
Abstract
This study aims to examine the extent to which a variety of pre-delivery factors (demographic, reproductive, psychological, psychiatric, and psychopathological) predict disturbances in mother–infant bonding (MIB) in the postpartum period. Two hundred fifty-one pregnant women enrolled at a public perinatal psychiatric service were assessed between the first and second trimester of pregnancy and at 6–7 weeks after delivery. During pregnancy, the psychological risk factors were assessed with the Vulnerable Personality Style Questionnaire, the Marital Adjustment Scale, the Early Trauma Inventory, and the General Health Questionnaire. To detect psychopathology, the Edinburgh Postnatal Depression Scale and the State-Trait Anxiety Inventory were used. At the postpartum evaluation, MIB was measured by the Postpartum Bonding Questionnaire. The results of the final regression model showed that emotional abuse in childhood, family psychiatric history, previous psychiatric hospitalization, and anxiety during pregnancy were significant predictors of MIB disturbances in postpartum, explaining 10.7% of the variance. The evaluation of women’s risk factors in pregnancy is important in order to prevent MIB disturbances and thus to ensure the welfare of mothers and their babies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mother–infant bonding (MIB) is the emotional relationship established between a mother and her newborn. A woman’s personal identity changes when she becomes a mother (Stern 1998), and a mother–infant bond is created through adaptive maternal behaviors during the early postpartum period (Feldman 2009). Newborns are particularly sensitive to environmental inputs during the postnatal period in which they are entirely dependent on the care of others (Moehler et al. 2006). Parents’ responsiveness plays a crucial role in this interaction and there is a significant association between maternal–infant bonding disturbances and parenting behavior (Muzik et al. 2013).
The alteration of this natural relationship has three main characteristics: maternal expression of dislike, resentment, or hatred toward the child; expressed desire for permanent relinquishment of care; or the desire that the baby should disappear (Brockington et al. 2006).
In the general population, the reported prevalence ranges from less than 1% (Brockington 2011) to 2.9%, or even as high as 8.6% (Edhborg et al. 2005; Reck et al. 2006; van Bussel et al. 2010; Garcia-Esteve et al. 2015), while in mothers attending psychiatric services, it ranges from 10 to 25% (Brockington 1996) to 38.75% (Brockington et al. 2006). In the Spanish population, MIB disturbances may be as high as 15.9% (Garcia-Esteve et al. 2015).
Current evidence shows how MIB disturbances can have a negative impact on the child’s brain development, maturational processes (Trevarthen and Aitken 2001), and cognitive progress (Murray et al. 1996), including the growth of language during the neonatal period. This development depends on the verbal and emotional behavior of the mother, whose responsiveness is critical for the baby’s emotional, affective, and social maturation (Hay et al. 2003; Feldman et al. 2004; Milgrom et al. 2004). Moreover, alterations of MIB increase the likelihood that the child will present psychopathology in the future (Mullen et al. 1996; Enns et al. 2002; Glasheen et al. 2013), more family conflicts (Reay et al. 2011), and a higher risk of suicide for offspring in adulthood (Heider et al. 2007).
Research concerning potential risk factors for MIB disturbances has approached the issue from a range of perspectives. Most studies have been carried out in the postpartum period and some have centered on variables that depend on the baby [e.g., temperament (Beck 1996; Sugawara et al. 1999; McGrath et al. 2008; Parfitt et al. 2014; Nolvi et al. 2016) or insomnia (Hiscock and Wake 2001)] while others have focused on parental psychopathology (Brockington 2004; Parfitt et al. 2014; Stein et al. 2014) or on the mother’s perception of receiving poor support from the partner (Feldman et al. 1997; Parfitt and Ayers 2014; Bicking Kinsey et al. 2014). Postpartum depression has attracted particular attention (Misri et al. 2006; Cornish et al. 2006; Palacios-Hernández 2015) since mothers with this condition become less sensitive to their baby’s need for emotional contact and have difficulty in establishing daily routines in breastfeeding, hygiene, and sleep patterns (Field 2010; Parsons et al. 2012).
In spite of these clinical findings, little is known about the pre-delivery factors that may affect the relationship between the mother and the newborn (Misri et al. 2010). Unwanted pregnancy (Barber et al. 1999; Goto et al. 2005; Brockington 2011; David 2011), low socio-economic status (Fuertes et al. 2008), and the mother’s experience of childhood abuse (Muzik et al. 2013) have been identified as prenatal factors that may undermine the establishment of a healthy MIB. Studies in the general population have identified certain other factors as being significant in the impairment of the mother–infant emotional bond, such as the prenatal wish for an abortion (Brockington et al. 2006), the type of delivery (Herguner et al. 2014), and the mother’s refusal to emotionally bond with the fetus (Müller 1996; Damato 2004; Dubber et al. 2014).
