
Abstract
Objectives
To analyze the association between systemic inflammatory burden of cardiovascular disease (CVD) risk and periodontitis in adolescents, including mediating pathways triggered by their common risk factors.
Materials and methods
Using a population-based sample study (n = 405) of Brazilian adolescents (17–18 years old), direct and mediation pathways triggered by “Socioeconomic Status,” “Adiposity,” Smoking, and “Blood Pressure” were modelled for the association between the “Systemic Circulating Inflammatory Burden of CVD Risk” (IL-1β, IL-6, IL-8, TNF-α) and the “Initial Periodontitis” (bleeding on probing (BoP), probing depth (PD) ≥ 4 mm, clinical attachment loss (CAL) ≥ 4 mm), both as continuous latent variables, using structural equation modeling. Sensitivity analysis was performed for the outcomes “Gingivitis” (visible plaque; BoP); “Moderate Periodontitis” (PD ≥ 5 mm and CAL ≥ 5 mm) and periodontitis (CDC-AAP case definition).
Results
Higher “Systemic Circulating Inflammatory Burden of CVD Risk” was directly associated with higher “Initial Periodontitis” (standardized coefficient [SC] = 0.178, P value < 0.001). Lower “Socioeconomic Status” (SC = − 0.022, P value = 0.015) and Smoking (SC = 0.030, P value = 0.021) triggered the “Initial Periodontitis”, mediated by “Systemic Circulating Inflammatory Burden of CVD Risk”. Sensitivity analysis showed a dose-response relationship between “Systemic Circulating Inflammatory Burden of CVD Risk” and “Moderate Periodontitis” (SC = 0.323, P value = 0.021).
Conclusions
“Systemic Circulating Inflammatory Burden of CVD Risk” appeared as an underlying mechanism of early periodontal breakdown in adolescents, also triggered by social vulnerability and smoking.
Clinical relevance
The association between periodontitis and CVD in adulthood seems to establish much earlier in life than had been previously studied, giving impetus to preventive approaches focused on their common risk factors.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Periodontitis has been consistently associated with cardiovascular diseases (CVD) in adults [1]. As periodontitis precedes CVD by decades, the hypothesis that periodontal infections may act as a risk factor for causing CVD seems biologically plausible [2]. As a counterpoint to this claimed causal relationship, interventional studies investigating the effect of periodontal therapy on decreasing CVD risk revealed inconsistent findings [3]. In this context, the common causes approach may explain the association between periodontitis and CVD, as both periodontitis and CVD share common risk factors, which include smoking, obesity, and arterial hypertension [3].
The mechanism underlying the association between periodontitis and CVD observed in adults involves systemic inflammation [3], with smoking and endocrine disorders as the most established risk factors leading to systemic inflammation [4]. An increase in circulating inflammatory mediators induces the production of reactive oxygen species, which results in endothelial dysfunction, contributing to the pathogenesis of CVD [5] and periodontitis [6]. In the implicit theory, common risk factors may trigger systemic inflammation; thus, the systemic inflammatory burden linked to CVD risk can reflect vascular damage in oral tissues, which can be observed by an early periodontal breakdown in adolescents. Bearing that in mind, one may hypothesize that the burden of systemic inflammatory linked to CVD risk is underlying early clinical signs of periodontal breakdown among adolescents, which is presumed to reflect a continuum, considering pathways triggered by their common risk factors. Nevertheless, most studies exploring this hypothesis have employed conventional regression approaches to deal with mediation and multidimensional variables, including periodontitis and systemic inflammatory burden, which might have led to methodological issues, as collider bias, and over adjustment.
In such a context, structural equation modeling (SEM) emerges as an alternative to investigate complex causal relationships between several variables taking into account mediation. Moreover, SEM allows modeling multidimensional (latent and factor) variables in such a complex scenario, reducing the magnitude of the measurement error [7]. Such an SEM property is of particular relevance to our study, owing to the characteristics of our variables of interest, that, once established, display chronic characteristics throughout the life course and maintain the individual at constant risk [3, 8]. This approach is of the utmost relevance among adolescents [9], as these individuals are amidst the continuum of most non-communicable diseases [10], including periodontitis and CVD [11], and may experience a higher risk of progression over the life course. Thus, it seems reasonable that preventive approaches take place at this stage of their lives.
Accordingly, this study aimed to investigate the association between the systemic inflammatory burden linked to CVD and periodontitis among adolescents, analyzing mediating pathways triggered by common risk factors via systemic inflammatory burden to periodontitis.
