
Abstract
Objectives
To evaluate the shaping ability and cleaning after oval root canal preparation using one or more instruments in reciprocating or rotary motion.
Materials and methods
Oval-shaped mandibular incisors were selected, based on the radiographic diameter (2 ≤ diameter ratio ≤ 4), and assigned according to root canal preparation (n = 18): single-file (Reciproc R40); two reciprocating files (Unicone size 20 and 40, .06 taper) or Mtwo rotary files until a size 40, .06 taper instrument. Root canal preparations were performed using an open root canal model. Scanning was performed before and after preparation using SkyScan 1176 with a voxel size of 17.42 μm. Volume, percentage of debris, and percentage of uninstrumented surface were analyzed in the entire root canal and in each root canal third. Data were compared using ANOVA and Tukey or Kruskal-Wallis and Dunn tests (α = 5%).
Results
The initial volume were similar among the groups (p > .05). Unicone preparation was associated with higher debris, increase in root canal volume and uninstrumented surface in entire root canal and in the middle third (P < .05). Mtwo was associated with lower uninstrumented surface in the entire root canal and in the cervical third. The apical third were similar for the three preparations.
Conclusions
Unicone system using two instruments in reciprocating motion resulted in higher increase in volume. However, less remaining debris was observed when Reciproc single-file and Mtwo rotary systems were used.
Clinical relevance
A preparation that volumetrically increases the root canal is not necessarily associated with better cleaning. Shaping and hard-tissue debris removal depends on root canal anatomy, kinematics, number of instruments, and instrument design.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Root canal preparation may be influenced by the design [1], kinematics [2,3,4], diameter and taper [5], and the number of instruments used [6, 7]. Reciprocating motion allows preparation with a lower number of instruments [8]. However, the importance of using more than one instrument to promote better root canal cleaning with less debris and uninstrumented root canal wall, including different diameters, has been demonstrated [6, 7, 9].
Oval-shaped and flattened root canals may make it difficult to root canal preparation, especially because they present areas that are difficult to access, favoring the accumulation of debris and microorganisms [10, 11]. The oval-shaped morphology has been studied [3, 4, 12, 13] and self-adjusting instruments [14] or different additional disinfection procedures [15, 16] have been proposed to improve cleaning. Nevertheless, some regions of the canal may remain unprepared [3, 17, 18].
The Unicone System (Medin, Nove Mesto Morave, Czech Republic) is composed of three instruments for reciprocating motion, with diameters #20, #25, and #40 and taper 6%, with conical core and smaller escape area [19]. It had less cyclic fatigue resistance when compared with the Reciproc R25 and WaveOne Primary instruments [20].
Reciproc is a single-file instrument made of a special NiTi alloy (M-Wire), used with reciprocating counterclockwise motion and available in three different sizes (R25, R40 and R50) to be used in different canal diameter. This instrument promotes preparation similar to Self-Adjusting File, WaveOne, and Protaper systems when used for oval-shaped root canal preparation [3] and greater increase in the root canal volume when compared with the BioRace rotary system size 40, .04 taper file in long oval root canals [21]. MTwo (VDW, Munich, Germany) is a system of NiTi files with S-shaped cross-sectional design, manufactured to operate in a rotary clockwise motion. In comparison to Reciproc, it demonstrated similar apical preparation in mandibular molars [22].
The aim of this study was to evaluate by means of micro-computed tomography (micro-CT) the shaping ability and cleaning effectiveness of different root canal preparation systems (Reciproc, Unicone and MTwo) in oval root canals.
Material and methods
Selection of teeth and preparation
Extracted mandibular incisors (CEP #31725014.7.0000.5416) were selected by using digital radiography (Kodak RVG 6100). Mesiodistal and buccolingual length measurements were used to define the diameter ratio (DR) at 9 mm from anatomic apex of each specimen. Single rooted teeth, with long oval canals (2 ≤ DR ≤ 4), completely formed apices and a root length of 20 ± 2 mm were initially selected. Sixty-six teeth were selected and stored in a glass bottle containing 0.1% thymol solution at 5 °C.
