
Abstract
Objectives
This study using contralateral teeth from human cadavers assessed the amount of unprepared wall surface areas (USA), accumulated hard tissue debris (AHTD), and dentinal crack formation after root canal preparation using either reciprocating or rotary instruments.
Materials and methods
Incisors with a single root canal from 11 human mandibles had their root canals prepared with Reciproc or Mtwo. Each contralateral tooth was treated with one of the test instruments in order to create matched pairs. Micro-CT scans were taken before and after preparation to instrument sizes 40 and 50 in both groups. USA and AHTD were evaluated in the full canal length or the apical portion only. Crack formation was also evaluated in the full root length.
Results
After size 40, no significant differences in USA and AHTD were observed in the full canal length (P > .05). Separate analysis of the apical 4-mm canal revealed no difference in AHTD, but significantly more USA with Mtwo than Reciproc (P < .05). After size 50, the amount of USA was similar between groups both in the full canal and in the apical canal (P > .05). More AHTD were observed in the full canal after using Mtwo size 50 (P < .05), but no difference occurred in the apical canal only (P > .05). Intragroup analyses showed a significant decrease of USA and a significant increase of AHTD when preparation size increased from 40 to 50 (P < .05). In teeth without any pre-existing detectable dentinal defect (n = 38), crack formation occurred in 4 teeth, 2 from each preparation system.
Clinical relevance
Reciproc instrument size 40 resulted in more prepared areas in the apical canal than Mtwo instrument of the same size. However, the amount of AHTD did not differ between them at this file size. Canal enlargement to size 50 prepared more walls but created more debris. Dentinal defects were produced after preparation with both systems.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Insufficient root canal preparation is a reason of concern when using conventional engine-driven instruments. The large majority of the available instrument systems work in reciprocating or continuous rotation and produce a round preparation, usually centered in the root. However, in oval-shaped or flattened canals, recesses usually remain unprepared when using these instruments [1]. Bacteria and tissue remnants may remain unaffected in unprepared areas, even when sodium hypochlorite is used for irrigation [2]. Different instrument systems leave from 10 to 80% of the full canal surface area unprepared [3]. In addition, a significant amount of hard tissue debris can accumulate in the recesses of oval canals [4]. Hard tissue debris is produced by the cutting action of instruments on dentin and may contain bacteria and necrotic tissue. Hard tissue debris may also make it difficult to fill the root canal system correctly [5]. Another concern related to root canal preparation using tapered instruments in reciprocating or rotary motions is the creation of forces that can lead to dentinal defects such as cracks and root fractures [6, 7], which may compromise the long-term retention of the tooth.
Many studies have compared rotary and reciprocating systems concerning the amount of unprepared root canal wall surfaces [8,9,10], accumulated hard tissue debris [11, 12], and dentinal defect formation [13, 14]. However, a common concern with these studies relates to specimen selection. Most of them used extracted teeth, stored under distinct conditions, from different individuals and thereby with different mechanical properties of the dentin. These factors can make it challenging to match teeth for anatomical similarities and distribution through the experimental groups. Another limitation of using extracted teeth is that the conditions for handling and preparation are rather artificial, and no efforts have been usually made to reproduce the real condition. For instance, it seems relevant to simulate the vapor lock effect [15] and the apical barrier provided by the periodontal ligament when debris accumulation is under investigation. The use of contralateral teeth from human cadavers may help circumvent those limitations.
Micro-computed tomography (micro-CT) has been widely used to evaluate the amount of unprepared areas, hard tissue debris accumulation, and dentinal defect formation after preparation [16,17,18]. Because of its non-destructive nature, preoperative and postoperative scans can be superimposed to evaluate changes in the root canal shape and untouched areas can be identified; accumulated hard tissue debris and dentinal defects can also be detected and quantified [16, 19, 20].
Therefore, the purpose of this study was threefold: to compare the amount of unprepared areas, accumulated hard tissue debris, and dentinal defect formation after root canal preparation of contralateral teeth from a cadaveric model using either a reciprocating (Reciproc) or a continuously rotating instrument (Mtwo), varying the final apical preparation size.
Materials and methods
The sample size was calculated using G* Power 3.1.9.7 (Universität Kiel, Germany), which revealed that at least 12 teeth per group would be required for the unprepared areas and accumulated hard tissue debris analysis with an alpha-type error of 0.05 and 95% power [21]. Twenty-two teeth per group were included, considering the possibility of sample loss during the experiment and to make the data more robust for analysis.