The present study explores the role of pre-delivery factors on the development of MIB disturbances in a group of mothers suffering from mental disorders during pregnancy. A part of the sample that had been previously studied for psychometric properties of the instrument employed in the measurement the criterion variable was used (Garcia-Esteve et al. 2015).
Methods
Study design, participants, and procedure
From 2011 to 2015, participants in this prospective longitudinal study were recruited from a variety of referral sources (general practitioner, psychiatric service, sexual and reproductive health center, or obstetrics service) via a public hospital perinatal psychiatry service. Socio-demographic, reproductive, psychological, psychiatric, and psychopathological data were recorded in their first psychiatric visit (between the first and second trimester of pregnancy). MIB was assessed in the second evaluation, at 6–7 weeks postpartum. Participants not attending both evaluations were excluded from the study. The final sample comprised 251 participants (Fig. 1).

Procedure of sample selection
The hospital’s Ethical Committee for Clinical Research approved both the design and the procedures of the study (HCB/2014/0014). All women gave informed consent to participate in the study prior to enrollment.
Measures and instruments
All standardized instruments used in this study were self-administered and demonstrated appropriate metric properties for the Spanish population (Garcia-Esteve et al. 2003; Navarro et al. 2007; Guillén-Riquelme and Buela-Casal 2011; Gelabert et al. 2011; Plaza et al. 2011; Garcia-Esteve et al. 2015).
Outcome assessed at postpartum
The Postpartum Bonding Questionnaire (PBQ) (Brockington et al. 2001, 2006) is a self-administered tool designed for early detection of disturbances in mother–infant bonding and comprises 25 questions rated on a 6-point Likert-type scale (0–5). It has four clinical relevance factors that are used to define four scales: scale 1 (impaired bonding), scale 2 (rejection and anger), scale 3 (anxiety about care), and scale 4 (incipient abuse). The total score ranges from 0 to 125, with a proposed minimum cut-off value of 26 indicating the presence of any type of bonding disorder. This questionnaire is valid and reliable for early detection of mother–infant bonding disturbances and was recently positively validated in the Spanish population (Garcia-Esteve et al. 2015). Cronbach’s alpha coefficients in the total sample were 0.90 for the General Factor (PBQ total score) and ranged from 0.56 to 0.85 for the four new primary factors (Garcia-Esteve et al. 2015). For the analysis of the criterion variable, we used the PBQ total score (α = 0.90, for this clinical sample).
Covariables assessed at pre-delivery evaluation
A general ad hoc clinical interview was administered by a specialized perinatal mental health professional during the first visit to record the following: five demographical data, i.e., nationality, age, marital status, educational level, and employment status; six reproductive health variables, i.e., planned/unplanned but accepted/accidental pregnancy (for analytical purposes, we dichotomized this variable as planned/unplanned), reproductive parity, type of conception, previous spontaneous abortion, previous induced abortions, and number of children under 3 years; two psychological variables, i.e., current relationship with partner and relationship with mother; and six psychiatric history variables, i.e., personal psychiatric history, episodes of previous hospitalization, family psychiatric background, history of completed suicide in the family, psychopathological state before pregnancy, and previous psychiatric treatment.
In order to compile these data, a professional-led 30/45-min interview was conducted. Previously, psychometric tests had been administered.
The General Health Questionnaire (GHQ-12) (Goldberg 1978) is a standard measure of psychological distress devised for population studies. The GHQ-12 has high validity, internal consistency, sensitivity, and specificity in the Spanish population (Sánchez-López del and Dresch 2008; Rocha and Obiols 2011), with a Cronbach’s alpha coefficient of 0.87. The cut-off score for psychological distress has been established at ≥ 3.
The State-Trait Anxiety Inventory (STAI) (Spielberger et al. 1983) is one of the most widely used self-inventories for measuring anxiety. It consists of two factors (state and trait); in this study, we used the first factor (anxiety state, STAI-S), which refers to a transitional period characterized by feelings of tension, apprehension, and increased activity of the autonomic nervous system, all of which may vary in intensity over time. The state anxiety scale consists of 20 items scored on a 4-point Likert-type scale (0 to 3). A higher score indicates a higher severity of anxiety.
The Early Trauma Inventory-Self Report (ETI-SR) (Bremner et al. 2007) is a 56-item inventory that assesses the presence of childhood trauma, including specific items for physical (ETI-p), emotional (ETI-e), and sexual abuse (ETI-s), as well as general trauma (ETI-g). The Cronbach alpha coefficients ranged from 0.72 to 0.88.
