
Abstract
Based on the principles of classic film tomography, a new digital X-ray device for dental sites was developed and clinically evaluated. The tomosynthesis process produces several slices from a finite number of radiographs taken from different projection angles, obtaining a three-dimensional image of the jaws and teeth. During evaluation of an industrial prototype, a total of 52 tomosynthesis data sets were made covering different anatomic areas. Of those, 32 sets were assessed by ten radiologically experienced dentists. Anatomic regions not shown on conventional intraoral dental films were displayed due to the extraoral sensor. Diagnostic images of high value were mainly achieved within the scope of lateral views and transverse views in the frontal region. Even small structures such as the periodontal ligament could be shown in several planes, resulting in superposition-free representation. The elimination of metal artefacts caused by dental restorations was facilitated. However, improvements can be made in definition and resolution. Views in the sagittal plane and incomplete blurring of the contralateral jaw are difficulties that remain. The tomosynthesis process combined with a planned 3D representation is likely to be well suited for dental radiology. The use of such a device could be much less expensive than computed tomography (CT). Furthermore, it offers higher spatial resolution, exposes patients to less radiation, and could be easily used in daily practice, even chairside.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The first digital tomosynthesis system was evaluated in 1972 by Grant [7]. Groenhuis et al. [8] started researching it in dentistry in 1983 by testing different projection geometries. Webber et al. [18] compared a very similar technique, "tuned aperture computed tomography" (TACT), with conventional and digital radiography in 1996. During the following years, TACT [20] and tomosynthetic reconstruction methods [17, 18] proved they can present digital three-dimensional imaging with high diagnostic accuracy and spatial resolution. These techniques were applied not only in digital mammography but also in the fields of traumatology [11, 12, 13, 14] and periodontology [1, 16].
Based on the tomosynthesis process, an extraoral digital imaging system for dental radiology was developed at the Centre for Dental Innovations (CDI) in cooperation with Sirona Dental Systems (both in Bensheim, Germany) [5, 6] and clinically evaluated in our department [21] (Fig. 1). The device was designed as a research prototype not for serial production. It produces an arbitrary number of tomographic slices from a finite number of radiographs taken from different projection angles during a single tomographic sweep. Circular projection geometry was used in this study. The object of interest was completely displayed three-dimensionally in multiple layers retrospectively with only one tomographic pass. This allowed reductions in patient dose, time, and cost, especially compared with conventional tomography.

Tomosynthesis-device (industrial prototype)
The aims of the first investigations were to improve and further develop the practical applicability, evaluate anatomic regions, and apply the system to clinical diagnosis, in which it was shown to be suitable.
Materials and methods
The radiographic source used in this investigation was a commercial dental X-ray tube (Heliodent DS, Sirona Dental Systems, Bensheim, Germany). The sensor was an extraoral CCD chip (Siemens Med, Sweden) with an active area of 49×86 mm. Exposures were made at 60 kV, 7 mA, and a radiation time of 0.4 s for each single image. An infinite number of projections would minimize the artefacts but would also cause an intolerably high radiation dose. On the other hand, a small number of projections would increase the number of artefacts, leading to insufficient diagnostic quality [10]. Therefore, a set of 24 radiographs were taken in circular scanning geometry with a tomosynthetic angle of ±11°. A smaller angle would have led to worse resolution. Scan time was about 40 s, with a total exposure time of 9.6 s.
Radiation doses were measured according to the German Industrial Norm (DIN) 6868 parts 5 and 5.1 for panoramic devices. A Diados dose sensor (PTW, Freiburg, Germany) was used. Exposures were made at 60 kV and 7 mA with exposure times of 0.08 s to 0.4 s.
For adequate representation of anatomic structures such as the periodontal ligament, a spatial resolution of 5 lp/mm and a slice thickness of 1 mm were used. Images were reconstructed from the projection data using a personal computer and displayed on a conventional high-resolution color monitor. The overall reconstruction time was 7 m. The reconstruction technique used in this study was ectomography [3], which is based on two-dimensional, filtered backprojection. In ectomography, the spatial frequencies of the component images are subjected to both high- and low-pass filtration in mutually perpendicular directions [10].