The selected specimens were scanned using a high-definition micro-CT scanner SkyScan 1176 (SkyScan 1176, Bruker-microCT, Kontich, Belgium) at 70 kV, 353uA, 360° rotations, a 0.5-mm-thick aluminum filter and 0.5° rotation step, resulting in an image with 17.42 μm voxel size. An initial reconstruction using NRecon software (NRecon v.1.6.3, Bruker-microCT) and analysis using CTAn software (CTAn v.1.14.4, Bruker-microCT) was performed according to morphological parameters of the root canals (length, volume, and surface area) to final selection of specimens. Fifty-four root canals (n = 54) were randomly assigned to one of the three different instrumentation groups.
After washing in water for 48 h, a conventional access to the root canals was created using high-speed diamond burs (n2, KG Sorensen, São Paulo, Brazil) and the patency of the root canals was confirmed when a #10 K-file (Dentsply Sirona, Ballaigues, Switzerland) was visible at the apical foramen. The working length was then set at 1.0 mm shorter and a single operator with clinical experience prepared all samples.
Root canal preparation with Reciproc 40 (n = 18): R40 (size 40, .06 taper) instruments were activated in reciprocating motion (VDW.SILVER, VDW GmbH), according to manufacturer’s instructions. Root canal preparations were performed using an open root canal model for all experimental groups. The instrument was gradually inserted into root canal in a slow in-and-out motion in the three levels (cervical, middle, and apical), with a brushing motion against the walls. After preparation of each third, the instrument was cleaned in a gauze and the root canal was irrigated. A new R40 instrument was used for each root canal preparation.
Root canal preparation with UniCone 20.06 and 40.06 (n = 18): a Unicone 20 (size 20, .06 taper) instrument was used before the Unicone 40 (size 40, .06 taper) instrument in reciprocating motion (VDW.SILVER, VDW GmbH). The recommended in-and-out motion was the same as described above for the R40 instrument.
Preparation with Mtwo files (n = 18): Mtwo files were used in sequence and in rotary motion (VDW.SILVER, VDW GmbH). For cervical, middle, and apical preparation, size 25, .07 taper, size 25, .06 taper and size 20, .06 taper instruments, respectively, were used. After this, a sequence of Mtwo files from size 25, .06 taper instrument up to size 40, .06 taper instrument were used. After the use of each instrument, root canal was irrigated.
Root canal irrigation during preparation was performed with 6 mL 2.5% NaOCl (2 mL for each third to Reciproc, 1 mL for each third after both instruments to Unicone and 1 mL for each instrument change to Mtwo rotary system). A 30-G NaviTip needle (NaviTip, Ultradent Products, South Jordan, UT, USA) placed to 1 mm short of working length in a 5-mL syringe (Ultradent Products, South Jordan, UT, USA) was used with a flow rate of 2 mL/min and simultaneous suction by using a 0.014-in tip (Capillary tips, Ultradent, USA). The continuous flow of the irrigant was associated with an in-and-out movement. A final irrigation with 5 mL 2,5% NaOCl followed by 2 mL 17% EDTA was performed in each sample. Root canals were aspirated with a capillary tip and dried with absorbent paper points (Dentsply Sirona), and the specimens submitted to postoperative scanning and reconstruction, applying the aforementioned parameters.
Micro-CT analysis
After reconstruction of the scans before and after root canal preparation by using NRecon software, the datasets were geometrically aligned by using the 3D registration function of the Data Viewer software (Data Viewer v.1.5.1, Bruker microCT). Images were quantitatively analyzed using CTan software (CTAn v.1.14.4, Bruker microCT) and defined parameters of increase in volume, percentage of debris, and percentage of uninstrumented surface were obtained as previously described [7, 23,24,25]. The analysis was performed in the total extension of root canal (from the coronal limit to the apex) and in thirds (cervical, middle, and apical).
Statistical evaluation
Data were compared using one-way ANOVA and Tukey to initial volume; to increase in volume (%) in the cervical, middle, and apical thirds; to debris (%) in the total and apical third; and to uninstrumented surface (%) in the total and middle and apical thirds (α = 5%). Kruskal-Wallis and Dunn tests were used to increase in volume (%) in the total; to debris (%) in the cervical and middle thirds; and to uninstrumented surface (%) in the cervical third (α = 5%).
