
Abstract
Diabetes therapy management in AAL environments, such as old people and diabetes patients homes, is a very difficult task since many factors affect a patient’s blood sugar levels. Factors such as illness, treatments, physical and psychological stress, physical activity, drugs, intravenous fluids and change in the meal plan cause unpredictable and potentially dangerous fluctuations in blood sugar levels. Right now, operations related to dosage are based on insulin infusion protocol boards, which are provided by physicians to the patients. These boards are not considering very influential factors such as glycemic index from the diet, consequently patients need to estimate the dosage leading to dose error, which culminates in hyperglycemia and hypoglycemia episode. Therefore, right insulin infusion calculation needs to be supported by the next generation of personal-care devices. For this reason, a personal device has been developed to assist and consider more factors in the insulin therapy dosage calculation. The proposed solution is based on Internet of things in order to, on the one hand, support a patient’s profile management architecture based on personal RFID cards and, on the other hand, provide global connectivity between the developed patient’s personal device based on 6LoWPAN, nurses/physicians desktop application to manage personal health cards, glycemic index information system, and patient’s web portal. This solution has been evaluated by a multidisciplinary group formed by patients, physicians, and nurses.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Diabetes mellitus is estimated as one of the major chronic diseases and growing public health problems in the world. This disease increases a patient’s risk of developing multiple health complications such as heart and kidney failure. However, these implications can significantly be reduced by controlling blood glucose level [1]. Factors such as the illness that patient suffers, treatments received, physical and psychological stress, physical activity, drugs, intravenous fluids, and meal plan (diet) can cause unpredictable, potentially dangerous fluctuations in blood sugar levels, resulting in hypoglycemia and hyperglycemia episodes. For example, hyperglycemia episode (high glucose level) slows down the healing process and boosts the risk of infection [2, 3].
Recent research indicates that using diabetes self-management systems help to control glycemia and associated blood glucose levels. For this reason, software solutions [4] have been defined for monitoring and modeling of blood glucose. Since these solutions have the problem that depends on a PC, different kinds of solutions closer to the user are being defined such as glucometers integrated in digital photography [5] and in cellular phones, i.e. mobile Health solutions (mHealth) [6]. In recent years, an extensive research work and system addressing the design and development of mHealth-based diabetes management systems have been witnessed [7, 8]. A recent systematic review has confirmed the feasibility of this approach regarding its efficacy on diabetes control and the impact on the intensification of blood pressure management [9].
Internet of things (IoT) is one of the major communication advances in recent years that links the internet with everyday sensors and working devices for an all-IP-based architecture, linking physical and virtual objects through the exploitation of data capture and communication capabilities. Internet of things architecture will offer specific object identification, sensor and connection capability as the basis for the development of independent cooperative services and applications. An extensive research on using this concept in different mHealth applications has been recently reported [10]. However, no study to date addresses this concept and presents architecture for ubiquitous personal diabetes management.
This paper presents a personal diabetes management device based on Internet of things, in order to provide a new generation of mobile assistance services and consider more of the mentioned factors for insulin therapy, in order to reduce the number of the patient hyperglycemia and hypoglycemia episodes and consequently their risks. This personal device supports 6LoWPAN connectivity in order to link the personal device with the developed home gateway [11], RFID identification in order to load patient’s profile from the personal health card, serial communication based on RS232 and IrDA to connect the glucometers from different vendors, and a color touch screen to interact with the patient. In addition, this personal device is complimented with a glycemic index information system (with more than 2,600 indexed products and growing) to provide information about the impact in the glucose of the diet, a desktop application for nurses/physicians to configure and review the patient’s personal health card based on RFID, a web portal for online patients and specialist management, and finally, this personal device is complemented with an application layer based on artificial intelligence to define an adaptive insulin therapy for the patients. The main goal of this approach is to provide the patients with better access, understanding, and involvement in their personal-care program, in order to reach better control and management of their insulin therapy.
The following sections of the paper are organized as follows. Section 2 presents the insulin therapy model followed for diabetes management. Section 3 presents architecture to support diabetes management in Ambient Assisted Living (AAL) environments. The architecture parts are described in the subsections. Section 3.1 presents the patient’s personal diabetes management device. Section 3.2 presents the desktop RFID-based management application for nurses and physicians. Section 3.3 presents the diabetes management web portal and glycemic index database. Section 4 presents the evaluation and discussion of the solution with a group formed by nurses, physicians, and patients. Finally, Sect. 5 concludes the paper.
