
Abstract
Background
We describe a method for the direct application of MR images to navigation-assisted bone tumor surgery as an alternative to CT–MRI fusion.
Method
Six patients with an orthopedic malignancy were employed for this method during navigation-assisted tumor resection. Tumor types included osteosarcoma (4), high-grade chondrosarcoma (1), and adamantinoma (1). Mean patient age was 25.3 years (range 18–52 years). Mean duration of follow-up was 25.8 months (range 18–32 months). Resorbable pin placement and rapid 3-dimensional spoiled gradient echo sequences made the direct application of MR images to computer-assisted bone tumor surgery without CT–MR image fusion possible. A paired-point registration technique was employed for patient-image registration in all patients.
Results
It took 20 min on average to set up the navigation (range 15–25 min). The mean registration error was 0.98 mm (range 0.4–1.7 mm). On histologic examination, distances from tumors to resection margins were in accord with preoperative plans. No patient had a local recurrence or distant metastasis at the last follow-up.
Conclusion
Direct patient-to-MRI registration is a very useful method for bone tumor surgery, permitting the application of MR images to intraoperative visualization without any additional costs or exposure of the patient to radiation from the preoperative CT scan.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The usefulness and accuracy of computer-assisted orthopedic surgery have been evaluated clinically in many fields, such as total joint replacement arthroplasty, cruciate ligament reconstruction, pedicle screw placement, and so on [1–3]. Recently, several preliminary reports have been issued on the application of computer assistance to bone tumor surgery [4–8]. These reports include applications to pelvic bone tumors [6], sacral tumors [4], and joint-preserving limb salvage surgery [5]. Despite improvements in treatment modalities, patients with a malignant tumor in the pelvic girdle are still at high risk of treatment failure because of the inadequacies of surgical margins. Accordingly, the introduction of navigation might help surgeons overcome difficulties in pelvic tumor surgery caused by the complex anatomy of the pelvis. In addition, the accuracy of intraoperative identification by the navigation system makes it possible to preserve the adjacent joint as well as to ensure safe excision of the tumor.
Surgical navigation systems can apply three-dimensional images such as CT and MR images to intraoperative visualization. Although CT is better at describing cortical bone status, MRI is considered the best method for defining the extent of marrow involvement for bone tumors and for planning surgical resection in bone tumor surgery. There have been only two reports on the application of MR imaging to navigation-assisted bone tumor surgery through CT–MR image fusion as far as we know [5, 7]. However, the CT–MRI fusion technique requires additional costs and exposure of the patient to radiation from the preoperative CT, as well as additional time for image fusion. Above all, the image fusion process is a kind of registration (image-to-image registration) that inevitably leads to registration error [9]. Although automatic registration has recently become available, image merging is still commonly carried out based on visual inspection, which has the potential to introduce errors. Herein we describe a new method for the direct application of MR images to navigation-assisted bone tumor surgery as an alternative to CT–MRI fusion. This study was approved by the institutional review board at Kyungpook National University Hospital. All patients included in this study were informed that the cases would be submitted for publication, and they consented.
Patients and methods
We have applied navigation assistance to patients with a pelvic girdle malignancy or a metaphyseal malignancy requiring en bloc resection since February 2005. In terms of metaphyseal lesions, if the residual remaining epiphysis was expected to be >1 cm long after tumor resection with a 1–2 cm surgical margin, and if preoperative chemotherapy was gauged to be effective by imaging studies, joint-preserving surgery was performed with navigation. Tumor responses to preoperative chemotherapy were determined at interdisciplinary sarcoma meetings of medical, surgical and radiation oncologists, radiologists, and pathologists. When tumor response to preoperative chemotherapy was expected to be poor, joint preservation was not considered. Navigation was considered to be contraindicated in skeletally immature patients with a sarcoma of the metaphysis because intraepiphyseal resection can be performed under fluoroscopic guidance. In these cases, an open physis could be used as a landmark for intraepiphyseal osteotomy.