The Vulnerable Personality Style Questionnaire (VPSQ) (Dennis and Boyce 2004) is an evaluation developed to detect nine personality traits that increase the risk of postpartum depression: coping, nervy, timid, sensitive, worrier, organized, obsessive, expressive, and volatility. Cronbach’s alpha coefficient for the VPSQ total score was 0.63. The test–retest reliability indicated a good temporal stability [Intraclass Correlation Coefficient (ICC) = 0.88; 95% confidence interval (CI) = 0.82–0.91]. In spite of a sub-optimal Cronbach alpha score (0.63), VPSQ was nevertheless included because it is a clear and concise scale reflecting a complex multidimensional construct, in which each item contributes unique, i.e., valid, information. The test–retest reliability results indicate that the VPSQ scores remain stable (ICC = 0.88; 95% confidence interval (CI) = 0.82–0.91). VPSQ and psychobiologically based personality traits were found to have a clear association (Gelabert et al. 2011) and were therefore included with a view to explaining MIB alterations.
The Edinburgh Postnatal Depression Scale (EPDS) (Cox et al. 1987) is a questionnaire designed to detect postpartum depression at maternal health centers. It can be used as a research tool to analyze the factors that influence the emotional well-being of mothers and their families. It consists of ten items scored on a 4-point Likert-type scale (0–3) to assess mothers’ mood and anxiety and contains one item to evaluate suicidal thoughts. The optimal cut-off value of the Spanish validation of the EPDS is 10/11 for combined major and minor depression, with a sensitivity of 79% and a specificity of 95.5%. The Cronbach alpha was 0.90 in this sample.
The Marital Adjustment Test (MAT) (Locke and Wallace 1959) is an instrument that measures the general evaluation of marriage, marital cohesion, and the level of agreement between the partners in a variety of domains. The instrument assesses marital satisfaction. The MAT is one of the most widely used measures of marital and relationship adjustment. It includes 15 questions that assess overall level of happiness, level of agreement on a number of issues, and ways of handling disagreements. The Cronbach alpha was 0.76 for the current sample.
Statistical analysis
Differences on MIB (PBQ total score) were tested (ANOVA) regarding all the potential determinants to construct stratified categories for each variable. Moreover, for continuous variables, Pearson correlations were calculated to assess their relation with MIB. Finally, multiple linear regression analysis was performed to identify factors related with PBQ score. For our main variable of interest, namely MIB, the total number of usable sample was 251.This enabled us to detect an effect size (mean difference measured in the unit of standard deviation) as small as 0.05 with at least 80% statistical power. Regarding the level of statistical significance selected, we used a value less than 0.05. As the missing pattern was near random and the percentage not high, no imputation was applied when computing the regressions.
Statistical analysis was carried out with SPSS v.18.
Results
The characteristics of the sample are described in Table 1. Women in the cohort (N = 251) were between 18 and 45 years old, most of them born of community origin, and the majority had completed at least secondary studies and were actively employed. In this cohort, more than a third of pregnancies were unplanned, and the majority were spontaneous.
Regarding psychiatric factors, almost all referred previous psychiatric treatment and part of them had a history of psychiatric hospitalization. The prevalence of MIB disorder measured in the postpartum period using the cut-off of 26 (Brockington et al. 2006) was below 10%. The prevalence, using the original cut-off (Brockington et al. 2006), in factor 1 (impaired bonding) was 10.8%, in factor 2 (rejection and anger) was 2.4%, in factor 3 (anxiety about care) was 6%, and, finally, for factor 4 (risk of abuse), it was 6%.
Table 2 shows the distribution of MIB regarding qualitative potential risk factors; the statistically significant differences among covariable groups were employment situation, history of previous hospitalization, and history of psychiatric background of first-degree family.
For quantitative variables, we found that six factors assessed during pregnancy, depression, psychiatric morbidity, anxiety, poor marital relationship, personality vulnerable to suffer postpartum depression, and emotional abuse in childhood, were positively correlated with MIB disturbances (PBQ).
The multiple linear regression model included independent (predictor) variables with statistically significant relationships with the dependent (outcome) variable (p < 0.05) in preceding analyses as determinants of PBQ score. Multivariate analysis provided a final model in which state anxiety in pregnancy, history of psychiatric background of first-degree family, previous psychiatric hospitalization, and emotional abuse in childhood were the best antenatal predictors of MIB disturbances, explaining 10.7% of the variance (Tables 3 and 4).
Discussion
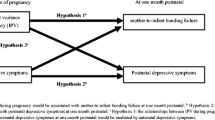
This study analyzes pre-delivery risk factors assessed during pregnancy and their association with MIB (Fig. 2). Three of them refer to situations or life events that the mother has suffered prior to becoming pregnant.

