
Abstract
Objectives
The objective of the study was to determine the erosive tooth wear (ETW) status of institutionalized patients for alcohol misuse rehabilitation therapy in the north of Portugal.
Material and methods
Descriptive, analytical, and cross-sectional study, conducted on 277 individuals (83.4 % men) with an average age of 43.6 ± 8.4 years, institutionalized at Instituto da Droga e Toxicodependência–Delegação Regional Norte (IDT-Norte). ETW prevalence and severity were assessed by Eccles and Jenkins index. Multivariate logistic regression was used to identify ETW risk factors. Subjects with ETW risk identification according to biological and behavioral exposure were determined in the study.
Results
ETW prevalence was 98.6 %. In the cohort, 51.3 % showed localized ETW lesions, 40.1 % generalized ETW lesions, and 7.2 % enamel ETW lesions, more frequently localized in maxilla. From the examined dental surfaces (n = 15,598), 11,493 had erosive wear lesions: 92.4 % (95 % CI 91.7–93.1 %) of all occlusal surfaces, 71.9 % (95 % CI 70.7–73.1 %) of all palatal/lingual, and 56.7 % (95 % CI 55.4–58.1 %) of all buccal surfaces. Buccal and lingual surfaces showed 43.2 and 41.8 % enamel erosive wear lesions; occlusal surfaces had 43.4 % localized erosive wear lesions in dentin. The main ETW risk factors were as follows: age, gastroesophageal reflux disease over 1 year, daily intake of alcohol ≥240 g (grams), and intra-oral location in anterior region; 46.2 % of the participants had erosive risk by exposure to biological and behavioral factors.
Conclusions
The ETW status showed high values for disease prevalence and severity, mainly located in the maxilla, and high frequency of erosive wear lesions at occlusal, buccal, and lingual surfaces, resulting from simultaneous exposure to several risk factors.
Clinical implications
For ETW differential diagnosis, the association of both clinical and biological/nutritional/behavioral risk factors should be done for each studied population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Erosive tooth wear (ETW) is defined as a chemical-mechanical process resulting in a cumulative loss of hard dental tissue caused by extrinsic and intrinsic acidic sources without bacterial involvement [1]. This is a phenomenon that hardly occurs in an isolated form, but in a synergistical, sequential, and additive way with other types of tooth wear, such us attrition or abrasion. Differential diagnosis of erosive wear is complex, since the association between defect morphology and the respective etiological factors has not been validly established. Clinical signs of erosive wear can vary from loss of surface luster to changes in tooth morphology, such us cupping and grooving on surfaces, depending on the stage of the erosive process. The interplay between patient (biological and behavioral) and nutritional factors determines the onset and severity of erosive wear explaining why individuals exposed to the same risk factors exhibit more tooth wear than others [2, 3].
For a better perception of the erosive wear occurrence, it is of the utmost importance to study populations that, through specific characteristics and exposure to several risk factors, may present aggressive forms of erosive wear [4]. Individuals with alcohol abusive behavior or alcohol misuse are considered risk populations for ETW. This can be explained by the simultaneous exposure to intrinsic etiological factors (gastroesophageal reflux (GER) and persistent vomiting), as well as extrinsic sources (depending on the type and frequency of alcoholic consumption). The alcoholic drink’s erosive potential results from its low pH (i.e., wine pH—from 2.9 to 5.1) and its low content on calcium (Ca2+) and phosphate (PO4 3−) ions [5]. Besides that, it causes gastric irritation and can reduce the lower esophageal sphincter tone, precipitating gastroesophageal reflux and allowing a direct contact between acid and tooth structure [6]. The prevalence of alcohol use disorders in general population worldwide is estimated in 1.7 % [7]. In Portugal, on a study published in 2012 using the AUDIT (Alcohol Disorders Identification Test), about 3 % of general population (between 15 and 65 years old) was screened with abusive alcohol consumption, and 0.3 % had alcohol dependence [8].
The association between chronic alcoholism and ETW is not well established in literature, given the few studies published with this group population, and with results hard to compare, since they use different diagnostic indices and several type of recording (individual, tooth, or surface based) [9].
Therefore, the aim of this study was to determine ETW status on institutionalized alcoholic patients, under rehabilitation therapy, in the north region of Portugal, through evaluation of prevalence, severity, and ETW-associated risk factors. It was also aimed to quantify the frequency of individuals with an assessed risk, therefore exposed, to ETW by biological and behavioral factors.
