
Abstract
Objectives
This study aimed to systematically review the literature regarding the risk of selective removal—in comparison with stepwise and nonselective removal—of carious tissue in permanent teeth.
Materials and methods
Controlled clinical trials and cohort studies involving patients with dental caries in permanent teeth were included. Databases used were PubMed, Embase, and Scopus. The test group should be composed of patients undergoing selective removal of carious tissues, and the control group should comprise patients undergoing nonselective removal and/or stepwise removal of carious tissue. Laboratory tests, studies on primary teeth, and studies that used temporary restorations were excluded, as were literature reviews. The primary outcome was overall success of maintaining pulpal health (both clinically and radiographically). Quality of the restoration, pulp exposure, dentin deposition, and microbiological examination were also assessed. A meta-analysis, using the pooled risk ratio (RR) and its 95% confidence interval (CI), was performed to assess the success of maintaining pulpal health, using the different control treatments as a subgroup analysis.
Results
A total of 2333 articles were retrieved, of which 10 were included in the systematic review and four in the meta-analysis. In the qualitative evaluation, the control groups presented a higher risk of pulp exposure in relation to the selective removal. In the meta-analysis, the selective carious tissue removal showed significantly higher overall success (RR, 95% CI 1.11, 1.02–1.21).
Conclusions
The selective carious tissue removal presented higher success of maintaining pulpal health.
Clinical relevance
In permanent teeth, selective carious tissue removal should be performed, as this technique results in lower numbers of pulp complications, such as pulp exposure, as compared with nonselective removal.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
When carious lesions progress and become cavitated, mechanical removal of carious tissue becomes part of the treatment. For a long time, complete surgical excision or nonselective removal of carious tissue was recommended. In this technique, all demineralized dentine is removed in order to reach hard dentine, where no part of the visible carious tissue is left [1, 2].
In recent years, excessive removal of sound tooth tissue was no longer recommended. However, nonselective removal of carious tissue, which consists of the removal of all softened dentin, not only from the surrounding walls but also from the cavity bottom, is the technique most used and preferred by dental surgeons [3, 4]. It is hypothesized that this technique completely eliminates bacteria, but it is has been reported that 25–50% of bacteria persist after nonselective removal of carious tissue [4, 5]. Moreover, in deep lesions, nonselective removal of carious tissue can lead to accidental pulpal exposure and/or postoperative symptoms. In relation to this, stepwise removal and selective removal of carious tissue are procedures based on the concept of minimal intervention dentistry, which aims at maintaining as much healthy tooth structure as possible, hence keeping teeth functional, supporting an up-to-date way to manage dental carious lesions. Consequently, nonselective removal of hard dentin (earlier recognized as complete excavation or total carious tissue removal) is considered overtreatment, with substantial risks for the pulp if deep carious lesions are treated, as pulp exposure and complications are numerous, frequently demanding supplementary longstanding endodontic interventions [4, 6, 7].
Although the paradigm in dentinal carious lesion treatment shifted when it was accepted that only infected, and not affected, dentine needs to be removed [8], recognition of the relationship between visual appearance of carious tooth tissue and its histopathologic characteristics is not easy. In addition, there have been reports of unnecessary removal of caries due to misunderstanding of histopathology and the feeling that the term “infected” could promote the obsolete and conveyed conception that dental caries is a communicable disease [9]. Consequently, terms referring to the clinically detectable tactile manifestations of carious dentine have been recommended instead of using the terms “infected dentin” and “affected dentin,” attempting to associate, as far as possible, the clinical outcomes to the histologic conditions. A previous recommendation reflected the consensus that the terms soft, leathery, firm, and hard dentine are more helpful in describing the degree to which carious tissues should be removed. For practical reasons, verifying how “soft” or “hard” dentine is most likely the best approach for guiding the clinical dentist in associating the dentinal physical properties with different states of dentine. It is important to remember that at one extreme of carious lesions, soft dentine is related to the histologic terms of necrotic and contaminated zones, with strong recommendation for removal, while at the other extreme, firm, and hard dentine is more associated with sound dentine that must be preserved [9].
