
Abstract
This in vitro study evaluated the influence of one halogen and two light-emitting diode (LED) curing units on the curing depth of a conventional hybrid and two translucent resin composites by measuring the Knoop microhardness. In the first part of the study, a conventional hybrid resin composite and three curing units (one halogen: 40 s polymerization time, two LEDs: 10 and 20 s) were used. Ten cylindrical resin composite samples were prepared for each curing unit and each polymerization time tested. After polymerization, the soft part of the samples was removed. The samples were embedded in a polyacrylic resin and separated in the middle towards the direction, top–bottom. On the section plane, Knoop microhardness measurements were performed every 1 mm, starting at 0.5 mm under the surface. In the second part of the study, two translucent resin composites and a conventional hybrid composite resin were cured with the three curing units, and the microhardness was measured as mentioned above. The difference between the curing units tested was found statistically significant (p = 0.0009), as well as the difference between the materials concerning curing depth (p = 0.0001). Both translucent materials achieved microhardness values equal to the 80% of the surface values, in depths 3.5–5.5 mm, depending on the curing units used.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The degree of the conversion affects the physical properties and the clinical performance of the resin composite materials [4, 20, 30]; therefore, it plays an important role in determining the ultimate success of the restoration [6, 29]. It is known that the degree of conversion of the composite resins ranges between 55 and 73% [21]. With high-molecular-weight monomers such as BisGMA or urethane dimethacrylate (UDMA), there is always an incomplete polymerization and significant concentration of unreacted C=C remaining within the resin, when it is cured with visible light at the oral temperature. In addition to the unreacted monomer, additional unreacted (C=C) structures may be present, from diluents such as TEGDMA. The incomplete polymerization is believed to be mainly because of the limitations on the mobility of molecules imposed by the rapid formation of a cross-linked polymeric network [4].
In general, total energy—the product of light intensity and exposure time—determines the mechanical properties of the resin composites. As light passes through the material, it is absorbed and scattered, attenuating the intensity and reducing the effectiveness of the light for resin polymerization [12, 26]. If the amount of light reaching the resin composite is reduced, the depth of cure could be decreased. Depth of cure for the visible-light-cured composite resins is a function of the filler size and composition, shade and translucency of the material, the intensity of the light source, and the length of irradiation exposure as well as monomer composition and the polymerization initiators concentration [12].
Halogen curing units are routinely used as curing units for the resin composites. However, the fact that they generate high operating temperature, large quantity of heat, and have a limited effective lifetime of 100 h results in a reduction in their curing efficacy over time, insufficient physical properties, and an increased risk of premature failure of restoration [5, 8–16]. Therefore, in the past years, to overcome the problems of the halogen light curing unit (LCU), the use of light-emitting diode (LED) technology has been proposed for the curing of the resin composites [10, 12]. The LED LCUs have shown to have an effective lifetime of 10,000 h and not to require the use of filters to produce blue light [23].
The surface hardness of dental composites is often used to measure the curing ability of LCUs [5–17] and the depth of cure of resin composites [19]. The surface hardness of resin composites correlates with the degree of monomer conversion [6] and is therefore used as an indirect measurement of curing depth in the present study. Knoop hardness measurement is one of the several suitable methods available for the determination of the surface hardness. The depth at which a resin composite achieves the 80% of its maximum hardness was used in several studies [4, 28] to represent the depth at which a resin composite can be used, having a satisfying hardness. This criterion was used in the present study.
In the past years, a great number of LED curing units have been introduced in the market recommending a sufficient polymerization in a curing time less than 40 s. Additionally, several translucent materials are fabricated, and they are proposed to be used in layers thicker than 2.5 mm, after polymerized once.
The aims of this study were to examine the following hypothesis: (a) that the two LED curing units can have a better curing performance than a halogen after evaluating the curing depth of a conventional hybrid composite resin (in two different shades), using the Knoop hardness test and (b) that the two translucent resin composites can be cured in layers thicker than 2.5 mm, comparing them with a traditional hybrid resin composite after using three different curing units.
