
Abstract
Bipolar disorder is a high-risk condition during pregnancy. In women receiving prenatal care, this study addresses the proportion screening positive for bipolar disorder with or without also screening positive for depression. This is a pilot study using chart abstraction of Edinburgh Postnatal Depression Scale (EPDS) and Mood Disorder Questionnaire (MDQ) scores from patients’ initial prenatal visits. Among 342 participants, 289 (87.1 %) completed the EPDS, 277 (81.0 %) completed the MDQ, and 274 (80.1 %) completed both. Among EPDS screens, 49 (16.4 %) were positive. Among MDQ screens, 14 (5.1 %) were positive. Nine (21.4 %) of the 42 participants with a positive EPDS also had a positive MDQ. Of the 14 patients with a positive MDQ, five (35.7 %) had a negative EPDS. The prevalence of positive screens for bipolar disorder in an obstetric population is similar to gestational diabetes and hypertension, which are screened for routinely. Without screening for bipolar disorder, there is a high risk of misclassifying bipolar depression as unipolar depression. If only women with current depressive symptoms are screened for bipolar disorder, approximately one third of bipolar disorder cases would be missed. If replicated, these findings support simultaneous screening for both depression and bipolar disorder during pregnancy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bipolar disorder is an especially high-risk condition during pregnancy and postpartum. Prospective studies from psychiatric tertiary care settings have found that approximately 60–70 % of women with bipolar disorder experienced mood episodes during pregnancy and/or the postpartum period (Freeman et al. 2002; Viguera et al. 2007). Risks of untreated perinatal depressive and manic episodes include preterm labor, decreased birth weight, elevated levels of fetal stress hormones, and changes in neurobehavioral function of the infant (Lee and Lin 2010; Davalos et al. 2012; Grigoriadis et al. 2013). Bipolar disorder can also adversely affect mother-infant dyadic interactions (Vance et al. 2008).
Despite its high prevalence and the substantial risks of untreated symptoms, perinatal bipolar disorder is under-diagnosed and under-treated (Freeman et al. 2002). As the risks of untreated perinatal depression have become increasingly understood, large-scale perinatal depression screening initiatives have become widespread throughout the USA. While such initiatives are likely to substantially improve the detection of perinatal depression, they may inadvertently lead to misclassification if there is no simultaneous screening for bipolar disorder. Misdiagnosis of depressive episodes as unipolar rather than bipolar can be especially problematic, as treatment with antidepressants without a concomitant mood stabilizer increases the risk of hypomania/mania and rapid cycling and psychotic episodes in patients with bipolar disorder and may increase the risk of recurrence (Ghaemi et al. 2003; Ghaemi et al. 2004). It is not yet known how many women who “screen positive” for antenatal depression have bipolar rather than unipolar depression. In a primary care clinic population, more than 20 % of patients receiving antidepressants for depression screened positive for bipolar disorder (Hirschfeld et al. 2005). In a study of women diagnosed with postpartum depression, more than half met the criteria for bipolar disorder based on structured interviews (Sharma et al. 2008). In addition, it has been found that a disproportionate number of women with bipolar disorder who experience a recurrence during pregnancy will experience either depressive or dysphoric mixed symptoms early in pregnancy (Viguera et al. 2007). This indicates not only that the likelihood of misdiagnosis is high, but also that in the absence of bipolar disorder screening early in pregnancy, offspring of women with bipolar disorder may be exposed to a lengthy period of maternal psychopathology in utero.
In order to determine the degree to which screening for bipolar disorder as part of prenatal care adds value, the first step is to ascertain the prevalence of positive bipolar screens in an obstetric clinic population, with or without screening positive for depression. This could help determine whether screening for perinatal depression and bipolar disorder should be simultaneous or sequential.
For these reasons, this pilot study aims to answer the following three questions:
-
1.
What proportion of a pregnant population screens positive for bipolar disorder?