2 Insulin therapy model
The American Diabetes Association recommends keeping blood glucose levels between 100 and 140 mg/dl in normal situation and below 180 mg/dl for 2 h after meals, i.e. period of digestion. Patients with diabetes mellitus need blood glucose control and usually insulin therapy, in AAL environments, in order to keep their glucose inside the mentioned range. Patients should be educated with a deeper understanding as to how changes in their therapeutic regimen could affect their glycaemic control, as such to motivate patients to optimize their own therapy with guidance from their physician. But, such as mentioned, many factors will affect patient blood sugar levels, and any of these factors can cause unpredictable and potentially dangerous fluctuations in blood sugar levels. It is not feasible for diabetic patients such as elderly people to consider all these factors, but they should be considered in order to reach an accurate insulin therapy. The proposed solution has defined an insulin therapy model considering the following factors: patient weight, glucose level, physician recommendations, and finally the carbohydrate absorption in quantitative terms such as glycemic index, volume of glucose, insulin distribution, and maximal rate of gastric emptying, which are based on the underlying pathophysiology of diabetes mellitus.
Insulin units (IU) are injected following the protocol presented in Fig. 1 and Eq. (1), where basal is the amount of insulin required to manage normal daily blood glucose fluctuations (0.5f(GL) one shot per day, see Fig. 1), bolus is the dosage required to manage mealtime blood glucose fluctuations (0.5f(GL) distributed during meals), and correction factor is the dosage required to manage the rest of factors that influence the blood glucose level. The proposed model focuses mainly on the accurate estimation of the correction factor, the other parameters i.e. bolus and basal dose can be calculated generically following the Table 1, but our system will follow the recommended by the physician, when they are available in the patient personal health card (see Sect. 2), in order to be aware of the patient-specific considerations defined by the physician.

Insulin infusion protocol
We focus on the correction factor, which is going to vary depending on the glucose level before each meal (see Table 2), and the carbohydrate absorption (insulin distribution and maximal rate of gastric emptying) based on meal product glycemic index.
Nutritional information of the food products is essential for patients on treatment with use of fast insulin before each meal or insulin pumps since they are able to adapt their insulin dosage depending on the total amount of included carbohydrates (CHO) in each meal. In addition, patients who cannot change their dose of insulin, i.e. those treated with oral medication or dietary simply should maintain a stable amount of CHO in each meal, in order to keep proper blood glucose values. CHO foods are the most influential with glucose level, other products such as protein foods (fish, meat or cheese) and fat foods (butter, oils or sauces) are very low in CHO. Therefore, they have little effect on blood glucose levels. However, this does not mean they are harmless and on consuming, the amount and type of fat and the presence of other nutrients such as protein, vitamins, minerals, and dietary fiber should be considered. Table 3 presents the relation between the CHO and additional insulin units required [12].
However, not all carbohydrates are equal. For example, some provide only calories such as sugar, sweets, and sodas, and others provide minerals, vitamins, and fibers such as vegetables and fruits. Therefore, the glycemic response of the carbohydrate absorption needs to be considered. This absorption is based on the ingestion process.
The amount of glucose in the gut (intestine), G gut, following the ingestion of a meal containing CHO grams of glucose equivalent of carbohydrates is defined as:
where K gabs is the constant rate of glucose absorption from the gut into the systemic circulation (estimated as constant to 1 per hour). G empt is the rate of gastric emptying (ge) (ge refers to the speed at which food and drink leave the stomach).
The duration of the period \(T_{\rm max\,ge}\) for gastric emptying depends on the CHO content of the meal ingested:
where \(V_{\rm max\,ge}\) is the maximal rate of gastric emptying, and \(T_{\rm asc\,ge}\) and \(T_{\rm des\,ge}\) are the respective lengths of the ascending and descending branches of the gastric emptying curve that have default values of 30 mins (0.5 h), considering it the usual time spent for lunch, breakfast, and dinner.