Results
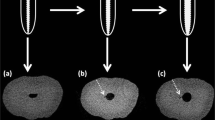
The results obtained showed that there was no difference among the samples evaluated with regard the initial volume, confirming the degree of homogeneity (baseline) of the groups (P > .05). Unicone group was associated with the highest increase in volume values (P < .05), with no difference among groups in the cervical and apical thirds (P > .05), as shown in Table 1. For this system, a higher percentage of debris was also observed in the entire root canal and in the middle third (P < .05). With regard to the percentage of uninstrumented surface, there was no significant difference among the systems in the middle and apical thirds (P > .05). However, a higher percentage of uninstrumented surface in the entire root canal and in the cervical third was observed for Unicone Group when compared with Reciproc group (P < .05) (Table 1). Figure 1 shows representative 3D reconstructions of mandibular incisors before and after canal preparation with the tested systems.

Tridimensional micro-CT scan reconstructions of the external and internal anatomy of oval canals of mandibular incisors, in the Reciproc, Unicone, and Mtwo groups. (A) The root canal before (green) and (B) after (red) preparation. (C) Superimposition of preoperative root canal (A) and post-instrumentation (B). (D) Superimposition of accumulated hard-tissue debris plus instrumented areas (black areas) on the postoperative anatomy (green). (E) Total accumulated hard-tissue debris plus instrumented areas (black areas). (F) Axial view of superimposed root canals before (green) and after (red) preparation at coronal (c), middle (m), and apical (a) thirds
Discussion
The volumetric increase of the root canal, percentage of debris, and uninstrumented surface have been evaluated by means of micro-computed tomography. Oval canal preparation represents a clinical challenge [17, 18], and the use of different instruments [14] or even auxiliary means of cleaning [15, 16] did not promote complete preparation and cleaning of oval canals, corroborating with the present study. The teeth were first selected by means of radiographic analysis, according to other studies [3, 18, 26]. Selected teeth were then analyzed using micro-CT and they were randomly assigned to one of the experimental groups. The initial volume was similar among the experimental groups (Table 1).
In the present study, the higher increase in the root canal volume throughout the extension of the canal and in the middle third was observed for the Unicone reciprocating system, using two instruments. However, in spite of the increase in volumetric values, a higher percentage of untouched areas were also observed for this system. In previous studies, WaveOne, for example, promoted a higher increase in the volume value of the canal, with a similar percentage of uninstrumented surfaces of oval canals to Easy ProDesign Logic and OneShape systems [27]. It was also observed that although the SAF system touched the canal walls to a larger extent, it removed less dentin in the preparation of oval root canals [18]. Corroborating with our results, these data demonstrated that root canal preparation was influenced by diverse factors, such as instrument design, kinematics, and number of instruments. An increase of canal volume indicates greater wear of dentin walls, but does not mean that this occurred following the root canal morphology. The preparation with Unicone promoted greater volume increase than the other systems. However, this wear was probably not higher in flattening areas that presented greater accumulation of debris. Also, the orientation of blades associated with reciprocating motion may have favored less cleaning of the root canal walls.
In spite of standardizing the size (instruments with tip #40) and taper (taper .06), the taper may be influenced the preparation. The Unicone instruments present a constant taper, while Reciproc presents taper .06 in the apical 3 mm and a reduction to 0.04 mm up to the end of the active part. This reduction may have favored the greater action in the middle of the oval canal, which narrows significantly [10, 11], thereby promoting a larger area of instrumented surface and a reduction in the percentage of debris. It means that the reduction of taper for Reciproc probably improves its capacity to reach flattening areas. In the apical region, where the tip and taper were similar among the systems, no difference in the uninstrumented surface value or accumulation of debris was observed.
The apical enlargement of root canal preparation can be associated to apical crack formation [28]. However, larger instruments are significantly more effective in eliminating bacteria [29,30,31]. The root canal enlargement up three sizes larger than the first apical binding file is considered a proper preparation [32]. Mandibular incisors may present unprepared surfaces and debris in the root canal system [10, 11], due to the prevalence of oval canals [12, 33, 34], which make it difficult to obtain efficient cleaning [3, 17, 18]. With basis on these concepts, regarding the root canal morphology, the preparation in the present study was standardized up to file #40, .06 taper.
