
Abstract
Objectives
To assess the effect of additional apical enlargement using nickel titanium (NiTi) instruments on the incidence of microcracks using micro-computed tomographic analysis.
Materials and methods
Fifty-one premolars with single canals were enlarged to ProTaper Gold (PTG) F2 (25/08) (Dentsply Sirona), ProFile Vortex Blue (VB) 25/06 (Dentsply Tulsa), or WaveOne Gold (WOG) primary (25/07) (Dentsply Sirona) NiTi rotary instruments (n = 17 each). Afterward, additional apical enlargement was performed in each group with its corresponding larger instrument (F3 (30/09), VB 30/06, or WOG Medium (35/06) instruments, respectively). All teeth were imaged with micro-computed tomography before canal enlargement and after initial and additional apical enlargements to detect new microcracks at the apical 5 mm. An Aligned Rank Transform ANOVA was conducted to examine the effects of file type and canal enlargement on the number of new microcracks resulting from enlargement. A Kruskal-Wallis test was run to compare the file types at each canal enlargement stage.
Results
A significant main effect (P = 0.026) of canal enlargement on the number of new microcracks was found; the number of apical microcracks found after additional enlargement was significantly greater than baseline (P = 0.021); no significant difference was found between baseline and initial enlargement (P = 0.506) and between initial enlargement and additional enlargement (P = 0.252). The Kruskal-Wallis tests found no difference between file types at baseline (P = 0.348), after initial enlargement (P = 0.369) or additional enlargement (P = 0.133).
Conclusions
Regardless of the instrumentation system used, additional apical enlargement led to the formation of high number of new microcracks.
Clinical significance
The results indicated that additional enlargement induced significant number of apical microcracks.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Root canal enlargement is performed to provide adequate space for efficient disinfection and filling of the root canal system. However, this step may weaken the root [1] by decreasing its thickness [2, 3] and creating stresses mainly at the apical area [4], thus inducing the formation of apical microcracks in root canal dentine [5,6,7,8,9,10]. Clinically, untreated cracked teeth show little progression of symptoms or cracks within the short-term [11] and do not usually have clinical implications until complete cracking or vertical root fracture (VRF) occurs [2], which could lead to tooth loss. Indeed, VRF reportedly affected 13.4% of extracted endodontically treated teeth [12]. Therefore, it is essential to investigate potential causes of microcracks. Several studies were conducted in order to understand the impact of different stages of endodontic procedures on crack formation or growth [5, 8,9,10, 13].
Advances in manufacturing technologies have come up with new thermomechanical processes and designs of rotary nickel-titanium (NiTi) instruments. ProTaper Gold system (PTG; Dentsply Sirona), a new version of ProTaper Universal, is made of gold wire and has different metallurgical characteristics with 2-stage specific transformation behavior to create an instrument with stable martensitic phase at intracanal temperature [14]. It consists of 3 shaping (SX, S1, and S2) and 5 finishing (F1, F2, F3, F4, and F5) instruments which have triangular cross-sections and variable tapers and are used in continuous motion. WaveOne Gold (WOG, Dentsply Sirona), the new generation of WaveOne, is a single-instrument system that uses reciprocating kinematics. This system has 4 instruments (Small, Primary, Medium, and Large) with an alternating offset and transitioning parallelogram-shaped cross-section [15]. The manufacturing process of this system is claimed to be similar to PTG. Vortex Blue (VB; Dentsply Tulsa Dental Specialties) was introduced as the second generation of ProFile Vortex system. VB instrument is made from M-wire with a proprietary manufacturing process that creates an oxide surface layer which gives it a blue color [16]. It is a multi-instrument system with a triangular cross-section, a novel design in helical angles and non-landed cutting blades, and is used in continuous motion. The abovementioned systems exhibit improved mechanical properties compared to their older versions [14,15,16].