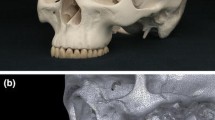
After receiving permission of the ethics committee, 52 tomosynthesis data sets were made from ten phantom X-rays (Alderson-Rando-Phantom) and 42 patients aged 18 to 72 years. Lateral and transversal radiographs (Fig. 2) were made by the tomosynthesis process covering different areas of the jaw, including the temporomandibular joint. During the first phase of the study, several changes in the software and construction of the device were made based on the ten phantom images and the first ten patient images. In general, subjects were recruited from outpatients of our department who required routine X-ray investigations independently of the tomosynthesis study. Excluded were patients below 18 years of age, pregnant women, and persons exposed to radiation.

Projection planes for lateral images (lower jaw)
The final 32 patient images were assessed by ten radiologically experienced dentists using a specially developed questionnaire. First, the diagnostic accuracy of the imaging system was evaluated. The observers scored subjective certainty of the presence or absence of a given disease using a 5-point confidence rating scale. These diseases were checked for certainty with reliable clinical findings (vitality tests, probing, pathologic mobility, etc.) and additional intraoperative diagnostics (apical bone lesions, cysts, fracture gaps, etc.). In line with other scientific publications [2], this served as a basis for calculating sensitivity and specificity. As there were only a limited number of X-rays and therefore identical anatomic areas investigated due to the regulations of the ethics commission, results were analyzed by using the curve of the conditional probability of true positive responses vs false positive responses from an ROC investigation. In order to minimize the radiation dose, comparison with standard projection radiographs was not carried out in this stage of testing. Furthermore, the observers were asked to assess diagnostic quality regarding the representation of anatomic structures in all images according to a five-point scale. They also assessed whether the respective areas of interest were sufficiently covered in the radiographs.
The digital images were displayed with various contrast and/or brightness enhancements (changes of 5% to a maximum of 10%). The observers were asked to assess whether the different options led to subjective improvement or impairment of image quality. Finally, they evaluated whether the option of reducing metal artefacts—using specially developed algorithms and programs—could increase image quality. Results were analyzed using Wilcoxon's signed rank test.
Results
A total of 52 tomograms were produced. At the beginning of the evaluation, image quality was not fully satisfactory. Due to early problems, several changes were made in the software and construction of the tomosynthesis unit during the first 20 images (ten of phantoms and ten of patients):
Adjustment of the exact anatomic position without an overlap of the blind frame could be reached by using a setup without previous adjustment for angle measurements. Positioning of the source-sensor unit (C arch) was accomplished only by marking the object to be examined on the patient's cheek and by final adjustment with a lighting sight.
Exact positioning of the focal plane, even in deviations from the anatomic norm, was achieved using a distance holder made of material that was virtually transparent to X-rays. It was fixed at the sensor and secured at a constant distance, resulting in correct positioning of the focal plane via adjustment to the area marked on the patient's cheek.
To avoid motion artefacts, the originally rigid frontal rest and bite block were replaced by an articulated arm with double ball-and-socket articulation. Also, a new, larger bite block was adapted and filled with wax. The handling thus became very simple, since the construction with the double articulation was very mobile and could be brought into any position and fixed with only one screw.
Image artefacts due to high absorption of metal objects (fillings and crowns) or thick bones (the jaw along the side arch) were minimized by developing new algorithms and software for artefact suppression. Finer structures such as the periodontal space were visualized.