Multivariate analysis included covariables with high significance of antenatal risk factors for MIB
The prevalence of MIB disorders during the postpartum period (8.4%) was much lower than the figure obtained in other Spanish studies, which recorded figures of 15.9% in the clinical group (Garcia-Esteve et al. 2015) while studies elsewhere in Europe found between 22 and 38.8% of women on psychiatric programs (Brockington et al. 2006; Parfitt and Ayers 2012; Palacios-Hernández 2015). The lower rate of MIB disturbances found in our study may be due to several design factors. First, women who only attended the unit during the postpartum period were not included in the study as a longitudinal approach was required. However, this group may present a higher rate of MIB disturbances (a postpartum depression being the reason for their visit). Second, psychiatric treatment for psychopathological manifestations received from pregnancy to the postpartum period may act as a protector, improving the mother’s psychological state in the postpartum and therefore preventing a potential MIB disorder. Third, being self-referential questionnaires, participants may be inclined to minimize their responses due to reasons of stigma or social desirability. Moreover, although the authors’ proposed cut-off point of 26 was used for the PBQ (Brockington et al. 2006), it may not be the most suitable value for our sample.
Abuse in childhood and mother–infant bonding disturbances
Our results are similar to those found by other researchers who consider that childhood abuse in the mother is a risk factor for abuse of her own children (Berlin et al. 2011) and for a harsher parenting style (Bailey et al. 2012).
Childhood emotional abuse may occur in up to 48% of women in the clinical population (Plaza et al. 2012) and is directly related to multiple problems in adulthood. Childhood abuse is associated with a greater incidence of psychopathology throughout life (Kaplan et al. 1998; Lange et al. 1999; MacMillan et al. 2001), including a higher incidence of prenatal and postpartum depression (Dayan et al. 2010; Rich-Edwards et al. 2011; Plaza et al. 2012; LaCoursiere et al. 2012), all of which are associated with alterations of the MIB. Childhood abuse is also associated with a higher incidence of psychopathology in adolescence. Prospective studies have shown a higher presence of behavioral problems, post-traumatic stress disorder, and criminal behavior in adolescents (Gilbert et al. 2009), all factors related with alterations in adulthood relationships and the adult attachment style. On the other hand, social isolation or difficulty to connect with other people’s emotional needs is related to abuse in childhood (Cook et al. 2003).
Teicher et al. (2016) found that adults who had suffered abuse in childhood consistently had changes in the areas related to circuits that regulate the perception of threat and reward anticipation. These factors increase the vulnerability to suffer stress in adulthood and may explain MIB disturbances.
Anxiety during pregnancy and mother–infant bonding disturbance
Though the research into the course of anxiety disorders in the perinatal period is very limited (Howard et al. 2014), anxiety during pregnancy has received increasing attention due to its clinical relevance and presence in not only the majority of mental disorders but also psychologically healthy women (Andersson et al. 2006; Beck 2006; Figueiredo and Costa 2009). Its prevalence during pregnancy ranges from 21% (Heron et al. 2004) to 25% (Ross and McLean 2006; Britton 2011). More than 60% of these women also present anxiety in the postpartum period (Heron et al. 2004). Other studies indicate that as much as 59.5% of women suffer from state anxiety during pregnancy (Faisal-Cury and Rossi Menezes 2007).
The presence of anxiety during pregnancy has a clinical and biological impact on maternal health, fetal development, and consequences on offspring (Hedegaard et al. 1993; Hansen et al. 2000; Di Pietro et al. 2002; O’Connor et al. 2002, 2003).
The most common perinatal worries are centered on fetal well-being, maternal wellness, illness in the partner, and parental mortality (Misri et al. 2015). If these worries persist during pregnancy, they may promote functional impairment in all areas of the mother’s activities (Misri et al. 2015) and affect her quality of life during the postpartum period (Misri and Swift 2015) and levels of parenting stress at the postpartum period (Misri et al. 2010). Additionally, anxious mothers have more difficulty interacting with their baby (Figueiredo and Costa 2009; Müller et al. 2013). Anxious thoughts trigger avoidant behavior, attention problems, and perpetuate preoccupation (Stein et al. 2009). If these thoughts arise during pregnancy, they may hold impede the development of mother–fetal bonding during pregnancy (Cranley 1981; Hart and McMahon 2006; Alhusen 2008), which is highly associated with MIB disturbances (Dubber et al. 2014).