This study was necessary to describe the oral features of this specific population in regard of ETW, since there are few studies on this matter.
Material and methods
This descriptive, cross-sectional observational study was designed, analyzed, and interpreted according to the STROBE statement.
Sample
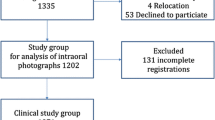
The sample was composed of 300 institutionalized patients for alcohol misuse rehabilitation therapies, between April of 2011 and July of 2012, in the Matosinhos Unit of the Instituto da Droga e Toxicodependência–Delegação Regional do Norte (Institute for Drugs and Drug Addiction—Northern Regional Delegation) (IDT-Norte), from Portugal. The local unit selection for conducting the study was done, based on epidemiologic national data concerning the number of individuals accessing drugs detoxification/rehabilitation (alcohol and other substances) programs at the IDT, in Portugal, in the year of 2009. The highest percentage (38.9 %) of individuals on treatment for drugs addictions was linked to functional units from IDT-Norte of Portugal. This way, the north region of Portugal proved to be the most prevalent geographical area as far as treatment for alcohol abusive consumption and other addictive substance addictions are concerned. The existence of physical and/or psychological conditions of the attendees, in a voluntary and informed way of consent to participate in the study, was defined as inclusion criteria. We considered as exclusion criteria all subjects with physical and/or psychological incompatibilities, and excluded from our evaluation all the surfaces with extensive tooth decay lesions, with calculus and with all the surfaces restored, which enabled their clinical examination.
Sample size (300 individuals) calculation was based upon national dimension, estimated to be approximately 2264 individuals on alcoholic misuse detoxification/rehabilitation therapy in the year 2009 and in an estimate situation of 50 % population prevalence concerning dental erosion, with a confidence interval range for the population prevalence estimate of ±5 % (accuracy) and a degree of confidence of 95 %. Considering the annual (2009 year) population, about 2500 users on treatment for alcohol misuse, the sample size should reach 334 individuals; the expected erosion prevalence in alcoholic subjects being different from 50 %, and based upon literature values, maintaining the confidence interval range for population prevalence estimate of ±5 % (95 % degree of confidence), it was then defined that a sample size of 300 individuals would allow inferring erosion prevalence within the alcoholic population on treatment in Portugal with a maximum precision of 10 % (±5 %). The sampling method was not probabilistic. This study was previously approved by the Ethics Committee of the University Fernando Pessoa (UFP) and complied with the ethical standards and recommendations laid down in the 1964 Declaration of Helsinki and its later amendments.
Survey and clinical examination
The study was performed according to good clinical practices, and a written informed consent was obtained from all participants, before entering the study, 1 week after patient’s institutionalization in IDT-Norte for alcohol misuse rehabilitation therapy.
For data collection purposes (April 2011 to July 2012), a structured self-filled questionnaire was designed to gather detailed information on social-demographic characteristics and behavioral and oral hygiene habits, and a face-to-face questionnaire was done to gather the medical history (Table 1). We consulted also the medical history done by the physician that admitted the patient into IDT-Norte, to gather information on the patient’s pathologies and the medication prescribed. A single observer at the UFP-mobile unit, with dental equipment and good lighting conditions, carried out all the clinical observations. Before the survey began, an intra-examiner calibration was done, by repeating the clinical examination of 10 patients and fulfilling the questionnaire, with 1-week interval, showing a Cohen-Kappa coefficient of at least 0.85.
From the 300 institutionalized patients, 23 were excluded (19 were edentulous and four had all tooth surfaces with extensive decay lesions or presence of calculus), in order to meet the examination conditions of ETW by Eccles and Jenkins (EJ) index criteria [10]; a cohort of 277 individuals was constituted for this study. The occlusal/incisal, buccal, and lingual/palatal surfaces of all teeth present in the oral cavity were observed with EJ index with the following criteria: (0) sound surface, without erosive wear lesions; (1) superficial lesion, involving enamel only (enamel erosive wear lesions); (2) localized erosive wear lesion, <1/3 of dentin surface; and (3) generalized erosive wear lesion, >1/3 of dentin surface.