During the early stages of our series, the CT–MR image fusion technique was employed to apply MR images to navigation-assisted bone tumor resection. In the latest 6 cases, we employed a direct MR image registration technique that used resorbable pins. Tumor types included osteosarcoma (4), high-grade chondrosarcoma (1), and adamantinoma (1). Mean patient age was 25.3 years (range 18–52 years). Joint-preserving limb salvage surgery was performed in 3 patients (patient nos. 1, 3, 6), partial joint resection in 2 patients (patient nos. 2, 4), and partial sacrectomy in 1 patient (patient no. 5). Mean duration of follow-up was 25.8 months (range 18–32 months).
The basic concept of this technique is the same as the paired-point registration technique used for CT with metallic Kirschner wires in our previous reports [4, 5], except that this method uses MR images and resorbable pins. The resorbable pins used in the present study were made of poly-p-dioxanone, a biodegradable polymer composite that is fully compatible with MRI. Furthermore, orthopedic bioabsorbable products have low signal intensities in T1- and T2-weighted images and do not cause image blurring [10]. The MR images employed in this study were rapid 3-dimensional spoiled gradient echo sequences. Such a sequence is able to provide a data set with a slice width of 1–3 mm, which made it possible to detect a resorbable pin 1.5 mm in diameter.
Surgical technique
Preoperative preparation
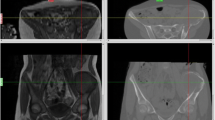
On the first preoperative day, with the patient under local anesthesia in the operating room, three or four resorbable pins (OrthoSorb®, DePuy ACE Medical, Warsaw, IN, USA) were placed as fiducial markers for registration, and then rapid 3-dimensional spoiled gradient echo (TE 3.2 ms, TR 7.6 ms, 1.5 mm slice thickness) axial MR images (1.5 T, Achieva, Philips, Eindhoven, The Netherlands) were acquired (Fig. 1). The pins should be placed beyond what would be the resection area to avoid tumor contamination. The diameter of a resorbable pin is 1.5 mm. Therefore, the thickness of the MR slice should be <1.5 mm so that no pin is missed.

An MR image after resorbable pin placement (arrow). A resorbable pin exhibits a low signal intensity in a rapid 3-dimensional spoiled gradient echo sequence without causing image blurring
Registration technique
The Stryker surgical navigation system (System II: Styker, Kalamazoo, MI, USA) was used in all patients. After conventional surgical dissection for a bone tumor, a dynamic reference base (DRB) was fixed to the cortical bone beyond the planned resection area. Patient-to-image registration was performed by paired-point registration using MR images and resorbable pins that had been placed preoperatively. Registration is a process that correlates some points on a patient’s body with corresponding points on an image. The discrepancy between virtual space on the image and real patient space is referred to as the registration error.
Usually, in order to direct a registration probe to the exact points where resorbable pins penetrated cortical bone, some additional skin incisions may be required around pins (Fig. 2a). However, we used a new registration probe to locate these penetration points, which consisted of a universal tracker and a metallic cannula (FGS Biopsy Probe: Stryker, Kalamazoo, MI, USA) (Fig. 2b). Pushing this registration probe over the pin until contact is made with the cortex of the bone makes it possible to perform registration without completely exposing the points at which the wires penetrate (Fig. 2c, d).

Paired-point registration with resorbable pins as fiducials. a Usually, in order to locate the precise point at which a resorbable pin penetrates cortical bone, additional skin incision and muscle dissection around the wire may be necessary. b We used a new registration probe that consisted of a universal tracker and a metallic cannula. c, d Pushing this registration probe over the pin until contact is made with the cortex of the bone makes it possible to perform registration with a skin incision of just a few millimeters over a pin
Functional evaluation
The functional evaluation of patients was performed using the classification system of the International Society of Limb Salvage, which includes six functional parameters: pain, function, emotional acceptance, use of walking supports, walking ability, and gait. Each parameter is awarded a score ranging from 0 to 5 points, yielding a maximum score of 30 points.