Canal enlargement is considered an important step to accomplish adequate canal debridement. However, there is no consensus on the ideal size for apical enlargement. Some authors promote a minimally tapered canal enlargement to preserve dentine, reduce the chance of apical transportation, and keep the canal size as small as practical in order to reduce teeth susceptibility to fracture [9]. Others, however, suggest shaping the canal up to eight file sizes larger than the initial apical binding instrument for improved disinfection and better removal of the infected debris and eradication of bacteria [17,18,19]. Duque et al. [20] showed that further apical enlargement favorably reduced the percentage of untouched areas and maintained the trajectory of curved canals with acceptable canal shaping abilities. Furthermore, a 12-month follow-up randomized controlled trial reported that the proportion of successfully healed cases was higher with increased apical preparation size in mandibular first molars [21]. However, crack studies that investigated the effect of canal enlargement with ProTaper Universal, K3, and ProFile systems found that greater apical enlargement is associated with higher number of microcracks [6, 9]. The observational techniques used in these studies were stereomicroscope and scanning electron microscope which have their inherent limitations such as inability to detect cracks that are formed before initiating the root canal procedure or reveal microcracks that are formed after canal enlargement; moreover, creation of cracks during slicing the root is also of concern [10, 22]. Currently, there is a trend to use non-invasive techniques in studies evaluating microcrack formation, and micro-computed tomography (microCT) got great attention since it has the ability to visualize the internal structure and cuspal deflection before and after canal enlargement [10, 22,23,24].
There is a paucity of scholarly literature on the use of this technique to evaluate the effect of additional apical enlargement on microcrack formation. Thus, this laboratory study was performed to detect the effect of additional canal enlargement on microcrack development in the apical region of the root using microCT with a very high isotropic resolution. The null hypothesis tested in the present study was that the additional canal enlargement with heat-treated NiTi instruments (PTG, WOG, and VB) does not cause microcracks.
Methodology
Tooth selection
Single-rooted defect-free premolar teeth with single straight (< 10○ curvature) canals, that were extracted for orthodontic reasons, were selected. Teeth were disinfected and kept in distilled water until use. Teeth were inspected clinically under a dental operating microscope to exclude teeth with external fracture lines, open apices, resorption, or external anatomic irregularities. The external surfaces of the selected teeth were cleaned by a sharp hand scaler.
Sample preparation
The samples were prepared as described previously [5]. Briefly, each root was covered with a single sheet of aluminum foil and embedded centrally in a mixed acrylic resin (Ostron; GC Corporation, Tokyo, Japan) surrounded by a custom-made rubber tube. This gave a resin with a height of 16 mm and a diameter of 20 mm. Then, the tooth was removed from the resin and the aluminum foil was discarded. The root surface and the negative impression of the root in the resin were coated with a hydrophilic vinyl polysiloxane impression material (Examixfine, GC Corporation), and the tooth was repositioned. The impression material filled the space created by the foil, thus simulating the periodontal ligament. Then, coronally the tooth was flattened to the upper edge level of the resin to standardize the root length, ensure a straight access line, and provide a reference plane. Working length (WL) was defined as the distance from the occlusal reference plane to the apex minus 1 mm. Canal width was defined by inserting a size 20 K-file instrument that would engage slightly at the working length. Otherwise, the tooth was excluded.
The sample size was calculated based on an effect size of 1.0 using a significance level of 0.05 and a power of 80% to detect a difference. The estimated sample size for each group was 17 (PiFace, http://homepage.stat.uiowa.edu/~rlenth/Power/). Fifty-one teeth were finally selected and maintained immersed in distilled water throughout the study.
Micro-computed tomography scanning
The tooth’s internal anatomy was initially scanned (Baseline) by using microCT (SkyScan 1172; Bruker micro-CT, Kontich, Belgium). Each tooth was mounted on the computer-controlled turntable of the microCT system in a way that would target the X-ray beam perpendicular to the long axis of the root. An aluminum-copper filter was placed in front of the detector. An air calibration of the detector was performed before each scan to decrease the beam hardening effect and lessen ring artifacts. X-rays were generated at a voltage of 80 kV and an electric current of 124 μA. Scanning was performed by rotating the tooth 360 degrees at 6 micrometers isotropic voxel size. The distances from the X-ray source to the sample and detector were 72 mm and 215 mm, respectively. TIFF files were acquired for the reconstruction of a 3D image of the apical 5 mm portion with NRecon 1.6.3 software (Bruker micro-CT) using ring artifact correction of 5 and beam hardening correction of 40% as well as minimum and maximum contrast limits.