Limitations
A limitation of this study is the low explanatory power of the model. This particular model, which explains 10.7% of variance in the outcome variable (MIB), was performed only with pre-delivery variables. We suggest that it should include variables at postpartum period and/or biological variables (such as oxytocin levels) so we do not have information on their role in the development and clinical expression of MIB dysfunctions. Nor was mother–fetal bonding evaluated, although certain studies suggest that it is associated with MIB disturbances in the postpartum period (Dubber et al. 2014). It could be included in future studies. Likewise, the use of self-administered questionnaires may have introduced a bias, given the inevitably subjective nature of the responses. Finally, we used the VPSQ questionnaire, with a low internal consistency, i.e., whose Cronbach’s alpha is lower than would be desirable (α = 0.63).
Conclusions
The study demonstrates the presence of several factors that must be considered in the evaluation of pregnant women suffering from a psychiatric disorder, in order to prevent disturbances in the MIB. Of these factors, only one, namely anxiety, can be identified and modified in the hospital context during pregnancy and the postpartum period. The other three factors are traditionally linked to psychopathological vulnerability. The presence of predisposing factors (family history), stressful life events (emotional abuse in childhood), psychiatric antecedents (psychiatric hospitalization), and psychological distress during pregnancy (especially anxiety symptoms) increases the risk of disturbances in MIB in the postpartum period. Our findings suggest the involvement of several clinical factors and provide a sound basis for the future detection and treatment of MIB disturbances to promote healthy interactive maternal behavior.
References
Alhusen JL (2008) A literature update on maternal-fetal attachment. J Obstet Gynecol Neonatal Nurs 37:315–328
Andersson L, Sundström-Poromaa I, Wulff M et al (2006) Depression and anxiety during pregnancy and six months postpartum: a follow-up study. Acta Obstet Gynecol Scand 85:937–944
Bailey HN, DeOliveira CA, Wolfe VV et al (2012) The impact of childhood maltreatment history on parenting: a comparison of maltreatment types and assessment methods. Child Abuse Negl 36:236–246
Barber JS, Axinn WG, Thornton A (1999) Unwanted childbearing, health, and mother–child relationships. J Health Soc Behav 40:231–257
Beck CT (1996) A meta-analysis of the relationship between postpartum depression and infant temperament. Nurs Res 45:225–230
Beck CT (2006) Postpartum depression: it isn’t just the blues. Am J Nurs 106:40–50–1
Berlin LJ, Appleyard K, Dodge KA (2011) Intergenerational continuity in child maltreatment: mediating mechanisms and implications for prevention. Child Dev 82:162–176
Bicking Kinsey C, Baptiste-Roberts K, Zhu J, Kjerulff KH (2014) Birth-related, psychosocial, and emotional correlates of positive maternal–infant bonding in a cohort of first-time mothers. Midwifery 30:e188–e194. https://doi.org/10.1016/j.midw.2014.02.006
Bremner JD, Bolus R, E a M (2007) Psychometric properties of the early trauma inventory—self report. J Nerv Ment Dis 195:211–218. https://doi.org/10.1097/01.nmd.0000243824.84651.6c.Psychometric
Britton JR (2011) Infant temperament and maternal anxiety and depressed mood in the early postpartum period. Women Health 51:55–71. https://doi.org/10.1080/03630242.2011.540741
Brockington I (2011) Maternal rejection of the young child: present status of the clinical syndrome. Psychopathology 44:329–336. https://doi.org/10.1159/000325058
Brockington I (2004) Postpartum psychiatric disorders. Lancet (London, England) 363:303–310
Brockington IF (1996) Motherhood and mental health. Oxford Universiity Press, Oxford
Brockington IF, Fraser C, Wilson D (2006) The postpartum bonding questionnaire: a validation. Arch Womens Ment Health 9:233–242. https://doi.org/10.1007/s00737-006-0132-1
Brockington IF, Oates J, George S et al (2001) A screening questionnaire for mother–infant bonding disorders. Arch Womens Ment Health 3:133–140. https://doi.org/10.1007/s007370170010
Cook A, Spinazzola J, Ford J et al (2003) Complex trauma in children and adolescents. Psychiatr Ann 35:40
Cornish AM, McMahon CA, Ungerer JA et al (2006) Maternal depression and the experience of parenting in the second postnatal year. J Reprod Infant Psychol 24:121–132
Cox JL, Holden JM, Sagovsky R (1987) Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry 150:782–786