Results
Brief characteristics of and postoperative results for 6 patients are listed in Table 1. The direct patient-to-MRI registration took 20 min on average to set up navigation (range 15–25 min). Mean registration error was 0.98 mm (range 0.4–1.7 mm). In all cases, registration errors were <2 mm. Although a sound analysis was not possible due to the small number of patients, there was no difference in registration error according to anatomical location. On histological examination, distances from tumors to resection margins were in accord with preoperative plans (Figs. 3, 4). No patient had a local recurrence or distant metastasis at the last follow-up. The mean functional score using the classification system of the International Society of Limb Salvage was 27.7 points (range 24–29 points).

A patient (patient no. 4) with osteosarcoma in the medial condyle of the left proximal tibia who underwent unplanned curettage at another hospital. a T1-weighted fat suppression enhanced image shows a residual lesion (arrow). The medial condyle of the proximal tibia was included in the resection (dotted line). b MR images (rapid 3-dimensional spoiled gradient echo) after placement of resorbable pins as fiducial markers for the registration. c The gross specimen, demonstrating an adequate resection as planned. d Plain radiographs at 24 months postoperatively

A patient (patient no. 5) with high-grade chondrosarcoma in the sacrum. a T1-weighted MR image shows a lesion involving the lateral portion of the right upper sacrum. b Resection including an iliac osteotomy, sacrifice of the right S1 nerve root, and sacral osteotomy was planned along the dotted line. c The gross specimen demonstrates that the tumor was resected with an adequate margin (arrows). The S1 nerve root was partially invaded by the tumor (arrowhead). The posterior portion of the ilium (I) and the right S1 nerve root were included in the excised specimen. d Plain radiograph at 20 months postoperatively
Discussion
Basically, there are two main registration methods for navigation-assisted surgery: surface registration and paired-point registration. In the context of bone tumor surgery, CT images can be used for surface registration [8] as well as paired-point registration using metallic Kirschner wires that are placed in cortical bone as fiducials [4–6]. However, MR images cannot be used for surface registration because the navigation system cannot recognize bony surfaces in MR images [5]. Therefore, possible methods of using MR images as intraoperative guides include paired-point registration and CT–MR image fusion. However, performing paired-point registration while keeping the registration error to <1 mm without any fiducial is not easy [4]. Moreover, some prominent osseous points that may be included in the resection area should be excluded from the landmarks for registration in bone tumor surgery. Given these limitations with registering MR images, another approach is to use these images as intraoperative guides by performing CT–MR image fusion. The use of fusion images during computer-assisted bone tumor surgery has been reported by Cho et al. [5] and Wong et al. [7]. However, the image fusion process is associated with image-to-image registration errors, and although automatic registration is now available, image merging is still commonly carried out by visual inspection, so there is the potential for substantial error. The best algorithms can sometimes fail and cause errors as large as 6 mm or more [9].
Paired-point registration using resorbable pins offers an alternative to CT–MRI fusion. The resorbable pins used in this study are made of poly-p-dioxanone, a biodegradable polymer composite that is fully compatible with modern diagnostic methods such as CT and MRI. Furthermore, orthopedic bioabsorbable products have low signal intensities in T1- and T2-weighted images and do not cause image blurring [10]. This method eliminates the errors associated with the image fusion process. In addition, it is less expensive and exposure to radiation during preoperative CT is avoided. Moreover, the times required for the CT scan and the image fusion process are eliminated. Rapid 3-dimensional spoiled gradient echo sequence was employed to get a thin-section thickness data set. This sequence provides information on the differentiation of the tumor/edema, soft tissue involvement and residual viable tumor after chemotherapy in malignant tumor of the long bone [11]. It can also provide a data set with a slice width of 1–3-mm, which makes it possible to detect a resorbable pin 1.5 mm in diameter. During registration, a universal tracker attached to a metallic cannula is used to locate the exact points where resorbable pins penetrate the cortical bone. The inner diameter of the cannula is 1.6 mm, wide enough to fit a resorbable pin. This tracker makes it possible to precisely perform the registration by making just a skin incision of just a few millimeters over the pin. Recently, a case report that described MRI-guided navigation surgery with temporary implantable bone markers was published [12]. The basic concept of the case report is very similar to ours. However, they did not mention the accuracy of the method in terms of registration error. In addition, they reported only one case of distal femoral malignancy with a short follow-up period. In this study, the mean registration error was 0.98 mm (range 0.4–1.7 mm). This result was comparable with other reports using CT-guided navigation-assisted surgery [4, 6, 8]. Moreover, this report included pelvic girdle as well as extremity malignancies, and suggests that the direct application of MR images to navigation-assisted surgery could be an alternative to CT–MRI fusion and applicable to pelvic girdle malignancy.