Materials and methods
Characterization of the curing units
Two LED and one halogen curing units were used in the present study. The LED curing units Smartlite PS (Dentsply DeTrey, Konstanz, Germany) and Ultralume 5 (Ultradent, USA) were used for 10 and 20 s exposure time. Smartlite PS had a wavelength range of 450–490 nm and a power density of 950 mW/cm2. Ultralume 5 had a wavelength range of 370–500 nm and a power density of 1,063 mW/cm2. The halogen curing unit was the Elipar Highlight (3M ESPE, Germany), used with 40 s exposure time, with the soft start mode. It had a power density of 150 mW/cm2 for the first 20 s and a maximum power density of 780–800 mW/cm2 for 20–40 s. The spectral power density of the curing lights was determined with a visible curing light meter, the Cure Rite (Dentsply, USA). The wavelength ranges of the LED LCUs mentioned were given by the manufacturers.
Resin composites
Three light-cured hybrid resin composites were used in this in vitro study, Tetric Ceram®, in shades A2 and A3 and two translucent resin composites, Adamant® and QuixFil™. These two translucent resin composites are recommended by the manufacturers for use in increments thicker than 2.5 mm. The list of the materials, their composition, the batch numbers, and the manufacturers are given in Table 1.
Construction of the samples
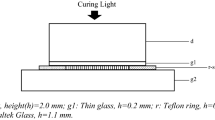
The samples were prepared using forms, given by Dentsply DeTrey GmbH, which allowed the production of standardized cylindrical specimens with 8-mm thickness and 4-mm diameter. A nontranslucent paper (3M ESPE, Seefeld, Germany) was used as an underground. The resin composites were placed into the forms using a composite instrument. A translucent plastic matrix strip (Kerr Hawe, Switzerland) was put over them before curing to avoid the oxygen-inhibited superficial layer with lower hardness. On top of the matrix, a glass slide was placed to straighten the surface. Every sample was then cured only once, for 10, 20, and 40 s, respectively. After curing, the unpolymerized soft part at the bottom of the samples was removed with a scalpel, and the rest was stored in distilled water, at room temperature for 24 h. After that, each sample was embedded in a polyacrylic resin (Technovit, Kulzer, Germany), and then it was separated under running water in the middle towards the direction, top–bottom. On the section plane, Knoop microhardness measurements were made every 1 mm, starting 0.5 mm under the surface up to 7.5 mm, if possible, using 0.5 N load.
For the first part of the study, four groups of Tetric Ceram® (ten samples each) were prepared with each LED LCU, one group with shade A2 and one group with shade A3, for each exposure time tested, 10 and 20 s. For the halogen LCU, two groups were prepared: one with shadeA2 and one with shade A3, both exposed for 40 s.
For the second part of the study, five additional groups (with ten samples each) were prepared of each translucent composite materials, cured with each of the three LCUs. The exposure times used were the same with the first part of the study.
The hardness values (in percent) at all depths (0.5–7.5 mm) and for all groups compared to the surface hardness are given in Figs 1, 2, and 3. For the LED LCUs, the 20 s were selected as exposure time, as recommended by the manufacturers, to be compared with the recommended 40 s of the halogen curing unit. For the Tetric Ceram®, the shade A2 was selected to be compared with the two translucent materials at the second part of the study.

Tetric Ceram®: Knoop hardness in percent of the surface hardness in each depth and for each group (LED 1: Smartlite PS, LED 2: Ultralume 5)

Adamant®: Knoop hardness in percent of the surface hardness in each depth and for each group (LED 1: Smartlite PS, LED 2: Ultralume 5)

QuiXfil: Knoop hardness in percent of the surface hardness in each depth and for each group (LED 1: Smartlite PS, LED 2: Ultralume 5)
Results
For the statistical analysis of the data, the repeated measures analysis of variance with up to three between factors and one within (depth) was used. Because of the fact that the data were not normally distributed, the logarithms of the values were used for the statistical analysis. According to the correlation analysis evaluating the relationship between the mean values and the standard deviations, it was shown that the log-transformed data were normally distributed (p = 0.1347).
In the first part of the study, the microhardness measurements for Tetric Ceram® could be performed up to a depth of 3.5 mm. Under this depth, the resin composite is so soft that it could be removed with a scalpel. Almost in all of the cases, the 80% of the surface hardness was achieved at the depth of 2.5 mm. Only the exposure to Smartlite PS for 10 s was shown to have controversial results, as shown in Fig. 1. However, at the depth of 2.5 mm, curing with the halogen resulted in higher microhardness values compared to the LED LCUs. This difference was statistically significant, but not in any case (Table 2).
