
Abstract
This study investigated the current incidence of hip fractures in Okinawa prefecture and compared the data with those obtained in our previous study, which was conducted using similar methods in 1987/1988. All patients, aged 50 years or older and residing in Okinawa, admitted to Okinawa hospitals in 2004 for a fresh hip fracture were identified from hospital registries. Details were obtained from the medical records and radiographs of all patients and classified according to fracture type (cervical or trochanteric), age, sex, and fracture location. Subtrochanteric fractures and pathological fractures were excluded. A total of 1,349 patients (242 men and 1,107 women) were admitted for a fresh hip fracture in 2004. Their average age was 76.9 years for men and 82.4 years for women. There were 671 cervical fractures, 654 trochanteric fractures, and 24 unclassified proximal femoral fractures. Comparing the data from 1987/1988 to those from 2004, the total number of hip fractures increased by 188%, from 469 to 1,349. The age-adjusted incidence rates per 100,000, standardized to the 2000 US population, were 75.7 and 296.1 in 1987/1988 and 123.6 and 420 in 2004 for men and women, respectively. The incidence rates in all age groups (at 5-year intervals) were higher in 2004 than in 1987/1988, indicating that people 50 years of age or older became more susceptible to hip fractures. Accordingly, the accretion of the hip fracture incidence rate was greater than that which could be explained purely by changes in population size and structure.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hip fractures are probably the most serious consequence of osteoporosis [1]. About half of previously independent elderly patients who develop hip fractures become partly or completely dependent on others for activities of daily living, and an increased rate of mortality has been observed within the first year after the fracture [2–4]. Therefore, the prevention of hip fractures is important for the elderly in maintaining a healthy life expectancy. However, the incidence rate of hip fractures increases exponentially with age, and the absolute number of fractures is still expected to rise due to population aging [5].
We need to clarify current epidemiological data on hip fractures at both national and prefectural levels for health care planning, particularly targeting fracture prevention. It is well known that the incidence of hip fracture varies substantially among countries, with higher rates being reported in Norway, Finland, the US and Western Europe, and lower rates in East Asia and Africa [6–9]. Although the age-adjusted incidence rates of hip fractures over the past several decades have increased in many countries [10, 11], recent studies in Canada, the US, Finland, and Norway have shown that they are no longer increasing [12–15].
Okinawa is well suited for an epidemiological study of hip fractures. Japan has the longest life expectancy in the world, and Okinawa has been shown to have Japan’s longest life expectancy for women since 1975. It has also been reported that Okinawa has the highest population of centenarians in the world [16]. Moreover, Okinawa prefecture, a chain of subtropical islands, is located northeast of Taiwan, east of China, and south of mainland of Japan. Because of its geographical situation, virtually all hip fractures occurring in the area are referred to local hospitals.
The purpose of this study was to investigate the current incidence of hip fractures in a population of men and women aged 50 years and older, and compare the data with our previous study, conducted using the same methods in 1987/1988 [17]. Hip fracture patients were identified from medical records of all the hospitals located in Okinawa prefecture. Although this study may have limitations, the data represent an accurate estimate of the occurrence of hip fracture in Okinawa.
Materials and methods
The subjects of this study were patients in Okinawa who had a new hip fracture between 1 January 2004 and 31 December 2004. Only patients residing in Okinawa and aged 50 years or older at the time of fracture were included. Cervical and trochanteric fractures were included, while subtrochanteric fractures and pathological fractures were excluded. All hospitals with orthopedic wards in Okinawa cooperated in this survey. Because Okinawa Prefecture consists of islands, all patients sustaining a hip fracture are referred to hospitals located within the prefecture. This fact makes Okinawa suitable for epidemiological studies of this type.
Lists of registered and computerized diagnoses were used to identify patients admitted to hospitals with hip fractures. Medical records and radiographs for all identified patients were retrieved, and the diagnoses were verified. Patients with two different fractures within the observation period had both fractures recorded. For patients who were re-admitted for the same fracture, only the first admissions were recorded. The patients’ sex, date of birth, type of fracture (cervical or trochanteric), date, and the location of the fracture were recorded.