For ETW status assessment, both prevalence and severity of erosive wear were evaluated in the cohort, and also the distribution (frequency and severity) of erosive wear lesions by dental surfaces examined (n = 15,598), according to its intra-oral location (maxilla, mandible, anterior, and posterior regions of oral cavity) considering the EJ index higher score clinically registered. A multivariate regression analysis (dental surface as unit) was done to identify risk and protective factors and to identify surfaces with ETW risk in this cohort.
The identification of individuals with risk for ETW was calculated (the frequency (n) of individuals) through the simultaneous combination of erosive wear (1, 2, or 3 scores from EJ index) and one primary risk criteria (biological or nutritional criteria) and also with two secondary risk factors (behavioral criteria). The distinction between primary and secondary risk factors was done based on epidemiological data and their presumed impact on ETW, according to EVIDE description [11].
Statistical analysis
The statistical analysis was done using IBM® SPSS® Statistics vs. 22.0, considering a significance level of 0.05 for all statistic inference situations. The comparison of mean values for two independent groups was done with the t test and for prevalence with the chi-square test. The 95 % confidence intervals for erosive wear prevalence were calculated by the adjusted Wald method. The identification of risk or protective factors, associated with erosive wear was evaluated through odds ratio (OR). The initial identification was done through bivariate analysis (simple logistic regression), and subsequently adjusted regarding age group and gender. Afterwards, a multivariate analysis of the factors independently associated with ETW was done, using multiple logistic regression, through the Wald regressive method, considering p = 0.05 for inclusion and p = 0.10 for factor exclusion. In the first stage, we included all variables, which showed a significant association with the considered outcome in the bivariate analysis, as well as those that, without being statistically associated, showed a p value up to 0.20.
Results
Of the 277 participants, 83.4 % were male and 16.6 % were female (Table 1). The average age was 43.6 ± 8.4 years (ranging from a minimum of 22 to a maximum of 72 years), without differences by gender (p = 0.751). This cohort presented a low educational level (88.4 % with schooling until the 9th grade) and a high percentage of professional inactivity, due to unemployment (26.7 %) or retirement (6.9 %). Alcohol consumption patterns showed a mean age of alcohol consumption onset at approximately 17.6 ± 8.3 years of age, an history of alcohol abuse, in average, for 20.9 ± 11.3 years, an average amount of pure alcohol ingested daily of 202.7 ± 121.1 g (grams), being significantly higher in men under 40 years (t test, p < 0.001, in both comparisons). Wine was the type of beverage users mentioned as being the most frequently ingested and in highest quantity. There was no difference between genders, concerning the type of alcohol beverage ingested, with the exception of white drinks/spirits, which men (chi-square test, p = 0.003) consumed in a significantly higher way. Approximately 27 % of the patients were diagnosed as having GERD, in average for 6.5 ± 7.8 years. Of the 277 participants, 38.6 % reported persistent vomiting, and these symptoms did not differ according to gender (chi-square test, p = 0.589).
Erosive tooth wear status
The prevalence of ETW in the cohort (n = 277) was 98.6 % (95 % CI 96.2–99.6 %). Analysis of erosive wear severity showed that 7.2 % (95 % CI 4.7 %–10.9 %) (n = 20) of the participants had superficial lesions, involving only the enamel (enamel erosive wear lesions); 51.3 % (n = 142) localized erosive wear lesions, <1/3 of dentin surface (95 % CI 45.4–57.1 %); and 40.1 % (n = 111) generalized erosive wear lesions, >1/3 of dentin surface (95 % CI 34.5–45.9 %) (Table 2).
Generalized erosive wear lesions affecting >1/3 of dentin surface were more prevalent (chi-square test, p < 0.001) in the maxilla (37.3 %) than in the mandible (23.4 %) when considered the clinical crowns location by dental arch. There was no difference (chi-square test, p > 0.05) between anterior and posterior region intra-oral location for ETW lesions’ in this cohort (Table 2).
From the examined dental surfaces in the cohort (n individuals = 277; n Surfaces = 15,598), 4105 surfaces were sound (without erosive wear lesions), but 11,493 (73.7 %) surfaces had erosive wear lesions (41.2 % registered enamel erosive wear lesions, 26.5 % were affected with localized erosive wear lesions (<1/3 of the dentin surface), and 6 % showed generalized erosive wear lesions, affecting >1/3 of dentin surface (Table 3)). From all the occlusal surfaces analyzed, 92.4 % (95 % CI 91.7–93.1 %) had erosive wear lesions, 71.9 % (95 % CI 70.7–73.1 %) of all the palatal/lingual surfaces had also erosive wear lesions, and 56.7 % (95 % CI 55.4–58.1 %) of all the buccal surfaces were detected as having erosive wear lesions. When we analyzed the erosion’s wear severity by surface, we realized that buccal and lingual surfaces had more frequently enamel erosive wear lesions (43.2 and 41.8 %, respectively) and occlusal surfaces had localized erosive wear lesions affecting <1/3 of dentin tissues (43.4 %).