Forty-four incisors with intact crowns, completely formed roots, no evidence of root resorption, and a single root canal were selected on the basis of micro-CT scans (see below) of 11 human anterior mandible segments. The material was obtained from corpses aged between 60 and 80 years, maintained infused and immersed in 10% formalin in the Department of Anatomy, Dental School, Iguaçu University. Mandible segments were obtained by parasymphyseal sectioning. The Institutional Ethics Committee provided approval for the study protocol (approval number 1.696.413). For each segment, central and lateral incisors from one side were assigned to one group and their contralateral to the other group, according to the root canal preparation system used.
Initial micro-CT scanning
The mandible segments were mounted on aluminum support and scanned in a SkyScan 1173 (Bruker Micro-CT, Kontich, Belgium) device with 114 μA and 70 Kv source. The scanning parameters included a 0.5° rotation step, a 360° rotation around the vertical axis, 9.9-μm pixel size, and 1.0-mm-thick aluminum filter. The following parameters were used in the software NRecon v.1.7.4.6 (Bruker micro-CT) to reconstruct the specimen’s image: beam hardening correction set in 50%, ring artifact correction of 5, and smoothing set in 0.
Root canal preparation
Before root canal preparation, periapical radiographs were obtained from all incisors using a Kodak RGV 6100 digital sensor (Kodak Dental Systems, Rochester, NY) and a Spectro 70X Seletronic X-ray source (Dabi Atlante Ltda., Ribeirão Preto, São Paulo, Brazil) by the paralleling technique. The setting parameters included 70 Kvp, 8 mA, and 0.3 s of exposure. The tooth length was obtained by using the software provided by the device’s manufacturer.
Each individual tooth was isolated with a rubber dam, and a conventional endodontic access cavity was prepared using 1012 and 3083 burs (KG Sorensen) at high speed under copious irrigation with water. The root canals were irrigated with 2 mL 2.5% NaOCl, and the apical foramen patency was checked with small K-type files (FKG Dentaire, La Chaux-de-Fonds, Switzerland). The working length (WL) was established 1 mm short of the root apex with the help of radiographs. A metal stop, made exclusively for this study, was used to ensure the accuracy and maintenance of the WL during instrumentation. The stop was maintained fixed at the instrument by using two metal screws. Next, hand K-type files sizes 10, 15, and 20 were sequentially worked at the WL to standardize the apical diameter of the canals prior to preparation. Canals were irrigated with 2 mL NaOCl before and after each file size.
The incisors were distributed into two groups according to the instrumentation technique. Contralateral teeth were prepared with different systems: the left teeth were prepared with the Reciproc system, and the right teeth were instrumented with the Mtwo system.
Prior to using each instrument, the root canal was irrigated with 2.5% NaOCl for 30 s under a flow rate of 4 mL/min, delivered by an open-ended NaviTip 30-G needle (Ultradent, South Jordan, UT).
Mtwo group
Mtwo instruments were driven by a VDW Silver motor (VDW, Munich, Germany) in continuous rotation at 280 rpm and torque as recommended by the manufacturer for each instrument: 10/.04 and 15/.05 (1 N.cm torque); 20/.06 and 25/.06 (2 N.cm torque); and 30/.05, 35/.05, 40/.04, and 50/.04 (1 N.cm torque). The instruments were used up to the WL, with short up-and-down movements, combined with brushing.
Reciproc group
Reciproc instruments R40 and R50 were operated in the VDW Silver engine in “Reciproc All” mode. Preparation was performed by introducing the instrument in the canal with slight apical pressure and up-and-down movements not exceeding 3 mm of amplitude. After every three strokes (one cycle), the instrument was removed and cleaned with gauze, and the patency of the apical canal was verified with a size 10 K-file. Five cycles of instrumentation were performed with the R40 instrument (the mean number of cycles to reach the WL was tested in a pilot study). Five cycles were carried out even when the instrument reached the WL before the fifth cycle in order to standardize the volume and retention time of NaOCl. Next, the tooth was subject to one more micro-CT scan (see below), and one cycle of instrumentation with the R50 instrument was performed. Only one cycle was necessary for the R50 to reach the WL of all teeth.
A single operator performed all root canal preparation procedures, and each instrument was used to prepare only two canals.
Irrigation conditions
Irrigation was performed throughout preparation with a NaviTip needle placed 3 mm short of WL. The irrigant was delivered with the aid of a peristaltic pump (VATEA, ReDent-Nova, Ra’nana, Israel) to keep the flow rate at 4 mL/min. The irrigant was simultaneously aspirated by a cannula positioned at the canal orifice.
After instrumentation, each root canal was irrigated with 5 mL 17% EDTA followed by 3 mL 2.5% NaOCl. The canal was dried with paper point sizes 40 and 50. In both groups, the total volume and the retention time of NaOCl were respectively standardized at 19 mL and 260 s for preparation up to the instrument size 40, and 26 mL and 340 s for preparation up to the instrument size 50.