The patients were subdivided into age groups at 5-year intervals according to sex and fracture type. Age- and sex-specific incidence rates for hip fractures were calculated and expressed as the number of cases per 100,000 person-years. The age- and sex-specific incidence rates were then applied to those of the US population in 2000 to calculate age-adjusted rates of hip fractures. The cervical-to-trochanteric ratio (C/T ratio) was also determined by dividing subjects into age groups at 5-year intervals. For comparison with our previous study [17], we included data from 1 January 1987 to 31 December 1988, collected following the same principle. The data were expressed as an average of 2 years.
In Japan, a national census is performed every 5 years. The most recent census was performed on 1 October 2005. An estimated annual midyear population of the age groups at 5-year intervals used in the present study can be calculated by interpolation from census data.
Student’s t test and Mentel–Haenszel test were used for statistical analysis. P values less than 0.05 were considered to be significant. All calculations were carried out using JMP version 8 (SAS Institute Inc., Cary, NC).
Results
A total of 1,349 fresh cases of hip fracture were recorded in 2004: 242 in men and 1,107 in women (Table 1), with a mean age of 76.9 and 82.4 years, respectively. Men were 5.5 years younger than women on average. The ratio of men to women was 1:4.6. Sixteen patients were omitted from the Table 1 and Fig. 1, because their ages were unknown.

Number of hip fractures in each age group in 2004. The number of fractures in both sexes tended to increase up to age 80–89 years and then decrease
The number of fractures in men increased gradually up to age 85–89 years and then decreased after 90 years. The number of fractures in women increased dramatically and reached its peak at age 80–89 years, and then decreased (Fig. 1). Fractures that occurred after the age of 80 years accounted for 68% of cases in women and 45% of cases in men.
Fractures were approximately equally distributed between the right (48%) and left (52%) sides. The number of patients with fractures on both sides during the 1-year study period was five. Sixty-five percent of the fractures occurred indoors, 17% outdoors, and 18% were not specified in the medical records.
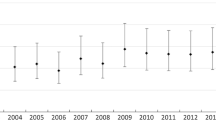
The numbers of cervical and trochanteric fractures in 2004 are given in Table 2. Of all hip fractures, 671 were cervical, 654 were trochanteric, and 24 were undetermined. The cervical-to-trochanteric (C/T) ratio was 1.23 in men and 0.98 in women. Women sustained more trochanteric fractures than men. The mean ages at the time of fracture were 77.8 and 75.9 years for cervical and trochanteric fractures, respectively, in men, and 80.1 and 84.7 years, respectively, in women. Women with trochanteric fractures were older than those with cervical fractures. In women, the C/T ratio decreased gradually with age, whereas it did not change in men (Fig. 2).

Ratio of cervical and trochanteric fractures in 2004. Men sustained more cervical fractures than trochanteric fractures whether or not they were over 75 years old. On the other hand, women sustained more trochanteric fractures with age
A total of 469 fresh hip fractures were recorded in 1987/1988: 74 in men and 395 in women, with a mean age of 77.5 and 80.4 years, respectively (Table 3). The ratio of men to women was 1:5.3. Thus, the number of hip fractures increased by 227% in men and 181% in women, for a combined increase of 188% in 2004.
The population aged 50 years and older increased from 286,000 (men 125,000; women 161,000) in 1987/1988 to 454,000 (men 210,000; women 244,000) in 2004 (Tables 1, 3). As the number of people 65 years and over increased, their proportion of the total population increased from 9.4% in 1987/1988 to 15.3% in 2004. There were considerable demographic changes within certain age strata, which were of importance for fracture incidence. The number of women over 85 years old increased by 140% and that of men increased by 100%; increases in the 55–59-year age group were 11 and 24% for women and men, respectively.
An exponential increase in the incidence rate of hip fractures by age was observed for both sexes (Tables 1, 3). More women than men sustained hip fractures in all age groups. The sex-specific age-adjusted incidence rates per 100,000, standardized to the 2000 US population, were 75.7 and 296.1 in 1987/1988 and 123.6 and 420 in 2004 for men and women, respectively. The age-adjusted incidence rate increased by 63% in men and 42% in women (P < 0.05%).