Based on these data, the teeth were randomly divided into 3 experimental groups of 17 teeth each according to the file system used: PTG, VB, and WOG. Since the data were normally distributed (Shapiro-Wilk test; P > 0.05), one-way ANOVA test was used to verify that the groups were not different with respect to the number of pre-existing microcracks, canal length, and canal diameters at the 2- and 3-mm levels observed in the microCT images (P > 0.05) (Table 1).
Canal enlargement
Each instrument had a rubber stopper firmly attached with cyanoacrylate 15 mm from the tip to limit instrumentation to the WL. All the instruments were driven using an X-Smart Plus Motor (Dentsply Sirona), and the rotational speed and torque were set following the manufacturer’s instructions. The samples were instrumented in two stages: initial instrumentation and additional instrumentation. In PTG, S1 (17/05) and S2 (20/06) instruments were used to instrument the coronal and middle parts of the canal. Then, S1, S2, F1 (20/07), and F2 (25/08 taper) were sequentially used to the WL at 300 rpm speed and 2 Ncm torque. In WOG, a WOG Primary instrument (25/07) was used with the WO system to shape the canals to the WL, inserted three times in a slow in-and-out pecking motion by using the “WAVEONE ALL” mode. In VB, sequential use of 20/04, 25/04, 20/06, and 25/06 instruments was performed to the WL at 500 rpm speed and 2 Ncm torque.
Afterward, additional apical enlargement was performed in each group with its corresponding larger instrument (F3 (30/09), VB 30/06, or WOG Medium (35/06) instruments, respectively). The canal patency was controlled with a K file size 10 and frequent irrigation with 2.5% sodium hypochlorite. All the samples were instrumented by an experienced endodontist.
Evaluation of newly formed microcrack
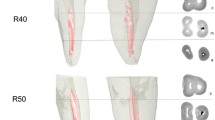
Using the same settings and procedures illustrated earlier for the first scan, a microCT scan was conducted two more times, after initial canal enlargement and after additional canal enlargement, to assess whether any new microcrack was present (Fig. 1). Serial cross-sectional views along the 5 mm apical portion (833 slices in each sample) were inspected by three independent trained observers. A microcrack that initiated from the canal space into the dentine and was not found in the previous scan was considered and annotated (Fig. 1). In the event of differences of opinions, a consensus was reached after discussion among the three observers.

Illustration of the experiment. Representative microCT images from the same level taken as a baseline (a), after initial canal enlargement (b), and after larger apical canal enlargement (c). A single microcrack that was caused by the initial enlargement is depicted with white dashed arrows
Statistical analysis
The dependent variable was the number of new microcracks, treated as count data. The between-subjects factor was file type (WOG, PTG, or VB), treated as categorical data, and the within-subjects factor was canal enlargement (baseline, initial canal enlargement, and additional canal enlargement), treated as ordinal data. An Aligned Rank Transform ANOVA was conducted to examine the effects of file type and canal enlargement on the number of new microcracks resulting from enlargement. Kruskal-Wallis test was run to compare the file types at each canal enlargement stage. Statistical analysis was performed with R version 3.6.0 at a 5% significant level.
Results
The frequency of teeth affected by microcracks and the total of microcracks are shown in Table 1. Pre-existing apical microcracks were found in 80% of the samples. No interaction effect was found between file type and time point on the number of new microcracks resulting from enlargement (P = 0.92). However, a significant main effect (P = 0.026) of canal enlargement on the number of new microcracks was found; the number of apical microcracks found after additional enlargement was significantly greater than baseline (P = 0.021); no significant difference was found between baseline and initial enlargement (P = 0.506) and between initial enlargement and additional enlargement (P = 0.252). Kruskal-Wallis tests found no difference between file types was found at baseline (P = 0.348), after initial enlargement (P = 0.369), or additional enlargement (P = 0.133). The microcracks were observed in buccolingual and mesiodistal directions and no VRFs were detected in the present data.