For small quantities of carbohydrate (under approximately 10 g), such values cannot be used because there will never be time for the gastric emptying curve to plateau out. Using linear interpolation, the rate of gastric emptying for meals containing CHO grams of carbohydrate greater than 10 g (see Table 3) can therefore be defined, according to the time elapsed from the start of the meal, t, the digestion process, and consequently, the carbohydrate absorption is defined as follows:
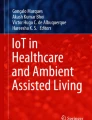
This carbohydrate absorption during the digestion process, see Eq. (4), can be adjusted for each product used in the meal considering its glycemic index (GI). GI is a numerical index that ranks carbohydrates based on their rate of glycemic response (i.e. their conversion to glucose within the human body) and duration of the digestion process for a given type of food and its effect on blood glucose level. GI uses a scale, nutrition with low glycemic index values causes the blood glucose level to rise slowly and over a long period of time, and nutrition with high glycemic index values causes the blood glucose level to rise more sharply, followed by a sheer drop such as presented in Fig. 2. Rise, peak, and drop of the blood glucose level is directly related to the evolution of the digestion presented in G empt, Eq. (4).

GI relation with blood glucose
GI function divides carbohydrates into two groups: rapid/medium absorption and slow absorption since slow absorption products are not considered inside the correction factor. Pure glucose serves as a reference point and is given a GI of 100, under 55 is considered low and medium/rapid in another way.
where gi represent the glycemic index for each product. Fig. 3 presents some values determined experimentally by feeding human test subjects a fixed portion of the food and subsequently extracting and measuring samples of their blood at specific intervals of time. Thereby, GI represents a generic value valid for all patients, since this defines a medium value from different subjects for the \(V_{\rm max\,ge}\) parameter of the G empt. This solution offers a database with more than 2,600 glycemic index values of usual products (see Sect. 3.3).

GI index database
Finally,other issues, such as the specific insulin action (Ia) of the insulin type used over the current insulin value (I), dosage-dependent peak times, onset time, flattish peak time, and duration, need to be considered:
where k1 and k2 are first-order rate constants that serve to describe the insulin action. Since the rate of insulin action depends on each insulin type, the specific brand of insulin used is also part of the patient’s health profile.
3 Architecture to support diabetes management in AAL environments
Self-monitoring blood glucose (SMBG) measurements are conventionally analyzed by the physician by visually scanning the patient’s logbook. As a consequence, clinical decisions are sometimes based on inadequate assessments of the available data. The ability of health care professionals (nurses and physicians) to efficiently access and analyze that data is crucial; therefore, a desktop application to review all the glucose value logs has been developed. In addition, the mentioned problem runs deeper than this since patients also need to be able to interpret their own data and act on it accordingly. SMBG will not lead to improve glycemic control without appropriate assessment and modification of the treatment with respect to the followed regimen. For that reason, an educational effort for teaching patients how to ’close the loop’ and adjust their own insulin injections, diet and lifestyle is required, but that teaching is not possible for elderly patients and even for the rest of diabetes patients, because, such as demonstrated in Sect. 3.2, those factors are not easily manageable by end users (patients). Therefore, in order to easily manage the information, we have defined, on the one hand, a patient’s personal management device to automatically carry out the logging of the glucose values and the calculation of the insulin therapy following the mentioned considerations in Sect. 3.2. On the other hand, in order to define in a simple way, the configuration of the personal device parameters to insulin injection board recommendation by physician, and to facilitate that a unique device can be used by different patients, personal health cards based on RFID are used. This section describes each one of the mentioned parts from the proposed solution. These parts are presented in Fig. 4.

Architecture diagram
3.1 Patient’s personal diabetes management device
The concept of providing a diabetic patient with a handheld electronic personal device that could store blood glucose readings and give the patient advice about the next meal and insulin injection has been the main goal for the design issues of this solution.
The system defined is based on Internet of things, which provides a global connectivity and management architecture of sensors, devices, users and information, and can be one of the key advances in the areas of mobile diabetes management system. Therefore, this proposal introduces an architecture to achieve a global connectivity with the diabetes management information system (glycemic index database), patient, sensors and everything around it to accelerate and enhance the management process. This architecture includes several advanced communication technologies for security, identification, control and connectivity with Internet; among them are 6LoWPAN and RFID technologies that form the basis of the new generation of personal services based on Internet of things. The main reason, because Internet of things has been considered for our proposal, has been, on the one hand, because 6LoWPAN connectivity allows to link the personnel directly to Internet and to external information systems, such as the defined diabetes management system, and on the other hand, because RFID allows an easy and quick patient identification and a medium to load the patient’s health record with just approaching their personal health card.