Postpreparation micro-CT analyses
Micro-CT scans were taken after preparation with the instruments size 40 and size 50 in both groups (Fig. 2). The same micro-CT parameters used in the initial scanning were used for these postpreparation scans.
Evaluation of the unprepared canal areas
The mandible segments were kept intact during all evaluations. However, for better image processing, each tooth specimen was digitally separated in blocks. The 3D Slicer 4.4.0 software (http://www.slicer.org) was used to co-register the pre and postpreparation images. Next, the volume (in mm3) and the surface area (in mm2), as well as the untouched root canal areas (static voxels), were measured using the Image J 1.50d software (National Institutes of Health, Bethesda, MD). Analyses involved the full canal length (up to 10-mm short of WL) and the 4-mm apical portion. Finally, the CTVol v.2.2.3.0 software (Bruker micro-CT) was used to set the color-coded standard for root canal models. Green was used for the preoperative canal surface, redfor the instrument size 40, and blue for the instrument size 50. One operator, blinded to the groups, performed all micro-CT analyses.
Evaluation of accumulated hard tissue debris
The quantification of accumulated hard tissue debris was performed as previously described [16], and expressed as a percentage of the initial volume of the root canal of each specimen. All materials with a density similar to dentin observed in the postpreparation micro-CT scans in regions previously empty of the unprepared canal (pre-preparation scan) were considered hard tissue debris. Debris volume (mm3) was quantified by the difference between pre-preparation and postpreparation images. All analyses were made using the Image J 1.50d software (National Institutes of Health). The images obtained were rendered three-dimensionally.
Evaluation of dentinal defects formation
Preoperative and postoperative images were examined by 2 pre-calibrated evaluators to identify the presence of dentinal defects in each cross-sectional slice and for each tooth. Calibration was performed with a set of 30 microtomographic images of extracted single-rooted teeth from another study (still unpublished), 15 containing dentinal defects and 15 without defects. The defects were produced by instrumenting the canals with manual files and were confirmed by scanning electron microscopy.
First, the postoperative images were analyzed, and the number of cross-sectional slices until a dentinal defect (if present) was detected was recorded. Subsequently, the corresponding preoperative cross-sectional slice was also examined to verify if the dentinal defect had already been present before preparation. The image analysis was repeated twice by each examiner, at 2-week intervals. Interobserver divergencies were solved by joint discussion. Intra-examiner and inter-examiner reliability was calculated using the Cohen Kappa coefficient. The crack incidence was evaluated per teeth. When a dentinal defect formation was detected, its longitudinal extension was evaluated by the number of cross-sectional slices in which the crack could be detected. The detected post-treatment dentinal defects were classified as incomplete crack, complete crack, and root fracture.
Statistical analysis
The Shapiro-Wilk test was applied to verify data normality. Accordingly, the dependent t-test was used to compare the intergroup and intragroup differences in the amount of unprepared canal surface areas in the full canal length. The Wilcoxon matched-pairs test was used for the other intergroup and intragroup comparisons involving data from unprepared surface areas and accumulated hard tissue debris. The Pearson correlation test was used to verify if there was a correlation between the amount of unprepared areas and the amount of accumulated debris. The Fisher’s exact test was used to compare the intragroup incidence of dentinal defect formation. The level of significance was set at 5% for all statistical tests (P < .05).
Results
Two teeth were excluded during the experiment, one from the Reciproc group due to fracture of a size 40 instrument and another from the Mtwo group because patency of the apical foramen was not achieved. Therefore, the analysis was performed in 42 teeth, 21 prepared with each instrumentation system.
Unprepared canal areas
After preparation to instruments size 40, the mean amount of unprepared surface areas in the full canal length was similar between the tested systems (8.1% in the Reciproc group and 7.7% in the Mtwo group) (P > .05) (Figs. 1 and 2, Table 1). However, a significant difference was observed between groups when only the apical 4-mm portion was evaluated (4.2% in the Reciproc group and 6.2% in the Mtwo group) (P < .05) (Figs. 1 and 2, Table 1). Overall, unprepared areas were observed in all specimens prepared to size 40, regardless of the system, with a mean 7.9 ± 2.4 mm2 and 5.2 ± 3.5 mm2 for the full canal length and the apical 4 mm, respectively.