The highest percentage of uninstrumented surface in the preparation with Unicone and the highest percentage of debris may also be related to its smaller metal mass, as observed after evaluating its preparation capacity [19]. Furthermore, the Unicone instruments presented smaller areas and lengths of flutes than the Reciproc instruments [35]. The smaller metal mass of the Unicone instruments could promote less contact of the instrument with the dentin walls. Areas that remained untouched during preparation may be colonized by biofilm, capable of compromising the endodontic treatment [16, 36].
In relation to cleaning (considered by the percentage of debris), the preparation of oval canals were shown to be cleaner (lower percentage of debris) with the reciprocating R40, and rotary system with the Mtwo sequence of instruments. A lower percentage of debris in the middle third of oval canals prepared with MTwo or R40 instruments was observed when compared with the preparation performed with a single Mtwo 40.06 instrument [7]. Favorable results were also obtained with the use of the Mtwo sequence of instruments, in the analysis of preparation in mandibular molars with two separate mesial canals and severe curvature [37]. The accumulation of debris during root canal preparation usually involves areas as isthmus, irregularities, and ramifications [25]. Oval canals present straightening in the middle region of the root canal [11], making this region critical to cleaning.
This Micro-Ct study presents limitations inherent to an in vitro root canal preparation study [38], as different NiTi systems and evaluated parameters. Also, root canal preparations were performed using an open root canal model. It is difficult to compare the results of this study with other experimental design and methodological studies. While considering these limitations, important considerations could be observed for root canal preparation and cleaning of oval-shaped root canals.
Conclusion
The Unicone system using two instruments in reciprocating motion resulted in higher increase in volume values. However, less remaining debris was present when Reciproc single-file and Mtwo rotary system were used. Root canal preparation and cleaning depend on root canal morphology, kinematics, and instrument design.
References
Peters OA (2009) Current challenges and concepts in the preparation of root canal systems: a review. J Endod 30:559–567
De-Deus G, Barino B, Zamolyi R et al (2010) Suboptimal debridement quality produced by the single-file F2 Protaper technique in oval-shaped canals. J Endod 36:1897–1900. https://doi.org/10.1016/j.joen.2010.08.009
Versiani MA, Leoni GB, Steier L, de-Deus G, Tassani S, Pécora JD, de Sousa-Neto MD (2013) Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file, Reciproc, WaveOne, and ProTaper universal systems. J Endod 39:1060–1066. https://doi.org/10.1016/j.joen.2013.04.009
Farmakis ET, Sotiropoulos GG, Abràmovitz I, Solomonov M (2016) Apical debris extrusion associated with oval shaped canals: a comparative study of WaveOne vs Self-Adjusting File. Clin Oral Investig 20:2131–2138. https://doi.org/10.1007/s00784-016-1709-3
Vandenberghe B, Bud M, Sutanto A, Jacobs R (2010) The use of high-resolution digital imaging technology for small diameter K-file length determination in endodontics. Clin Oral Investig 14:223–231. https://doi.org/10.1007/s00784-009-0285-1
Robinson JP, Lumley PJ, Cooper PR, Grover LM, Walmsley AD (2013) Reciprocating root canal technique induces greater debris accumulation than a continuous rotary technique as assessed by 3-dimensional micro-computed tomography. J Endod 39:1067–1070. https://doi.org/10.1016/j.joen.2013.04.003
Espir CG, Nascimento-Mendes CA, Guerreiro-Tanomaru JM, Freire LG, Gavini G, Tanomaru-Filho M (2017) Counterclockwise or clockwise reciprocating motion for oval root canal preparation: a micro-CT analysis. Int Endod J. https://doi.org/10.1111/iej.12776