Erosive tooth wear risk and protective factors: multivariate regression analysis by dental surface
Multivariate logistic regression analysis detected as risk factors for erosive wear at the occlusal surfaces (Table 4): age—individuals older than 40 years old (OR = 1.3), anterior region surfaces’ intra-oral location (OR = 2.5), abusive alcohol consumption for more than 10 years (OR = 1.6), drinking before going to bed (OR = 1.6), vomiting (OR = 1.5) and GERD over than one year (OR = 2.7). There were detected, as protective erosive wear factors, with an increase of 23 %, the mouthwash rinsing, as well as a 28 % increase through the daily alcohol ingestion equal or higher than 240 g (OR = 0.72).
Erosive wear risk factors at the buccal surfaces (Table 4) were as follows: the anterior region surfaces’ intra-oral location (OR = 1.4); age, individuals older than 40 years old (OR = 1.3); professional inactivity (OR = 1.3); the daily intake of alcohol doses equal or higher than 240 g (OR = 1.2); drinking on an empty stomach (OR = 1.3), GERD over than one year (OR = 2.3); and tooth brushing at least three times a day (OR = 1.2). Erosive wear protective factors were related with an increase in 42 % for drug abuse (OR = 0.58) and in 34 % for drinking before going to bed (OR = 0.66) and for vomiting (OR = 0.66).
At the palatal/lingual surfaces (Table 4), risk factors for erosive wear were as follows: the anterior region (OR = 3.3) and the maxilla (OR = 1.7) surfaces intra-oral location, having a higher level of education (OR = 1.4), daily ingestion of alcohol doses equal or higher than 240 g (OR = 1.4), drinking on an empty stomach (OR = 1.4), GERD over than 1 year (OR = 2.1), and rinsing with mouthwash (OR = 1.2). Drug use (increased protection in 29 % (OR = 0.71)), drinking before going to bed (OR = 0.64), vomiting (OR = 0.77), and tooth brushing (OR = 0.625 and 0.706) were registered as erosive wear protective factors on lingual/palatal surfaces.
The multivariate logistic regression model for occlusal/incisal, buccal, and lingual/palatal surfaces showed a sensitivity of 59.0, 74.5, and 59.2 %, respectively, and a specificity of 76.8, 46.8, and 72.4 %, respectively. It showed an area under the ROC curve of 70.1 % (95 % CI 67.6–72.6 %) for the occlusal/incisal, 64.1 % (95 % CI 62.6–65.7 %) for the buccal, and 70.2 % (95 % CI 68.6–71.7 %) for lingual/palatal surfaces.
Individuals with risk of erosive tooth wear in the cohort
From the 277 participants, 73 (26.4 %, 95 % CI 21.5–31.9 %) were identified with risk for ETW associated with a primary etiologic factor (biological—GERD) (Table 5); 71 (25.6 %, 95 % CI 20.6–31.2 %) subjects had ETW risk associated with two secondary risk criteria, (behavioral—alcohol abuse for more than 10 years and daily alcohol consumption ≥240 g). Sixteen subjects (5.8 %) were identified as being simultaneously exposed both to, one biological and two behavioral risk factors, under study; it was estimated that 128 subjects, meaning 46.2 % (95 % CI 40.4–52.1 %) of the cohort (n = 277), are the patients with an evaluated risk for ETW.
Discussion
Sample and cohort
The present study was conducted according to published national epidemiologic data (2009 year) on the number of subjects, which accessed to alcohol misuse detoxification/rehabilitations therapy at the IDT, in Portugal. A higher percentage of patients treating drug/alcohol addiction (38.9 %) were linked to organizational structures in the north region of Portugal, which had an impact on the selection decision regarding the local unit (Matosinhos) for patient’s examination, namely the IDT-Norte. As this sample of 300 institutionalized alcoholic patients under rehabilitation therapy was a convenient sample concerns regarding precision, representation and bias may raise.