Discussion
Canal enlargement produces significant strain in root dentine leading to the formation of microcracks [5, 8, 10, 25] that might progress to VRF, which is pathognomonic for a distinctive fatigue type of failure mechanism [2, 10]. The current study was designed to evaluate the effect of additional enlargement on microcrack development non-invasively. Damage initiation and propagation in dentine seem to increase in aged specimens [26]; therefore, the teeth were obtained from young patients that had their teeth extracted for orthodontic reasons. A layer of impression material was used to simulate the periodontal ligament and allow the sample to move within a limited space and avoid external reinforcement [5]. The apical region of the root was scanned and presently studied since the enlargement forces near the instrument’s tip are inevitable and generate the most stresses along with the instrument [4] that could generate microcrack [5,6,7,8,9,10]. Each sample was scanned by microCT three times: before canal enlargement (baseline), after initial enlargement, and after additional enlargement. There were no significant differences between the tested file systems (P > 0.05). Throughout the experimental groups, the additional enlargement caused a statistically significant increase in microcracks compared to baseline (P < 0.05). Therefore, the null hypothesis was rejected.
Throughout the experimental groups, initial enlargement caused new microcracks but the number of these microcracks was not significant compared to baseline. However, when larger instruments were used, the number of microcracks increased significantly and many samples were affected by more than 1 new microcrack (Table 1). This can be explained by greater contact between the larger instrument and the canal wall which creates numerous stress concentration areas from which a microcrack may develop [27]. Our results are in agreement with earlier studies which were conducted using other NiTi systems [6, 9].
The NiTi systems were used according to the manufacturers’ instructions. It is of note that although the motion kinematics and number of files used during initial enlargement were different (PTG and VB used 4 instruments, and WOG used 1 instrument), there was no statistical difference between the number of new microcracks found after both initial and additional enlargements. Thus, the results of this study suggest that these differences do not reflect the development of new microcracks, but rather, further removal of dentine during additional enlargement.
The literature on microcrack development induced by different endodontic procedures is full of discrepancies and controversies [6,7,8, 10, 21]. This inconsistency is attributed to differences in tooth selection, storing conditions, experimental set-up, observational technique, spatial resolution of microCT scanning, and the definition used to classify the dentinal defects [10, 28]. Microcracks were previously assessed by observing sectioned roots with stereomicroscope under different magnifications [6, 10, 29, 30]. However, this approach is considered invasive since root sectioning is needed at each level of observation. Moreover, it only allows evaluating a few slices per tooth thus increasing the chances of a defect going undetected [10]. Most of root dentine microcracks run in an apical to coronal direction; thus, in the studies where root sectioning is performed, the same microcrack might be counted more than once leading to an exaggerated estimate of the number of microcracks. On the other hand, microCT is used to provide cross-sectional slices with high resolution that can be compiled to create three-dimensional images [22]. This non-invasive novel technology has the advantage of studying dentinal microcracks longitudinally throughout the experimental procedures [8, 22], thus allowing sequential analysis without sample destruction and assessing microcrack developed at different stages of root enlargement.
Previous studies have raised concerns regarding dehydration-induced microcracking [10, 31]. This is a limitation when utilizing extracted teeth. To address this issue, the samples were maintained in distilled water for the duration of the present study. It is worth mentioning that earlier crack studies did not specify the storing media [10] which could compromise the dentine’s mechanical characteristics. Lim et al. [32] showed that the biomechanical response of dentine to enlargement was affected by hydration. The loss of water causes residual strain in dentine [33], which adversely affects the mechanical integrity and the response of dentine to enlargement forces, thus facilitating microcrack development [34]. Therefore, each sample was kept moist by wrapping the root with gauze soaked in a distilled water to prevent heat-induced dehydration of the samples during the scanning process [35]. Each sample was returned to the storing media soon after each scan.
The microCT images with high spatial resolution and very small voxel size were found to better visualize microcracks [28]. In this regard, a previous study suggested the use of microCT technology with higher resolution in order to confirm the presence of all microcracks more precisely [36]. It was reported that the 9-μm resolution is potentially useful and effective in detecting fracture lines [28]. Therefore, the present study used a resolution of 6 μm. To our knowledge, this is the smallest microCT voxel size used to detect dentinal microcracks which could explain the high incidence of apical microcracks in this study especially in the baseline observation. The baseline microCT images were used to observe the presence of pre-existing microcracks before root canal enlargement. In our study, 80% of the samples showed pre-existing apical microcracks which might be the result of occlusal or extraction forces, or the storage conditions of the extracted teeth. Consistently, previous microCT studies (22, 36) showed pre-existing microcracks in their samples. Moreover, the microCT was able to show internal microcracks that were not evident during teeth selection under the dental operating microscope. This adds a major benefit to the use of this non-invasive technology in endodontic research.