Pedullà E, Grande NM, Plotino G, Gambarini G, Rapisarda E (2013) Influence of continuous or reciprocating motion on cyclic fatigue resistance of 4 different nickel-titanium rotary instruments. J Endod 39:258–261. https://doi.org/10.1016/j.joen.2012.10.025
Amoroso-Silva P, Alcalde MP, Duarte MA et al (2016) Effect of finishing instrumentation using niti hand files on volume, surface area and uninstrumented surfaces in C-shaped root canal systems. Int Endod J 50:604–611. https://doi.org/10.1111/iej.12660
Metzger Z, Zary R, Cohen R, Teperovich E, Paqué F (2010) The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a threedimensional micro-computed tomographic study. J Endod 36:1569–1573. https://doi.org/10.1016/j.joen.2010.06.003
Moura-Netto C, Palo RM, Pinto LF, Mello-Moura AC, Daltoé G (2015) Wilhelmsen NS (2015) CT study of the performance of reciprocating and oscillatory motions in flattened root canal areas. Braz Oral Res 29:1–6. https://doi.org/10.1590/1807-3107BOR-2015.vol29.0006
Wu MK, R’Oris A, Barkis D, Wesselink PR (2000) Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 89:739–743. https://doi.org/10.1067/moe.2000.106344
Jou YT, Karabucak B, Levin J, Liu D (2004) Endodontic working width: current concepts and techniques. Dent Clin N Am 48:323–335. https://doi.org/10.1016/j.cden.2003.12.006
Versiani MA, Pécora JD, de Sousa-Neto MD (2011) Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 37:1002–1007. https://doi.org/10.1016/j.joen.2011.03.017
Siqueira JF Jr, Alves FR, Almeida BM, de Oliveira JC, Rôças IN (2010) Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. J Endod 36:1860–1865. https://doi.org/10.1016/j.joen.2010.08.001
Alves FR, Almeida BM, Neves MA, Moreno JO, Rôças IN, Siqueira JF Jr (2011) Disinfecting oval-shaped root canals: effectiveness of different supplementary approaches. J Endod 37:496–501. https://doi.org/10.1016/j.joen.2010.12.008
De-Deus G, Belladonna FG, Silva EJ et al (2015) Micro-CT evaluation of non-instrumented canal areas with different enlargements performed by NiTi systems. Braz Dent J 26:624–629. https://doi.org/10.1590/0103-6440201300116
Zuolo ML, Zaia AA, Belladonna FG, Silva EJNL, Souza EM, Versiani MA, Lopes RT, de-Deus G (2017) Micro-CT assessment of the shaping ability of four root canal instrumentation systems in oval-shaped canals. Int Endod J. https://doi.org/10.1111/iej.12810
Alcalde MP, Tanomaru-Filho M, Bramante CM, Duarte MAH, Guerreiro-Tanomaru JM, Camilo-Pinto J, Só MVR, Vivan RR (2017) Cyclic and torsional fatigue resistance of reciprocating single files manufactured by different nickel-titanium alloys. J Endod 43:1186–1191. https://doi.org/10.1016/j.joen.2017.03.008
Silva EJ, Villarino LS, Vieira VT et al (2016) Bending resistance and cyclic fatigue life of Reciproc, Unicone, and WaveOne reciprocating instruments. J Endod 42:1789–1793. https://doi.org/10.1016/j.joen.2016.08.026
Busquim S, Cunha RS, Freire L, Gavini G, Machado ME, Santos M (2015) A micro-computed tomography evaluation of long-oval canal preparation using reciprocating or rotary systems. Int Endod J 48:1001–1006. https://doi.org/10.1111/iej.12398
Sant’Anna Júnior A, Cavenago BC, Ordinola-Zapata R, de-Deus G, Bramante CM, Duarte MAH (2014) The effect of larger apical preparations in the danger zone of lower molars prepared using the Mtwo and Reciproc systems. J Endod 40:1855–1859. https://doi.org/10.1016/j.joen.2014.06.020
Freire LG, Iglecias EF, Cunha RS, Dos Santos M, Gavini G (2015) Micro-computed tomographic evaluation of hard tissue debris removal after different irrigation methods and its influence on the filling of curved canals. J Endod 41:1660–1666. https://doi.org/10.1016/j.joen.2015.05.001
da Silva Limoeiro AG, Dos Santos AH, De Martin AS et al (2016) Micro-computed tomographic evaluation of 2 nickel-titanium instrument systems in shaping root canals. J Endod 42:496–499. https://doi.org/10.1016/j.joen.2015.12.007
Paqué F, Laib A, Gautschi H, Zehnder M (2009) Hard-tissue debris accumulation analysis by high-resolution computed tomography scans. J Endod 35:1044–1047. https://doi.org/10.1016/j.joen.2009.04.026