In relation with the accuracy of ETW prevalence estimated in the population (from the sample), it was verified that the range of the confidence interval for this prevalence was of ±1.7 % (95 % CI for erosion prevalence 96.2–99.6 %), whereby the accuracy of the estimate was higher than the initially imposed. National epidemiologic data of the year 2013 [8], and assuming a uniform distribution by gender and age group in the years 2011 and 2012 (inherent to lack of national data), the sample from the present study was representative of the population for the year 2013, regarding gender (chi-square test, p = 0.265) but not age (Student’s t test, p < 0.001). We consider the outcomes of the present study as valuable information for developing ETW strategies for institutionalized alcohol misuse patients under rehabilitation therapies in the north region of the country.
Erosive tooth wear status, risk factors, and individuals with erosive wear risk on the cohort
ETW prevalence in present study was higher than the outputs of other trials in similar populations, with alcohol misuse or addiction; the variation stated between 23 % [12] and 92 % [13] may be due to design and methodology differences applied, namely evaluation indexes, sample sizes, social-demographic characteristics of the populations under study, and the assessed units (by individual, by tooth, and by dental surface) as erosive wear were concerned [14]. There were many indices developed in the past years, such us TWI (tooth wear index) [15], Lussi index [16], and a more recent scoring system, named BEWE (basic erosive wear system) [17]. In the present study, we used EJ index in order to allow data comparison between a pilot study done in 2009 by one of this study investigator (PM) in a similar alcoholic population [18] and with another study with a large sample of alcoholic patients that also used this index [12].
In the present study, severity analysis regarding the hard dental tissues affected by erosive wear lesions reveled that most of the cohort participants had localized erosive wear lesions affecting <1/3 of dentin tissues (51.3 %, 95 % CI 45.4–57.1 %) and generalized erosive wear lesions, >1/3 of dentin surface (40.1 %, 95 % CI 34.5–45.9 %); only 7.2 % (95 % CI 4.7–10.9 %) of the participants registered erosive wear lesions confined to the enamel.
Generalized erosive wear lesions affecting >1/3 of the dentin surface were more frequent in the maxilla than in the mandible, when considering the participants dental arch location. The preferred location of erosive wear lesions in dental surfaces located both in the anterior and maxilla region of the oral cavity and in the lingual/palatal surfaces suggests that the predominant etiological factor affecting the dental surfaces had an intrinsic origin. These findings are supported by other studies [11–13]. The higher frequency of ETW detected in the occlusal/incisal surfaces in the present findings might be due to the possible lack of specificity associated with the EJ index, including the detection of wear lesions for non-erosive reasons, as mechanical wear [19, 20]. To counteract that possibility and based on the EVIDE description, we crossed etiological factors with clinical data, in order to allow accuracy for ETW diagnosis.
In the multivariate logistic regression analysis, the participants’ age (at least of 40 years old) was detected as erosive wear risk factors at the occlusal/incisal surfaces. Considering erosive pathology as a cumulative process over time, one can expect age to be a risk factor for ETW. Participants’ age was equally identified as risk factor for ETW in a longitudinal study conducted by Lussi and Shaffner [21]; the subjects’ age and the intake of acidic food were responsible for 28 % of the cases of tooth erosion progression [21]. The results of Manarte et al. study revealed an increased risk of 1.52-fold of erosion only in occlusal surfaces for subjects with an alcoholism history, with 40 or more years of age (p = 0.008) [18]. According to other authors, the subject’s age (OR = 1.27, p = 0.003) was also a risk factor for dental hard tissues loss, as a cumulative effect of chemical-mechanical processes [22].
The relationship between the social-demographic variables of the cohort under study and the ETW risk showed that subjects with higher education levels presented a higher risk for hard tissues loss in the lingual surfaces. These findings were corroborated with outputs from other trials [18].
In the present study, participants exposed to alcohol abuse for more than 10 years showed a 1.6 higher risk of erosive wear in occlusal surfaces. According to Hede study [12], abusive alcohol consumption over 4 years corresponded to an OR of 0.42, when compared with the associated risk of abusive consumption for 15 years. Also, the results of Manarte et al. study indicated an increased risk of 1.59-fold for erosion lesions in occlusal surfaces when considered subjects with an abusive alcohol consumption over than 10 years [18].