In our experience, direct patient-to-MRI registration is a very useful method for bone tumor surgery, permitting the application of MR images to intraoperative visualization without any additional costs or exposure of the patient to radiation from the preoperative CT scan, even though the technique has the disadvantage of requiring an additional procedure to place resorbable pins as fiducial markers.
References
Amiot LP, Lang K, Putzier M, Zippel H, Labelle H. Comparative results between conventional and computer-assisted pedicle screw installation in the thoracic, lumbar, and sacral spine. Spine. 2000;25(5):606–14.
Hart R, Krejzla J, Svab P, Kocis J, Stipcak V. Outcomes after conventional versus computer-navigated anterior cruciate ligament reconstruction. Arthroscopy. 2008;24(5):569–78.
Jolles BM, Genoud P, Hoffmeyer P. Computer-assisted cup placement techniques in total hip arthroplasty improve accuracy of placement. Clin Orthop. 2004;426:174–9.
Cho HS, Kang HG, Kim HS, Han I. Computer-assisted sacral tumor resection. A case report. J Bone Joint Surg Am. 2008;90:1561–6.
Cho HS, Oh JH, Han I, Kim HS. Joint-preserving limb salvage surgery under navigation guidance. J Surg Oncol. 2009;100:227–32.
Hufner T, Kfuri M, Galanski M, Bastian L, Loss M, Pohlemann T, Krettek C. New indications for computer-assisted surgery—tumor resection in the pelvis. Clin Orthop. 2004;426:219–25.
Wong KC, Kumta SM, Antonio GE, Tse LF. Image fusion for computer-assisted bone tumor surgery. Clin Orthop. 2008;466:2533–41.
Wong KC, Kumta SM, Chiu KH, Antonio GE, Unwin P, Leung KS. Precision tumour resection and reconstruction using image-guided computer navigation. J Bone Joint Surg Br. 2007;89:943–7.
Pappas IP, Puja M, Styner M, Liu J, Caversaccio M. New method to assess the registration of CT–MR images of the head. Injury. 2004;35(Suppl 1):S-A105–12.
Baidya KP, Ramakrishna S, Rahman M, Ritchie A. Quantitative radiographic analysis of fiber reinforced polymer composites. J Biomater Appl. 2001;15:279–89.
Brisse H, Ollivier L, Edeline V, Pacquement H, Michon J, Glorion C, Neuenschwander S. Imaging of malignant tumours of the long bones in children: monitoring response to neoadjuvant chemotherapy and preoperative assessment. Pediatr Radiol. 2004;34:595–605.
Kim JH, Kang HG, Kim HS. MRI-guided navigation surgery with temporary implantable bone markers in limb salvage for sarcoma. Clin Orthop. 2010;468:2211–7.
Acknowledgments
This study was supported by a Korea Healthcare Technology R&D Project grant from the Ministry for Health, Welfare and Family Affairs, Republic of Korea (A084177). No benefits of any form have been or will be received from a commercial party directly or indirectly relating to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Cho, H.S., Park, IH., Jeon, IH. et al. Direct application of MR images to computer-assisted bone tumor surgery. J Orthop Sci 16, 190–195 (2011). https://doi.org/10.1007/s00776-011-0035-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-011-0035-5