The capacity of the built-in Heliodent DS X-ray tube turned out to be too weak for transversal radiographs of posterior teeth and the temporomandibular joint and for lateral radiographs of the anterior teeth. Thus, in the second phase of the study (during imaging of the final 32 patients), these images were omitted, but using an X-ray source with higher voltage should easily solve this problem. The total absorbed dose measured for 24 single images with an exposure time of 0.4 s was a maximum of 16 mGy. This represents a maximum equivalent body dose of 16 mSv. A blank test of an Orthophos plus DS digital panoramic device (Sirona, Bensheim, Germany) showed a dose of 12.1 mGy under comparable conditions.
Tomosynthesis delivers sharp and focused images of objects in the desired slice with high resolution. Objects distant from this slice appear blurred. Reconstructions show blurred images of object details outside the focal plane superimposed on the desired image of the slice of interest. This is caused by the tomographic process, which adds information from out-of-focus planes to that required in the plane of interest. Otherwise, by adjusting the imaging algorithms including different filter techniques, the image quality already showed striking improvement in the first 20 images (ten phantoms and ten patients).
Results of the questionnaire based on the final patient series
The last 32 images were used for a questionnaire to evaluate the diagnostic quality. Analysis of the assessment by the ten observers using the ROC curve revealed an overall sensitivity of 71%, with a specificity of 49%. The area below the ROC curve, which is an indicator of diagnostic accuracy, was 81.8%.
The 32 images were rated (five-point scale of image quality) on average at 3.14. The best results were achieved in lateral images for the temporomandibular joint (out of ten images altogether), the molar region of the lower jaw (out of 12), and the basal mandibular angle (one image), followed by radiographs of the molar region of the upper jaw (out of 11), e.g., in the image of the basal mandibular angle, the course of the mandibular canal and its spatial relation to wisdom teeth were considered to be well evaluable (Fig. 3, Fig. 4). Concerning anatomic structures, the best results were achieved for the apical region of the teeth, pulp/root canal fillings, and the periodontal ligament.

Tomosynthesis image of the upper molar region

Occlusal filtered image of the mandible as an example for future perspectives
Subjectively viewed, digital contrast and brightness enhancement options revealed general improvement in image quality for increased contrast alone and increased contrast and brightness in combination. The use of other possibilities or combinations of digital refinishing options showed no diagnostic advantage. Finally, Wilcoxon's signed rank test (P<0.03) revealed significantly improved image quality regarding the comparison of metal artefact-reduced images with original radiographs.
Discussion
Patient and phantom studies demonstrate the potential of this tomosynthesis device [5]. The purpose of a preliminary study was to explore the potential and limitations of digital tomosynthesis in the dental field as well as the advantages and disadvantages of this prototype [21]. The number of projections has to be sufficiently high to avoid ripple artefacts [10] but should be as low as possible to keep patient doses in an acceptable range. In 12 projections, the manufacturers of the device had already registered an immense number of artefacts and also disturbances due to overlapping of neighboring structures. Therefore, a compromise of 24 projections was chosen. A small tomosynthesis angle is desirable concerning the reduction of projection images but, when too small, leads to poor depth resolution. Therefore, this angle must be large enough to allow reconstructions with acceptable depth resolution [10].
The absorbed patient dose of 16 mSv per image was almost in the range of that in panoramic X-rays (ratio of 1.3:1) [2, 9] and therefore lower than for other imaging techniques such as CT [4, 6, 22]. Compared with conventional tomography [15], tomosynthesis has the advantage that several layers can be reconstructed from the same set of projection data. Therefore, if the focal plane is incorrect, the scan does not have to be repeated, which reduces time, cost, and patient dose. With a limited number of projection images, an unlimited number of slices of the desired object can be reconstructed after only one tomographic sweep.
In comparison to intraoral systems, techniques with extraoral sensors need higher radiation exposure, and image quality is affected by cross-talk of out-of-focus structures due to incomplete blurring of objects of the opposite jaw. On the other hand, the extraoral sensor is not affected by spatial or anatomic limitations. Therefore, regions which cannot be reached with an intraoral sensor can easily be displayed by this technique (impacted third molars of the lower jaw and the relation of their apices to the inferior alveolar nerve, the basal mandibular angle, and the temporomandibular joint). The technique offers 3D information and might therefore be superior to conventional 2D display options.