Stepwise caries removal consists of the nonselective removal of carious tissue over two sessions. In the first session, all carious dentin is removed from the surrounding walls of the cavity, and then, only the most necrotic and contaminated dentin is removed from the pulp wall, with a temporary sealing (2–6 months) then applied [6, 10, 11]. After this period, the cavity is reopened, remineralization is evaluated, the softened remaining carious tissue is completely removed, and the final restoration is performed. The purpose of this treatment is to reduce the risk of pulpal exposure by stimulating the deposition of tertiary dentin. It is important to consider that stepwise excavation can also be executed selectively, in cases where, during the reopening procedure, a central amount of so far not completely re-hardened dentin is purposely left. However, it is not possible to assume that most stepwise excavations are treated this way, and complications of this treatment include the need for patient return, temporary restoration failure, and accidental pulp exposure during the second intervention [10,11,12,13].
Based on the limitations of the stepwise removal technique and the fact that the presence of leathery carious tissue does not interfere in the inactivation of the carious lesion, the need for cavity reopening has been questioned [4, 5], and selective carious tissue removal has being proposed. This technique is less invasive, consisting of nonselective removal of carious tissue from the surrounding cavity walls, allowing the possibility of remineralizing the affected dentin in the pulpal wall, after a definitive cavity sealing is executed in the same session [4, 13].
Most of the published clinical studies focusing on selective carious removal were performed in deciduous teeth. Furthermore, published systematic reviews did not distinguish the impact of selective removal in permanent or primary teeth [3, 14, 15], and some have suggested that stepwise removal is a type of selective removal [3, 14, 15], which seems inappropriate, since stepwise removal is considered a two-step type of nonselective removal of carious tissue [10,11,12]. For these reasons, further scientific evidence for using selective carious removal in permanent teeth is still necessary.
The focused question of this systematic review is “In permanent teeth, does selective removal of carious tissue for the treatment of dentinal caries present lower risks when compared with nonselective or stepwise removal? Therefore, the PICO question includes dentinal caries in permanent teeth (P), selective removal of carious tissue (I), nonselective or stepwise removal of carious tissue (C), and pulp exposure, dentin deposition, microbiological examination, quality of the restoration, and success of maintaining pulpal health (O).
Therefore, this study aimed to systematically review the literature with meta-analysis regarding the risk of selective removal, in comparison with stepwise and/or nonselective removal, of carious tissue for treating carious permanent teeth with dentinal lesions.
Materials and methods
Search strategy
The databases searched were PubMed, Embase, and Scopus. The search strategy for Pubmed was performed as follows:
#1 - partial caries removal[Title/abstract] OR partial carious dentin removal[Title/abstract] OR Partial Removal of Carious Dentine[Title/abstract] OR Incomplete excavation[Title/abstract] OR Partial excavation[Title/abstract] OR Selective caries removal[Title/abstract] OR Selective carious tissue removal[Title/abstract] OR Selective removal[Title/abstract] OR indirect pulp therapy[Title/abstract] OR Partial Removal of carious dentin[Title/abstract] OR Partial* remov*[Title/abstract]
#2 - Dental Caries[Mesh Terms] OR Decay, Dental[Title/abstract] OR Dentin, Carious[Title/abstract] OR Carious lesions [Title/abstract] OR Caries [Title/abstract] OR Stepwise[Title/abstract] OR Nonselective removal[Title/abstract] OR Complete removal[Title/abstract] OR Complete excavation[Title/abstract]
#3 - #1 AND #2
An adaptation of the abovementioned search strategy was used for the Embase and Scopus databases. The search for available literature was carried out until August 24th, 2018.
Selection criteria
The screening of titles and abstracts was performed independently by two different reviewers (MMAFB and MIQR). Disagreements were resolved through extensive review and discussion by the two reviewers. A third reviewer (FWMGM) was involved when a consensus was not possible.
For inclusion in each study, the following characteristics had to be fulfilled:
Controlled clinical trials and cohort studies. No restriction was imposed regarding the follow-up.
Patients with diagnosis of dental caries in permanent teeth.
Studies in which the treatment was performed, making a definitive restoration.
The test group should be composed of patients undergoing selective removal of carious tissue from permanent teeth, with execution of definitive restoration in the same session. However, in the test group, studies that reopen the cavity could be included if this procedure did not remove further carious tissue.
The control group may consist of nonselective removal and/or stepwise removal of carious tissue.
The primary outcome was overall success of maintaining pulpal health (both clinically and radiographically). The secondary outcomes may be evaluation of the quality of the restoration, microbiological examinations, and dentin deposition.