Caution must be exercised when interpreting the results of this study. This investigation was based on an evaluation of extracted teeth with varying morphology. However, equal and comparable distribution was undertaken with respect to the number of pre-existing apical microcracks, apical canal diameter, and the WL. Furthermore, the canal enlargement procedures were done by an endodontist who has prior training and experience in using the NiTi rotary systems utilized in this study and meticulous efforts were made to maintain a consistent force on the instruments with slow “in-and-out” movements.
Conclusions
Regardless of the instrumentation system used, canal enlargement led to the formation of microcracks. The significant development of new microcracks was found to be a product of the removal of dentine during additional apical enlargement.
References
Sathorn C, Palamara JE, Messer HH (2005) A comparison of the effects of two canal preparation techniques on root fracture susceptibility and fracture pattern. J Endod 31:283–287
Wilcox LR, Roskelley C, Sutton T (1997) The relationship of root canal enlargement to finger-spreader induced vertical root fracture. J Endod 23:533–534
Lang H, Korkmaz Y, Schneider K, Raab WH (2006) Impact of endodontic treatments on the rigidity of the root. J Dent Res 85:364–368
Nalla RK, Kinney JH, Ritchie RO (2003) On the fracture of human dentin: is it stress- or strain-controlled? J. Biomed. Mater. Res. 67:484–495
Adorno CG, Yoshioka T, Suda H (2009) The effect of root preparation technique and instrumentation length on the development of apical root cracks. J Endod 35:389–392
Adorno CG, Yoshioka T, Suda H (2011) Crack initiation on the apical root surface caused by three different nickel-titanium rotary files at different working lengths. J Endod 37:522–525
Ashwinkumar V, Krithikadatta J, Surendran S, Velmurugan N (2014) Effect of reciprocating file motion on microcrack formation in root canals: an SEM study. Int Endod J 47:622–627
Jamleh A, Komabayashi T, Ebihara A, Nassar M, Watanabe S, Yoshioka T, Miyara K, Suda H (2015) Root surface strain during canal shaping and its influence on apical microcrack development: a preliminary investigation. Int Endod J 48:1103–1111
Çapar ID, Uysal B, Ok E, Arslan H (2015) Effect of the size of the apical enlargement with rotary instruments, single-cone filling, post space preparation with drills, fiber post removal, and root canal filling removal on apical crack initiation and propagation. J Endod 41:253–256
Versiani MA, Souza E, De-Deus G (2015) Critical appraisal of studies on dentinal radicular microcracks in endodontics: methodological issues, contemporary concepts, and future perspectives. Endod Topics 33:87–156
Hilton TJ, Funkhouser E, Ferracane JL, Gilbert GH, Gordan VV, Bennett S, Bone J, Richardson PA, Malmstrom H, National Dental PBRN Collaborative Group (2020) Symptom changes and crack progression in untreated cracked teeth: one-year findings from the National Dental Practice-Based Research Network. J Dent. 93:103269
Toure B, Faye B, Kane AW, Lo CM, Niang B, Boucher Y (2011) Analysis of reasons for extraction of endodontically treated teeth: a prospective study. J Endod 37:1512–1515
Adorno C, Yoshioka T, Jindan P, Kobayashi C, Suda H (2013) The effect of endodontic procedures on apical crack initiation and propagation ex vivo. Int Endod J 46:763–768
Hieawy A, Haapasalo M, Zhou H, Wang ZJ, Shen Y (2015) Phase transformation behavior and resistance to bending and cyclic fatigue of ProTaper Gold and ProTaper Universal instruments. J Endod 41:1134–1138
Adıgüzel M, Çapar ID (2017) Comparison of cyclic fatigue resistance of WaveOne and WaveOne Gold small, primary, and large instruments. J Endod 43:623–627
Gao Y, Gutmann JL, Wilkinson K, Maxwell R, Ammon D (2012) Evaluation of the impact of raw materials on the fatigue and mechanical properties of ProFile Vortex rotary files. J Endod 38:398–401
Weiger R, Bartha T, Kalwitzki M, Löst C (2006) A clinical method to determine the optimal apical preparation size. Part I. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:686–691
