
Abstract
The relationship between hip fracture risk and opioid use remains controversial. Thus, we performed a meta-analysis to assess the risk of hip fracture among opioid users. PubMed and EMBASE were searched for studies published from the inception of the databases until June 2015. The information was extracted independently by two teams of authors. When the heterogeneity was significant, the random-effects model was used to calculate the overall pooled risk estimates. Ten studies with 697,011 patients were included in the final meta-analysis. The overall combined relative risk for the use of opioids and hip fracture was 1.54 [95 % confidence interval (CI) 1.34–1.77]. Subgroup analyses revealed sources of heterogeneity, and sensitivity analysis indicated stable results, and no publication bias was observed. This meta-analysis demonstrates that opioids significantly increase the risk of hip fracture.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hip fracture is a common cause of disability and mortality among the elderly [1]. It is predicted that the number of hip fractures will rise to 6.26 million worldwide by 2050 [2]. Therefore, hip fractures remain a severe public health problem. The risk factors for hip fracture have become an important topic. Several factors may be associated with hip fractures, including cigarette smoking [3], serum estradiol levels [4], serum vitamin D levels [5], and opioid use [6]. Opioids are widely used for their and psychotropic effects and also cause drowsiness, sedation and cognitive impairment, which results in an increased risk of hip fracture [7–10]. However, the misuse of opioids is increasing and frequently results in accidental overdoses and mortality [11]. Therefore, the relationship between opioid use and hip fracture risk warrants attention. Previous studies have described a relationship between opioid use and an increased risk of hip fracture [9, 12–15], whereas others have failed to demonstrate a significant increase in the risk of fracture in the setting of opioid use [16, 17]. A previous meta-analysis [8] suggested that opioids are associated with a 36 % increase in the risk of hip fracture. However, only a small number of studies on opioids were included in this analysis, which did not allow for firm conclusions because of the potential for both heterogeneity and publication bias [8]. A previous meta-analysis by Teng et al. [6] demonstrated that opioids cause a two-fold increase in the risk of hip fracture; however, only three cohort studies on opioids were included in their analysis.
Therefore, the relationship between hip fracture risk and opioid use remains controversial. Thus, we performed an updated meta-analysis to assess the risk of hip fracture among opioid users.
Materials and methods
Search strategy and data sources
We searched MEDLINE (PubMed) and EMBASE (1947 to June 24, 2015) for observational studies describing the relationship between opioid use and hip fracture risk, without restrictions. We also searched the bibliographies of the retrieved articles to identify additional studies. We used the following search terms—(1) fracture*[Title/Abstract] OR ‘Fractures, Bone’[Mesh] OR ‘Hip fractures’[Mesh] OR Hip fracture*[Title/Abstract], and (2) opioid*[Title/Abstract] OR ‘Analgesics, Opioid’[Mesh].
Study selection
Studies were considered eligible if they met the following criteria—(1) presented original data from a cohort study or a case–control study or a case-crossover study, (2) evaluated the relationship between opioid use and hip fracture incidence, (3) studied opioids as the exposure of interest, and (4) provided relative risks, odds ratios, hazard ratios (HRs) or adjusted relative risks (RRs) and corresponding 95 % confidence intervals (CIs). If the data were duplicated or the population was studied in more than one study, we included the study with the largest sample size and the most comprehensive outcome evaluation.
Data extraction and quality assessment
Two teams of investigators (FP, YW, JW, JC, WZ, YL, and HZ) independently evaluated the eligibility of the studies based on the pre-determined selection criteria. Additionally, a cross-reference search of eligible articles was conducted to identify studies not found during the computerized search. The two teams of authors independently extracted the following data—the first author’s name, the year of publication, age of the patients, study regions, years of follow-up, study design, HR or RR or OR and 95 % CIs, and statistical adjustments for confounding factors. Any disagreements were resolved by discussion or in consultation with the co-corresponding authors (YL and HZ).
Statistical analyses
We investigated the relationship between the use of opioids and the risk of hip fracture using adjusted data for the primary analyses. We computed a pooled RR and 95 % CI from the adjusted RRs or HRs or ORs and 95 % CIs reported in the studies. The HRs or ORs were considered corresponding variables to the RRs. The Cochran Q and I 2 statistics were used to evaluate the statistical heterogeneity [18]. When the P value was <0.1 and the I 2 value was >50 %, the data were considered heterogeneous, and a random-effects model (Der-Simonian and Laird method) [19] was utilized because it represented a more conservative approach to the calculation of a weighted estimate effect using an RR. Otherwise, a fixed-effects model [20] was used to estimate the overall summary effect sizes when no heterogeneity was present in the included studies. To further explore the origin of the heterogeneity, we also performed subgroup analyses of study design and study region before performing additional analyses. For the cohort studies, we performed a subgroup meta-analysis of prospective and retrospective cohort studies.
Data analysis
To assess the stability of our results, a sensitivity analysis (by excluding each single study in turn) was conducted to estimate the influence of individual studies on the pooled result. We used Egger’s test (linear regression method) [21] and Begg’s test (rank correlation method) [22] to assess the potential for publication bias.
Results
Literature search and study characteristics
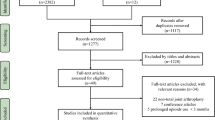
A total of 1,264 articles were identified in the initial search. Of these, 1,242 were excluded after reviewing the titles and abstracts and removing duplicates and irrelevant articles. Twenty-two relevant studies remained for further review. After thoroughly reading the full text of each study, we excluded 12 studies without data on the risk of hip fracture. We included ten studies with 697,011 patients in our final analysis (Fig. 1) [9, 12–17, 23–25]. Of the ten studies, four [14, 17, 23, 24] were case–control studies, four [12, 13, 16, 25] were prospective cohort studies, one [9] was a retrospective cohort study, and one [15] was a case-crossover study. Two [16, 25] studies were from the United States, two [17, 24] were from Denmark, two [9, 12] were from Sweden, two [13, 14] were from the United Kingdom, one [23] was from Canada, and one [15] was from Australia. The general characteristics of the studies are summarized in Table 1.