Cranley MS (1981) Development of a tool for the measurement of maternal attachment during pregnancy. Nurs Res 30:281–284
Damato EG (2004) Prenatal attachment and other correlates of postnatal maternal attachment to twins. Adv Neonatal Care 4:274–291
David HP (2011) Born unwanted: mental health costs and consequences. Am J Orthop 81:184–192. https://doi.org/10.1111/j.1939-0025.2011.01087.x
Dayan J, Creveuil C, Dreyfus M et al (2010) Developmental model of depression applied to prenatal depression: role of present and past life events, past emotional disorders and pregnancy stress. PLoS One 5:e12942
Dennis CL, Boyce P (2004) Further psychometric testing of a brief personality scale to measure vulnerability to postpartum depression. J Psychosom Obstet Gynaecol 25:305–311
Di Pietro JA, Hilton SC, Hawkins M et al (2002) Maternal stress and affect influence fetal neurobehavioral development. Dev Psychol 38:659–668. https://doi.org/10.1037/0012-1649.38.5.659
Dubber S, Reck C, Müller M, Gawlik S (2014) Postpartum bonding: the role of perinatal depression, anxiety and maternal-fetal bonding during pregnancy. Arch Womens Ment Health:187–195. https://doi.org/10.1007/s00737-014-0445-4
Edhborg M, Matthiesen A-S, Lundh W, Widström A-M (2005) Some early indicators for depressive symptoms and bonding 2 months postpartum—a study of new mothers and fathers. Arch Womens Ment Health 8:221–231
Enns MW, Cox BJ, Clara I (2002) Parental bonding and adult psychopathology: results from the US National Comorbidity Survey. Psychol Med 32:997–1008
Faisal-Cury A, Rossi Menezes P (2007) Prevalence of anxiety and depression during pregnancy in a private setting sample. Arch Womens Ment Health 10:25–32. https://doi.org/10.1007/s00737-006-0164-6
Feldman R (2009) The development of regulatory functions from birth to 5 years: insights from premature infants. Child Dev 80:544–561. https://doi.org/10.1111/j.1467-8624.2009.01278.x
Feldman R, Eidelman AI, Rotenberg N (2004) Parenting stress, infant emotion regulation, maternal sensitivity, and the cognitive development of triplets: a model for parent and child influences in a unique ecology. Child Dev 75:1774–1791
Feldman R, Greenbaum CW, Mayes LC, Erlich SH (1997) Change in mother–infant interactive behavior: relations to change in the mother, the infant, and the social context. Infant Behav Dev 20:151–163. https://doi.org/10.1016/S0163-6383(97)90018-7
Field T (2010) Postpartum depression effects on early interactions, parenting, and safety practices: a review. Infant Behav Dev 33:1–6
Figueiredo B, Costa R (2009) Mother’s stress, mood and emotional involvement with the infant: 3 months before and 3 months after childbirth. Arch Womens Ment Health 12:143–153
Fuertes M, Faria A, Soares H, Crittenden P (2008) Developmental and evolutionary assumptions in a study about the impact of premature birth and low income on mother–infant interaction. Acta Ethol 12:1–11. https://doi.org/10.1007/s10211-008-0051-4
Garcia-Esteve L, Ascaso C, Ojuel J, Navarro P (2003) Validation of the Edinburgh postnatal depression scale (EPDS) in Spanish mothers. J Affect Disord 75:71–76
Garcia-Esteve L, Torres A, Lasheras G et al (2015) Assessment of psychometric properties of the postpartum bonding questionnaire (PBQ) in Spanish mothers. Arch Womens Ment Health 19:385–394
Gelabert E, Subirà S, Plaza A et al (2011) The vulnerable personality style questionnaire: psychometric properties in Spanish postpartum women. Arch Womens Ment Health 14:115–124
Gilbert R, Widom CS, Browne K et al (2009) Burden and consequences of child maltreatment in high-income countries. Lancet (London, England) 373:68–81. https://doi.org/10.1016/S0140-6736(08)61706-7
Glasheen C, Richardson GA, Kim KH et al (2013) Exposure to maternal pre- and postnatal depression and anxiety symptoms: risk for major depression, anxiety disorders, and conduct disorder in adolescent offspring. Dev Psychopathol 25:1045–1063
Goldberg D (1978) Manual of the general health questionnaire. National Foundation for Educational Research, Windsor
Goto A, Yasumura S, Yabe J et al (2005) Association of pregnancy intention with parenting difficulty in Fukushima, Japan. J Epidemiol 15:244–246
Guillén-Riquelme A, Buela-Casal G (2011) Actualización psicométrica y funcionamiento diferencial de los items en el state trait anxiety inventory (STAI). Psicothema 23:510–515
Hansen D, Lou HC, Olsen J (2000) Serious life events and congenital malformations: a national study with complete follow-up. Lancet 356:875–880. https://doi.org/10.1016/S0140-6736(00)02676-3