-
2.
What percent of women who screen positive for depression also screen positive for bipolar disorder (risking misdiagnosis with unipolar depression in the absence of bipolar screening)?
-
3.
What percent of women who screen positive for bipolar disorder screen negative for depression (risking lack of detection if bipolar screens were only used for women screening positive for depression)?
Materials and methods
Study participants
The study consisted of 342 women consecutively presenting for initiation of prenatal care in the Brigham and Women’s Hospital Resident Obstetrics clinic between February 2012 and September 2012. The mean age of the clinic patients during that time frame was 30.95 years (SD 7.21 years), with a racial/ethnic distribution of 35.9 % black, 23.3 % Hispanic, 21.6 % non-Hispanic white, 6.8 % Asian, 7.5 % other, and 4.0 % not recorded.
Screening tools
As part of routine clinical care within that clinic, every patient initiating prenatal care was given the Edinburgh Postnatal Depression Scale (EPDS) and the Mood Disorder Questionnaire (MDQ).
The EPDS is a depression screening tool specifically designed and validated for use during pregnancy and postpartum. Cutoff scores between 10 and 12 have consistently yielded a sensitivity of at least 0.8 and specificity of at least 0.7 in detecting perinatal major depression, which is appropriate for most clinical settings (Miller et al. 2011). In this study, we chose to use the cutoff score of 11 to indicate a positive screen, though we present results for all three cutoff points.
The MDQ is the most widely researched brief self-report screen for bipolar disorder. It has been validated for use in primary care settings (Hirschfeld et al. 2003), and one study validated its use in the postpartum period (Sharma and Xie 2011); it has not yet been validated during pregnancy. Because it assesses lifetime bipolar disorder rather than current symptoms, there is less concern that normal pregnancy changes would confound the results. Based on studies to date, there are two methods of scoring the MDQ. The initially developed scoring method requires endorsement of at least seven of 13 lifetime manic symptoms, several co-occurring symptoms, and moderate or serious associated functional impairment. With the Structured Clinical Interview for the DSM IV as the gold standard, the original validation study reported a sensitivity of 0.73 and a specificity of 0.90 in a psychiatric outpatient population (Hirschfeld et al. 2000). However, a subsequent study in the general population revealed a sensitivity of 0.28 and specificity of 0.97 (Hirschfeld et al. 2003). Dodd and colleagues studied a community sample of women, with similar results (Dodd et al. 2009). These results indicated that the psychometric properties of the MDQ may vary according to the population studied, and that the sensitivity could be unacceptably low in non-psychiatric populations. Subsequent studies found that the sensitivity was improved by excluding the last two supplementary questions (clustering of symptoms and impairment of functioning) in both general (Chung et al. 2009) and perinatal (Sharma and Xie 2011; Frey et al. 2012) populations. For the current study of a non-psychiatric perinatal population, reducing false-negatives was a more central concern than reducing false-positives, because the central intent of screening was to detect risk of perinatal mood episodes early in pregnancy. Therefore, to best meet the purposes of this study, we used the modified MDQ scoring system to enhance sensitivity.
Procedure
As part of routine clinical practice, patients initially presenting to the clinic were given the EPDS and MDQ screens by a front desk staff and returned completed screens to a nursing staff. Each patient seen for prenatal care underwent an initial nursing assessment during which these screening tools were scored and reviewed. Scores were recorded by nurses in the patients’ electronic medical records, within templated nursing assessment notes. For this study, investigators recorded whether there was documentation that the EPDS and/or MDQ were given and completed, and if so, the numeric score for each. This study was approved by the Institutional Review Board of the hospital. To protect patient confidentiality, no data containing personal identifiers were collected.
Data analysis
Positive screens for major depression and bipolar disorder were examined in terms of counts and frequencies. Associations between positive screens for bipolar disorder and positive screens for major depression were represented as odd ratios and evaluated for statistical significance using chi-square tests.