Discussion
Investigation of the incidence rate of hip fracture in Okinawa was relevant. Since 1975, Okinawa has ranked number one in Japan for female life expectancy, while Japan itself has the longest life expectancy in the world. The mean age of elderly people with a hip fracture in Okinawa was higher than that previously reported in other countries [9, 18–20], especially for women. This is thought to be a reflection of the increased life expectancy. The hip fracture mean age changed from 77.5 years in 1987/1988 to 76.9 years in 2004 for men, and from 80.4 to 82.4 years for women. In the meantime, the mean life expectancy in Okinawa for men rose from 76.6 years in 1990 to 78.6 years in 2005 and from 84.4 years to 86.8 years for women.
The Okinawa population of people 50 years and older increased from 286,000 (men 125,000; women 161,000) in 1987/1988 to 454,000 (men 210,000; women 244,000) in 2004, amounting to a 68% increase in men and a 52% increase in women. The number of hip fractures in Okinawa during the same period increased from 74 to 242 in men and from 395 to 1,107 in women, amounting to 227 and 180% increases in men and women, respectively. Moreover, the sex-specific age-adjusted incidence rates per 100,000 standardized to the 2000 US population, also increased from 75.7 to 123.6 in men and from 296.1 to 420 in women, amounting to a 63% increase in men and a 42% increase in women. Surprisingly, the incidence rates in all age groups (at 5-year intervals) were higher in 2004 than in 1987/1988. Thus, elderly people 50 years of age and older were more susceptible to hip fracture in 2004 than in 1987/1988.
In this study, we found that the incidence rate of hip fractures increased considerably compared with previous data collected 17 years earlier. Although many studies have indicated that the overall number of hip fractures will increase as the population ages [5–11], the increment in Okinawa was greater than could be accounted for by demographic changes alone. This suggests the existence of factors other than aging. However, the actual reasons for the rising hip fracture incidence rate have not been identified. Proper use of recent advances in the identification of risk factors could be utilized to clarify potential causes for the rising hip fracture incidence rate. For example, various risk assessments have been developed based on risk factors, such as low bone mineral density, age, sex, prior fracture, family history, and body mass index [21]. Hip fractures are the most frequent type of fall-related injury, and risk factors for falls include age, muscle weakness, functional limitation, declined cognitive ability, environmental hazards, and a history of falls [22, 23]. There might be the possibility that persons with a high risk of osteoporotic fracture increased in 2004 compared to 1987/1988.
The incidence rate of hip fractures varies from region to region. The difference in incidence rates between countries or regions of countries can be ascribed to racial, cultural, and lifestyle factor [24]. The incidence rate in Okinawa was higher than those of other Japanese prefectures, such as Niigata [25] and Tottori [26], although it was lower than in Western countries [6, 14, 15]. Okinawa is known to have highest rate of obesity in young people in Japan, and increased morbidity of lifestyle-related disease [27, 28], such as heart disease, stroke, and diabetes, might increase the risk of hip fracture. Lifestyle changes within the geographical area could influence the hip fracture incidence rates.
It is important to investigate incidence rates at periodic intervals in order to identify trends over time and to assess osteoporosis prevention strategies. A major limitation of our study is that, as we only compared incidence rates between 1987/1988 and 2004, we were not able to analyze incidence rate trends over the whole time period in order to clarify recent changes. The hip fracture incidence rate has reached a plateau or even declined in some countries. For example, there has been a change in the trend in Scandinavian countries, where a further increase in the incidence rate was not found [14, 15]. In the US, the time trend is toward declining age-adjusted incidence rates [13].
It is important to consider the etiological difference between cervical and trochanteric fractures in developing appropriate approaches to the prevention of hip fractures, because trochanteric fractures are more closely related to osteoporosis and advancing age than cervical fractures [29–32]. Previous studies have compared the C/T ratios between countries and regions [7–11, 17–20, 25]. Many recent studies indicate that trochanteric fractures have increased more than cervical fractures [18, 25]. The present study also indicates that incidence rates of trochanteric fractures increase according to age, especially for women. The exponential increase in hip fracture incidence rates with aging could be related to decreasing bone mineral density and an increasing tendency to fall, especially in older patients with trochanteric fractures [6, 33].