Hart R, McMahon CA (2006) Mood state and psychological adjustment to pregnancy. Arch Womens Ment Health 9:329–337
Hay DF, Pawlby S, Angold A et al (2003) Pathways to violence in the children of mothers who were depressed postpartum. Dev Psychol 39:1083–1094
Hedegaard M, Henriksen TB, Sabroe S, Secher NJ (1993) Psychological distress in pregnancy and preterm delivery. BMJ 307:234–239
Heider D, Bernert S, Matschinger H et al (2007) Parental bonding and suicidality in adulthood. Aust N Z J Psychiatry 41:66–73
Herguner S, Cicek E, Annagur A et al (2014) Association of delivery type with postpartum depression, perceived social support and maternal attachment. J Psychiatry Neurol Sci 27:15–20. https://doi.org/10.5350/DAJPN2014270102
Heron J, O’Connor TG, Evans J et al (2004) The course of anxiety and depression through pregnancy and the postpartum in a community sample. J Affect Disord 80:65–73
Hiscock H, Wake M (2001) Infant sleep problems and postnatal depression: a community-based study. Pediatrics 107:1317–1322
Howard LM, Molyneaux E, Dennis C-L et al (2014) Non-psychotic mental disorders in the perinatal period. Lancet (London, England) 384:1775–1788. https://doi.org/10.1016/S0140-6736(14)61276-9
Kaplan SJ, Pelcovitz D, Salzinger S et al (1998) Adolescent physical abuse: risk for adolescent psychiatric disorders. Am J Psychiatry 155:954–959
LaCoursiere DY, Hirst KP, Barrett-Connor E (2012) Depression and pregnancy stressors affect the association between abuse and postpartum depression. Matern Child Health J 16:929–935
Lange A, de Beurs E, Dolan C et al (1999) Long-term effects of childhood sexual abuse: objective and subjective characteristics of the abuse and psychopathology in later life. J Nerv Ment Dis 187:150–158
Locke HJ, Wallace KM (1959) Short marital adjustment and prediction tests: their reliability and validity. Marriage Fam Living 21:251–255
MacMillan HL, Fleming JE, Streiner DL et al (2001) Childhood abuse and lifetime psychopathology in a community sample. Am J Psychiatry 158:1878–1883
McGrath JM, Records K, Rice M (2008) Maternal depression and infant temperament characteristics. Infant Behav Dev 31:71–80
Milgrom J, Westley DT, Gemmill AW (2004) The mediating role of maternal responsiveness in some longer term effects of postnatal depression on infant development. Infant Behav Dev 27:443–454
Misri S, Abizadeh J, Sanders S, Swift E (2015) Perinatal generalized anxiety disorder: assessment and treatment. J Women’s Heal 24:762–770. https://doi.org/10.1089/jwh.2014.5150
Misri S, Kendrick K, Oberlander TF et al (2010) Antenatal depression and anxiety affect postpartum parenting stress: a longitudinal, prospective study. Can J Psychiatr 55:222–228
Misri S, Reebye P, Milis L, Shah S (2006) The impact of treatment intervention on parenting stress in postpartum depressed mothers: a prospective study. Am J Orthop 76:115–119
Misri S, Swift E (2015) Generalized anxiety disorder and major depressive disorder in pregnant and postpartum women: maternal quality of life and treatment outcomes. J Obs Gynaecol Can 37:798–803. https://doi.org/10.1016/S1701-2163(15)30150-X
Moehler E, Brunner R, Wiebel A et al (2006) Maternal depressive symptoms in the postnatal period are associated with long-term impairment of mother–child bonding. Arch Womens Ment Health 9:273–278. https://doi.org/10.1007/s00737-006-0149-5
Mullen PE, Martin JL, Anderson JC et al (1996) The long-term impact of the physical, emotional, and sexual abuse of children: a community study. Child Abuse Negl 20:7–21
Müller D, Teismann T, Havemann B et al (2013) Ruminative thinking as a predictor of perceived postpartum mother–infant bonding. Cognit Ther Res. https://doi.org/10.1007/s10608-012-9454-7
Müller ME (1996) Prenatal and postnatal attachment: a modest correlation. J Obstet Gynecol Neonatal Nurs 25:161–166
Murray L, Hipwell A, Hooper R et al (1996) The cognitive development of 5-year-old children of postnatally depressed mothers. J Child Psychol Psychiatry 37:927–935
Muzik M, Bocknek EL, Broderick A et al (2013) Mother-infant bonding impairment across the first 6 months postpartum: the primacy of psychopathology in women with childhood abuse and neglect histories. Arch Womens Ment Health 16:29–38. https://doi.org/10.1007/s00737-012-0312-0
Navarro P, Ascaso C, Garcia-Esteve L et al (2007) Postnatal psychiatric morbidity: a validation study of the GHQ-12 and the EPDS as screening tools. Gen Hosp Psychiatry 29:1–7
Nolvi S, Karlsson L, Bridgett DJ et al (2016) Maternal postnatal psychiatric symptoms and infant temperament affect early mother–infant bonding. Infant Behav Dev. https://doi.org/10.1016/j.infbeh.2016.03.003