Overall success of maintaining pulpal health was defined as simultaneous clinical (absence of pulp exposure, presence of pulp sensitivity to cold and/or heat tests, absence of spontaneous pain, soft tissue pathology, or pathologic mobility) and radiographic favorable signs (absence of internal/external root resorption, furcation or periapical radiolucency).
No delimitation of language or date was included in the selection of studies for this systematic review:
Laboratory tests.
Studies on deciduous teeth.
Studies in which the treatment form was constituted by temporary restorations.
Narrative or systematic reviews.
All references to related reviews [15, 16] and the list of references of all included studies detected during the electronic survey were searched for eligibility. During the screening of the title/abstract, the agreement between reviewers resulted in a kappa of 0.87; meanwhile, no disagreement was detected during the full-text reading, resulting in a kappa of 1.
Risk of bias assessment
The risk of bias assessment was performed by two independent reviewers (MMAFB and MIQR), following the criteria defined by the Cochrane Collaboration tool for randomized clinical trials [17]. The following criteria were assessed: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcomes data, selective reporting, and other bias. The risk of bias for the analyzed criteria was classified as low, high, or uncertain.
The Newcastle–Ottawa Quality Assessment Scale was used to evaluate the cohort studies, in which each study can receive one star for each item. Only in the comparability criterion can a maximum of two stars be received. This scale is composed of eight criteria divided into three groups: selection, comparability, and outcome [18]. The discrepancies in the evaluations of the study were solved after extensive discussion between the two reviewers (MMAFB and MIQR). A third reviewer (FWMGM) was involved only when a consensus was not possible.
Data extraction
Data extraction included the following variables: author(s), year of publication, country of patients, number of individuals in each group, mean age or age range, number of restorations performed in all groups, number of teeth lost in the follow-up, class and depth of restorations, number and time of evaluations, and use of calcium hydroxide; and the results of overall success of maintaining pulpal health, failure in restoration, dentin deposition, microbiological analysis, and pulp exposure were the outcomes evaluated. The data extraction was also performed independently by two reviewers (MMAFB and MIQR), and the third reviewer (FWMGM) was involved only when a consensus was not possible.
Statistical analysis: meta-analysis
Initially, no minimum follow-up period was imposed on the studies for inclusion in the present systematic review, since it was intended to perform several meta-analyses according to the different follow-up periods. However, this was not possible because sufficient information was available only for studies with at least 1-year follow-up, and consequently, only one meta-analysis was performed. The pooled risk ratio for the overall success of the pulp status, as previously described, using the different techniques for carious tissue removal, was calculated. Four studies present the same sample [6, 13, 19, 20], and from this sample, only the data from the 18-month study was used, since the follow-up time was the most similar to those periods applied in the other selected studies [20]. In order to make comparisons easier, the data of these individuals were included in the meta-analysis. Those studies with follow-up of less than 1 year [5, 7, 21] were not included in the meta-analysis.
The pooled risk ratio and its 95% confidence interval were calculated for the primary outcome, and subgroups were created, considering the different techniques for caries removal, such as stepwise excavation and nonselective removal of carious tissue. Heterogeneity was assessed by the Q test and quantified by the I2 statistic. As a higher heterogeneity, determined as I2 > 40%, was detected, a random effect model was applied. Meta-analysis was conducted using the software Review Manager (version 5.3).
Results
Study selection
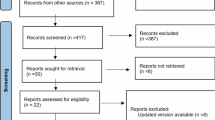
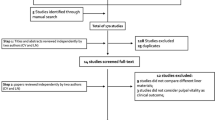
After elimination of the duplicates, 2333 articles were retrieved, and among them, only 10 studies were included in the present systematic review (Fig. 1). However, just six of these studies had clinical trials with different samples [4, 5, 7, 21,22,23], since four articles presented the same group of individuals analyzed at different follow-ups [6, 13, 19, 20]. All studies selected for this systematic review were written in English.

Flowchart of the studies selection of this systematic review
Characteristics of included studies
Of the selected studies, only one was not randomized [4]. Regarding the control group, four studies performed only nonselective removal of carious tissue [4, 5, 7, 23], four studies performed only stepwise removal [6, 13, 19, 20], and two studies performed nonselective or stepwise removal of carious tissue [21, 22]. All studies performed definitive restorations after the interventions—six studies used composite resin as the restorative material [4, 5, 7, 21,22,23], while the other four studies had also used amalgam [6, 13, 19, 20] (Table 1).