Hip fracture should not be regarded as unavoidable event for a longer life. Thus, it is important to develop effective approaches for preventing or treating osteoporosis and for reducing the frequency of falling in order to decrease the incidence rate of hip fractures. José et al. [34] reported that, over a period of 14 years in Spain, the number of trochanteric fractures decreased and that of cervical fractures increased. They believed that the increase in osteoporosis drug use, the growth in the proportion of people older than 65 years engaging in physical activity, and the increase in average height caused a decrease in trochanteric fractures.
A major strength of this study was the availability of the data on hip fractures taken from the comprehensive hospital records of Okinawan patients. Our results include almost all incidents of hip fractures in Okinawa because all patients are admitted to local hospitals.
In conclusion, this study provided absolute numbers and age-adjusted incidence rates of hip fractures for Okinawa. These showed a dramatic increase compared with our previous data. It will be important to periodically investigate fracture incidence data to clarify trends in order to develop an effective strategy for the prevention of hip fractures.
References
Melton LJ 3rd (2003) Adverse outcomes of osteoporotic fractures in the general population. J Bone Miner Res 18:1139–1141
Farahmand BY, Michaëlsson K, Ahlbom A, Ljunghall S, Baron JA (2005) Survival after hip fracture. Osteoporos Int 12:1583–1590
Tsuboi M, Hasegawa Y, Suzuki S, Wingstrand H, Thorngren KG (2007) Mortality and mobility after hip fracture in Japan: a ten-year follow-up. J Bone Joint Surg Br 89:461–466
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 12:1726–1733
Melton LJ 3rd (1996) Epidemiology of hip fractures: implications of the exponential increase with age. Bone 18(3 Suppl):121S–125S
Cummings SR, Melton LJ 3rd (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
El Maghraoui A, Koumba BA, Jroundi I, Achemlal L, Bezza A, Tazi MA (2005) Epidemiology of hip fractures in 2002 in Rabat, Morocco. Osteoporos Int 16:597–602
Clark P, Lavielle P, Franco-Marina F, Ramírez E, Salmerón J, Kanis JA, Cummings SR (2005) Incidence rates and life-time risk of hip fractures in Mexicans over 50 years of age: a population-based study. Osteoporos Int 16:2025–2030
Lesić A, Jarebinski M, Pekmezović T, Bumbasirević M, Spasovski D, Atkinson HD (2007) Epidemiology of hip fractures in Belgrade, Serbia Montenegro, 1990–2000. Arch Orthop Trauma Surg 127:179–183
Shao CJ, Hsieh YH, Tsai CH, Lai KA (2009) A nationwide seven-year trend of hip fractures in the elderly population of Taiwan. Bone 44:125–129
Giversen IM (2006) Time trends of age-adjusted incidence rates of first hip fractures: a register-based study among older people in Viborg County, Denmark, 1987–1997. Osteoporos Int 17:552–564
Jaglal SB, Weller I, Mamdani M, Hawker G, Kreder H, Jaakkimainen L, Adachi JD (2006) Population trends in BMD testing, treatment, and hip and wrist fracture rates: are the hip fracture projections wrong? J Bone Miner Res 20:898–905
Newman ED, Ayoub WT, Starkey RH, Diehl JM, Wood GC (2003) Osteoporosis disease management in a rural health care population: hip fracture reduction and reduced costs in postmenopausal women after 5 years. Osteoporosis Int 14:146–151
Kannus P, Niemi S, Parkkari J, Palvanen M, Vuori I, Järvinen M (2006) Nationwide decline in incidence of hip fracture. J Bone Miner Res 21:1836–1838
Bjørgul K, Reikerås O (2007) Incidence of hip fracture in southeastern Norway: a study of 1,730 cervical and trochanteric fractures. Int Orthop 31:665–669