Like all digital imaging techniques, digital tomosynthesis also allows image enhancement options such as filtering, contrast or brightness enhancement, and elimination of metal artefacts [9, 22].
The correct positioning of the source-sensor unit (C arch) needs further attention, even after our changes in the construction of the prototype, in order to avoid adjustment problems and guarantee a satisfactorily constant representation of the region of interest.
Patient fixation could be greatly improved by the modified construction of the bite block. Patient movement during the scan time (40 s) leads to double contours and thus to a loss of image quality. Other techniques (e.g., tuned aperture computed tomography) restrict the period during which the patient may not move to the actual exposure time; movement within the different projections does not influence image quality [19], since reconstruction does not require the projection geometry to be known in advance. This is carried out by using a fiduciary point that is displayed on each component radiograph.
The algorithms and programs developed to eliminate artefacts caused by metal objects within the X-ray beam showed a striking improvement in image quality (Wilcoxon's signed rank test, P<0.03) and are considered to improve diagnostics as well. Further studies are necessary in this area. Additionally, diagnostics in areas adjacent to metal pieces in the displayed object could be improved by burnishing strong contrast differences in order to guarantee reliable caries diagnosis near fillings and crowns.
Computed tomography reconstructs slice by slice, ideally showing in each slice only the objects within that single slice. Tomosynthesis shows the objects in the desired slice sharply and in focus, displaying better resolution than with CT. The objects distant to this slice appear blurred; the more distant they are, the more blurred and less visible they become [6].
In this stage of testing, we had only the possibility and permission for a limited amount of radiographic investigations on patients. For better evaluation of the system's accuracy and diagnostic quality, a significantly higher number of images is desirable covering the different areas and indications. Furthermore, this system should also be compared with other imaging techniques based on a gold standard.
Conclusions
In our opinion, the tomosynthesis procedure combined with planned 3D reconstruction presents an imaging technique well-suited to the field of dental radiology, since it presents more information than conventional 2D radiographic devices. As there are no spatial limitations or anatomic restrictions, areas that cannot be displayed by intraoral systems can easily be shown. Since the radiation dose is relatively low compared with other 3D imaging techniques, tomosynthesis could be useful in planning surgery for dental implants. With further improvements, this technology could offer higher spatial resolution than CT or conventional tomography. Furthermore, it subjects patients to less radiation exposure and could be much cheaper than CT.
References
Chai-U-Dom O, Ludlow JB, Tyndall DA, Webber RL (2001) Detection of simulated periodontal bone gain by digital substraction radiography with tuned aperture computed tomography. The effect of angular disparity. Dentomaxillofac Radiol 30: 92–97
Dannewitz B, Hassfeld S, Eickholz P, Mühling J, Ziegler C (2001) Dosisreduktion bei digitalen Panoramaschichtaufnahmen. Dtsch Zahnärztl Z 56: 490–494
Edholm P, Granlund G, Knutsson H, Petersson C (1980) Ectomography. A new radiographic method for reproducing a selected slice of varying thickness. Acta Radiologica 21: 433–442
Ekestubbe A, Thilander A, Gröndahl K, Gröndahl HG (1993) Absorbed doses from computed tomography for dental implant surgery: comparison with conventional tomography. Dentomaxillofac Radiol 22: 13–17