6LoWPAN is a protocol defined by the Internet Engineering Task Force (IETF), which extends wireless sensor networks (WSN) to Internet, adding to IEEE 802.15.4 a layer to support IPv6. It specifies a wireless link for low-power personal area networks (LoWPANs). These kinds of networks are characterized by their more limited capabilities than other WPANs (e.g. Bluetooth) and WLANs (e.g. WiFi), they have small frame size, low data rate, low bandwidth, and low transmit power. All this with the purpose of making sensors with low-power consumption and low cost.
RFID is the evolution of the barcode, which allows the identification of the doctors, nurses, and patients in an easy way. In addition, this improves the solutions based on barcode in that RFID cards and tags allow storing a lot of information, while barcode just allows storing an ID code. That extra memory space is very useful for storing information related with patient profile i.e. part of the Electronic Health Record. This is interesting, since it allows checking patient health profile in a local way, even when the system does not have access to Internet.
The developed system name is Movital, which means mobile solution for vital signs monitoring. Movital is the combination of the mentioned new generation technologies including, on the one hand, the module SkyeModule M2 from SkyeTek for contactless identification (RFID and NFC) to identify patients, and load patient health profile from the MiFare DesFire card, and on the other hand, the module Jennic JN5139 for Wireless Sensor Networks (WSN) communications based on Future Networks (6LoWPAN) to connect wireless clinical devices, such as glucometer to the AAL environment gateway, named Monere, which means in Latin language monitoring, remind, warn, and advise.
The features of these devices are the following:
Movital size has been minimized to credit card size to make it easily integrable with clinical sensors such as the glucometer. Power consumption has been optimized to ensure a high lifetime; power is based on reachable Lithium Batteries. Thereby, it defines a compact and autonomous module, which acts as gateway between the patient and the information systems such as glycemic index database (see Sect. 3.3). In order to ensure the Quality of Privacy (QoP) [14], Movital offers security capacities for user authentication, through symmetric-key encryption AES 128 bits and asymmetric-key encryption ECC 160 bits [16], and integrity based on CRC16-ITT.
The Movital solution offers two interfaces to connect the glucometer; on the one hand, this offers serial communication based on RS232, which is used for the LifeScan OneTouch Ultra Blood Glucose Meter. Right Fig. 5 presents the movital connected through a serial jack cable, with an RFID reader and the touch LCD screen. On the other hand, this offers IrDA communication to connect other glucometers such as Roche Accu-check Aviva Blood Glucose Meter. Left Fig. 5 presents the Movital version with the IrDA module.

Movital with LCD color touch screen, RFID reader with some Desfire Mifare cards, and glucometer connected through RS232 (right) and IrDA (left)
Monere is a platform developed to support ubiquitous data collection and global access. The main goal of this architecture is to facilitate, on the one hand, the retrieval of information from the different clinical sources, such as clinical sensors, and, on other hand, the integration of information with information systems such as the developed Diabetes Information System, Hospital Information System (where the electronic health record is located), Context Management Framework and Knowledge-Based System. In order to ensure QoP, such as Movital, Monere offers security capacities for authentication, privacy, and security through symmetric-key encryption AES-CBC (256-bit key), and integrity based on SHA256 and CRC16-ITT. The Monere platform is shown in Fig. 6.

Monere platform: AAL environment gateway
Finally, Movital includes an application layer to define an intelligent system based on the model defined in the Sect. 2, in order to calculate insulin therapy with the information gathered from the glucometers connected to Movital, the information of the patient health card (see Sect. 3.2) and the indications from the user through the touch screen, where mealtime and products consumed, in order to get the GI value, is indicated.
3.2 RFID-based management application
This application is used by physician and nurse to design and/or consult the patient profile and the recommended insulin dosage board. These records are stored in the patient’s personal health card, which is used by Movital, such as presented in Sect. 3.1.
The program has the following structure (Fig. 8):
-
User data: this section includes the patient’s personal information such as: name, surname, age, height, weight, and the national or private health insurance number (nin). The field left is the ATR card number.