Oliveira MA, Alves LD, Pereira AG, Raposo LH, Biffi JC (2015) Influence of flexion angle of files on the decentralization of oval canals during instrumentation. Braz Oral Res. 29:1–6. https://doi.org/10.1590/1807-3107BOR-2015.vol29.0078
Coelho BS, Amaral RO, Leonardi DP et al (2016) Performance of three single instrument systems in the preparation of long oval canals. Braz Dent J 27:217–222. https://doi.org/10.1590/0103-6440201302449
Çapar İD, Uysal B, Ok E, Arslan H (2015) Effect of the size of the apical enlargement with rotary instruments, single-cone filling, post space preparation with drills, fiber post removal, and root canal filling removal on apical crack initiation and propagation. J Endod 41:253–256. https://doi.org/10.1016/j.joen.2014.10.012
Siqueira JF Jr, Lima KC, Magalhães FA, Lopes HP, de Uzeda M (1999) Mechanical reduction of the bacterial population in the root canal by three instrumentation techniques. J Endod 25:332–333. https://doi.org/10.1016/S0099-2399(06)81166-0
Mickel AK, Chogle S, Liddle J, Huffaker K, Jones JJ (2007) The role of apical size determination and enlargement in the reduction of intracanal bacteria. J Endod 33:21–23. https://doi.org/10.1016/j.joen.2006.08.004
Rollison S, Barnett F, Stevens RH (2002) Efficacy of bacterial removal from instrumented root canals in vitro related to instrumentation technique and size. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 94:366–371. https://doi.org/10.1067/moe.2002.126164
Saini HR, Tewari S, Sangwan P, Duhan J, Gupta A (2012) Effect of different apical preparation sizes on outcome of primary endodontic treatment: a randomized controlled trial. J Endod 38:1309–1315. https://doi.org/10.1016/j.joen.2012.06.024
Milanezi de Almeida M, Bernardineli N, Ordinola-Zapata R, Villas-Boas MH, Amoroso-Silva PA, Brandao CG, Guimaraes BM, Moraes IG, Hungaro-Duarte MA (2013) Micro–computed tomography analysis of the root canal anatomy and prevalence of oval canals in mandibular incisors. J Endod 19:1529–1533. https://doi.org/10.1016/j.joen.2013.08.033
Leoni GB, Versiani MA, Pécora JD, Sousa-Neto MD (2014) Micro–computed tomographic analysis of the root canal morphology of mandibular incisors. J Endod 40:710–716. https://doi.org/10.1016/j.joen.2013.09.003
Sampaio FC, Brito AP, Veloso HH, de Alencar AH, Decurcio DA, de Figueiredo JA, Estrela C (2017) Flute and shank dimensions of reciprocating instruments before and after simulated root canal shaping. J Contemp Dent Pract 18:198–204
Dietrich MA, Kirkpatrick TC, Yaccino JM (2012) In vitro canal and isthmus debris removal of the self-adjusting file, K3, and WaveOne files in the mesial root of human mandibular molars. J Endod 38:1140–1144. https://doi.org/10.1016/j.joen.2012.05.007
Pedullà E, Plotino G, Grande NM, Avarotti G, Gambarini G, Rapisarda E, Mannocci F (2016) Shaping ability of two nickel-titanium instruments activated by continuous rotation or adaptive motion: a micro-computed tomography study. Clin Oral Investig 20:2227–2233. https://doi.org/10.1007/s00784-016-1732-4
Hulsmann M, Peters OA, Dummer PMH (2005) Mechanical preparation of root canals: shaping goals, techniques and means. Endod Top 10:30–76
Funding
This study was funded by São Paulo Research Foundation—FAPESP 2015/03437-6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. All applicable international, national, and/or institutional guidelines for the care and use of animals were followed. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study, formal consent is not required. Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Espir, C.G., Nascimento-Mendes, C.A., Guerreiro-Tanomaru, J.M. et al. Shaping ability of rotary or reciprocating systems for oval root canal preparation: a micro-computed tomography study. Clin Oral Invest 22, 3189–3194 (2018). https://doi.org/10.1007/s00784-018-2411-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2411-4