Methods
Study design
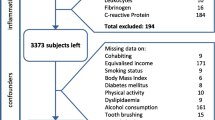
A cross-sectional observational study of a population-based sample was conducted in São Luís, Brazil, between January 2014 and July 2016. A three-stage complex random sampling was used to obtain a representative sample of 17–18-year-old students enrolled in public high schools in that city (n = 405) [12]. In the first stage, all public high schools in the urban zone (n = 52) were randomized for sample selection (n = 13 schools). In the second stage, we isolated three class levels of students (10th, 11th, and 12th grades from the selected schools (n = 39 classes). In the third stage, all 17–18-year-old students in these classes (n = 2,030) were considered eligible for enrollment to this study, and randomization was performed, yielding 638 students. Subjects who used orthodontic appliances (n = 52) and adolescents who were pregnant (n = 3) were excluded. No adolescent had diabetes (fasting glycemia > 110 mg/dl) or reported cardiovascular disease or even used medications to control such diseases. It was estimated that a sample of 400 adolescents would provide a power of 80% to detect significant prevalence ratios for the outcomes of interest to achieve a minimum effect size of 0.3 with a level of significance of 0.05 and assuming 30% refusals and losses (EpiInfo software version 6.0). The final sample consisted of 405 adolescents (Fig. 1).

Flowchart showing sample selection of adolescents enrolled in public high schools in São Luís, Brazil (2014 to 2016)
The Federal University of Maranhão Ethics Committee (CAAE 12498713.8.0000.5087, process number 441.226) approved the study, and written informed consent was obtained from all subjects and their legal representatives. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013, and conformed to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Data collection
A structured questionnaire was applied for the collection of sociodemographic and smoking data of adolescents. Smoking was recorded if participants had smoked at least one cigarette in the last 30 days preceding the interview.
Height and weight were collected using standardized techniques according to a previous protocol [12] and were used to calculate the body mass index (BMI kg/m2). The waist circumference was measured, and the waist-to-height ratio (cm2) was calculated [13]. Total body fat was obtained by electrical bioimpedance (Biodynamics M450®, EUA) [14].
Blood samples were collected from the participants after 10–12-h fasting. Serum samples were stored in a freezer at – 80 °C for analysis of serum levels of inflammatory markers: interleukin (IL)-1β (pg/mL), IL-6 (pg/mL), IL-8 (pg/mL), ultrasensitive C-reactive protein (us-CRP, ng/mL), and TNF-α (tumor necrosis factor alpha, pg/mL). Analyses were carried out with the MILLIPLEX MAP Human Cytokine Kit (HADK2MAG-61K and HCVD3MAG-67K, Millipore, Sigma) using Luminex™ technology (EMD Millipore Corporation, Germany).
Blood pressure measurement was obtained in duplicate at resting seated position, with an interval of 5 min between measurements (Microlife digital monitor, MedLevensohn/Lot: 121400001, Ministry of Health Registration: 10222460055) before the blood samples were drawn.
Three periodontal clinical parameters, including bleeding on probing (BoP), clinical attachment level (CAL), and probing depth (PD) [15], were examined on six sites of all teeth, excluding third molars, using a Williams periodontal probe (Hu-Friedy, Chicago, IL, USA), by two calibrated dentists. The interexaminer reliability kappa of 0.79 for PD and 0.85 for BoP was obtained in a previous pilot study performed on 17–18-year-old subjects (n = 20) [12]. Full-mouth plaque index (FMPI) [16] was estimated by examining four surfaces of all teeth, excluding third molars, by the same calibrated dentists.
Latent variables
Latent variables are constructs (unobserved variables) presumed to reflect a continuum of a multiple dimension phenomenon estimated by the intercorrelation of observed variables (effect indicators). In other words, the effect indicators are intercorrelated because they share a common variance. The variance not explained by the factor that the corresponding indicators are supposed to measure is estimated by a residual term, resulting in an effect estimation free of measurement errors and greater power to detect differences [7, 17]. Variables presumed to measure the same construct show convergent validity if their intercorrelations are appreciable in magnitude (factor loading > 0.4), further decreasing systematic measurement error [7] . For this study, we used the following as latent variables: “Socioeconomic Status”, “Adiposity”, “Blood Pressure”, “Systemic Circulating Inflammatory Burden of CVD Risk”, and “Initial Periodontitis”.
Socioeconomic status
The latent variable “Socioeconomic Status” was validated in a previous study [12] and based on the categorical variables: (a) household income in minimal monthly wage (minimum monthly salary equal to $ 389.38 — in August 2014); (b) maternal education level (years of schooling); and (c) family economic class according to Brazilian Economic Classification Criteria [18], ranging from E (lowest economic class) to A (highest economic class).
Adiposity
“Adiposity” was a latent variable deduced from the correlation among (a) BMI (kg/m2), (b) total body fat (kg), and (c) waist-to-height ratio, all as continuous variables.
Systemic circulating inflammatory burden of CVD risk
This latent variable was deduced from the intercorrelation of the observed variables IL-8, IL-6, IL-1β, and TNF-α levels, which in turns means that these indicators share a common variance that is explained by the construct “Systemic Circulating Inflammatory Burden of CVD Risk”. All indicators were continuous variables since no defined cutoff values exist for these serum inflammatory markers [19].
