
Abstract
Autism spectrum disorder (ASD) is a lifelong neurodevelopmental condition that is accompanied by an atypical development of brain maturation. So far, brain development has mainly been studied during early childhood in ASD, and using measures of total or lobular brain volume. However, cortical volumetric measures are a product of two distinct biological neuroanatomical features, cortical thickness, and surface area, which most likely also have different neurodevelopmental trajectories in ASD. Here, we therefore examined age-related differences in cortical thickness and surface area in a cross-sectional sample of 77 male individuals with ASD ranging from 7 to 25 years of age, and 77 male neurotypical controls matched for age and FSIQ. Surface-based measures were analyzed using a general linear model (GLM) including linear, quadratic, and cubic age terms, as well as their interactions with the main effect of group. When controlling for the effects of age, individuals with ASD had spatially distributed reductions in cortical thickness relative to controls, particularly in fronto-temporal regions, and also showed significantly reduced surface area in the prefrontal cortex and the anterior temporal lobe. We also observed significant group × age interactions for both measures. However, while cortical thickness was best predicted by a quadratic age term, the neurodevelopmental trajectory for measures of surface area was mostly linear. Our findings suggest that ASD is accompanied by age-related and region-specific reductions in cortical thickness and surface area during childhood and early adulthood. Thus, differences in the neurodevelopmental trajectory of maturation for both measures need to be taken into account when interpreting between-group differences overall.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a lifelong neurodevelopmental condition characterized by a triad of symptoms in (1) impaired social communication, (2) deficits in social reciprocity, and (3) repetitive and stereotypic behavior (Wing 1997). These ‘core’ symptoms of ASD typically manifest before the age of 2 years and are accompanied by developmental differences in brain anatomy and connectivity (Geschwind and Levitt 2007; Amaral et al. 2008; Ecker et al. 2013b). However, the wider neural systems underlying ASD are complex and involve abnormalities in multiple, spatially distributed neurocognitive systems (Ecker et al. 2012). This makes the neuroanatomy of ASD inherently difficult to describe in vivo.
So far, most existing structural neuroimaging studies in ASD have examined either children or adults with ASD in order to determine the set of brain regions that differ most from typical controls in terms of their neuroanatomy. For example, neuroanatomical differences have consistently been reported in (1) the fronto-striatal system, which has been linked to repetitive and stereotyped behaviors (Langen et al. 2007, 2011); (2) fronto-temporal regions and the amygdala, which are associated with abnormalities in socio-emotional processing (Waiter et al. 2004; Schumann et al. 2009; Nordahl et al. 2012); and (3) speech and language regions that may underlie impaired social communication and language (Redcay and Courchesne 2008). However, to date, there are few neuroimaging studies examining neuroanatomy in ASD across different age-groups in order to characterize age-dependent anatomical variations between individuals with ASD and healthy controls. Moreover, the few existing studies mainly focus on cortical development through early infancy into late childhood. For instance, there is evidence to suggest that the brain is enlarged in toddlers with ASD (between 2 and 5 years of age) (Courchesne and Pierce 2005; Schumann et al. 2010; Hazlett et al. 2011), while no significant differences in total brain volume are typically observed during late childhood or adulthood (McAlonan et al. 2005; Hardan et al. 2009). However, it is largely unknown how the brain develops during adolescence in ASD, and there is thus a need for neuroimaging studies to also examine neurodevelopmental trajectories from late childhood into adulthood.
Furthermore, previous structural neuroimaging studies in ASD have largely used volume-based approaches and focused on measures of global or regional differences in brain volume (e.g., Waiter et al. 2004; Carper and Courchesne 2005; McAlonan et al. 2005). However, cortical volume is by definition a product of cortical thickness and surface area and can therefore be fractionated into different morphometric sub-components, which have distinct genetic determinants (Panizzon et al. 2009), contrasting phylogeny (Rakic 1995), and differing developmental trajectories (Raznahan et al. 2011). It is therefore important to examine cortical thickness and surface area in isolation in order to better understand the neurobiological mechanisms associated with brain abnormalities in ASD.