Flow chart illustrating the literature search for studies on the association between opioids and hip fracture
Primary analysis
The meta-analysis of the ten studies, which included 697,011 individuals, demonstrated a significant, positive correlation between opioid use and hip fracture risk (RR 1.54, 95 % CI 1.34–1.77). Additionally, substantial heterogeneity was observed (P = 0.000, I 2 = 84.6 %) (Fig. 2).

Forest Plot of RR with CI for opioid use and hip fracture risk according to subgroup meta-analysis by study design in a random-effects model
Subgroup meta-analysis
A subgroup meta-analysis was performed according to study design. We observed a significant, positive correlation between opioid use and hip fracture risk in both the case–control and the cohort studies. However, substantial heterogeneity was also observed in each type (case–control: P = 0.085, I 2 = 54.6 %; cohort: P = 0.005, I 2 = 73.0 %) (Fig. 2). For the cohort studies, we subsequently performed a subgroup meta-analysis of the prospective and retrospective cohort studies and observed a significant, positive correlation between opioid use and hip fracture risk in the prospective cohort studies. No statistical heterogeneity was observed in the prospective cohort group (P = 0.265, I 2 = 24.4 %) (Fig. 3). For the case–control studies, after omitting a single [23] study, we observed a significant, positive correlation between opioid use and hip fracture risk, and no heterogeneity was observed (Fig. 4).

Forest Plot of RR with CI for opioid use and hip fracture risk according to subgroup meta-analysis by prospective and retrospective cohort studies in a random-effects model

Forest Plot of RR with CI for opioid use and hip fracture risk according to case–control studies after omitting one study in a fixed-effects model
The subgroup analysis by region demonstrated a significantly increased fracture risk in conjunction with the use of opioids. However, substantial heterogeneity was also observed in both the European group and American group (Europe: P = 0.075, I 2 = 50.0 %; America: P = 0.007, I 2 = 79.6 %) (Fig. 5). In the American group, after omitting a single study [25], we observed a significant correlation between opioid use and hip fracture risk, and no heterogeneity was observed (Fig. 6).