According to the general linear models procedure, Ultralume 5 produced statistically significant higher microhardness values than the Smartlite PS, for the 10 s exposure time (p = 0.03). There was no significant difference between the two LED LCUs, for the 20 s exposure time.
Between the three curing units tested (halogen, t = 40 s, and LED, t = 20 s), there were found statistically significant differences (p = 0.0009), for the shades A2 and A3. These differences are shown in Table 2, where the results of the Tukey’s studentized range test for both shades are given. According to the Tukey’s test, for the shade A2, halogen produced statistically significant higher microhardness values (p ≤ 0.05) compared to the two LED units at 0.5 and 2.5 mm. For this shade, at 1.5 mm, no significant difference was found between the three curing units (p > 0.05). The same test showed, for the shade A3, no significant difference between the halogen and Smartlite PS (p > 0.05), while halogen was found to produce significantly higher microhardness values (p ≤ 0.05) compared to Ultralume 5. Between the two LED LCUs, for this shade, Smartlite PS was significantly better (p ≤ 0.05) than Ultralume 5 at 0.5 and 1.5 mm, while at 2.5 mm, no significant difference was found between them (p > 0.05).
In the second part of the study where the curing depth of the transparent materials Adamant® and QuiXfil was compared to that of Tetric Ceram®, the three resin composites were found to differ significantly (p = 0.0001). According to the statistical analysis, Adamant reached the 80% of the surface microhardness at a depth of 3.5 mm when it was cured with the halogen or the Smartlite PS. Curing with Ultralume 5 resulted in a depth of cure up to 4.5 mm. For QuiXfil, the 80% of the surface hardness was reached at a depth of 4.5 mm when the material was cured with the halogen LCU. Similar results were given by Ultralume 5. As shown in Fig. 3, curing with Smartlite PS could transfer the satisfying limit of the 80% to 5.5mm. Between the three tested LCUs, QuiXfil, Ultralume 5 (10 and 20 s), and the 20 s of Smartlite PS resulted in higher hardness values compared to Halogen and the 10 s of Smartlite PS.
Tukey’s studentized range test (p ≤ 0.05) for the three restorative materials (Table 3), and the three LCUs (LEDs, t = 20 s, and halogen, t = 40 s), showed the following concerning microhardness:
-
(a)
For the halogen curing unit, no significant difference (p > 0.05) was found between the three resin composites.
-
(b)
For Smartlite PS, no significant difference was found between Tetric Ceram® and Adamant®. QuiXfil polymerized with Smartlite PS produced significantly higher microhardness values compared to Tetric Ceram®. No significant difference was found between Adamant® and QuiXfil for the depths 0.5, 1.5, and 3.5 mm, after polymerization with Smartlite PS.
-
(c)
For Ultralume 5, no significant difference was found between Tetric Ceram® and Adamant®. QuiXfil polymerization with Ultralume 5 produced significantly higher microhardness values compared to Tetric Ceram®, for the depths 1.5–3.5 mm. No significant difference was found between QuiXfil and Adamant® at the depths 1.5, 2.5, and 3.5 mm, after curing with Ultralume 5.
Discussion
The need for an adequate polymerization of the resin composites to result in good physical properties of the materials creates a dilemma to the clinicians concerning the selection of the appropriate LCU.
Several studies [2, 16] have addressed the application of blue LED technology to cure better dental materials. In comparison of the camphoroquinone (CQ) absorption spectrum with the emission characteristics of halogen lights, it is found that only a small portion of the halogen emission spectrum actually is used to activate the photoinitiator molecules. It has been shown that blue light in different parts of the absorption spectrum of CQ has a different effectiveness, and that light near to the absorption peak (468 nm) is more effective at curing [16, 30].
Previous studies [13, 27] have used bottom/top Knoop hardness ratios to obtain a percentage depth of cure, and if that value exceeded 80%, specimens were considered to be adequately cured. According to this criterion, all three LCUs tested in the first part of our study succeeded the 80% of the hardness of 0.5 mm under the top surface at a depth of 2.5 mm for Tetric Ceram®. Only the 10-s exposure in Smartlite PS for the shade A2 was shown not to achieve this curing depth. In the present study, maximum hardness (surface hardness) was determined as the hardness 0.5 mm beneath the surface and not on the surface of the samples because of the fact that the samples used in the present study were not polished like it would be in clinical situation. In our study, the “surface” hardness was found to vary with significant difference depending on the LCU used. That is, in contrast with the findings of Lindberg et al. [11], who found that the composite closer to the surface was equally well cured with all the LCUs tested. The different LCUs and the different exposure times used could be the reason for the different results. In the study of Lindberg et al. [11] a longer exposure time was used.