Initially, us-CRP was tested as one of the indicators of the latent, but it was excluded due to its low factor loading in the confirmatory factor analysis (data not shown). Thus, us-CRP was analyzed separately as an observed variable in the structural model. However, we assumed its correlation with the “Systemic Circulating Inflammatory Burden of CVD Risk”.
Blood pressure
“Blood Pressure” was a latent variable inferred from the correlation between diastolic blood pressure (mmHg) and systolic blood pressure (mmHg), both as continuous variables.
Initial periodontitis
We carried out an exploratory factor analysis (EFA) for periodontitis based on the percent of surfaces with visible plaque (FMPI), the number of teeth with BoP, the number of teeth affected by PD ≥ 3 mm, the number of teeth affected by PD ≥ 4 mm, the number of teeth affected by PD ≥ 5 mm, the number of teeth affected by CAL ≥ 3 mm, the number of teeth affected by CAL ≥ 4 mm, and the number of teeth affected by CAL ≥ 5 mm (Supplementary Table 2). We observed three factors: one factor included FMPI and BoP and was dubbed “Gingivitis” after confirmatory factor analysis (CFA) (Supplementary Table 3). The second periodontal factor included BoP, the number of teeth affected by PD ≥ 3 mm, the number of teeth affected by PD ≥ 4 mm, the number of teeth affected by CAL ≥ 3 mm, and the number of teeth affected by CAL ≥ 4 mm, dubbed “Initial Periodontitis”. In order to increase specificity, the specific thresholds of ≥ 4 mm were considered for PD and CAL in confirmatory factor analysis. Thus, the latent variable “Initial Periodontitis” was generated on the basis of three variables identified in the EFA (BoP, the number of teeth affected by PD ≥ 4 mm, and the number of teeth affected by CAL ≥ 4 mm) and showed satisfactory fit (Table 2). The third factor was indicated by EFA on the basis of two observed variables: the number of teeth affected by PD ≥ 5 mm and the number of teeth affected by CAL ≥ 5 mm. However, the model could not be specified for these two variables due to the under identification of the confirmatory and structural models. To account for satisfactory fit, buccal and interproximal sites were included separately in CFA, which resulted in a latent variable dubbed “Moderate Periodontitis” based on four observed variables: the number of teeth affected by PD ≥ 5 mm in interproximal sites, the number of teeth affected by PD ≥ 5 mm in buccal sites, the number of teeth affected by CAL ≥ 5 mm in interproximal sites, and the number of teeth affected by CAL ≥ 5 mm in buccal sites (Supplementary Table 4).
Theoretical model
The proposed theoretical model was built to analyze the association between the “Systemic Circulating Inflammatory Burden of CVD Risk” and the “Initial Periodontitis”. “Socioeconomic Status”, “Adiposity”, Smoking, and “Blood Pressure” were assumed as common risk factors. Sex was also considered in model adjustment (Fig. 2). Sensitivity analysis was also carried out for the association between the “Systemic Circulating Inflammatory Burden of CVD Risk” and the outcomes: (1) “Moderate Periodontitis”; (2) periodontitis according to the Center for Disease Control and Prevention (CDC) and the American Academy of Periodontology (AAP) case definition [20]; (3) “Gingivitis”.

Theoretical model proposed for the association among common risk factors, the “Systemic Circulating Inflammatory Burden of Cardiovascular Disease Risk” and the “Initial Periodontitis” in adolescents (n = 405), São Luís, Brazil (2014 to 2016). Latent variable drawn as an ellipse. Observed variable drawn as a rectangular box. Only main direct and mediating pathways are shown in the figure for the ease of the interpretation. aBody mass index. bWaist-to-height ratio. cUltrasensitive C-reactive protein. dInterleukin 1β. eInterleukin 8. fTumor necrosis factor alpha. gInterleukin 6
Statistical analysis
SEM was used to analyze the association between the “Systemic Circulating Inflammatory Burden of CVD Risk” and the “Initial Periodontitis”, evaluating direct pathways and indirect (mediated) pathways triggered by their common risk factors, such as “Socioeconomic Status”, “Adiposity”, Smoking, and “Blood Pressure”. This epidemiological tool enables the use of latent variables and estimation of multiple regression equations simultaneously, which is useful for multiple-variable analyses associated with complex phenomena, thus minimizing bias originated from measurement errors [7].
The latent variables “Socioeconomic Status”, “Adiposity”, “Blood Pressure”, “Systemic Circulating Inflammatory Burden of CVD Risk”, and “Initial Periodontitis” were constructed using exploratory factor analysis to extract factors that are effect indicators of the latent variables (data not shown). Next, all latent variables were submitted to a confirmatory factor analysis, and a factor loading > 0.40 was adopted as the minimum value to consider the indicator reflected the latent variable [21].