-
Dose information: this is the insulin therapy board recommended by the physician. The column Values are the mg/dl of glucose in blood measured by the glucometer. Therefore, taking into account these ranges, these fields are filled in depending on the physician recommendation according to the patient’s profile. All this process is applied to the three main daily meals; breakfast, lunch, and dinner.
-
Insulin type: here are the two types of insulin: basal (slow) and bolus (fast). The basal insulin is taken once per day. The table filled in on the dose information section is related to the Bolus insulin, for each insulin active component chosen, the duration, the peak effect time and the onset time are indicated, in order to calculate the insulin action indicated in the model (see Sect. 2).
-
Body mass index: here this factor is calculated known as well as BMI.
-
RFID reader configuration: the last section to mention is the configuration connection, where IP Address and Port are chosen. This application is connected to the libNFC-based program that receives the information from the RFID card reader. This is connected through a socket, since the communication with the USB reader is based on C, and the diabetes management application is based on Java. In addition, this offers the opportunity to use the RFID reader included in Movital through the IPv6 network in the future. Fig. 7 presents how the application is linked with libNFC and the USB reader. The RFID module used is ACS 122 from Touchatag.

Application bridge between RFID reader, accessed through LibNFC based on C, and the nurse/physician diabetes management application based on Java

RFID-based desktop application screenshot to set-up Personal Health Card based on Mifare Desfire
The mentioned patient’s personal health profile information is stored in a MiFare DesFire card (ISO 14443 Type B). This provides extended security capabilities in the authentication. Symmetric keys, through 3DES (Triple Data Encryption Standard) cryptography, are used to decipher the tag information, since quality of privacy is one of the most important issues in health care solutions [14, 15]. In addition, the card structure has been defined using techniques to reduce access latency, optimize capacity, and guarantee integrity, as is described in a previous work [13], which includes CRC, memory map pointers, and type length value fields for variable length fields. This is presented in Fig. 9.

patient’s personal health card content and structure for management and system set-up
3.3 Web portal and glycemic index database
The diabetes management system is divided into two parts. On the one hand, this defines the Diabetes Information System, where we define the database with the glycemic index products database. The Diabetes Information System is accessed by the Movital (see Sect. 3.1) through the Internet, in order to consult the GI values. On the other hand, that information is also accessible from the developed web portal that provides registered users (see registration form Fig. 10)with an easy way to consult and obtain a list of food products according to the requirements from their insulin therapy. The patient can realize a search through form (see middle Fig. 11) or by categories (see bottom Fig. 11), being able to choose the desired products that meet their glycemic index and preserve the products list for the future.

Registration form in the web portal

Top: Home screen. Middle: Form to look for GI products. Bottom: GI categorized by the food pyramid
4 Evaluation and discussion
This solution has been designed, evaluated, and validated by a multidisciplinary group formed by patients, physicians, and nurses. The goals of this evaluation have been, on the one hand, to evaluate how this solution is accepted by clinical staff (nurses and physicians) and patients, and in addition to determinate how the intelligent insulin therapy supports nurse and physician tasks. On the other hand, to evaluate how the current clinical devices and clinical information systems such as Hospital Information System (HIS) need to be adapted in order to connect with the new generation of Internet (IPv6), technical issues of Internet of things technologies such as security requirements, and changes/adaptations in the deployed infrastructure to support them.
Based on a first prototype described in [8], nurses, physicians, and patients provided their feedback, comments, and recommendations, which have been used for the design of the actual solution.
First, nurses and physician recommendations and feedback have been:
-
Nurses and physicians recommended us to focus mainly in the adaptation correction factor, instead of a full insulin therapy determination. For that reason, insulin therapy recommendation board from the physician is included in the personal health card and web portal (see Sect. 3).
-
They also recommended considering the specific kind of insulin based on three parameters (onset, duration, and peak), which could be modified for bolus insulin, in order to support mixed insulin dosages.