Forest Plot of RR with CI for opioid use and hip fracture risk according to subgroup meta-analysis by region in a random-effects model

Forest Plot of RR with CI for opioid use and hip fracture risk according to America studies after omitting one study in a fixed-effects model
A subgroup analysis was performed according to the above analysis. We assigned one case-crossover study [15] and three studies [9, 23, 25], which may have contributed to the above-mentioned heterogeneity, to group 1; the other studies were assigned to group 2. We observed a significant, positive correlation between opioid use and the risk of hip fracture in group 1. No statistical heterogeneity was observed in group 1 (Fig. 7).

Forest Plot of RR with CI for opioid use and hip fracture risk according to subgroup meta-analysis by two groups in a random-effects model
Sensitivity analysis
To evaluate the robustness of our analysis, we conducted a sensitivity analysis by recalculating the pooled results of the primary analysis by excluding one study per iteration. The outcome demonstrated that the exclusion of any single study did not alter the overall combined result (Fig. 8).

Sensitivity analysis of the relationship between opioid use and hip fracture risk
Publication bias
The Begg rank correlation test and the Egger linear regression test demonstrated no evidence of publication bias among the studies (Begg, P > |z| = 1.000; Egger, P = 0.713, 95 % CI −4.45 to 3.19) (Figs. 9, 10).