Franetzki M, Mougoui N, Ziegler CM (2000) An extra-oral tomosynthetic device with circular scanning. In: Lemke HU, Vannier MW, Inamura K (eds) Computer-assisted radiology and surgery. Proceedings of the 14th International Congress and Exhibition on Computer-Assisted Radiology and Surgery, San Francisco, June 28 July 1, 2000. Elsevier, Amsterdam, p 853
Franetzki M (2001) Dreidimensionales Röntgen in der Zahnheilkunde. ZWR 11: 741–745
Grant DG (1972) Tomosynthesis: a 3-dimensional radiographic imaging technique. IEEE Trans on Biomed Eng 19: 20–28
Groenhuis RAJ, Webber RL, Ruttimann UE (1983) Computerized tomosynthesis of dental tissues. Oral Surg Oral Med Oral Pathol 56: 206–214
Hassfeld S, Ziegler C, Mühling J (1997) Kann die digitale Panoramaschichtröntgentechnik das filmbasierte Verfahren ersetzen? ZWR 106: 510–514
Lauritsch G, Härer WH (1998) A theoretical framework for filtered backprojection in tomosynthesis. Proceedings of the SPIE Medical Imaging Conference, Image Processing 3338, San Diego
Nair MK, Webber RL, Johnson MP (2000) Comparative evaluation of tuned aperture computed tomography for the detection of mandibular fractures. Dentomaxillofac Radiol 29: 297–301
Nair MK, Seyedain A, Webber RL, Nair UP, Piesco NP, Agarwal S, Mooney MP, Grondahl HG (2001a) Fractal dimension analysis of osseous healing using tuned aperture computed tomography images. Eur Radiol 11: 1510–1515
Nair MK, Seyedain A, Agarwal S, Webber RL, Nair UP, Piesco NP, Mooney MP, Grondahl HG (2001b) Tuned aperture computed tomography to evaluate osseous healing. J Dent Res 80: 1621–1624
Nair MK, Nair UDP, Grondahl H-G, Webber RL, Wallace JA (2001c) Detection of artificially induced vertical radicular fractures using tuned aperture computed tomography. Eur J Oral Sci 109: 375–379
Quintero JC, Trosien A, Hatcher D, Kapilla S (1999) Craniofacial imaging in orthodontics: historical perspective, current status and future development. Angle Orthod 69: 491–506
Ramesh A, Ludlow JB, Webber RL, Tyndall DA, Paquette D (2002) Evaluation of tuned aperture computed tomography in the detection of simulated periodontal defects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 93: 341–349
Suryanarayanan S, Karellas A, Vedantham S, Glick SJ, D'Orsi CJ, Baker SP, Webber RL (2000) Comparison of tomosynthesis methods used with digital mammography. Acad Radiol 7: 1085–1097
Suryanarayanan S, Karellas A, Vedantham S, Baker SP, Glick SJ, D'Orsi CJ, Webber RL (2001) Evaluation of linear and nonlinear tomosynthetic reconstruction methods in digital mammography. Acad Radiol 8: 219–224
Webber RL, Horton RA, Underhill TE, Ludlow JB, Tyndall DA (1996) Comparison of film, direct digital, and tuned-aperture computed tomography images to identify the location of crestal defects around endosseous titanium implants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 81: 480–490
Webber RL, Underhill HR, Freimanis RI (2000) A controlled evaluation of tuned aperture computed tomography applied to digital spot mammography. J Digit Imaging 13: 90–7
Ziegler CM, Hassfeld S, Franetzki M (2000) First clinical experiences with the tomosynthesis process. In: Lemke HU, Vannier MW, Inamura K (eds) Computer-assisted radiology and surgery. Proceedings of the 14th International Congress and Exhibition on Computer-Assisted Radiology and Surgery, San Francisco, June 28 to July 1, 2000. Elsevier, Amsterdam, p 857
Ziegler CM, Wörtche R, Brief J, Hassfeld S (2002) Clinical indications for digital volume tomography in oral and maxillofacial surgery. Dentomaxillofac Radiol 31: 126–130
Acknowledgements
This study was performed together with the Centre for Dental Innovations and supported by Sirona Dental Systems.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ziegler, C.M., Franetzki, M., Denig, T. et al. Digital tomosynthesis—experiences with a new imaging device for the dental field. Clin Oral Invest 7, 41–45 (2003). https://doi.org/10.1007/s00784-003-0195-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-003-0195-6