The present findings revealed that the behavior of daily intake of alcohol amounts equal or higher than 240 g was a risk factor for erosive wear lesions located both in buccal and lingual/palatal surfaces. A higher amount of daily alcohol consumption may create condition for higher amounts of acidic intake, mainly in contact with palatal surfaces. These findings corroborate the results obtained by Harris et al. in their study, in which the ETW had shown to be positively associated (r = 0.41; p = 0.02) to the average number of consumed alcohol units per week [23]. Similar results were verified in another study, which identified an increased risk (OR = 1.62) for erosion in the palatal surfaces, associated with standard amount of alcohol units consumed [18].
In this cohort, a higher risk for ETW was detected in the occlusal surfaces of participants who reported vomiting and in all the dental surfaces (occlusal, buccal, lingual/palatal) of subjects with GERD over than 1 year. Some studies stated the erosive risk in subjects with pathology inducing GER: a higher risk (3.37) of dental erosion in subjects with frequent vomiting episode [24], erosion increased risk in all dental surfaces (OR = 2.15 for the occlusal surface, 2.84 for the palatal surface and 2.91 for the buccal surface) in individuals with GER [18], and the presence of symptoms associated with GER and to frequent vomiting showed a significant relationship with tooth erosion [25]. However, recent findings from the Margaritis et al. study revealed the absence of a significant relationship between the presence of GER and tooth erosion in the population studied [26]. An explanation for this fact may be due to the action of other risk factors associated with the time period of GERD and GERD symptoms in the studied populations [26].
In the present study, subjects who brushed their teeth, at least, three times a day, registered an increased erosive wear risk in buccal surfaces comparatively with those participants who mentioned that they did not brush their teeth at all or brushing less frequently. This result can be justified by the tooth erosive wear multifactorial etiology, potentiated by the association of other possible etiologic mechanisms. The “use of mouthwash” was identified as a protective factor for erosive wear in the occlusal surfaces; however, it proved to be a risk factor for erosive wear lesions in the lingual surfaces. The supply of high amounts of fluoride to the mineral structure trough mouthwashes may allow a mineral structure reinforcement preventing dental hard tissues loss due to chemical process [27–31]. On the other hand, some mouthwashes may exhibit acidic pH values, which may predispose to tissues demineralization and erosive wear lesions [32]. This conflicting result might be explained by the interplay of different risk factors, which determine different effects, such us differences on salivary composition, flow rate, or buffer capacity that, when contacting with some mouth rinses, may predispose for lingual surfaces erosive wear or simply because occlusal surfaces might have a longer contact with fluoride compounds, which enhances acid resistance. In the present study, we did not evaluate the type of mouth rinses used by this population, not even the salivary flow rate and buffer capacity, and those factors may interfere on surface erosive wear. In clinical practice, there are different agents with a prophylactic/therapeutic action, several concentrations, and ways of delivering available for professional and/or population use. Some of them are experimentally tested mostly in vitro and in situ trials. The mechanism of action of these agents and all the factors that might interfere with their efficacy are not completely understood, and that might be reflected also on these results. In a clinical level, it is also relevant to evaluate the salivary flow and buffer capacity when using some mouth rinses, especially in some populations that may have some compromised systemic/oral alterations, such us alcoholic patients. More studies should be done to evaluate the effect of mouth rinses use and its effects according to salivary composition, rate, and flow/buffer capacity in some specific populations.
Despite the multivariate logistic regression model had shown a feeble discriminative power in relation to the predictive capacity concerning ETW, it made possible the identification of several risk factors that can characterize this specific population. The identification of suitable populations in which to conduct clinical studies on ETW is difficult, and the conclusions that can be drawn from them are limited. Our purpose was to evaluate a population that is exposed to several sources of acid and with an expected higher risk of ETW. Some of the conflicting results of the multivariate regression analysis are due to the self-report information (i.e., vomiting as a protective factor). The variables whose data were confirmed by medical report or by other persons’ report (i.e., patients’ family) did not show conflicting results. Another reason might be the inclusion of non-erosive lesions into an erosive index, and in order to reduce the risk of that, we adapted the principles and the criteria of EVIDE index and crossed etiological criteria (biological, nutritional, and behavioral), with clinical data obtained with EJ index [11]. This allowed a more accurate ETW assessment, in order to exclude dental hard tissues loss by non-erosive reasons. In the cohort under study, prevalence of ETW was 98.6 %, based on the EJ index. However, after its association with risk factors as biological (GERD over than one year) and behavioral (alcohol abuse for more than 10 years and daily alcohol consumption ≥240 g) criteria determined in this cohort, only 46.2 % of the subjects were identified as patients with evaluated risk for ETW; this prevalence value can be a numerical representative basis of the exclusive consequences of erosive pathology in the cohort under study, as the association of clinical criteria and other risk factors identified in the logistic regression analysis could assess this identification. The selection of the risk factors as GERD over 1 year (biological factor) and alcohol consumption behaviors (alcohol abuse over 10 years and daily consumption ≥240 g) was made in order to analyze ETW status that is the effect of chemical process in dental hard tissues loss, in this population with the specific features described. A population is considered at risk of ETW when through the assessment of the behavioral, biological, and environmental factor analysis to which that population is exposed, a causal relationship can be established between factors/variables and ETW prevalence/severity.