Risk of bias assessment
None of the nine randomized clinical trials presented low risk of bias for all evaluated criteria. Four studies reported that participant blinding was not possible [6, 13, 19, 20], and two others did not mention blinding of participants or personnel [21, 22]. One study presented five criteria as having an unclear risk of bias [7], and another presented three criteria as having unclear risk of bias [23]. All studies had a low risk of bias for incomplete outcome data and selective reporting. Operator calibration was mentioned in only four studies [6, 20, 22, 23]. The other five studies did not report the calibration process, besides being considered as unclear for other bias criteria [5, 7, 13, 19, 21]. Therefore, the risk of bias assessment showed a moderate heterogeneity among the included studies, ranging from one point not mentioned (unclear risk) or a negative point (low risk of bias) to four points not mentioned (unclear risk) (Fig. 2).

Risk assessment of bias from the included randomized clinical trials
Only one retrospective cohort study was included in this systematic review [4], with one criterion regarding the representativeness of the sample being considered inappropriate, since the research consisted of a retrospective study and presented a convenience sample. All other criteria evaluated were considered adequate (Fig. 3).

Risk assessment of bias of the non-randomized study included
Qualitative analysis
Microbiological evaluation was performed in two studies by counting the number of colony forming units (CFU) for total viable microorganisms, Streptococcus species and Lactobacillus species [5, 21]. In both studies, the selective and nonselective removals of carious tissue were effective in reducing the total microbial load, without statistically significant differences between groups [5, 21].
Only one study evaluated the quality of the restorations after the treatments and concluded that no significant difference in the longevity of the restorations was detected (p = 0.163). Additionally, a single study evaluated the deposition of dentin after the treatments, using mineral trioxide aggregate (MTA) as pulp protection material. After 4 weeks, no significant difference in the remineralization level was found between the groups that performed nonselective or selective removal of carious tissue [7].
Regarding the pulp exposure outcome, the three studies in which the control group was represented by nonselective or stepwise removal of carious tissue treatments presented a greater risk of pulp exposure compared with the selective removal [4, 6, 20]. However, stepwise removal presented a lower risk of accidental pulp exposure when compared with nonselective removal [22]. One of the studies included in this review reported that pulp exposure occurred during treatments, but these teeth were excluded from the study, so it is not known to which group they belonged [21].
Meta-analysis for success of maintaining pulpal health
Four studies were included in the meta-analysis for overall success of maintaining pulpal health [4, 6, 22, 23] (Fig. 4). Statistically significant differences were found between groups (risk ratio, 95% confidence interval 1.11, 1.02–1.21). Selective removal proved to be more effective in preserving pulpal health status. Analysis of the subgroups demonstrated the same trend of results for the nonselective removal until reaching hard dentine (RR, 95% CI 1.09, 1.02–1.17). However, no statistically significant difference was detected for the stepwise excavation (RR, 95% CI 1.10, 0.88–1.38).

Meta-analysis for the overall success of the pulp status (success of the pulp status was defined as simultaneous clinical (absence of pulp exposure, presence of pulp sensitivity to cold and/or heat tests, absence of spontaneous pain, soft tissue pathology, or pathologic mobility) and radiographic success (absence of internal/external root resorption, furcation, or periapical radiolucency) at the follow-up of at least 12 months. The control group was composed by stepwise excavation or nonselective removal of carious tissue removal
Discussion
This study compared the risk difference of selective removal of carious tissue in permanent teeth with stepwise excavation and nonselective removal. The meta-analysis showed a statistically significant difference, favoring selective removal of carious tissues for overall success of maintaining pulpal health. Secondary outcomes, such as microbiological evaluation [5, 21], restoration quality [4], and dentin deposition [7], also did not differentiate the treatments. However, pulp exposure is more frequent when techniques of nonselective removal of carious tissue are used as compared with selective removal [4, 6, 20, 22]. In addition, one of the selected articles concluded that regardless of the caries removal technique, multiple surface restorations, restorations performed with glass ionomer cements, and poor oral hygiene are risk factors for failure [4].
Previously published systematic reviews of selective removal versus nonselective removal of carious tissue or stepwise excavation did not differentiate between the success of the technique for deciduous and permanent teeth [3, 14, 15]. However, it is known that deciduous teeth have a greater potential for regeneration and greater capacity for self-renewal and cellular proliferation [24], and thus, these results should not be extrapolated to permanent dentition.