Box plot graphs. Amount of unprepared areas (UpA) following preparation with instruments sizes 40 (a) and 50 (b), considering the full canal length and the apical 4 mm. Amount of accumulated hard tissue debris (HTD) following preparation with instruments sizes 40 (c) and 50 (d), considering the full canal length and the apical 4 mm

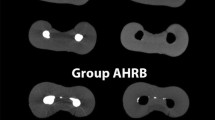
Superimposed micro-computed tomographic scans taken before (green) and after root canal preparation (red and blue for final preparation sizes 40 (a) and 50 (b)), showing unprepared areas in the full canal length. Accumulated hard tissue debris (HTD) in the full canal length after preparation sizes 40 (c) and 50 (d). Accumulated hard tissue debris (HTD) before root canal preparation (e) and after enlargement to sizes 40 (f) and 50 (g), respectively. Images were obtained from the same cross-sectional level located 5-mm short the root apex
After preparation to instrument's size 50, the amount of unprepared surface areas was similar between the tested systems, regardless of the evaluation length (full canal or apical canal) (P > .05). The means of unprepared areas in the full canal were 4.1% for the Reciproc group and 3.9% for the Mtwo group (Table 1); corresponding figures in the apical 4 mm were 1.9% and 1.8%, respectively (Figs. 1 and 2, Table 1). Overall, unprepared areas were observed in all teeth instrumented to size 50, irrespective of the test system, with a mean 4.0 ± 1.9 mm2 and 1.9 ± 1.6 mm2 for the full canal length and the apical 4 mm, respectively.
Intragroup analyses revealed a significant decrease in the amount of unprepared surface areas after enlarging from size 40 to 50 with both instrument systems and in both evaluation levels (P < .05).
Accumulated hard tissue debris
The mean amount of accumulated hard tissue debris after preparation size 40 was similar between the tested systems in both levels evaluated (P > .05). The means for the full canal length were 14.1% in the Reciproc group and 15.3% in the Mtwo group; for the apical 4-mm segment, the means were 5.1% in the Reciproc group and 5.1% in the Mtwo group (Figs. 1 and 2, Table 2). After preparation to size 40, hard tissue debris was detected in all specimens irrespective of the tested system, with a mean 1.1 ± 0.6 and 0.5 ± 0.3 mm3 for the full canal length and the apical 4 mm, respectively.
Preparation to size 50 revealed a significant difference in accumulated hard tissue debris between the test systems at the full canal length: 31.6% in the Reciproc group and 42.5% in the Mtwo group (P < .05) (Figs. 1 and 2, Table 2). There was no significant difference between groups in the apical 4 mm (P > .05); the means were 14.6% for Reciproc and 19% for Mtwo instruments (Figs. 1 and 2, Table 2). Hard tissue debris after preparation size 50 also occurred in all teeth independent of the system, with a mean 2.2 ± 1.2 mm3 and 7.5 ± 10.9 mm3 for the full canal length and the apical 4 mm, respectively.
Intragroup analyses revealed a significant increase in the amount of accumulated hard tissue debris after canal enlargement from size 40 to size 50 with both instrument systems and in both levels evaluated (P < .05) (Figs. 1 and 2, Table 2).
There was no correlation between the amount of unprepared areas and accumulated hard tissue debris.
Dentinal defect formation
The intra-examiner and inter-examiner reliability was excellent and substantial not only for evaluation of dentinal defects incidence but also their extension (Cohen’s Kappa = 1.0 and 0.97, respectively).
Incidence and location
Dentinal defects were detected in 4 teeth prior to root canal preparation (1 tooth from the Mtwo group and 3 from the Reciproc group). In teeth without any pre-existing dentinal defect (n = 38), dentinal defect formation occurred in 2 teeth (9.5%) from different mandibles in the Reciproc group (1 complete crack in the apical third of the root (Fig. 3b), and 1 root fracture in the apical third (Fig. 3d)) and in 2 teeth (9.5%) from different mandibles in the Mtwo group (1 incomplete crack in the middle third of the root (Fig. 3f) and 1 root fracture in the apical third (Fig. 3h)) after preparation to size 40. No other defects were found after further enlargement. No new dentinal defect was detected in teeth with pre-existing dentinal defects. There were no statistically significant differences in the incidence of dentinal defects in both intragroup and intergroup analysis (P > .05) (Table 3 and Supplementary Table).

Micro-CT images taken before and after root canal preparation with Reciproc (a and b, c, and d, respectively) and Mtwo (e and f, g and h, respectively). No dentinal defect is observed in the preoperative images (a, c, e, and g). However, dentinal defects are easily visualized in the postoperative images: a complete crack in the apical third of the root (b), root fractures in the apical third (d and h), and an incomplete crack in the middle third of the root (f)
Extension
The amount of cross-sectional slices in which a dentinal defect was detected increased after enlarging from size 40 to size 50 with both instrument systems. However, this was not observed in teeth with the pre-existing dentinal defects (Supplementary Table).