O’Connor TG, Heron J, Golding J et al (2002) Maternal antenatal anxiety and children’s behavioural/emotional problems at 4 years. Report from the Avon longitudinal study of parents and children. Br J Psychiatry 180:502–508
O’Connor TG, Heron J, Golding J et al (2003) Maternal antenatal anxiety and behavioural/emotional problems in children: a test of a programming hypothesis. J Child Psychol Psychiatry 44:1025–1036
Palacios-Hernández B (2015) Comparative study of the factors involved in the mother–infant bonding in women with and without postpartum depression. Universitat Autònoma de Barcelona
Parfitt Y, Ayers S (2014) Transition to parenthood and mental health in first-time parents. Infant Ment Health J 35:263–273
Parfitt Y, Ayers S (2012) Postnatal mental health and parenting: the importance of parental anger. Infant Ment Health J 33:400–410
Parfitt Y, Ayers S, Pike a et al (2014) A prospective study of the parent–baby bond in men and women 15 months after birth. J Reprod Infant Psychol 32:441–456. https://doi.org/10.1080/02646838.2014.956301
Parsons CE, Young KS, Rochat TJ et al (2012) Postnatal depression and its effects on child development: a review of evidence from low- and middle-income countries. Br Med Bull 101:57–79
Plaza A, Garcia-Esteve L, Torres A et al (2012) Childhood physical abuse as a common risk factor for depression and thyroid dysfunction in the earlier postpartum. Psychiatry Res 200:329–335. https://doi.org/10.1016/j.psychres.2012.06.032
Plaza A, Torres A, Martin-Santos R et al (2011) Validation and test–retest reliability of early trauma inventory in Spanish postpartum women. J Nerv Ment Dis 199:280–285
Reay R, Matthey S, Ellwood D, Scott M (2011) Long-term outcomes of participants in a perinatal depression early detection program. J Affect Disord 129:94–103
Reck C, Klier CM, Pabst K et al (2006) The German version of the postpartum bonding instrument: psychometric properties and association with postpartum depression. Arch Womens Ment Health 9:265–271
Rich-Edwards JW, James-Todd T, Mohllajee A et al (2011) Lifetime maternal experiences of abuse and risk of pre-natal depression in two demographically distinct populations in Boston. Int J Epidemiol 40:375–384
Rocha KB, Obiols JE (2011) Propiedades psicométricas y valores normativos del General Health Questionnaire (GHQ-12) en población general española 1. Int J Clin Heal Psychol 11:125–139
Ross LE, McLean LM (2006) Anxiety disorders during pregnancy and the postpartum period. J Clin Psychiatry 67:1285–1298. https://doi.org/10.4088/JCP.v67n0818
Sánchez-López del MP, Dresch V (2008) The 12-item general health questionnaire (GHQ-12): reliability, external validity and factor structure in the Spanish population. Psicothema 20:839–843
Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA (1983) Manual for the state-trait anxiety inventory. Consulting Psychologists Press, Palo Alto
Stein A, Lehtonen A, Harvey AG et al (2009) The influence of postnatal psychiatric disorder on child development. Is maternal preoccupation one of the key underlying processes? Psychopathology 42:11–21
Stein A, Pearson RM, Goodman SH et al (2014) Effects of perinatal mental disorders on the fetus and child. Lancet (London, England) 384:1800–1819
Stern D (1998) Mothers’ emotional needs. Pediatrics. https://doi.org/10.1542/peds.102.5.SE1.1250
Sugawara M, Kitamura T, Toda MA, Shima S (1999) Longitudinal relationship between maternal depression and infant temperament in a Japanese population. J Clin Psychol 55:869–880
Teicher MH, Samson JA, Anderson CM, Ohashi K (2016) The effects of childhood maltreatment on brain structure, function and connectivity. Nat Rev Neurosci 17:652–666. https://doi.org/10.1038/nrn.2016.111
Trevarthen C, Aitken KJ (2001) Infant intersubjectivity: research, theory, and clinical applications. J Child Psychol Psychiatry 42:3–48
van Bussel JCH, Spitz B, Demyttenaere K (2010) Reliability and validity of the Dutch version of the maternal antenatal attachment scale. Arch Womens Ment Health 13:267–277
Acknowledgements
The authors would like to thank Bruma Palacios and Bea Gonzalez for their assistance in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Farré-Sender, B., Torres, A., Gelabert, E. et al. Mother–infant bonding in the postpartum period: assessment of the impact of pre-delivery factors in a clinical sample. Arch Womens Ment Health 21, 287–297 (2018). https://doi.org/10.1007/s00737-017-0785-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00737-017-0785-y