In addition, the present study is the first review to include nonselective removal of carious tissue and stepwise excavation treatments in the control group, since they are considered one and two step, respectively, nonselective removals of carious tissue. Previous reviews have compared only selective removal and nonselective removal of carious tissue [15] or further consider the stepwise excavation as a selective two-step removal [3, 14].
One of the difficulties for all studies of caries removal is the lack of standardization of the degree of excavation. This drawback is inherent in this type of study because an operator can remove more or less carious tissue using the same technique, making accurate comparisons more difficult. In addition, it is still unclear whether leaving more carious dentin may be beneficial (less exposure to pulp and symptoms) or harmful (increased risk of failure for restorations) [3].
In the scientific literature, the term selective removal may be presented as synonymous with partial or incomplete caries removal. However, these terms are considered inappropriate, since they give the idea of a negative association with treatment, as if it were below ideal, being considered as a disadvantage in the support and acceptance of this procedure as a reliable technique [25].
In the included studies, the follow-ups varied considerably from 3 months to 5 years, preventing the inclusion of all studies in the meta-analysis regarding success of maintaining pulpal health. Most studies reported that deep caries treatments were performed, but the scientific literature describes at least four parameters in the selected studies defining what constitutes a deep caries (radiolucency in half or more of the dentin, radiolucency in three quarters or more of the dentin, in 0.25 to 1 mm of the pulp, or equal to or greater than the middle third of the dentin), making the comparisons more heterogeneous [6, 7, 20, 22, 23].
It was not possible to carry out the meta-analysis of the microbiological results of the studies of this review, because they collected carious dentin at different times, with one study collecting the material for microbiological analysis before final restoration and the other study collecting the material months after restoration, after reopening the cavity. Despite the methodological differences, both studies demonstrated reductions in the microbial load for all the evaluated groups, without statistical differences between the groups with selective removal or nonselective removal of carious tissue, or stepwise excavation [5, 21].
Selective removal, when compared with stepwise excavation of carious tissue, presented similar and satisfactory results regarding the maintenance of pulpal health. Selective removal has several advantages, such as the maintenance of part of the affected dentin, reduced risk of pulpal exposure, no need for cavity reopening, less time wasted and a reduction in material employed, and no need for patient collaboration for returning [4, 10,11,12,13].
None of the studies included in this systematic review were considered as having low risk of bias in all criteria, decreasing the overall strength of evidence of these studies. However, most studies presented several risk assessment criteria for bias as low risk. In addition, it is possible to define the methodological and sample differences of the studied articles as limitations of this study, rendering meta-analysis of all the outcomes impossible.
Furthermore, with regard to pulp status, the main outcome examined in this study, the absence of differences between the removal techniques may be also attributed to the limited number of teeth included, as well as other factors, such as the material used for performing the indirect pulp capping as well as cytotoxic effects of restorative materials (e.g., adhesive systems), which may be more important factors concerning long-term success of maintaining pulpal health. Although the studies of this systematic review used different materials when performing pulp capping, with the calcium hydroxide liner the most reported, no evidence is provided that assures the clinical success of treatment for deep caries lesions when the calcium hydroxide liner is used [25].
Scientific evidence already advises the use of selective removal over other techniques to achieve similar efficacy [19, 26, 27]. This systematic review now confirms this evidence in permanent teeth. In addition, one study confirmed that selective caries removal is more cost-effective, and that teeth with deep caries may be kept longer in the oral cavity [3]. All the studies included in the present systematic review have demonstrated safety and efficacy related to selective removal of carious tissue for permanent teeth, because it leads to reduced pulp exposure [3, 27]. However, the adoption of selective removal procedures does not appear to be a popular choice among dentists, since the scientific literature shows that several clinicians prefer more invasive techniques despite these latter techniques being associated with an increased risk of pulpal exposure and the absence of reduced bacteria counts in the remaining dentin [27,28,29]. Accordingly, although the proportion of dentists who prefer invasive instead of evidence-based management strategies for deep carious lesions in permanent teeth seems to have decreased in recent years, the majority of dentists in most countries have rejected evidence-based carious tissue removal strategies [28,29,30]. Furthermore, a previous study showed that a significant association was found between the use of evidence-based information in the English-language scientific literature and Japanese dentists’ preference for selective removal procedures [29], rather than those dentists opting for removal of all carious tissues and proceeding with endodontic-related procedures. Thus, this review may help in disseminating these important findings to the dental community, reducing resistance among clinicians regarding this conservative technique.