Discussion
Reciproc and Mtwo were chosen for the present study because of the following reasons: both systems are currently very popular among clinicians; the former is a single-file and the latter is a multifile system; they are produced by the same manufacturer; the former is operated using reciprocating movements, while the latter works in continuous rotation; and they have the same cross-section design. Because one purpose of this study was to compare the effects of different final apical preparation sizes in the amount of unprepared canal surface areas, hard tissue debris accumulation, and dentinal defects formation, a final preparation size 50 was also tested. However, it is important to point out that this instrument diameter is not commonly recommended for apical preparation in mandibular incisors.
No significant difference in unprepared areas was observed between the two systems when the full canal was evaluated. This is in agreement with a previous study using extracted teeth [9] that did not find differences in unprepared areas between these systems when the full canal length was evaluated either. However, a separate analysis of the apical canal after enlargement to size 40 revealed better results for Reciproc, even though no difference in the apical canal was observed for preparation up to size 50. These findings may be explained by the fact that the difference in taper of the tested systems over their last 3-mm segment is higher for the instrument 40 (Reciproc = .06 and Mtwo = .04 mm/mm) than 50 (Reciproc = .05 and Mtwo = .04 mm/mm). Studies confirmed that the occurrence of unprepared areas after instrumentation could be related to the instrument dimensions [8, 10]. Apparently, the movement type (reciprocating or continuous rotation) had no significant influence in the results for unprepared areas, given the lack of difference in most analyses. Brushing was applied to Mtwo instruments as recommended by the manufacturer, but this had no apparent effects on the results either.
Intragroup comparisons for both systems showed that as the final preparation size increased, the amount of unprepared areas decreased significantly. This finding was expected and is in consonance with previous studies [22, 23]. Clinical and ex vivo studies have demonstrated that the larger the root canal preparation, the greater the bacterial reduction [24, 25]. Therefore, one of the reasons for improved disinfection may be the increase in prepared areas, enhancing the removal of infected dentin and bacterial biofilms adhered to the canal walls. The treatment outcome of teeth with apical periodontitis has been shown to be positively affected by larger preparations [26]. However, overenlargement of the canal should be avoided in order not to unnecessarily remove dentin and put the tooth in an increased risk of fracture.
The amount of accumulated hard tissue debris was not different between the two tested instrumentation systems when the final preparation size was 40. This result is in accordance with a previous study using extracted mandibular incisors that did not find differences in the amount of debris comparing Reciproc and Mtwo systems [4]. Similar results were also observed in curved canals using different instrument diameters [19, 27]. On the other hand, significantly less debris was accumulated in the Reciproc group when the preparation size was 50, considering the full canal length. A previous study found opposite results as the amount of accumulated debris was higher with a reciprocating system (WaveOne) in comparison with rotary instruments (ProTaper) to a preparation size 25/.08 in mandibular molar mesial canals connected by an isthmus [12]. Differences between studies may have been due to variables such as tooth type, instruments used, apical preparation size, and presence of isthmuses, which are very difficult to standardize.
In contrast to a previous study [19], the intragroup analyses revealed that debris accumulation was higher after larger preparations. The amount of debris was more than twice higher for canals prepared to size 50, which could be explained because as the more dentin is cut, more debris is produced. These findings reinforce the need for using adjunctive procedures, such as irrigation agitation with passive ultrasonic irrigation [11], XP-Endo Finisher instrument [28], and sonic devices [29] to improve root canal cleaning and disinfection.
Studies have demonstrated that engine-driven instrumentation generates stress on the root canal walls, which may create dentinal defects, independent of the activation mode [30, 31]. In the present study, root canal preparation with Mtwo or Reciproc produced dentinal defects in teeth without pre-existing defects (2 for Reciproc and 2 for Mtwo). These dentinal defects were detected after the final preparation size 40, and no additional defect was verified when the preparation size was increased to 50. However, the longitudinal extension of these defects was aggravated after enlargement to size 50. Other studies also found an increased number and length of dentinal defects associated with rotary and reciprocating root canal preparations [30, 32]. On the other hand, the present findings are in disagreement with a study in which root canal shaping with rotary and reciprocating systems did not produce dentinal defects, and the longitudinal length of the pre-existing defects was not modified [13]. However, the pixel size in the previous study was bigger (33 μm) in comparison with the present one (9.9 μm), which could lead to false-negative results.