Differences in cortical thickness have been reported in children (Hardan et al. 2006; Mak-Fan et al. 2011) and adults with ASD (Hyde et al. 2010; Ecker et al. 2013a), and seem most prominent in temporal, parietal, and frontal lobes. In children with ASD, cortical thickness in these regions mainly seems to be increased relative to controls, while decreased cortical thickness in ASD is typically observed in adult samples. Thus, the sign of between-group differences in cortical thickness (i.e., increased or decrease) in ASD seems to be dependent on the particular age-group under investigation, which prompted several studies to also examine age-related differences in cortical thickness in ASD. For example, Wallace et al. (2010) investigated differences in cortical thickness in individuals with ASD and matched controls ranging from 12 to 24 years of age, and noted extensive temporal and parietal reductions in cortical thickness in ASD while controlling for age, and a more accelerated age-related decline in cortical thickness over time (Wallace et al. 2010). Similar findings of an accelerated cortical thinning in ASD were reported in individuals ranging from 10 to 60 years (Raznahan et al. 2010) and 20 to 55 years of age (Scheel et al. 2011). While these studies were important first steps in determining age-dependent differences in a specific aspect of cortical pathology implicated in ASD, a major limitation to these studies is that only linear age effects were examined. Studies of typical gray matter maturation suggest that there is considerable regional variation in complexity of the normal developmental trajectory of cortical thickness across the cerebral cortex, including cubic, quadratic, and linear effects (Shaw et al. 2006). As noted previously by Wallace et al. (2010), the cubic and quadratic developmental trajectories (i.e., inverted U-shapes) of gray matter maturation pose a challenge for comparisons across cross-sectional studies as a precocious or delayed maturation in a particular subject group could lead to a significantly positive difference at one age and a negative difference at a different age (Wallace et al. 2010). It is therefore important to examine a variety of statistical models in order to find the model best suited to examine age-related differences in cortical thickness in ASD. Moreover, while the typical neurodevelopmental trajectories are well established for measures of cortical thickness, there is currently no comparable data for vertex-based measures of surface area.
Differences in cortical surface area remain relatively unexplored in ASD, particularly on the local (i.e., vertex) level, and results seem to be in disagreement. Raznahan et al. (2010) reported that there was no main effect of group nor a group × age interaction in lobar-level surface area when comparing individuals with ASD to neurotypical controls ranging from 10 to 60 years (Raznahan et al. 2010). Similarly, Mak-Fan et al. (2011) found no significant between-group differences but reported a significant group × age interaction in occipital lobe surface area in older children with ASD (Mak-Fan et al. 2011). There are also two studies examining vertex-level differences in surface area in ASD. A recent study by Wallace et al. (2013) reported no group differences in vertex-wise estimates of surface area, and no interaction between age and group, in a sample of individuals with ASD and matched controls ranging from 12 to 24 years of age (Wallace et al. 2013). Also, Doyle-Thomas et al. (2013) investigated a larger age range of individuals with ASD (7–39 years of age), reporting that surface area in the right cingulate was significantly different between groups and decreased more rapidly with age in ASD compared to controls. There is thus a need for replicating these findings in a large and well-characterized sample of individuals with ASD and matched neurotypical controls, and to contrast differences in the neurodevelopmental trajectory of cortical thickness with age-dependent variations in surface area.
Here, we employed a cross-sectional design to examine age-related differences in cortical thickness and surface area in the same group of individuals with ASD and matched healthy controls between 7 and 25 years of age. We examined linear, quadratic, and cubic age effects on both measures in order to find the most ‘parsimonious’ model (i.e., model with the smallest number of parameters) that allowed us to examine between-group differences in cortical thickness and surface area in ASD in the presence of significant age effects, as well as age × group (age ‘by’ group) interactions.
Materials and methods
Participants
Seventy-seven (77) right-handed male individuals with ASD and 77 controls aged 7–25 years were recruited by advertisement and subsequently assessed at the Institute of Psychiatry, King’s College, London. Both groups were matched for gender (all male), age, full-scale IQ, and handedness (all right-handed). Exclusion criteria for all participants included a history of major psychiatric disorder, head injury, genetic disorder associated with autism (e.g., fragile × syndrome and tuberous sclerosis), or any other medical condition affecting brain function (e.g., epilepsy). We excluded potential participants with a history of substance abuse (including alcohol) and individuals taking antipsychotic medication, mood stabilizers, or benzodiazepines. All participants with ASD were initially assessed according to the International Statistical Classification of Diseases, 10th Revision (ICD-10) research criteria. Diagnosis for individuals with ASD was then confirmed using the Autism Diagnostic Interview–Revised [ADI-R, (Lord et al. 1994)] to ensure that all participants with ASD met the criteria for childhood autism. All cases of ASD reached ADI-R algorithm cutoff values in the three domains of impaired reciprocal social interaction, communication, and repetitive behaviors and stereotyped patterns, although failure to reach cutoff in one of the domains by one point was permitted (see Table 1 for details). Current symptoms were assessed using the Autism Diagnostic Observation Schedule [ADOS, (Lord et al. 1989)], but were not used as inclusion criteria. Overall intellectual ability was assessed using the Wechsler Abbreviated Scale of Intelligence (Wechsler 1999) in all participants. All participants fell within the high-functioning range of the spectrum, defined by a full-scale IQ higher than 70. All participants gave informed written consent in accordance with ethics approval by the National Research Ethics Committee, Suffolk, England.
MRI data acquisition
All participants were scanned at the Centre for Neuroimaging Sciences, Institute of Psychiatry, London, UK, using a 3-T GE Signa System (General-Electric, Milwaukee, WI). High-resolution structural T1-weighted volumetric images were acquired with full-head coverage, 196 contiguous slices (1.1 mm thickness, with 1.09 × 1. 09-mm in-plane resolution), a 256 × 256 × 196 matrix, and a repetition time/echo time (TR/TE) of 7/2.8 ms (flip angle = 20 in., FOV = 28 cm). A (birdcage) head coil was used for radiofrequency transmission and reception. Consistent image quality was ensured by a semiautomated quality control procedure.