Conclusion
Selective removal resulted in greater success of maintaining pulp vitality compared with both stepwise excavation and nonselective removal. Secondary results, such as microbiological evaluation, restoration quality, and dentin deposition, also presented similar results among treatments. However, a higher frequency of pulp exposure was found when using nonselective removal or stepwise excavation. Therefore, selective removal should be performed in permanent teeth, since it is performed in a single session and preserves a greater amount of dental structure.
References
Manton D (2013) Partial caries removal may have advantages but limited evidence on restoration survival. Evid Based Dent 14:74–75. https://doi.org/10.1038/sj.ebd.6400948
Schwendicke F, Frencken J, Innes N (2018) Caries excavation: evolution of treating cavitated carious lesions. Karger Medical and Scientific Publishers, Basel
Schwendicke F, Stolpe M, Meyer-Lueckel H, Paris S, Dorfer CE (2013) Cost-effectiveness of one-and two-step incomplete and complete excavations. J Dent Res 92:880–887. https://doi.org/10.1177/0022034513500792
Casagrande L, Seminario AT, Correa MB, Werle SB, Maltz M, Demarco FF, Araujo FB (2017) Longevity and associated risk factors in adhesive restorations of young permanent teeth after complete and selective caries removal: a retrospective study. Clin Oral Investig 21:847–855. https://doi.org/10.1007/s00784-016-1832-1
Bitello-Firmino L, Soares VK, Damé-Teixeira N, Parolo CCF, Maltz M (2018) Microbial load after selective and complete caries removal in permanent molars: a randomized clinical trial. Braz Dent J 29:290–295. https://doi.org/10.1590/0103-6440201801816
Maltz M, Garcia R, Jardim JJ, Paula LM, Yamaguti PM, Moura MS, Garcia F, Nascimento C, Oliveira A, Mestrinho HD (2012) Randomized trial of partial vs. stepwise caries removal: 3-year follow-up. J Dent Res 91:1026–1031. https://doi.org/10.1177/0022034512460403
Pratiwi AR, Meidyawati R, Djauharie N (2017) The effect of MTA application on the affected dentine remineralization after partial caries excavation (in vivo). Journal of Physics: Conf Series 884:012119. https://doi.org/10.1088/1742-6596/884/1/012119
Fusayama T (1997) The process and results of revolution in dental caries treatment. Int Dent J 47:157–166
Innes NP, Frencken JE, Bjorndal L, Maltz M, Manton DJ, Ricketts D, Van Landuyt K, Banerjee A, Campus G, Doméjean S, Fontana M, Leal S, Lo E, Machiulskiene V, Schulte A, Splieth C, Zandona A, Schwendicke F (2016) Managing carious lesions: consensus recommendations on terminology. Adv Dent Res 28:49–57. https://doi.org/10.1177/0022034516639276
Bjørndal L, Larsen T, Thylstrup A (1997) A clinical and micro-biological study of deep carious lesions during stepwise excavation using long treatment intervals. Caries Res 31:411–417. https://doi.org/10.1159/000262431
Bjørndal L, Larsen T (2000) Changes in the cultivable flora in deep carious lesions following a stepwise excavation procedure. Caries Res 34:502–508. https://doi.org/10.1159/000016631
Bjørndal L (2008) Indirect pulp therapy and stepwise excavation. Pediat Dent 30:225–229. https://doi.org/10.1016/j.joen.2008.02.035
Maltz M, Koppe B, Jardim JJ, Alves LS, Paula LM, Yamaguti PM, Almeida JCF, Moura MS, Mestrinho HD (2018) Partial caries removal in deep caries lesions: a 5-year multicenter randomized controlled trial. Clin Oral Investig 22:1337–1343. https://doi.org/10.1007/s00784-017-2221-0
Ricketts D, Lamont T, Innes NP, Kidd E, Clarkson JE (2013) Operative caries management in adults and children. Cochrane Database Syst Rev 3. https://doi.org/10.1002/14651858.CD003808.pub3
Li T, Zhai X, Song F, Zhu H (2018) Selective versus non-selective removal for dental caries: a systematic review and meta-analysis. Acta Odontol Scand 76:135–140. https://doi.org/10.1080/00016357.2017.1392602