Some other studies did not mention the number of teeth with new dentinal defects [20, 33, 34], referring only to the number of cross-sectional slices in which dentinal defects were detected. Therefore, these studies considered the number of slices in which a dentinal defect was detected as the number of defects, which may lead to misinterpretation. It is important to consider that the analysis of the number of slices with dentinal defect may be referring not only to the number of different defects but also the longitudinal extension of the same defect. In this context, a direct comparison of findings from these studies with the present one, in which only one dentinal defect was detected per tooth, is compromised.
One of the strengths of the present study was the use of cadaveric human mandibles. This allowed the comparison of both systems in the same anatomical piece with the teeth positioned in their original alveolar bone alveolus, with preserved periodontal ligament. This is important to simulate the clinical conditions of irrigation, resistance to debris and irrigant extrusion, and stress dissipation during canal preparation; these conditions have not been usually addressed in previous studies. In addition, the model also allowed for a better simulation of the clinical condition, including working under rubber dam isolation. Contralateral teeth were used for comparing Reciproc and Mtwo, permitting optimal pairwise matching analysis. This is crucial for studies comparing the shaping and cleaning abilities of instruments and techniques. Another advantage of the method used was that the teeth were intact and had the pulps preserved (although fixed); this is closer to the clinical conditions than using extracted teeth and has not been used in most studies evaluating accumulated hard tissue debris. Finally, micro-CT was chosen for the 3-dimensional assessments because it is a non-invasive and reproducible imaging method with a high resolution. However, it is important to emphasize that the present findings (obtained in cadavers with age ranging from 60 to 80 years) may not be directly applicable to younger teeth, since aging results in an increase in both the rate of damage initiation and propagation in dentin [35, 36].
Conclusions
Mtwo left more unprepared areas than Reciproc in the apical portion of the canals when the final apical preparation size was 40. The amount of accumulated hard tissue debris was similar between the tested systems at this file size. While the amount of unprepared surface areas decreased in both groups after larger preparation (size 50), the volume of accumulated hard tissue debris increased. Preparation with both systems produced dentinal defects and their longitudinal extension increased after further enlargement from instrument size 40 to size 50.
References
Wu MK, R'Oris A, Barkis D, Wesselink PR (2000) Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 89:739–743. https://doi.org/10.1067/moe.2000.106344
Perez AR, Ricucci D, Vieira GCS, Provenzano JC, Alves FRF, Marceliano-Alves MF, Rocas IN, Siqueira JF Jr (2020) Cleaning, shaping, and disinfecting abilities of 2 instrument systems as evaluated by a correlative micro-computed tomographic and histobacteriologic approach. J Endod 46:846–857. https://doi.org/10.1016/j.joen.2020.03.017
Siqueira JF Jr, Rôças IN, Marceliano-Alves MF, Pérez AR, Ricucci D (2018) Unprepared root canal surface areas: causes, clinical implications, and therapeutic strategies. Braz Oral Res 32:e65. https://doi.org/10.1590/1807-3107bor-2018.vol32.0065
Espir CG, Nascimento-Mendes CA, Guerreiro-Tanomaru JM, Cavenago BC, Hungaro Duarte MA, Tanomaru-Filho M (2018) Shaping ability of rotary or reciprocating systems for oval root canal preparation: a micro-computed tomography study. Clin Oral Investig 22:3189–3194. https://doi.org/10.1007/s00784-018-2411-4
Endal U, Shen Y, Knut A, Gao Y, Haapasalo M (2011) A high-resolution computed tomographic study of changes in root canal isthmus area by instrumentation and root filling. J Endod 37:223–227. https://doi.org/10.1016/j.joen.2010.10.012
Abou El Nasr HM, Abd El Kader KG (2014) Dentinal damage and fracture resistance of oval roots prepared with single-file systems using different kinematics. J Endod 40:849–851. https://doi.org/10.1016/j.joen.2013.09.020
Rivera ER, Walton RE (2009) Longitudinal tooth fractures: findings that contribute to complex endodontic diagnoses. Endod Top 16:3