In the SEM, weighted least squares means and variance adjusted (WLSMV) estimation and theta parameterization were used for control of residual variances [21]. The goodness of fit of the model was evaluated by (a) P value > 0.05 and upper limit of the 90% confidence interval < 0.08 for root mean square error of approximation (RMSEA) and (b) comparative fit index (CFI) and Tucker-Lewis index (TLI) > 0.90 [7].
Direct and indirect pathways between the explanatory variables (observed or latent variables) and the multiple outcomes of interest, including the main outcome, “Initial Periodontitis,” were estimated considering the effect to be significant when P value < 0.05. Full estimation maximum likelihood was used to impute missing data assuming data are missing at random [7]. All analyses were performed with Mplus® 7.0 software [21].
Results
The study included 405 adolescents aged 17–18 years (180 male and 225 female). All participants provided complete data and were included in the analysis. We observed 40.2% (n = 163) of the sample whose mother completed 9 to 11 years of formal education, 47.4% (n = 192) whose household income was 1 to <3 times the monthly minimum wage, and 64.4% (n =261) who were classified as class C. Only 11.8% (n = 48) of the participants had smoked in the last 30 days preceding the interview (Table 1). Clinical periodontal data are presented for the whole sample (Table 1) and non-periodontitis and the entire periodontitis group (mild and moderate periodontitis) according to the CDC-AAP case definition [20] (Supplementary Table 1). Mild and moderate periodontitis case accounted for 33% of the sample (n = 134). No severe periodontitis case was observed.
The latent variables “Socioeconomic Status”, “Adiposity”, “Blood Pressure”, and “Initial Periodontitis” had factor loading > 0.4 and P value < 0.001 indicating convergent validity, which shows good validity of these constructs [21]. The latent variable “Systemic Circulating Inflammatory Burden of CVD Risk” showed good convergent validity for all indicators (factor loading ≥ 0.4; P value < 0.001), except for TNFα (factor loading = 0.320; P value < 0.001). However, as a fact of biological plausibility, we decided to keep this variable in the latent [22] (Table 2).
The significant effects for the association between the “Systemic Circulating Inflammatory Burden of CVD Risk” and the “Initial Periodontitis” are shown in Table 3. A higher “Systemic Circulating Inflammatory Burden of CVD Risk” was associated with higher values of the “Initial Periodontitis” (P value < 0.001). A higher “Socioeconomic Status” reduced the “Initial Periodontitis”, mediated by the reduced “Systemic Circulating Inflammatory Burden of CVD Risk” (P value = 0.015). Smoking increased the “Initial Periodontitis”, mediated by the increased “Systemic Circulating Inflammatory Burden of CVD Risk” (P value = 0.021). “Adiposity” and “Blood Pressure” had no effect on the “Initial Periodontitis” (P value > 0.05). Sensitivity analysis showed a consistent association between “Systemic Circulating Inflammatory Burden of CVD Risk” and the “Moderate Periodontitis”. However, no significant effects were observed when the outcome was either the CDC-AAP periodontitis definition or “Gingivitis” (Supplementary Table 5).
As secondary findings, we observed that higher “Socioeconomic Status” increased the “Adiposity” values (SC = 0.191; SE = 0.071, P value = 0.008) and decreased the “Systemic Circulating Inflammatory Burden of CVD Risk” (SC = − 0.122; SE = 0.056, P value = 0.029); “Adiposity” increased the “Blood Pressure” (SC = 0.587, SE = 0.089, P value < 0.001) and increased the us-CRP (SC = 0.280, SE = 0.062, P value < 0.001). Smoking increased the “Systemic Circulating Inflammatory Burden of CVD Risk” (SC = 0.169, SE = 0.069, P value = 0.014) and us-CRP (SC = 0.332, SE = 0.093, P value < 0.001). Girls had higher values of “Adiposity” (SC = 0.506, SE = 0.038, P value < 0.001) and lower values of “Blood Pressure” (SC = − 0.797, SE = 0.093, P value < 0.001) (data not shown in table).
All proposed model had excellent fit (Supplementary Table 6).
Discussion
Our findings revealed that higher levels of “Systemic Circulating Inflammatory Burden of CVD Risk” were associated with “Initial Periodontitis”. As mediating pathways, a higher “Socioeconomic Status” was associated with lower “Initial Periodontitis” by reducing the Circulating Inflammatory Burden of CVD Risk, while Smoking was associated with increased “Initial Periodontitis” by increasing the Circulating Inflammatory Burden of CVD Risk. “Adiposity” and “Blood Pressure” did not affect the “Initial Periodontitis”. Together, these findings confirm our hypothesis that systemic inflammatory burden is associated with early clinical signs of periodontal breakdown already in adolescents. Besides, social vulnerability and smoking were shown as common causes to trigger this pathway, irrespective of “Adiposity” and “Blood Pressure” in this young population.