-
Finally, they have recommended the defining of a solution of the system for hospitals, since management in blood glucose control is necessary for all patients in a hospital, since insulin is given even to hospitalized patients who usually are not using it. For example, on the one hand, insulin may be administered to patients without diabetes mellitus before, during, or after surgery because tight diabetes control around a surgery has been shown to reduce illness, shorten hospital stays, and even lower the risk of death, additionally individual circumstances vary on the glucose level pursued, usually the American Diabetes Association recommends keeping blood glucose levels below 180 mg/dl while in the hospital. However, for some patients, the recommendation is to keep blood glucose levels below 110 mg/dl. On the other hand, patients with type-2 diabetes, who do not usually use it, receive insulin as a way to temporarily control blood sugar levels when usual medication, diet, and exercise control regimens are disrupted. This is a reason why many factors will affect patient’s blood glucose level and consequently is recommended the extension to the hospital for the solution.
Secondly, patients recommendations and feedback have been:
-
Patients recommended us to define a categorized structure to make the management of the glucose index easier. For that reason, the LCD touch screen from the personal device and web portal have defined a food pyramid in order to classify the meal products (see bottom Fig. 11).
-
Patients commented that they made some bad considerations with respect to the correction factor based on meals, for example, some of them considered fat products as products that required an extra insulin dosage, when it has been presented that the relation is mainly focused on CHO. Therefore, the understanding of the diabetes insulin therapy is being enhanced.
-
With respect to the relevance and requirements of this solution in everyday life, one of the volunteers recognized that he suffered problems with hypoglycemia since the insulin therapy dosage was too high, resulting in “cold sweat”, and in one occasion, he went into a coma during some hours because of this. Usually, patients when suffering this situation consume some sweets like candy, which is very common, demonstrating that the insulin therapy followed is not accurate.
-
Comparability of the new doses with respect to the previous dosage has presented that insulin therapy recommended by the system is usually lower than the dosage that they used to define, and that the glucose level before the next meal was inside of the recommended range.
They consider that after the 2-week evaluation period, patients and physicians ask to continue using the system in their current life, in order to, on the one hand from the patients point of view continue improving their insulin therapy, and on the other hand, from the physician/nurses point of view, in order to measure the HbA1c after the following 6 months, which is used to show objectively with clinical relevance how their insulin therapy has been accurate adjusted.
With respect to the technological evaluation, this has been required to define an adaptor for the glucometers in order to connect them to the Internet, which has been presented in Sect. 3.1. The main problems related with this solution have been related to security issues, since the QoP is one of the most important design issues of our solution. For that reason, two pieces of research have been carried out in order to enhance the security for the personal health card [15] and support authentication of the personal device with the Diabetes Information System [16]. Finally, with respect to the adaptation of the current information systems, this has been required to define a Diabetes Information System to define the glycemic index database 3.
5 Conclusions and future work
mHealth based on Internet of things and Ambient Assisted Living are the research lines from ICT to alleviate the problems posed by chronic diseases such as diabetes mellitus. Our contribution has been an Internet of things-based AAL architecture to support blood glucose management and insulin therapy. This architecture offers a set of services for monitoring, interconnecting with the Diabetes Information System (glycemic index database), and ubiquitous access to the information based on the developed personal device (Movital), AAL environment gateway (Monere), web portal, and the management desktop application.
The important aspect of this solution is that most of the measurements and interactions with the patient are done at home, which enhances the self-monitoring blood glucose solutions, allowing the interaction of the nurses and physicians with the proposed platform through new technologies such as personal health card based on RFID and the Web diabetes management portal, which is connected to the Movital device through 6LoWPAN and the Internet to keep it updated.
Our conclusion is that the Internet of things is an interesting and promising approach for personalized health care systems in the next generation of mHealth solutions. The evolution of the technology allows to define new advanced systems, to reach a more accurate treatment of chronic diseases such as diabetes. In addition, Internet of things allows the defining of solutions closer to the patient, physician, and nurses, which allows an easier integration and acceptance of them. Our evaluation has presented that nurses and physicians are very interested and open to these kinds of solutions, and consider it very useful, recommending to us to include it also in hospitals.
In future work, this system and insulin therapy model are going to be enhanced with the inclusion of a context management framework (CMF) in order to get additional information about the physical activity, and communication with electronic health record (EHR) from the Hospital Information System (HIS) to get relevant information such as illness, treatments, and drugs. In addition, an identity management system (IdM) is being added to the architecture in order to offer an extended security, privacy, and IdM features to ensure anonymous consultation from external doctors, and patients privacy. Finally, the system is going to be extended to hospitals such as recommended during the evaluation by the nurses and physicians.