Conclusions
In this cohort of institutionalized alcoholic patients for rehabilitation therapies in the North region of Portugal, the ETW status revealed high levels of disease prevalence and severity. The erosive wear lesions were preferentially detected in dental surfaces located on maxilla dental arch and in lingual/palatal surfaces, suggesting an erosive source effect caused by endogenous origin. This tendency is corroborated by the risk and protective factors of erosion tooth wear analysis. The simultaneous association of erosive wear clinical data with one biological and two behavioral risk factors, previously identified in the studied cohort, acted as a weighting factor on the differential diagnosis, enabling the clarification of clinically detected values, and in some way value the identification of subjects with wear lesions associated to a chemical process, over those of non-erosive origin (mechanical process). The presented data are specific to the population under study and should not be extrapolated to groups or populations with social-demographic characteristics, behavioral and oral hygiene habits, and a medical history (biological characteristics) distinct from those described. Further studies are needed in order to validate the association method, between the risk factors identified for a specific population and the measuring instruments capable of enhancing the ETW indexes’ and approaches specificity.
References
Carvalho TS, Colon P, Ganss C, Huysmans MC, et al. (2015) Consensus report of the European Federation of Conservative Dentistry: erosive tooth wear—diagnosis and management. Clin Oral Investig 19:1557–1561
Ganss C, Lussi A (2014) Diagnosis of erosive tooth wear. Erosive Tooth Wear. Monogr Oral Sci. Karger, Basel, pp. 22–31
Shellis RP, Addy M (2014) The interactions between attrition, abrasion and erosion in tooth wear. Erosive Tooth Wear. Monogr Oral Sci. Karger, Basel, pp. 32–45
Huysmans MC, Chew HP, Ellwood RP (2011) Clinical studies of dental erosion and erosive wear. Caries Res 45(Suppl 1):60–68
Mandel L (2005) Dental erosion due to wine consumption. J Am Dent Assoc 136:71–75
Moazzez R, Bartlett D (2014) Intrinsic causes of erosion. In: Lussi A, Ganss C (eds) Erosive tooth wear. Monogr Oral Sci. Karger, Basel, pp. 180–196
WHO (2004) http://www.who.int/substance_abuse/publications/global_status_report_2004_overview.pdf?ua=1 Accessed in May 2014
Sicad (2014) Relatório Anual de 2013—a situação do país em matéria de álcool http://www.sicad.pt. Accessed April 2014
Schlueter N, Tveit AB (2014) Prevalence of erosive tooth wear in risk groups. Erosive Tooth Wear. Monogr Oral Sci. Karger, Basel, pp. 74–98
Eccles JD (1979) Dental erosion of nonindustrial origin: a clinical survey and classification. J Prosthet Dent 42:649–653
Margaritis V, Mamai-Homata E, Koletsi-Kounari H, Polychronopoulou A (2011) Evaluation of three different scoring systems for dental erosion: a comparative study in adolescents. J Dent 39:88–93
Hede B (1996) Determinants of oral health in a group of Danish alcoholics. Eur J Oral Sci 104:403–408
Robb ND, Smith BG (1990) Prevalence of pathological tooth wear in patients with chronic alcoholism. Br Dent J 169:367–369
Salas MM, Nascimento GG, Huysmans MC, Demarco FF (2015) Estimated prevalence of erosive tooth wear in permanent teeth of children and adolescents: an epidemiological systematic review and meta-regression analysis. J Dent 43:42–50
Smith BGN, Knight JK (1984) An index for measuring the wear of teeth. Br Dent J 157:16–19
Lussi A (1996) Dental erosion: clinical diagnosis and case history taking. Eur JOral Sci 104:191–198
Bartlett D, Ganss C, Lussi A (2008) Basic erosive wear examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig 12(Suppl 1):S65–S68