Prior to the discussion of our findings, one should carefully examine the limitations and strengths of this study. The main limitation of our study relied on its cross-sectional design, which precluded the establishment of a causal relationship between the “Systemic Circulating Inflammatory Burden of CVD Risk” and “Initial Periodontitis”, as both were collected at the same visit. However, our original plan was to identify incipient periodontal parameters reflecting initial signs of periodontal breakdown and its association with indicators of systemic inflammation, a goal achieved with the current study design. Moreover, determining temporality between these conditions would have remained challenging even with a longitudinal study design, as one might not rule out a potential bidirectional relationship between periodontal and systemic conditions [23], although the reverse causality in which periodontitis can lead to increased levels of systemic inflammatory mediators may be unlikely because our sample is characterized by young individuals with periodontal an incipient destruction.
Among the strengths, our methodological approach should be highlighted. The use of SEM allows to study outcomes that are not a result of one or two variables but are complex conditions resulting from the effect of a set of variables. As in this study, periodontitis was the target outcome, and we investigated direct and indirect paths connecting sociodemographic, behavioral, and systemic conditions to periodontitis. Additionally, this approach supported the use of latent variables, i.e., constructs deduced from a shared variance of a set of indicators, which reduces measurement error of phenomena that are difficult to measure by a single indicator, especially among adolescents [7, 9]. Such a concept suits well our idea of a “Initial Periodontitis”, as periodontal disease is believed to entail ongoing inflammatory changes, measured by probing depth and bleeding on probing, culminating in periodontal breakdown expressed by clinical attachment loss [24]. Thus, it is not possible to identify the moment when gingivitis progresses to periodontitis since both periodontal diseases are a continuum of the same chronic inflammatory disease [25]. Furthermore, as no single parameter can be used alone to define the periodontitis, this condition ought to be better understood as a multidimensional condition, so ought the systemic inflammatory burden that may regulate the CVD-periodontitis association. Whenever one seeks to quantify multidimensional variables, as periodontitis, challenges regarding the operationalization of these variables are faced. The use of categorical unidimensional variables to quantify this condition may deselect important potential features prior to the analysis, as the case definition of periodontitis may be based on arbitrary cutoff values [17]. It would also apply for CVD risk, justifying, then, our claim for a “continuum” CVD and periodontitis risk. Corroborating this assumption, sensitivity analysis showed no significant effects between “Systemic Circulating Inflammatory Burden of CVD Risk” and the outcome periodontitis classified according to the CDC-AAP case definition. We believe that the use of categorical unidimensional variable does not properly measure all aspects related to the extent and severity of periodontal disease, as well as it is not possible to estimate an effect free of measurements errors. Previous study evidenced no significant association when metabolic syndrome and periodontitis were set as observed variables in the structural equation models, irrespective of the criteria used for periodontitis classification [17]. To overcome this methodological issue, periodontitis has been previously addressed as a latent variable [17], even in adolescents [26], reinforcing the advantages of using multidimensional latent variables, which results in more realistic quality analysis for estimating the association between systemic inflammation and periodontal disease.
In terms of periodontal health, this study sample comprises adolescents that experience a mild periodontal breakdown. Instead of a periodontitis case definition, we estimated as a primary outcome a latent variable, dubbed “Initial Periodontitis”, by the shared variance of periodontal disease indicators, which reflected a clinical condition of bleeding on probing, shallow pocket depth, and mild attachment loss. We cannot rule out the possibility that the “Initial Periodontitis” may not reflect an established periodontitis case in these adolescents; however, the systemic inflammatory burden was already linked to this incipient periodontal breakdown, indicating a potential impact on the pathogenesis of periodontal disease, which could, in turn, drive the shift to chronic tissue destruction [24, 27]. A previous study showed that uncontrolled systemic inflammation expressed by higher levels of white blood cell counts were associated with an increased number of sites with periodontal pocket, clinical attachment loss, and periodontitis progression after an 11-year follow-up in adults [28]. The impact of systemic inflammation on the periodontal pathogenesis may be more evident when observing the effect of the “Systemic Circulating Inflammatory Burden of CVD Risk” on the “Moderate Periodontitis”, a latent variable that reflects a chronic periodontal breakdown explicitly. The greater coefficient found on the association between systemic inflammation and an established periodontitis, “Moderate Periodontitis”, reveals a clear dose-response relationship, reinforces the robustness of our findings, and sheds light on the current understanding of the CVD-periodontitis relationship. Thus, the clinical evidence of periodontal disease in this study could be taken as both an early clinical sign of periodontal breakdown and a predictor of progressive clinical attachment loss [29], representing a risk phenotype indeed.