Busquim S, Cunha RS, Freire L, Gavini G, Machado ME, Santos M (2015) A micro-computed tomography evaluation of long-oval canal preparation using reciprocating or rotary systems. Int Endod J 48:1001–1006. https://doi.org/10.1111/iej.12398
Espir CG, Nascimento-Mendes CA, Guerreiro-Tanomaru JM, Freire LG, Gavini G, Tanomaru-Filho M (2018) Counterclockwise or clockwise reciprocating motion for oval root canal preparation: a micro-CT analysis. Int Endod J 51:541–548. https://doi.org/10.1111/iej.12776
Zuolo ML, Zaia AA, Belladonna FG, Silva E, Souza EM, Versiani MA, Lopes RT, De-Deus G (2017) Micro-CT assessment of the shaping ability of four root canal instrumentation systems in oval-shaped canals. Int Endod J. https://doi.org/10.1111/iej.12810
Paque F, Boessler C, Zehnder M (2011) Accumulated hard tissue debris levels in mesial roots of mandibular molars after sequential irrigation steps. Int Endod J 44:148–153. https://doi.org/10.1111/j.1365-2591.2010.01823.x
Robinson JP, Lumley PJ, Cooper PR, Grover LM, Walmsley AD (2013) Reciprocating root canal technique induces greater debris accumulation than a continuous rotary technique as assessed by 3-dimensional micro-computed tomography. J Endod 39:1067–1070. https://doi.org/10.1016/j.joen.2013.04.003
de Oliveira BP, Camara AC, Duarte DA, Heck RJ, Antonino ACD, Aguiar CM (2017) Micro-computed tomographic analysis of apical microcracks before and after root canal preparation by hand, rotary, and reciprocating instruments at different working lengths. J Endod 43:1143–1147. https://doi.org/10.1016/j.joen.2017.01.017
Stringheta CP, Pelegrine RA, Kato AS, Freire LG, Iglecias EF, Gavini G, Bueno C (2017) Micro-computed tomography versus the cross-sectioning method to evaluate dentin defects induced by different mechanized instrumentation techniques. J Endod 43:2102–2107. https://doi.org/10.1016/j.joen.2017.07.015
Tay FR, Gu LS, Schoeffel GJ, Wimmer C, Susin L, Zhang K, Arun SN, Kim J, Looney SW, Pashley DH (2010) Effect of vapor lock on root canal debridement by using a side-vented needle for positive-pressure irrigant delivery. J Endod 36:745–750. https://doi.org/10.1016/j.joen.2009.11.022
Versiani MA, Alves FR, Andrade-Junior CV, Marceliano-Alves MF, Provenzano JC, Rocas IN, Sousa-Neto MD, Siqueira JF Jr (2016) Micro-CT evaluation of the efficacy of hard-tissue removal from the root canal and isthmus area by positive and negative pressure irrigation systems. Int Endod J 49:1079–1087. https://doi.org/10.1111/iej.12559
Siqueira JF Jr, Perez AR, Marceliano-Alves MF, Provenzano JC, Silva SG, Pires FR, Vieira GC, Rôças IN, Alves FR (2018) What happens to unprepared root canal walls: a correlative analysis using micro-computed tomography and histology/scanning electron microscopy. Int Endod J 51:501–508. https://doi.org/10.1111/iej.12753
Rodig T, Kramer J, Muller C, Wiegand A, Haupt F, Rizk M (2019) Incidence of microcracks after preparation of straight and curved root canals with three different NiTi instrumentation techniques assessed by micro-CT. Aust Endod J 45:394–399. https://doi.org/10.1111/aej.12339
De-Deus G, Marins J, Silva EJ, Souza E, Belladonna FG, Reis C, Machado AS, Lopes RT, Versiani MA, Paciornik S, Neves AA (2015) Accumulated hard tissue debris produced during reciprocating and rotary nickel-titanium canal preparation. J Endod 41:676–681. https://doi.org/10.1016/j.joen.2014.11.028
Bayram HM, Bayram E, Ocak M, Uzuner MB, Geneci F, Celik HH (2017) Micro-computed tomographic evaluation of dentinal microcrack formation after using new heat-treated nickel-titanium systems. J Endod 43:1736–1739. https://doi.org/10.1016/j.joen.2017.05.024
Vieira GCS, Perez AR, Alves FRF, Provenzano JC, Mdala I, Siqueira JF Jr, Rocas IN (2020) Impact of contracted endodontic cavities on root canal disinfection and shaping. J Endod 46:655–661. https://doi.org/10.1016/j.joen.2020.02.002
Perez AR, Alves FRF, Marceliano-Alves MF, Provenzano JC, Goncalves LS, Neves AA, Siqueira JF Jr (2017) Effects of increased apical enlargement on the amount of unprepared areas and coronal dentine removal: a micro-computed tomography study. Int Endod J 51:684–690. https://doi.org/10.1111/iej.12873
Peters OA, Arias A, Paque F (2015) A micro-computed tomographic assessment of root canal preparation with a novel instrument, TRUShape, in mesial roots of mandibular molars. J Endod 41:1545–1550. https://doi.org/10.1016/j.joen.2015.06.007