Manarte P, Manso MC, Souza D, Frias-Bulhosa J, Gago S (2009) Dental erosion in alcoholic patients under addiction rehabilitation therapy. Med Oral Patol Oral Cir Bucal 14:376–383
Moazzez R, Bartlett D, Anggiansah A (2004) Dental erosion, gastro-oesophageal reflux disease and saliva: how are they related? J Dent 32:489–494
Tantbirojn D, Pintado MR, Versluis A, Dunn C, Delong R (2012) Quantitative analysis of tooth surface loss associated with gastroesophageal reflux disease: a longitudinal clinical study. J Am Dent Assoc 143:278–285
Lussi A, Schaffner M (2000) Progression of and risk factors for dental erosion and wedge-shaped defects over a 6-year period. Caries Res 34:182–187
Bartlett DW, Lussi A, West NX, Bouchard P, Sanz M, Bourgeois D (2013) Prevalence of tooth wear on buccal and lingual surfaces and possible risk factors in young European adults. J Dent 41:1007–1013
Harris C, Warnakulasuriya KS, Gelbier NW, Johnson NW, Peters TJ (1997) Oral and dental health in alcohol misusing patients. Alcohol Clin Exp Res 21:1707–1709
Hamasha AA, Zawaideh FI, Al-Hadithy RT (2014) Risk indicators associated with dental erosion among Jordanian school children aged 12–14 years of age. Int J Paediatr Dent 24:56–68
Zebrauskas A, Birskute R, Maciulskiene V (2014) Prevalence of dental erosion among the young regular swimmers in Kaunas, Lithuania. J Oral Maxillofac Res 5:1–6
Margaritis V, Mamai-Homata E, Koletsi-Kounari H (2011) Novel methods of balancing covariates for the assessment of dental erosion: a contribution to validation of a synthetic scoring system for erosive wear. J Dent 39:361–367
Young A, Thrane PS, Saxegaard E, Jonski G, Rolla G (2006) Effect of stannous fluoride toothpaste on erosion-like lesions: an in vivo study. Eur J Oral Sci 114:180–183
Sauro S, Mannocci F, Piemontese M, Mongiorgi R (2008) In situ enamel morphology evaluation after acidic soft drink consumption: protection factor of contemporary toothpaste. Int J Dent Hyg 6:188–192
Brand HS, Tjoe Fat GM, Veerman EC (2009) The effects of saliva on the erosive potential of three different wines. Aust Dent J 54:228–232
Hjortsjo C, Jonski G, Thrane PS, Saxegaard E, Young A (2009) The effects of acidic fluoride solutions on early enamel erosion in vivo. Caries Res 43:126–131
Ganss C, Schlueter N, Hardt M, Schattenberg P, Klimek J (2008) Effect of fluoride compounds on enamel erosion in vitro: a comparison of amine, sodium and stannous fluoride. Caries Res 42:2–7
Pontefract H, Hughes J, Kemp K, Yates R, Newcombe RG, Addy M (2001) The erosive effects of some mouthrinses on enamel: a study in situ. J Clin Periodontol 28:319–324
Acknowledgments
The authors are grateful to the Instituto da Droga e Toxicodependência–Delegação Regional do Norte (IDT-Norte), Porto, Portugal, and to all the participants for their cooperation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in this study involving the participants, were in accordance with the ethical standards and with the 1964 Helsinki Declaration and its later amendments. This was formally approved, monitored, and reviewed by the University Fernando Pessoa Ethical Committee.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article. The authors also state that have full control of all primary data and that agreed to allow the journal to review the data if requested.
Funding
The authors received no financial support.
Informed consent
After explaining to all individual the risks involved on this survey, the written informed consent was obtained from all participants included in the study.
Rights and permissions
About this article

Cite this article
Teixeira, L., Manso, MC. & Manarte-Monteiro, P. Erosive tooth wear status of institutionalized alcoholic patients under rehabilitation therapy in the north of Portugal. Clin Oral Invest 21, 809–819 (2017). https://doi.org/10.1007/s00784-016-1823-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-016-1823-2