Results
Data from 342 participants were collected from February 2012 through September 2012. Of these participants, 298 (87.1 %) were screened with the EPDS and 277 (81.0 %) were screened with the MDQ. A total of 274 participants (80.1 %) completed both screens.
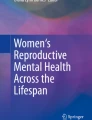
Figure 1 shows the proportion of study participants who screened positive for depression and bipolar disorder. As shown in Table 1, the odds of having a positive MDQ screen are significantly higher for those with a positive EPDS screen (with cutoff score of 11, odd ratio = 12.38, p < 0.001) than for those with a negative EPDS screen. At the same time, five out of 14 participants (35.7 %) with a positive MDQ screen would be missed by only screening those with an EPDS-positive screen. Since the percentage of missed positive MDQs is influenced by choice of EPDS cutoff, Table 1 shows positive bipolar screens with EPDS cutoff scores of 10, 11, and 12.

EPDS and MDQ screening results for pregnant women at initial prenatal care visits using EPDS cutoff of 11 and MDQ cutoff of 7. 1 total participants screened with the EPDS, with or without MDQ screening. 2 total participants screened with both the EPDS and MDQ. 3 total participants screened with the MDQ, with or without EPDS screening
Discussion and conclusion
This study found that 5.1 % of a prenatal, non-psychiatric population screened positive for a high risk of bipolar disorder. This is similar to the 4.4 % lifetime prevalence of bipolar spectrum disorders in the general US population reported in the National Comorbidity Survey Replication (Merikangas et al. 2007). Additionally, Hoertel et al. found the lifetime prevalence of bipolars I and II in the general population to be 3.31 % using data from the 2001–2002 National Epidemiologic Survey of Alcohol and Related Conditions (NSARC), though this increased to 5.84 % if cases with subthreshold hypomania were included (Hoertel et al. 2013). Studies of primary care clinic populations have found rates of bipolar disorder between 0.5 and 4.3 % using structured interviews, though studies using screening tools reported higher rates of 7.6–9.8 % (Cerimele et al. 2014).
Guidelines from the US Preventive Task Force (Pignone et al. 2002) and UK National Screening Committee (Buist et al. 2002) on determining whether screening for a particular disorder should be initiated are based in part on prevalence. The findings from this study suggest that the proportion of pregnant women in an obstetric clinic setting screening positive for bipolar disorder is similar to the prevalence of gestational diabetes (2–6 %) (Buckley et al. 2012) and gestational hypertension (5.0 %) (Haddad and Sibai 1999). Although the latter two are part of routine prenatal screening, screening for bipolar disorder is not. The finding that more than 80 % of women completed the MDQ on their initial prenatal visit, with nursing-recorded scores entered into the medical record, suggests that screening for bipolar disorder is largely acceptable and feasible for both patients and practitioners.
In this study, 21.4 % of patients who endorsed active depressive symptoms on the EPDS also screened positive for bipolar disorder on the MDQ and may have been at risk for being misdiagnosed with unipolar depression. This is similar to Hirschfeld’s findings from a primary care clinic, showing that more than 20 % of patients receiving antidepressants for depression also screened positive for bipolar disorder (Hirschfeld et al. 2005). These findings underscore that depressive symptoms detected during pregnancy may be part of a bipolar diathesis.
Additionally, the results of our study suggest that if a clinic were to use bipolar screening only for women who had already screened positive for depression, a substantial proportion of patients with bipolar disorder would be missed. Depending on the EPDS cutoff score chosen, at least 21.4 % (EPDS cutoff 10) or as many as 57.1 % (EPDS cutoff 12) of MDQ-positive women would not have been detected if only EPDS-positive women had been screened for bipolar disorder in this study.