We showed that Smoking in adolescence was associated with increased systemic inflammation by increasing both the “Systemic Circulating Inflammatory Burden of CVD Risk” and the us-CRP levels; and that the association between Smoking and the “Initial Periodontitis” was mediated by higher values of the “Systemic Circulating Inflammatory Burden of CVD Risk”. As an explanation, it is plausible that smoking precedes systemic inflammatory burden [4], which plays an essential role in the development of chronic inflammatory diseases such as periodontitis [24] and cardiovascular disease [3]. Smoking activates the NF-κβ pathway, which induces transcription of genes involved in immune regulation [30] and may result in a systemic inflammatory response expressed by a higher number of circulating leukocytes [30, 31], lymphocytes [31], and release of proinflammatory mediators such as TNF-α [31], IL-1β [32], IL-6 [33], IL-8 [31], and CRP [33], even with low dose of exposure [33]. In addition, despite the vast evidence about the impact of smoking on the risk of onset and progression of periodontitis [34], our study adds to the existing knowledge as it demonstrates that the systemic commitment of smoking underlies this relationship already in adolescence.
Increased levels of proinflammatory cytokines, primarily TNF-α, an early inflammatory marker, causes uncontrolled reactive oxygen species production and contributes to endothelial cell damage, resulting in endothelial dysfunction [35]. Vascular dysfunction, known to be induced by a range of risk factors such as inflammation and smoking, may influence the pathogenesis of periodontitis and the long-term process of atherogenesis [36]. In this context, periodontitis and atherosclerosis may share a pathogenic background expressed by systemic inflammation [3], oxidative stress [36], and vascular dysfunction [37], which can be reflected by vascular damage in oral tissues, as observed in our study with adolescents presenting periodontal breakdown already associated with systemic inflammatory burden of CVD risk. Accordingly, we observed no significant association between “Systemic Circulating Inflammatory Burden of CVD Risk” and the outcome “Gingivitis”, a local inflammatory response that results from plaque accumulation due to neglected oral hygiene and tooth-related factors.
Our findings also revealed that higher “Adiposity” was not associated with the “Initial Periodontitis” values, despite the evidence that obesity is associated with periodontitis in adolescents and young adults [38]. This lack of association between “Adiposity” and periodontitis might have been influenced by the low prevalence of obesity among adolescents in this population-based study. Another factor could be related to the method used to determine obesity, which considered BMI, an extensively used measure of obesity [39], but also total fat mass and waist-to-height ratio, which is usually recommended as a measure of central obesity [13]. However, “Adiposity” was associated with higher levels of us-CRP, indicating that the adipose tissue is involved in the regulation of systemic inflammatory markers [24, 40].
The higher “Socioeconomic Status” was associated with a lower “Initial Periodontitis”, as it reduced the “Systemic Circulating Inflammatory Burden of CVD Risk”, which confirms previous studies showing an association between social vulnerability and systemic inflammation [41] and periodontal disease [42]. Our findings increase the existing knowledge of this field by showing that systemic inflammation could play a role as a mediator of this relationship in the early stages of life.
There is enormous evidence that chronically increased levels of inflammatory biomarkers can predict CVD [22]. In our study, systemic inflammatory burden was triggered by “Socioeconomic Status”, Obesity and Smoking and associated with the “Initial Periodontitis,” which can expose the individual to continuous risk for both periodontal disease progression [28] and CVD [22]. Any approach to reduce disease burden in adulthood should be focused on intercepting disease at early stages, such as controlling early clinical signs of periodontal breakdown and modifiable risk factors such as smoking [25, 43]. This approach improves the cost-effectiveness of the treatment, thus facilitating the inclusion of dental care as part of the health coverage in populations with low socioeconomic status [43].
Conclusion
To our knowledge, this was the first population-based study showing that serum levels of inflammatory markers are associated with early clinical signs of periodontal breakdown in adolescents through mediating pathways triggered by social vulnerability and smoking, placing the individual at sustained risk of CVD and progression of periodontal breakdown. These results may explain the association between periodontitis and CVD in the future and give impetus to an early intervention approach focused on common risk factors.