In the first part of the present study, it was shown that the halogen LCU produced higher microhardness values compared to the two LED LCUs, for a standard resin composite in two shades.
Our results from the first part of the study coincide with those of previous studies [5, 10] which showed that the halogen LCUs produced significantly harder composite surfaces, up to a depth of 2.5 mm, than did the LED LCUs. However, our findings with the conventional hybrid resin composite come in contrast with the results of Mills et al. [16], who used a power density of 290 mW/cm2 from LED unit and 300 mW/cm2 halogen LCU to compare the depths of cure of resin composites. Under those conditions, the LED LCU cured hybrid resin composites of medium shades significantly deeper than did the halogen LCU. This is in line with the results of the second part of the study concerning the translucent resin composites.
The important parameter concerning the performance of the different LCUs is the amount of light energy with an appropriate wavelength emitted during irradiation [30]. Additionally, the CQ conversion, within the resin composite, is correlated with the radiant exposure and the power densities of the LCUs [3].The power density values received from the measurements with curing radiometers involve the whole energy output, more than just the narrow CQ spectrum. Therefore, halogen-based lights, in most cases, demonstrate higher power densities than LEDs. Manufacturers of LED LCUs warn against using radiometers to compare LED performance with that of halogen-based LCUs. The Cure Rite curing light meter which is used in the present study can give only a rough guide concerning some of the LCUs measured. Especially for Ultralume 5, which has a large (10 × 14 mm) oval curing footprint, larger than the measurement’s position of the Cure Rite (8 mm), it could be possible that the irradiance measured in the present study may show not the exact results.
According to our results, the performance of the two LED LCUs differed significantly for the two shades of the resin composite tested. For the shade A2, no significant difference was found between the two LED LCUs. For the shade A3, Smartlite PS had a significantly better performance for the depths 0.5 and 1.5 mm compared to Ultralume 5. This finding may be explained by the fact that Ultralume 5 has a wavelength range of 370–500 nm instead of the spectrum of Smartlite PS, which is centered in the 450–490 nm region near the sensitivity peak of CQ in 465 nm. The difference between the results of the two shades could be the fact that the concentration of CQ in lighter shades is lower.
In some previous studies [5, 8], the difference of the number of the LEDs was assumed to have a significant effect on the performance of the LED LCUs. Ultralume 5 contains five LEDs, while Smartlite PS contains only one 5-W LED. However, Ultralume 5 has a larger footprint, and only one of the five LEDs (blue LED) has the major role on the polymerization of the resin composites. The other four (yellow) are placed peripherally and have only a neglectable influence on the cure of the materials. Therefore, the difference on the number of the LEDs contained is not probably the reason for the different performance of the two LED curing units in the present study.
The energy density of LCUs can be calculated after multiplying the power density with the exposure time. For the units tested in the present study, the total energy densities calculated are: 1,063 mW/cm2 × 20 s = 21,260 mJ/cm2 for Ultralume 5, 950 mW/cm2 × 20 s = 19,000 mJ/cm2 for Smartlite PS and (150 mW/cm2 × 20 s) + (800 mW/cm2 × 20 s) = 19,000 mJ/cm2 for the halogen LCU. These are the energy densities produced by the LCUs based on the measurements of the curing light meter. According to the values mentioned above, there was no big difference between the LCUs. Although the halogen LCU has a smaller power density in comparison to the two LED LCUs, the fact that a longer polymerization time was used resulted in similar total energy density. It can be concluded that the exposure time used was a significant parameter for the results found in the present study between the three LCUs. This parameter is the one that differs between the different studies [11, 17]. The higher temperature produced by the halogen boosts the polymerization, and therefore, it can be also a reason for the good results of the halogen LCU [1, 22].