Egger’s publication bias plot

Begg’s funnel plot of the 10 studies
Discussion
This meta-analysis demonstrated a significant positive correlation between opioid use and the risk of hip fracture (RR 1.54, 95 % CI 1.34–1.77). These findings are comparable with a meta-analysis by Teng et al. [6], which demonstrated a significantly increased risk of hip fracture secondary to opioid use. Additionally, our results are comparable with those of meta-analyses analyzing the relationships between other factors and hip fracture risk. For instance, a study by Wu et al. [26] reported that high vitamin A intake and retinol increased the risk of hip fracture. Furthermore a study by Shen et al. [3] revealed that cigarette smoking may play an important modifiable role in the development of hip fracture (RR 1.30, 95 % CI 1.16–1.45), and a study by Takkouche et al. [8] reported a significant positive correlation between the use of psychotropic medications and the risk of hip fracture. Additional studies on opioid medications have suggested that opioids are associated with a 31 % increase in hip fracture risk (RR 1.31, 95 % CI 1.24–1.40). However, only six trials were included in the study by Takkouche et al., which did not allow for conclusions to be drawn because of the potential for both heterogeneity and publication bias. In the meta-analysis by Teng et al., the pooled results indicated that opioids contribute significantly to the risk of hip fracture (RR 2.00, 95 % CI 1.84–2.19); however, only four cohort studies with 471,795 patients were included. In the present study, we performed a meta-analysis including ten studies with 697,011 patients to evaluate the relationship between opioid use and hip fracture risk. Substantial heterogeneity was also observed; however, the findings were stable and robust based on our sensitivity analysis.
Opioids are widely used for their analgesic and psychotropic effects, which may cause dizziness, drowsiness, sedation and cognitive impairment, resulting in an increased risk of hip fracture [7–10]. Additionally, as discussed previously [6], opioids may affect the endocrine system, mediating the suppression of both innate and acquired immunity, and may decrease bone mineral density, which may weaken bone structure by interfering with bone metabolism [27–29]. As elderly persons are susceptible to both osteoporosis and pain, the opioids used to treat pain in this population may also increase the risk of subsequent hip fractures.
Heterogeneity was observed in this meta-analysis. First, we performed a subgroup analysis by study design. We subsequently analyzed each subgroup. For example, regarding the cohort group, we performed a subgroup analysis in which the prospective cohort studies were assigned to one group, and the retrospective cohort studies were assigned to another group. We observed that the retrospective cohort studies [9] may have contributed to the above-mentioned heterogeneity. Regarding the case–control group, we omitted a study [23] and observed that the heterogeneity disappeared in the case–control group, which indicated that this study [23] may have introduced the heterogeneity. After carefully reading the original studies, we observed that this study [23] focused on only two types of opioids (codeine and propoxyphene). Therefore, the types of the opioids used may have introduced the heterogeneity. Second, we performed a subgroup analysis by region. We analyzed the American group after omitting one study [25] and observed that the heterogeneity disappeared, which indicated that the study [25] contributed to the heterogeneity. A possible reason for the heterogeneity may have been the inclusion of studies conducted in different regions. Third, we omitted three studies [9, 23, 25] that may have contributed to the heterogeneity before performing the meta-analysis. However, we still observed substantial heterogeneity. After excluding a case-crossover study [15], we observed that the heterogeneity disappeared, which indicated that the study [15] contributed to the heterogeneity. We ultimately surmised that four studies [9, 15, 23, 25] played a key role in the heterogeneity. Therefore, study design, region and the type of opioid used may increase heterogeneity. Identifying the source of heterogeneity was important for our meta-analysis.
The combined result of our meta-analysis was stable and robust according to our sensitivity analysis, and publication bias was not observed. However, previous meta-analyses evaluating the relationship between opioid use and hip fracture risk did not perform a sensitivity analysis or test for publication bias. Therefore, their results are ambiguous.
A major strength of our study was that compared with the original included studies, the increased number of participants enhanced the power to identify a significant positive correlation between opioid use and fracture risk and provided more precise estimates of the effects of opioid use. Most of the studies had large sample sizes and accurate outcome assessments. Additionally, although a high I 2 (84.6 %) was present for hip fracture risk, we identified heterogeneity sources by performing subgroup analyses.