Our study has important limitations. Because this was a pilot study collecting only de-identified data, we were not able to investigate factors, such as parity or psychotropic medication use, which might differentiate positive responders to the MDQ from positive responders to the EPDS and from the general population. Another limitation is the unresolved controversy about optimal scoring of the MDQ. Because of the significant clinical implications of under-diagnosing bipolar disorder in pregnancy, a high sensitivity is especially important in any screening tool used for this condition. Thus, we used the modified MDQ scoring to maximize detection of bipolar disorder among these high-risk patients. However, this modified scoring has not yet been rigorously validated. In addition, our use of the modified scoring limits the comparison of our findings to those from studies using the initial MDQ scoring system.
In summary, our study provides support for universal screening of bipolar disorder during pregnancy. Detecting bipolar disorder in the beginning of pregnancy allows for the implementation of interventions early enough to prevent exacerbation during the particularly high-risk postpartum period. It also reduces the inadvertent increase in risk that could otherwise come from misdiagnosis of bipolar disorder as unipolar depression. As a result, screening for bipolar disorder in pregnancy may prevent adverse clinical events for both the pregnant patient and her fetus. Further research is needed to validate optimal screening tools and scoring methods for a perinatal population.
References
Buckley BS, Harreiter J, Damm P, Corcoy R, Chico A, Simmons D, Vellinga A, Dunne F, Group DCI (2012) Gestational diabetes mellitus in Europe: prevalence, current screening practice and barriers to screening. A review. Diabet Med 29(7):844–854. doi:10.1111/j.1464-5491.2011.03541.x
Buist AE, Barnett BE, Milgrom J, Pope S, Condon JT, Ellwood DA, Boyce PM, Austin MP, Hayes BA (2002) To screen or not to screen—that is the question in perinatal depression. Med J Aust 177(Suppl):S101–S105
Cerimele JM, Chwastiak LA, Dodson S, Katon WJ (2014) The prevalence of bipolar disorder in general primary care samples: a systematic review. Gen Hosp Psychiatry 36(1):19–25. doi:10.1016/j.genhosppsych.2013.09.008
Chung KF, Tso KC, Chung RT (2009) Validation of the Mood Disorder Questionnaire in the general population in Hong Kong. Compr Psychiatry 50(5):471–476. doi:10.1016/j.comppsych.2008.10.001
Davalos DB, Yadon CA, Tregellas HC (2012) Untreated prenatal maternal depression and the potential risks to offspring: a review. Arch Womens Ment Health 15(1):1–14. doi:10.1007/s00737-011-0251-1
Dodd S, Williams LJ, Jacka FN, Pasco JA, Bjerkeset O, Berk M (2009) Reliability of the Mood Disorder Questionnaire: comparison with the Structured Clinical Interview for the DSM-IV-TR in a population sample. Aust N Z J Psychiatry 43(6):526–530. doi:10.1080/00048670902873706
Freeman MP, Smith KW, Freeman SA, McElroy SL, Kmetz GE, Wright R, Keck PE Jr (2002) The impact of reproductive events on the course of bipolar disorder in women. J Clin Psychiatry 63(4):284–287
Frey BN, Simpson W, Wright L, Steiner M (2012) Sensitivity and specificity of the Mood Disorder Questionnaire as a screening tool for bipolar disorder during pregnancy and the postpartum period. J Clin Psychiatry 73(11):1456–1461. doi:10.4088/JCP.12m07856
Ghaemi SN, Hsu DJ, Soldani F, Goodwin FK (2003) Antidepressants in bipolar disorder: the case for caution. Bipolar Disord 5(6):421–433