In the second part of the present study, the three composite materials were found to behave differently. The depth in which the measurements were able to be performed varied between the resin composites from 3.5 to 7.5 mm. The analysis showed that the hardness of QuiXfil was satisfying (80% of the hardness at 0.5 mm) at the depth of 4.5 mm compared with the halogen and Ultralume 5. Curing of QuiXfil with Smartlite PS resulted in an increase of curing depth up to 5.5 mm. This is a result with high clinical significance. This material can be used in thick increments and result in satisfying microhardness after cured once with any type of LCU. The Tetric Ceram®, according to the results of the present study, can be used in layers with maximum of 2.5-mm thickness, independently of the curing unit used. For Adamant®, it was shown that it could be used in increments of 3.5 mm when it is cured with halogen and Smartlite PS and in increments of 4.5 mm when it is cured with the Utralume 5. According to the above results, it seems that, based on the criterion of the 80% of the surface hardness, Smartlite PS can achieve for QuiXfil and Adamant® a better curing depth compared to Ultralume 5 and halogen. However, it must be mentioned that the absolute microhardness values of QuiXfil cured with Smartlite PS were in the same level as with that achieved with the halogen LCU, but lower to that achieved after curing with Ultralume 5. Concerning the translucent materials tested, these findings are in line with previous studies [17, 24, 25] that showed that the LED LCUs achieved a greater depth of cure with the halogen LCUs, when hybrid resin composite and ormocer were polymerized.
Many light-cured resin composites contain only the photoinitiator CQ for the generation of free radicals, and thus the polymerization reaction [18]. Some resin composites contain other photoinitiators in addition to CQ, the so-called co-initiators, which absorb light at shorter wavelengths (<410 nm) [18]. This is shown in the study of Uhl et al. [25], where the measurements with a penetrometer showed that the LED LCU achieved greater depth of cure than the halogen LCU. The results for the different resin composites were explained by the authors by the fact that one of the resin composites contains, in addition to CQ, co-initiators which absorb light at wavelengths shorter that 410 nm.
However, none of the resin composites used in the present study contained co-initiators beyond the photoinitiator CQ, according to the information given by the manufacturers. The results, however, were different between the three resin composites. The difference of the composition of the resin composites used, the higher amount of the filler loading, and the translucency of the two resin composites seem to be the reason for their greater curing depth compared to the standard hybrid resin composite. QuiXfil contains in its matrix also, besides the photoinitiator CQ, the accelerator dimethylaminobenzoic acid ester. This may also be a reason for its different performance.
In conclusion, within the limitations of this study, the present findings showed that that the LED LCUs were able to achieve at least similar depths of cure with those of the halogen unit in less curing time. The short exposure time is one of the beneficial characteristics of the LED LCUs since their introduction in the dental market.
However, as far as the Tetric Ceram® is concerned, the halogen LCU was found to produce higher Knoop hardness values compared to the two LED LCUs. The effectiveness of cure associated with LED curing lights was material dependent. However, it must be mentioned that the present results correspond only to the parameters (exposure times and resin composites) tested in the present studies. According to the two translucent resin composites, the hypothesis made in the aims of the present study can be accepted. These resin composites were found to be able to have a satisfying hardness for the clinical use, at a depth of at least 4.5 mm, after being cured once. Further experiments are necessary to investigate the shrinkage behavior of the translucent materials, when they are used in layers thicker than 2.5 mm and cured with halogen or LED LCUs, so that their clinical advantage can be confirmed.
References
Aravamudhan K, Floyd CJ, Rakowski D, Flaim G, Dickens SH, Eichmiller FC, Fan PL (2006) Light-emtting diode curing light irradiance and polymerization of resin-based composite. J Am Dent Assoc 137:213–223
Campregher UB, Samuel SM, Fortes CB, Medina AD, Collares FM, Ogliari FA (2007) Effectiveness of second-generation light-emitting diode (LED) light curing units. J Contemp Dent Pract 8:35–42
Chen Y, Ferracane JL, Prahl SA. (2005) Quantum yield of conversion of the dental photoinitiator camphorquinone. Saratov fall meeting 2004: optical technologies in biophysics and medicine IV. In: Tuchin VV (ed) Proc SPIE vol 5771. pp 256–266