Despite the advantages of this study, some limitations must also be discussed. First, although we searched for all possible studies describing the relationship between opioids and hip fractures, study eligibility was limited to studies published in English. Additionally, we may have missed studies that were excluded from the computer databases used in our search. Second, although we did not observe publication bias, publication bias could not be completely ruled out. Therefore, the pooled effect measure may not have been absolutely precise. Third, although the sources of the heterogeneity were identified, several other factors may have contributed to its development, including ethnicity, opioid dose, participant education level, socioeconomic class and confounding variables. We will evaluate these factors in the future when the necessary data are available. Fourth, as was the case with the results of the previous study, these results cannot be generalized to other populations, particularly Asian populations. Therefore, studies on Asian populations are necessary. Fifth, some limitations described in the study by Teng et al. [6] persisted in this study. For example, we were unable to determine hip fracture timing. Hence, additional research on hip fracture timing is needed. Finally, the quality of the included studies was not evaluated, and no high-quality original studies, such as randomized controlled trials, have been published. Therefore, large randomized controlled trials and higher quality analyses remain necessary as additional relevant data become available.
In conclusion, our meta-analysis demonstrates that opioid use may significantly increase hip fracture risk. Further higher quality studies, such as randomized controlled trials, especially dose–response studies that research opioids and hip fracture, are urgently required.
References
Parker MJ, Pryor GA (1993) Hip fracture management. Blackwell Scientific Publications, Oxford
Cooper C, Campion G, Melton L III (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2:285–289
Shen GS, Li Y, Zhao G et al (2015) Cigarette smoking and risk of hip fracture in women: a meta-analysis of prospective cohort studies. Injury 46:1333–1340
Kanungo J, Cuevas E, Guo X et al (2012) Nicotine alters the expression of molecular markers of endocrine disruption in zebrafish. Neurosci Lett 526:133–137
Gumieiro DN, Murino Rafacho BP, Buzati Pereira BL et al (2015) Vitamin D serum levels are associated with handgrip strength but not with muscle mass or length of hospital stay after hip fracture. Nutrition 31:931–934
Teng Z, Zhu Y, Wu F et al (2015) Opioids contribute to fracture risk: a meta-analysis of 8 cohort studies. PLoS One 10:e0128232
Stewart G, Owen M (2013) Opioids in the management of persistent non-cancer pain. Anaesth Intensive Care Med 14:533–535
Takkouche B, Montes-Martínez A, Gill SS et al (2007) Psychotropic medications and the risk of fracture. Drug Saf 30:171–184
Thorell K, Ranstad K, Midlöv P et al (2014) Is use of fall risk-increasing drugs in an elderly population associated with an increased risk of hip fracture, after adjustment for multimorbidity level: a cohort study. BMC Geriatr 14:131
Lindestrand AG, Christiansen MLS, Jantzen C et al (2015) Opioids in hip fracture patients: an analysis of mortality and post hospital opioid use. Injury 46:1341–1345
Compton WM, Volkow ND (2006) Major increases in opioid analgesic abuse in the United States: concerns and strategies. Drug Alcohol Depend 81:103–107
Guo Z, Wills P, Viitanen M et al (1998) Cognitive impairment, drug use, and the risk of hip fracture in persons over 75 years old: a community-based prospective study. Am J Epidemiol 148:887–892
Card T, West J, Hubbard R et al (2004) Hip fractures in patients with inflammatory bowel disease and their relationship to corticosteroid use: a population based cohort study. Gut 53:251–255
Li L, Setoguchi S, Cabral H et al (2013) Opioid use for noncancer pain and risk of fracture in adults: a nested case–control study using the general practice research database. Am J Epidemiol 178:559–569
Leach MJ, Pratt NL, Roughead EE (2015) Psychoactive medicine use and the risk of hip fracture in older people: a case-crossover study. Pharmacoepidemiol Drug Saf 6:576–582
Ensrud KE, Blackwell T, Mangione CM et al (2003) Central nervous system active medications and risk for fractures in older women. Arch Intern Med 163:949–957
Jensen J, Nielsen L, Lyhne N et al (1991) Drugs and femoral neck fracture: a case–control study. J Intern Med 229:29–33
Higgins J, Thompson SG, Deeks JJ et al (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Woolf B (1955) On estimating the relation between blood group and disease. Ann Hum Genet 19:251–253
Egger M, Smith GD, Schneider M et al (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50:1088–1101
Shorr RI, Griffin MR, Daugherty JR et al (1992) Opioid analgesics and the risk of hip fracture in the elderly: codeine and propoxyphene. J Gerontol 47:M111–M115
Vestergaard P, Rejnmark L, Mosekilde L (2006) Fracture risk associated with the use of morphine and opiates. J Intern Med 260:76–87
Kamal-Bahl SJ, Stuart BC, Beers MH (2006) Propoxyphene use and risk for hip fractures in older adults. Am J Geriatr Pharmacother 4:219–226
Wu AM, Huang CQ, Lin ZK et al (2014) The relationship between vitamin A and risk of fracture: meta-analysis of prospective studies. J Bone Miner Res 29:2032–2039
Vuong C, Van Uum SH, O’Dell LE et al (2010) The effects of opioids and opioid analogs on animal and human endocrine systems. Endocr Rev 31:98–132
Vallejo R, de Leon-Casasola O, Benyamin R (2004) Opioid therapy and immunosuppression: a review. Am J Ther 11:354–365
Ricardo Buenaventura M, Rajive Adlaka M, Nalini Sehgal M (2008) Opioid complications and side effects. Pain Physician 11:S105–S120
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
There are no identified conflicts of interest with any of the authors.
About this article

Cite this article
Ping, F., Wang, Y., Wang, J. et al. Opioids increase hip fracture risk: a meta-analysis. J Bone Miner Metab 35, 289–297 (2017). https://doi.org/10.1007/s00774-016-0755-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-016-0755-x