Willcox BJ, Willcox DC, Suzuki M (2001) The Okinawa Program: how the World’s longest-lived people achieve everlasting health and how you can too. Three Rivers Press, New York
Yoshikawa T, Norimatsu H (1991) Epidemiology of osteoporosis in Okinawa. J Bone Miner Metab 9(Suppl):135–145
Lönnroos E, Kautiainen H, Karppi P, Huusko T, Hartikainen S, Kiviranta I, Sulkava R (2006) Increased incidence of hip fractures. A population based-study in Finland. Bone 39:623–627
Yan L, Zhou B, Prentice A, Wang X, Golden MH (1999) Epidemiological study of hip fracture in Shenyang, People’s Republic of China. Bone 24:151–155
de Pina MF, Alves SM, Barbosa M, Barros H (2008) Hip fractures cluster in space: an epidemiological analysis in Portugal. Osteoporos Int 19:1797–1804
Yoshimura N, Suzuki T, Hosoi T (2005) Epidemiology of hip fracture in Japan: incidence and risk factors. J Bone Miner Metab 23(Suppl):78–80
Dargent-Molina P, Favier F, Grandjean H, Schott A M, Hausherr E, Meunier P J, Bréart G, for EPIDOS Group (1996) Fall-related factors and risk of hip fracture: the EPIDOS prospective study. Lancet 348:145–149
Matsuueda M, Ishii Y (2000) The relationship between dementia score and ambulatory level after hip fracture in the elderly. Am J Orthop 29:691–693
Moayyeri A, Soltani A, Larijani B, Naghavi M, Alaeddini F, Abolhassani F (2006) Epidemiology of hip fracture in Iran: results from the Iranian Multicenter Study on Accidental injuries. Osteoporos Int 17:1252–1257
Morita Y, Endo N, Iga T, Tokunaga K, Ohkawa Y (2002) The incidence rate of cervical and trochanteric fractures of the proximal femur in 1999 in Niigata Prefecture, Japan. J Bone Miner Metab 20:311–318
Hagino H, Katagiri H, Okano T, Yamamoto K, Teshima R (2005) Increasing incidence of hip fracture in Tottori Prefecture, Japan: trend from 1986 to 2001. Osteoporos Int 16:1963–1968
Takasu N, Yogi H, Takara M, Higa M, Kouki T, Ohshiro Y, Mimura G, Komiya I (2007) Influence of motorization and supermarket-proliferation on the prevalence of type 2 diabetes in the inhabitants of a small town on Okinawa, Japan. Intern Med 46:1899–1904
Shimabukuro M (2009) “26 shock” and management to the metabolic syndrome in Okinawa (in Japanese). Pharma Medica 27:67–72
Michaëlsson K, Weiderpass E, Farahmand BY, Baron JA, Persson PG, Zidén L, Zetterberg C, Ljunghall S (1999) Differences in risk factor patterns between cervical and trochanteric hip fractures. Osteoporos Int 10:487–494
Mautalen CA, Vega EM (1993) Different characteristics of cervical and trochanteric hip fractures. Osteoporos Int (Suppl):102–106
Mautalen CA, Vega EM, Einhorn TA (1996) Are the etiologies of cervical and trochanteric hip fractures different? Bone 18(Suppl):133S–137S
Löfman O, Berglund K, Larsson L, Toss G (2002) Changes in hip fracture epidemiology: redistribution between ages, genders and fracture types. Osteoporos Int 13:18–25
Takada J, Beck TJ, Iba K, Yamashita T (2007) Structural trends in the aging proximal femur in Japanese postmenopausal women. Bone 41:97–102
Hernández JL, Olmos JM, Alonso MA, González-Fernández CR, Martínez J, Pajarón M, Llorca J, González-Macías J (2006) Trend in hip fracture epidemiology over a 14-year period in a Spanish population. Osteoporos Int 17:464–470
Acknowledgments
We would like to thank Dr. Tomoaki Yoshikawa of Nishizaki Hospital for his valuable discussion of fracture assessment. This work was supported in part by the Japanese Ministry of Education, Culture, Sports, Science, and Technology.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Arakaki, H., Owan, I., Kudoh, H. et al. Epidemiology of hip fractures in Okinawa, Japan. J Bone Miner Metab 29, 309–314 (2011). https://doi.org/10.1007/s00774-010-0218-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-010-0218-8