Chung KH (1990) The relationship between composition and properties of posterior resin composites. J Dent Res 69:852–856
Dunn WJ, Bush AC (2002) A comparison of polymerization by light-emitting diode and halogen-based light-curing units. J Am Dent Assoc 133:335–341
Ferracane JL (1985) Correlation between hardness and degree of convention during the setting reaction of unfilled dental restorative resins. Dent Mater 1:11–14
Hofmann N, Hugo B, Schubert K, Klaiber B (2000) Comparison between a plasma arc light source and conventional halogen curing units regarding flexural strength, modulus, and hardness of photoactivated resin composites. Clin Oral Investig 4:140–147
Jandt KD, Mills RW, Blackwell GB, Ashworth SH (2000) Depth of cure and compressive strength of dental composites cured with blue light emitting diodes (LEDs). Dent Mater 16:41–47
Jung H, Friedl KH, Hiller KA, Haller A, Schmalz G (2001) Curing efficiency of different polymerization methods through ceramic restorations. Clin Oral Investig 5:156–161
Knezevic A, Tarle Z, Meniga A, Sutalo J, Pichler G (2001) Degree of conversion and temperature rise during polymerization of composite resin samples with blue diodes. J Oral Rehabil 28:586–591
Lindberg A, Peutzfeldt A, van Dijken JW (2004) Curing depths of a universal hybrid and a flowable resin composite cured with a quartz tungsten halogen and light-emitting diode units. Acta Odontol Scand 62:97–101
Lindberg A, Peutzfeldt A, van Dijken JW (2005) Effect of power density of curing unit, exposure duration, and light guide distance on composite depth of cure. Clin Oral Investig 9:71–76
Magna RK, Charlton DG, Wakefield CW (1995) In vitro evaluation of a curing radiometer as a predictor of polymerization depth. Gen Dent 43:241–246
Martin FE (1998) A survey of the efficiency of visible light curing units. J Dent 26:239–243
Mills RW (1995) Blue light emitting diodes - another method of light curing. Br Dent J 178:169(Letter)
Mills RW, Jandt KD, Ashworth SH (1999) Dental composite depth of cure with halogen and blue light emitting diode technology. Br Dent J 186:388–391
Mills RW, Uhl A, Jandt KD (2002) Optical power outputs, spectra and dental composite depths of cure, obtained with blue light emitting diode (LED) and halogen light curing units (LCUs). Br Dent J 193:459–463
Park YJ, Chae KH, Rawls HR (1999) Development of a new photoinitiator system for dental light-cure composite resins. Dent Mater 15:120–127
Pilo R, Oelgiesser D, Cardash HS (1999) A survey of output and potential for depth of cure among light-cured composite. J Dent 27:235–241
Rodrigues Junior SA, Zanchi CH, Carvalho RV, Demarco FF (2007) Flexural strength and modulus of elasticity of different types of resin-based composites. Pesqui Odontol Bras 21:16–21
Ruyter IE (1985) Monomer systems and polymerization. In: Vanherle G, Smith DC (eds) Posterior composite resin dental restorative materials. Peter Szulc Publishing Co, Amsterdam, pp 109–136
Schneider LF, Consani S, Correr-Sobrino L, Correr AB, Sinhoreti MA (2006) Halogen and LED light curing of composite temperature increase and Knoop hardness. Clin Oral Investig 10:66–71
Stahl F, Ashworth SH, Jandt KD, Mills RW (2000) Light-emitting diode (LED) polymerization of dental composites: flexural properties and polymerization potential. Biomaterials 21:1379–1385
Uhl A, Michaelis C, Mills RW, Jandt KD (2004) The influence of storage and indenter load on the Knoop hardness of dental composites polymerized with LED and halogen technologies. Dent Mater 20:21–28
Uhl A, Sigusch BW, Jandt KD (2004) Second generation LEDs for the polymerization of oral biomaterials. Dent Mater 20:80–87
Vargas MA, Cobb DS, Schmit JL (1998) Polymerization of composite resins: argon laser vs conventional light. Oper Dent 23:87–93
Watts DC, Amer O, Combe EC (1984) Characteristics of visible-light-activated composite systems. Br Dent J 56:209–215
Watts DC, Amer OM, Combe EC (1987) Surface hardness determination in light-cured composites. Dent Mater 3:265–269
Witzel MF, Calheiros FC, Goncalves F, Kawano Y, Braga RR (2005) Influence of photoactivation method on conversion, mechanical properties, degradation in ethanol and contraction stress of resin-based materials. J Dent 33:773–779
Yoon TH, Lee YK, Lim BS, Kim CW (2002) Degree of polymerization of resin composites by different light sources. J Oral Rehabil 29:1165–1173
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Polydorou, O., Manolakis, A., Hellwig, E. et al. Evaluation of the curing depth of two translucent composite materials using a halogen and two LED curing units. Clin Oral Invest 12, 45–51 (2008). https://doi.org/10.1007/s00784-007-0142-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-007-0142-z