Rodrigues RCV, Zandi H, Kristoffersen AK, Enersen M, Mdala I, Orstavik D, Rocas IN, Siqueira JF Jr (2017) Influence of the apical preparation size and the irrigant type on bacterial reduction in root canal-treated teeth with apical periodontitis. J Endod 43:1058–1063. https://doi.org/10.1016/j.joen.2017.02.004
Siqueira JF Jr, Lima KC, Magalhaes FA, Lopes HP, de Uzeda M (1999) Mechanical reduction of the bacterial population in the root canal by three instrumentation techniques. J Endod 25:332–335. https://doi.org/10.1016/S0099-2399(06)81166-0
Saini HR, Tewari S, Sangwan P, Duhan J, Gupta A (2012) Effect of different apical preparation sizes on outcome of primary endodontic treatment: a randomized controlled trial. J Endod 38:1309–1315. https://doi.org/10.1016/j.joen.2012.06.024
Burklein S, Hinschitza K, Dammaschke T, Schafer E (2012) Shaping ability and cleaning effectiveness of two single-file systems in severely curved root canals of extracted teeth: reciproc and WaveOne versus Mtwo and ProTaper. Int Endod J 45:449–461. https://doi.org/10.1111/j.1365-2591.2011.01996.x
Leoni GB, Versiani MA, Silva-Sousa YT, Bruniera JF, Pecora JD, Sousa-Neto MD (2017) Ex vivo evaluation of four final irrigation protocols on the removal of hard-tissue debris from the mesial root canal system of mandibular first molars. Int Endod J 50:398–406. https://doi.org/10.1111/iej.12630
Blank-Goncalves LM, Nabeshima CK, Martins GH, Machado ME (2011) Qualitative analysis of the removal of the smear layer in the apical third of curved roots: conventional irrigation versus activation systems. J Endod 37:1268–1271. https://doi.org/10.1016/j.joen.2011.06.009
Burklein S, Tsotsis P, Schafer E (2013) Incidence of dentinal defects after root canal preparation: reciprocating versus rotary instrumentation. J Endod 39:501–504. https://doi.org/10.1016/j.joen.2012.11.045
Karatas E, Gunduz HA, Kirici DO, Arslan H, Topcu MC, Yeter KY (2015) Dentinal crack formation during root canal preparations by the twisted file adaptive, ProTaper Next, ProTaper Universal, and WaveOne instruments. J Endod 41:261–264. https://doi.org/10.1016/j.joen.2014.10.019
Pop I, Manoharan A, Zanini F, Tromba G, Patel S, Foschi F (2015) Synchrotron light-based muCT to analyse the presence of dentinal microcracks post-rotary and reciprocating NiTi instrumentation. Clin Oral Investig 19:11–16. https://doi.org/10.1007/s00784-014-1206-5
Zuolo ML, De-Deus G, Belladonna FG, Silva EJ, Lopes RT, Souza EM, Versiani MA, Zaia AA (2017) Micro-computed tomography assessment of dentinal micro-cracks after root canal preparation with TRUShape and self-adjusting file systems. J Endod 43:619–622. https://doi.org/10.1016/j.joen.2016.11.013
Aksoy C, Keris EY, Yaman SD, Ocak M, Geneci F, Celik HH (2019) Evaluation of XP-endo Shaper, Reciproc Blue, and ProTaper Universal NiTi systems on dentinal microcrack formation using micro-computed tomography. J Endod 45:338–342. https://doi.org/10.1016/j.joen.2018.12.005
Bajaj D, Sundaram N, Nazari A, Arola D (2006) Age, dehydration and fatigue crack growth in dentin. Biomaterials 27:2507–2517. https://doi.org/10.1016/j.biomaterials.2005.11.035
Arola D, Reprogel RK (2005) Effects of aging on the mechanical behavior of human dentin. Biomaterials 26:4051–4061. https://doi.org/10.1016/j.biomaterials.2004.10.029
Acknowledgements
Our respect and gratitude to the donor-cadaver-patients.
Funding
This study was supported by grants from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazilian Governmental Institutions.
Author information
Authors and Affiliations
Contributions
Andrea F. Campello — Teeth selection and preparation, root canal preparation, and data collection.
Marília F. Marceliano-Alves — Microtomographic analysis.
José F. Siqueira Jr — Study concept/design and manuscript writing and revision.
Simone C. Fonseca — Teeth selection and preparation.
Ricardo T. Lopes — Microtomographic analysis.
Flávio R. F. Alves — Study concept/design, data analysis, statistical analysis, and manuscript writing and revision.
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 53 kb)
Rights and permissions
About this article

Cite this article
Campello, A.F., Marceliano-Alves, M.F., Siqueira, J.F. et al. Unprepared surface areas, accumulated hard tissue debris, and dentinal crack formation after preparation using reciprocating or rotary instruments: a study in human cadavers. Clin Oral Invest 25, 6239–6248 (2021). https://doi.org/10.1007/s00784-021-03922-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-021-03922-8