References
Diabetes Control and Complications Trial Group (1977) The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes Mellitus. N Engl J Med 329:977–986
Bhargava A (2005) Insulin therapy. Insulin J 4(1):68–69
Berghe GV (2004) How does blood glucose control with insulin save lives in intensive care?. J Clin Investig 114(9):1187–1195
Lehmann ED (1997) Interactive educational simulators in diabetes care. Med Inform 22:47–76
Smith BK, Frost J, Albayrak M, Sudhakar R (2007) Integrating glucometers and digital photography as experience capture tools to enhance patient understanding and communication of diabetes self-management practices. Pers Ubiquitous Comput 11:273–286
Istepanian RSH, Zitouni K, Harry D, Sungoor A, Tang B, Earle KA (2009) Evaluation of a mobile phone telemonitoring system for glycaemic control in patients with diabetes. J Telemed Telecare 15:125–128
Villarreal V, Laguna J, López C, Fontecha J, Fuentes C, Hervás R, López-de-Ipiña D, Bravo J (2009) A proposal for mobile diabetes self-control: towards a patient monitoring framework. IWANN 2:870–877
Jara AJ, Istepanian RSH, Sungoor A, Alcazar N, Zamora M, Skarmeta AFG (2010) Diabetes management and insulin therapy in the hospital and AAL environments based on mobile health. II international workshop on ambient assisted living, Valencia, Spain
Earle KA, Istepanian RSH, Zitouni K, Sungoor A, Tang B (2010) Mobile telemonitoring for achieving tighter targets of blood pressure control in patients with complicated diabetes: a pilot study. Diabetes Technol Ther 12(7):575–579. http://dx.doi.org/10.1089/dia.2009.0090
Istepanian RSH, Jara A, Sungoor A, Philips N (2010) Internet of things for M-health applications (IoMT). AMA-IEEE medical technology conference on individualized healthcare, Washington
Zamora Izquierdo MA, Santa Lozano J, Antonio F, Gómez Skarmeta (2010) An integral and networked home automation solution for indoor ambient intelligence. IEEE Pervasive Comput 9:66–77
Babic B, Nicoletta M, Martin L (2010) Manual de Conteo de Hidratos de Carbono. ADU Uruguay Diabetes Association
Jara AJ, Alcolea AF, Zamora M, Skarmeta AFG (2010) Analysis of different techniques to define metadata structure in NFC/RFID cards to reduce access latency, optimize capacity, and guarantee integrity. 10th IFAC workshop on intelligent manufacturing systems, Lisbon, Portugal
Tentori M, Favela J, González JM (2006) Quality of privacy (QoP) for the design of ubiquitous healthcare applications. J Univers Comput Sci 12(3):252–269
Jara AJ, Zamora MA, Skarmeta AFG (2009) NFC/RFID applications in medicine—security challenges and solutions, 5th international conference on intelligent environments, Barcelona, Spain
Ayuso J, Marin L, Jara AJ, Skarmeta AFG (2010) Optimization of public key cryptography (RSA and ECC) for 8-bits devices based on 6LoWPAN. First international workshop on the security of the internet of things, Tokyo, Japan
Acknowledgments
The authors would like to thank the Spanish ministry for Industry, Tourism and infrastructure, and the ministry for education, social politic and sport for sponsoring the research activities under the grants AIRE (TSI-020302-2010-95) and FPU program (AP2009-3981). This work has been carried out by the Intelligent Systems group of the University of Murcia, awarded as an excellence researching group in frames of the Spanish “Plan de Ciencia y Tecnología de la Región de Murcia” from the “Fundación Séneca” (04552/GERM/06). Finally, thanks to the volunteers, who evaluated this solution, nurses, and physicians: Noemí Alcazar, Fermín Alcolea, José Javier Campuzano, and María Jesús Carrillo, and to the patients: José García and Belinda Herrero.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jara, A.J., Zamora, M.A. & Skarmeta, A.F.G. An internet of things–based personal device for diabetes therapy management in ambient assisted living (AAL). Pers Ubiquit Comput 15, 431–440 (2011). https://doi.org/10.1007/s00779-010-0353-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00779-010-0353-1