, Cr: YSGG laser irradiation on Enterococcus faecalis in infected root canals. Photomed Laser Surg 28(Suppl 1):S91–S96. https://doi.org/10.1089/pho.2009.2539
Franzen R, Rashidisangsary B, Ozturan S, Vanweersch L, Gutknecht N (2015) Intrapulpal temperature changes during root surface irradiation with dual-wavelength laser (2780 and 940 nm): in vitro study. J Biomed Opt 20(1):018002. https://doi.org/10.1117/1.JBO.20.1.018002
Hwang D, Fong H, Johnson JD, Paranjpe A (2017) Efficacy of different carriers for the triple antibiotic powder during regenerative endodontic procedures. Aust Endod J 44:208–214. https://doi.org/10.1111/aej.12228
Vatkar NA, Hegde V, Sathe S (2016) Vitality of Enterococcus faecalis inside dentinal tubules after five root canal disinfection methods. J Conserv Dent 19(5):445–449. https://doi.org/10.4103/0972-0707.190019
Sireesha A, Jayasree R, Vidhya S, Mahalaxmi S, Sujatha V, Kumar TSS (2017) Comparative evaluation of micron- and nano-sized intracanal medicaments on penetration and fracture resistance of root dentin—an in vitro study. Int J Biol Macromol 104(Pt B):1866–1873. https://doi.org/10.1016/j.ijbiomac.2017.05.126
Schafer E, Bossmann K (2005) Antimicrobial efficacy of chlorhexidine and two calcium hydroxide formulations against Enterococcus faecalis. J Endod 31(1):53–56
Siqueira JF Jr, Perez AR, Marceliano-Alves MF, Provenzano JC, Silva SG, Pires FR, Vieira GC, Rocas IN, Alves FR (2017) What happens to unprepared root canal walls: a correlative analysis using micro-computed tomography and histology/scanning electron microscopy. Int Endod J 51:501–508. https://doi.org/10.1111/iej.12753
Ishizaki NT, Matsumoto K, Kimura Y, Wang X, Kinoshita J, Okano SM, Jayawardena JA (2004) Thermographical and morphological studies of Er,Cr:YSGG laser irradiation on root canal walls. Photomed Laser Surg 22(4):291–297. https://doi.org/10.1089/pho.2004.22.291
Al-Karadaghi TS, Gutknecht N, Jawad HA, Vanweersch L, Franzen R (2015) Evaluation of temperature elevation during root canal treatment with dual wavelength laser: 2780 nm Er,Cr:YSGG and 940 nm diode. Photomed Laser Surg 33(9):460–466. https://doi.org/10.1089/pho.2015.3907
Martins MR, Carvalho MF, Vaz IP, Capelas JA, Martins MA, Gutknecht N (2013) Efficacy of Er,Cr:YSGG laser with endodontical radial firing tips on the outcome of endodontic treatment: blind randomized controlled clinical trial with six-month evaluation. Lasers Med Sci 28(4):1049–1055. https://doi.org/10.1007/s10103-012-1172-6
Acknowledgments
We acknowledge the support from the NIH to the UW W. M. Keck Microscopy Center (S10 OD016240).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report that a financial affiliation exists for this paper. The corresponding author, Dr. Paranjpe, received research grants from BIOLASE (Irvine, CA). Dr. Darveau reports that financial affiliations exist for this paper (Dr. Darveau was a consultant for BIOLASE).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Erben, P., Chang, A.M., Darveau, R.P. et al. Evaluation of the bactericidal potential of 2780-nm ER,CR:YSGG and 940-nm diode lasers in the root canal system. Laser Dent Sci 3, 137–146 (2019). https://doi.org/10.1007/s41547-019-00060-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41547-019-00060-z