Ghaemi SN, Rosenquist KJ, Ko JY, Baldassano CF, Kontos NJ, Baldessarini RJ (2004) Antidepressant treatment in bipolar versus unipolar depression. Am J Psychiatry 161(1):163–165
Grigoriadis S, VonderPorten EH, Mamisashvili L, Tomlinson G, Dennis CL, Koren G, Steiner M, Mousmanis P, Cheung A, Radford K, Martinovic J, Ross LE (2013) The impact of maternal depression during pregnancy on perinatal outcomes: a systematic review and meta-analysis. J Clin Psychiatry 74(4):e321–e341. doi:10.4088/JCP.12r07968
Haddad B, Sibai BM (1999) Chronic hypertension in pregnancy. Ann Med 31(4):246–252
Hirschfeld RM, Cass AR, Holt DC, Carlson CA (2005) Screening for bipolar disorder in patients treated for depression in a family medicine clinic. J Am Board Fam Pract 18(4):233–239
Hirschfeld RM, Holzer C, Calabrese JR, Weissman M, Reed M, Davies M, Frye MA, Keck P, McElroy S, Lewis L, Tierce J, Wagner KD, Hazard E (2003) Validity of the Mood Disorder Questionnaire: a general population study. Am J Psychiatry 160(1):178–180
Hirschfeld RM, Williams JB, Spitzer RL, Calabrese JR, Flynn L, Keck PE Jr, Lewis L, McElroy SL, Post RM, Rapport DJ, Russell JM, Sachs GS, Zajecka J (2000) Development and validation of a screening instrument for bipolar spectrum disorder: the Mood Disorder Questionnaire. Am J Psychiatry 157(11):1873–1875
Hoertel N, Le Strat Y, Angst J, Dubertret C (2013) Subthreshold bipolar disorder in a U.S. national representative sample: prevalence, correlates and perspectives for psychiatric nosography. J Affect Disord 146(3):338–347. doi:10.1016/j.jad.2012.09.016
Lee HC, Lin HC (2010) Maternal bipolar disorder increased low birthweight and preterm births: a nationwide population-based study. J Affect Disord 121(1–2):100–105. doi:10.1016/j.jad.2009.05.019
Merikangas KR, Akiskal HS, Angst J, Greenberg PE, Hirschfeld RM, Petukhova M, Kessler RC (2007) Lifetime and 12-month prevalence of bipolar spectrum disorder in the National Comorbidity Survey Replication. Arch Gen Psychiatry 64(5):543–552. doi:10.1001/archpsyc.64.5.543
Miller LJ, Gupta R, Scremin AM (2011) The evidence for perinatal depression screening and treatment. In: Hadler A (ed) Reducing racial/ethnic disparities in reproductive and perinatal outcomes: the evidence from population-based interventions. Springer Science + Business Media, pp 301–327
Pignone MP, Gaynes BN, Rushton JL, Burchell CM, Orleans CT, Mulrow CD, Lohr KN (2002) Screening for depression in adults: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 136(10):765–776
Sharma V, Khan M, Corpse C, Sharma P (2008) Missed bipolarity and psychiatric comorbidity in women with postpartum depression. Bipolar Disord 10(6):742–747. doi:10.1111/j.1399-5618.2008.00606.x
Sharma V, Xie B (2011) Screening for postpartum bipolar disorder: validation of the Mood Disorder Questionnaire. J Affect Disord 131(1–3):408–411. doi:10.1016/j.jad.2010.11.026
Vance YH, Huntley Jones S, Espie J, Bentall R, Tai S (2008) Parental communication style and family relationships in children of bipolar parents. Br J Clin Psychol 47(Pt 3):355–359. doi:10.1348/014466508X282824
Viguera AC, Whitfield T, Baldessarini RJ, Newport DJ, Stowe Z, Reminick A, Zurick A, Cohen LS (2007) Risk of recurrence in women with bipolar disorder during pregnancy: prospective study of mood stabilizer discontinuation. Am J Psychiatry 164(12):1817–1824. doi:10.1176/appi.ajp.2007.06101639, quiz 1923
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Merrill, L., Mittal, L., Nicoloro, J. et al. Screening for bipolar disorder during pregnancy. Arch Womens Ment Health 18, 579–583 (2015). https://doi.org/10.1007/s00737-015-0527-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00737-015-0527-y