References
Blaizot A, Vergnes J, Nuwwareh S et al (2009) Periodontal diseases and cardiovascular events: meta-analysis of observational studies. Int Dent J 59:197–209. https://doi.org/10.1922/IDJ_2114SIXOU13
Janket SJ, Baird AE, Chuang SK, Jones JA (2003) Meta-analysis of periodontal disease and risk of coronary heart disease and stroke. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 95:559–569. https://doi.org/10.1067/moe.2003.107
Lockhart PB, Bolger AF, Papapanou PN et al (2012) Periodontal disease and atherosclerotic vascular disease: does the evidence support an independent association?: a scientific statement from the American heart association. Circulation 125:2520–2544. https://doi.org/10.1161/CIR.0b013e31825719f3
Menezes AMB, Oliveira PD, Wehrmeister FC et al (2019) Association of modifiable risk factors and IL-6, CRP, and adiponectin: findings from the 1993 birth cohort, Southern Brazil. PLoS One 14:1–18. https://doi.org/10.1371/journal.pone.0216202
Zhang H, Park Y, Wu J et al (2009) Role of TNF-α in vascular dysfunction. Clin Sci 116:219–230. https://doi.org/10.1042/CS20080196
Chapple ILC, Matthews JB (2007) The role of reactive oxygen and antioxidant species in periodontal tissue destruction. Periodontol 43:160–232. https://doi.org/10.1111/j.1600-0757.2006.00178.x
Kline RB (2011) Principles and practice of structural equation modeling. Guilford Press, New York
Sawyer SM, Afifi RA, Bearinger LH et al (2012) Adolescence: a foundation for future health. Lancet 379:1630–1640. https://doi.org/10.1016/S0140-6736(12)60072-5
Botero JE, Rösing CK, Duque A et al (2015) Periodontal disease in children and adolescents of Latin America. Periodontol 2000(67):34–57. https://doi.org/10.1111/prd.12072
GBD 2016 Risk Factors Collaborators, Gakidou E, Afshin A et al (2017) Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet 390:1345–1422. https://doi.org/10.1016/S0140-6736(17)32366-8
Dzau VJ, Antman EM, Black HR et al (2006) The cardiovascular disease continuum validated: clinical evidence of improved patient outcomes: part I: pathophysiology and clinical trial evidence (risk factors through stable coronary artery disease). Circulation 114:2850–2870. https://doi.org/10.1161/CIRCULATIONAHA.106.655688
Carmo CDS, Ribeiro MRC, Teixeira JXP et al (2018) Added sugar consumption and chronic oral disease burden among adolescents in Brazil. J Dent Res 97:508–514. https://doi.org/10.1177/0022034517745326
Lo K, Wong M, Khalechelvam P, Tam W (2016) Waist-to-height ratio, body mass index and waist circumference for screening paediatric cardio-metabolic risk factors: a meta-analysis. Obes Rev 17:1258–1275. https://doi.org/10.1111/obr.12456
Ellis KJ, Bell SJ, Chertow GM et al (1999) Bioelectrical impedance methods in clinical research: a follow-up to the NIH technology assessment conference. Nutrition 15:874–880. https://doi.org/10.1016/S0899-9007(99)00147-1
American Academy of Periodontology (2001) Glossary of periodontal terms. https://members.perio.org/libraries/glossary?_ga=2.171418080.19602079.1549170589-926308261.1548130467&ssopc=1. Accessed 1 Jun 2020
Ainamo J, Bay I (1975) Problems and proposals for recording gingivitis and plaque. Int Dent J 25:229–235
Nascimento GG, Leite FRM, Peres KG et al (2019) Metabolic syndrome and periodontitis: a structural equation modeling approach. J Periodontol 90:655–662. https://doi.org/10.1002/JPER.18-0483
ABEP AB de E de P (2012) Critério de Classificação Econômica Brasil. http://www.abep.org/criterio-brasil. Accessed 29 Sep 2015
Monastero RN, Pentyala S (2017) Cytokines as biomarkers and their respective clinical cutoff levels. Int J Inflam 2017:4309485. https://doi.org/10.1155/2017/4309485
Eke PI, Page RC, Wei L et al (2012) Update of the case definitions for population-based surveillance of periodontitis. J Periodontol 83:1449–1454. https://doi.org/10.1902/jop.2012.110664
Muthén B, Muthén BO (2009) Statistical analysis with latent variables. Wiley, New York
Libby P, Crea F (2010) Clinical implications of inflammation for cardiovascular primary prevention. Eur Heart J 31:777–783. https://doi.org/10.1093/eurheartj/ehq022
Carrizales-Sepúlveda EF, Ordaz-Farías A, Vera-Pineda R, Flores-Ramírez R (2018) Periodontal disease, systemic inflammation and the risk of cardiovascular disease. Heart Lung Circ 27:1327–1334. https://doi.org/10.1016/j.hlc.2018.05.102
Genco RJ, Genco FD (2014) Common risk factors in the management of periodontal and associated systemic diseases: The dental setting and interprofessional collaboration. J Evid Based Dent Pract 14:4–16. https://doi.org/10.1016/j.jebdp.2014.03.003
Jepsen S, Blanco J, Buchalla W et al (2017) Prevention and control of dental caries and periodontal diseases at individual and population level: consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J Clin Periodontol 44(Suppl 1):S85–S93. https://doi.org/10.1111/jcpe.12687
Nascimento GG, Baelum V, Dahlen G, Lopez R (2018) Methodological issues in assessing the association between periodontitis and caries among adolescents. Community Dent Oral Epidemiol 46:303–309. https://doi.org/10.1111/cdoe.12367