Rodrigues RCV, Zandi H, Kristoffersen AK, Enersen M, Mdala I, Ørstavik D, Rôças IN, Siqueira JF Jr (2017) Influence of the apical preparation size and the irrigant type on bacterial reduction in root canal-treated teeth with apical periodontitis. J Endod 43:1058–1063
Siqueira JF Jr, Perez AR, Marceliano-Alves MF et al (2018) What happens to unprepared root canal walls: a correlative analysis using micro-computed tomography and histology/ scanning electron microscopy. Int Endod J 51:501–508
Duque JA, Vivan RR, Duarte MAH, Alcalde MP, Cruz VM, Borges MMB, Bramante CM (2019) Effect of larger apical size on the quality of preparation in curved canals using reciprocating instruments with different heat thermal treatments. Int Endod J 52:1652–1659
Saini HR, Tewari S, Sangwan P, Duhan J, Gupta A (2012) Effect of different apical preparation sizes on outcome of primary endodontic treatment: a randomized controlled trial. J Endod 38:1309–1315
De-Deus G, Belladonna FG, Souza EM et al (2015) Microcomputed tomographic assessment on the effect of ProTaper next and twisted file adaptive systems on dentinal cracks. J Endod 41:1116–1119
Oliveira LRS, Braga SSL, Bicalho AA, Ribeiro MTH, Price RB, Soares CJ (2018) Molar cusp deformation evaluated by micro-CT and enamel crack formation to compare incremental and bulk-filling techniques. J Dent. 74:71–78
Jamleh A, Mansour A, Taqi D, Moussa H, Tamimi F (2020) Microcomputed tomography assessment of microcracks following temporary filling placement. Clin Oral Investig. 24:1387–1393
Jamleh A, Adorno CG, Ebihara A, Suda H (2016) Effect of nickel titanium file design on the root surface strain and apical microcracks. Aust Endod J 42:25–31
Arola D, Reprogel RK (2005) Effects of aging on the mechanical behavior of human dentin. Biomaterials 26:4051–4061
Kim H, Lee M, Yum J et al (2010) Potential relationship between design of nickel-titanium rotary instruments and vertical root fracture. J Endod 36:1195–1199
Huang CC, Chang YC, Chuang MC, Lin HJ, Tsai YL, Chang SH, Chen JC, Jeng JH (2014) Analysis of the width of vertical root fracture in endodontically treated teeth by 2 micro-computed tomography systems. J Endod 40:698–702
Bürklein S, Tsotsis P, Schäfer E (2013) Incidence of dentinal defects after root canal preparation: reciprocating versus rotary instrumentation. J Endod 39:501–504
Arslan H, Karataş E, Çapar ID, Ozsu D, Doganay E (2014) Effect of ProTaper Universal, Endoflare, Revo-S, HyFlex coronal flaring instruments, and Gates Glidden drills on crack formation. J Endod 40:1681–1683
Shemesh H, Lindtner T, Portoles CA, Zaslansky P (2018) Dehydration induces cracking in root dentin irrespective of instrumentation: a two-dimensional and three-dimensional study. J Endod 44:120–125
Lim H, Li FC, Friedman S, Kishen A (2016) Residual microstrain in root dentin after canal instrumentation measured with digital moire interferometry. J Endod 42:1397–1402
Kishen A, Rafique A (2006) Investigations on the dynamics of water in the macrostructural dentine. Biomed Res Int 11:054018
Hill MR, Panontin TL (1999) Effect of residual stress on brittle fracture testing. In: Panontin TL, Sheppard SD (eds) Fatigue and Fracture Mechanics. West Conshohocken, PA, ASTM International
Sprawls P (1995) Physical principles of medical imaging. Medical Physics Publishing, Madison, WI
PradeepKumar AR, Shemesh H, Chang JW et al (2017) Preexisting dentinal microcracks in nonendodontically treated teeth: an ex vivo micro-computed tomographic analysis. J Endod 43:896–900
Funding
This work was supported by a research grant (RC15/027/R) from King Abdullah International Medical Research Centre, National Guard Health Affairs, Riyadh, Kingdom of Saudi Arabia.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors
Informed consent
For this type of study, formal consent is not required
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jamleh, A., Nassar, M., Alfadley, A. et al. Influence of additional apical enlargement on microcrack formation in root dentine: a micro-computed tomography investigation. Clin Oral Invest 25, 4137–4143 (2021). https://doi.org/10.1007/s00784-020-03745-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-020-03745-z