Schwendicke F, Dörfer CE, Paris S (2013) Incomplete caries removal: a systematic review and meta-analysis. J Dent Res 92:306–314. https://doi.org/10.1177/0022034513477425
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj 343:d5928. https://doi.org/10.1136/bmj.d5928
Wells G, Shea B, O’Connell D (2012) The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa, ON. http://www.ohri.ca/programs/clinical_epidemiology/oxford_web.ppt. Accessed 12 October 2018
Maltz M, Moura MS, Jardim JJ, Marques C, Paula LM, Metrinho HD (2010) Partial caries removal in deep lesions: 19-30 months follow-up study. Rev Fac Odontol 51:20–23
Maltz M, Jardim JJ, Mestrinho HD, Yamaguti PM, Podestá K, Moura MS, Paula LM (2013) Partial removal of carious dentine: a multicenter randomized controlled trial and 18-month follow-up results. Caries Res 47:103–109. https://doi.org/10.1159/000344013
Orhan AI, Oz FT, Ozcelik B, Orhan K (2008) A clinical and microbiological comparative study of deep carious lesion treatment in deciduous and young permanent molars. Clin Oral Investig 12:369–378. https://doi.org/10.1007/s00784-008-0208-6
Orhan AI, Oz FT, Orhan K (2010) Pulp exposure occurrence and outcomes after 1-or 2-visit indirect pulp therapy vs complete caries removal in primary and permanent molars. Pediatr Dent 32:347–355
Rando-Meirelles MPM, Tôrres LHN, Sousa M (2013) Twenty-four months of follow-up after partial removal of carious dentin: a preliminary study. Dentistry. 3:2161–1122.1000162. https://doi.org/10.4172/2161-1122.1000162
Kaukua N, Chen M, Guarnieri P, Dahl M, Lim ML, Yucel-Lindberg T, Sundstrom E, Adameyko I, Mao JJ, Fried K (2015) Molecular differences between stromal cell populations from deciduous and permanent human teeth. Stem Cell Res Ther 6:59. https://doi.org/10.1186/s13287-015-0056-7
da Rosa WLO, Lima VP, Moraes RR, Piva E, da Silva AF (2018) Is a calcium hydroxide liner necessary in the treatment of deep caries lesions? A systematic review and meta-analysis. Int Endod J 52:588–603. https://doi.org/10.1111/iej.13034
Oliveira EF, Carminatti G, Fontanella V, Maltz M (2006) The monitoring of deep caries lesions after incomplete dentine caries removal: results after 14–18 months. Clin Oral Investig 10:134–139. https://doi.org/10.1007/s00784-006-0033-8
Thompson V, Craig RG, Curro FA, Green WS, Ship JA (2008) Treatment of deep carious lesions by complete excavation or partial removal: a critical review. J Am Dent Assoc 139:705–712
Schwendicke F, Göstemeyer G (2016) Understanding dentists’ management of deep carious lesions in permanent teeth: a systematic review and meta-analysis. Implement Sci 11:142–153. https://doi.org/10.1186/s13012-016-0505-4
Kakudate N, Yokoyama Y, Sumida F, Matsumoto Y, Gordan VV, Gilbert GH (2019) Dentists’ practice patterns of treatment for deep occlusal caries: findings from a dental practice-based research network. J Dent 84:76–80
Oen KT, Thompson VP, Vena D, Caulfield PW, Curro F, Dasanayake A, Ship JA, Lindblad A (2007) Attitudes and expectations of treating deep caries: a PEARL Network survey. Gen Dent 55:197–203
Funding
This study was supported by the Brazilian Governmental Agency CAPES by using the Portal de Periódicos CAPES. The first author was supported by a CAPES (National Council for the Improvement of Higher Education) scholarship funded by the Brazilian government during her Ph.D course, when this research was conducted.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Barros, M.M.A.F., De Queiroz Rodrigues, M.I., Muniz, F.W.M.G. et al. Selective, stepwise, or nonselective removal of carious tissue: which technique offers lower risk for the treatment of dental caries in permanent teeth? A systematic review and meta-analysis. Clin Oral Invest 24, 521–532 (2020). https://doi.org/10.1007/s00784-019-03114-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-03114-5