Nyvad B, Takahashi N (2020) Integrated hypothesis of dental caries and periodontal diseases. J Oral Microbiol 12:1710953. https://doi.org/10.1080/20002297.2019.1710953
Pink C, Kocher T, Meisel P et al (2015) Longitudinal effects of systemic inflammation markers on periodontitis. J Clin Periodontol 42:988–997. https://doi.org/10.1111/jcpe.12473
Tanner ACR, Kent R, Kanasi E et al (2007) Clinical characteristics and microbiota of progressing slight chronic periodontitis in adults. J Clin Periodontol 34:917–930. https://doi.org/10.1111/j.1600-051X.2007.01126.x
Gonçalves RB, Coletta RD, Silvério KG et al (2011) Impact of smoking on inflammation: overview of molecular mechanisms. Inflamm Res 60:409–424. https://doi.org/10.1007/s00011-011-0308-7
Andreoli C, Bassi A, Gregg EO et al (2015) Effects of cigarette smoking on circulating leukocytes and plasma cytokines in monozygotic twins. Clin Chem Lab Med 53:57–64. https://doi.org/10.1515/cclm-2013-0290
Barbieri SS, Zacchi E, Amadio P et al (2011) Cytokines present in smokers serum interact with smoke components to enhance endothelial dysfunction. Cardiovasc Res 90:475–483. https://doi.org/10.1093/cvr/cvr032
Al Rifai M, DeFilippis AP, McEvoy JW et al (2017) The relationship between smoking intensity and subclinical cardiovascular injury: the multi-ethnic study of atherosclerosis (MESA). Atherosclerosis 258:119–130. https://doi.org/10.1016/j.atherosclerosis.2017.01.021
Leite FRM, Nascimento GG, Baake S et al (2019) Impact of smoking cessation on periodontitis: a systematic review and meta-analysis of prospective longitudinal observational and interventional studies. Nicotine Tob Res 21:1600–1608. https://doi.org/10.1093/ntr/nty147
Chen X, Andresen B, Hill M et al (2008) Role of reactive oxygen species in tumor necrosis factor-alpha induced endothelial dysfunction. Curr Hypertens Rev 4:245–255. https://doi.org/10.2174/157340208786241336
Bullon P, Newman HN, Battino M (2014) Obesity, diabetes mellitus, atherosclerosis and chronic periodontitis: a shared pathology via oxidative stress and mitochondrial dysfunction? Periodontol 64:139–153. https://doi.org/10.1111/j.1600-0757.2012.00455.x
Mendes RT, Fernandes D (2016) Endothelial dysfunction and periodontitis: the role of inflammatory serum biomarkers. Dent Hypotheses 7:4–11. https://doi.org/10.4103/2155-8213.177401
Khan S, Barrington G, Bettiol S et al (2018) Is overweight/obesity a risk factor for periodontitis in young adults and adolescents?: a systematic review. Obes Rev 19:852–883. https://doi.org/10.1111/obr.12668
Ayvaz G, Çimen AR (2011) Methods for body composition analysis in adults. Open Obes J 3:62–69. https://doi.org/10.2174/1876823701103010062
Genco RJ, Grossi SG, Ho A et al (2005) A proposed model linking inflammation to obesity, diabetes, and periodontal infections. J Periodontol 76:2075–2084. https://doi.org/10.1902/jop.2005.76.11-S.2075
Hostinar CE, Ross KM, Chen E, Miller GE (2015) Modeling the association between lifecourse socioeconomic disadvantage and systemic inflammation in healthy adults: The role of self-control. Health Psychol 34:580–590. https://doi.org/10.1037/hea0000130
Schuch HS, Peres KG, Singh A et al (2017) Socioeconomic position during life and periodontitis in adulthood: a systematic review. Community Dent Oral Epidemiol 45:201–208. https://doi.org/10.1111/cdoe.12278
GBD 2017 Oral Disorders Collaborators, Bernabe E, Marcenes W et al (2020) Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: a systematic analysis for the global burden of disease 2017 study. J Dent Res 99:362–373. https://doi.org/10.1177/0022034520908533
Funding
This study was funded by FAPEMA (Maranhão State Foundation for Research and Scientific and Technological Development), CNPq (National Council for Scientific and Technological Development), CAPES (Coordination for the Improvement of Higher Education Personnel)Finance Code 001, and PPSUS (Research Program for the Unified Health System/SUS – Ministry of Health).
Author information
Authors and Affiliations
Contributions
C.C.C. Ribeiro, C.D.S. Carmo and A.R.O. Moreira contributed to conception, design, data acquisition, analysis and interpretation, drafted and critically revised the manuscript; C.M.C. Alves contributed to conception, design, data acquisition and interpretation, drafted and critically revised the manuscript; B.B. Benatti contributed to conception, data acquisition, drafted and critically revised the manuscript; R.V.C. Casarin and G.G. Nascimento contributed to conception and data interpretation, critically revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of the Federal University of Maranhão (CAAE 12498713.8.0000.5087, process number 441.226) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Conflict of interest
The authors declare no competing of interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(PDF 172 kb).
Rights and permissions
About this article

Cite this article
Ribeiro, C.C.C., Carmo, C.D.S., Benatti, B.B. et al. Systemic circulating inflammatory burden and periodontitis in adolescents. Clin Oral Invest 25, 5855–5865 (2021). https://doi.org/10.1007/s00784-021-03891-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-021-03891-y