Cortical reconstruction using FreeSurfer
All individual T1-weighted scans were initially screened by a radiologist to exclude images with visible clinical abnormalities or large-scale movement artifacts. Scans of insufficient quality were excluded from the analysis (dropout <2 %). The FreeSurfer analysis suite (vFS5.3.0 release, http://surfer.nmr.mgh.harvard.edu/) was used to derive models of the cortical surface in each T1-weighted image. These well-validated and fully automated procedures have been extensively described elsewhere (e.g., Fischl et al. 1999b, a; Dale et al. 1999; Ségonne et al. 2004). In brief, a single filled white matter volume was generated for each hemisphere after intensity normalization, skull stripping, and image segmentation using a connected components algorithm. Then, a surface tessellation was generated for each white matter volume by fitting a deformable template. This resulted in a triangular cortical mesh for gray and white matter surfaces consisting of approximately 150,000 vertices (i.e., points) per hemisphere. Following standard FreeSurfer preprocessing, each reconstructed surface was then visually inspected for reconstruction errors, and images that did not reconstruct correctly (i.e., with visible anatomical abnormalities) were further excluded from the statistical analysis (dropout 5 %).
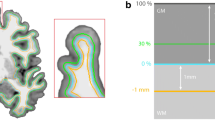
Measures of cortical thickness were computed as the closest distance from the gray and white matter boundary to the gray matter and cerebrospinal fluid boundary at each vertex on the tessellated surface. For each participant, we also computed mean cortical thickness across the entire brain. Vertex-based estimates of surface area were derived as outlined by (Winkler et al. 2012). Here, the individual’s native surface is initially transformed into a spherical representation, which preserves vertex identities (e.g., total numbers) and original areal quantities, and subsequently registered to a common atlas/template. This registration does not change areal quantities but shifts vertex positions to match the template. Finally, areal quantities are transferred to a common grid via areal interpolation. Here, the final amount of ‘area’ each face receives on the new grid depends on the overlap between the original source face and the target (i.e., common grid) face. In this way, the fixed target surface is redistributed across one of more source faces and can be used as weighting factor to account for inter-individuals differences in surface reconstructions. We also computed total surface area and mean cortical thickness (across both hemispheres) for each participant. To improve the ability to detect population changes, each parameter was smoothed using a 10-mm surface-based smoothing kernel.
Statistical analysis
Statistical analysis was conducted using the SurfStat toolbox (http://www.math.mcgill.ca/keith/surfstat/) for Matlab (R2010b; MathWorks). To determine developmental trajectories at each vertex, we initially tested for linear, cubic, and quadratic age effects on measures of cortical thickness and surface area, in addition to the main effect of group. Here, an F test for nested model comparisons was used at each vertex employing a step-up model selection procedure. Initially, the linear (i.e., most reduced) model was compared to a more complex quadratic model in order to determine whether the addition of a quadratic age effect significantly improved the goodness of fit. If the quadratic model performed significantly better, it was then compared to the full cubic (i.e., most complex) model, which contained a linear, quadratic, and cubic age term. This allowed us to identify the most parsimonious model at each vertex, i.e., most simple plausible model that explains variations in measures of brain morphology with the smallest set of predictors. Parameter estimates for CT and SA (Y i) were estimated separately by regression of a general linear model (GLM) at each vertex i and subject j, with (1) group (G) as categorical fixed-effects factor, (2) linear, quadratic, and cubic terms for age as well as their interactions with group, and (3) FSIQ as continuous covariate.
Thus, the cubic model was formalized as: Y i = β 0 + β 1 G j + β 2 Agej + β 3 Age 2j + β 4 Age 3j + β 5 (Agej × Group) + β6 (Age 2j × Group) + β 7 (Age 3j × Group) + β 8 IQj + ε i, where ε denotes the residual error. The quadratic model lacked the cubic age term, so that: Y i = β 0 + β 1 G j + β 2 Agej + β 3 Age 2j + β 4 (Age × G j) + β 5 (Age 2j × Group) + β 6 IQj + ε i. The linear model lacked cubic and quadratic age terms, so that: Y i = β 0 + β 1 G j + β 2 Agej + β 3 Agej × G j + β 4 IQj + ε i. Subsequently, we examined between-group differences in the neurodevelopmental trajectory of cortical thickness and surface area using the most parsimonious model resulting from the nested model comparison.
Age-related differences in cortical thickness and surface area were firstly examined based on the fixed-effect coefficient β 1 normalized by the corresponding standard error, which indicated significant between-group differences while controlling for the effects of age. Secondly, we examined the interactions between group and each corresponding age term. Thus, for the linear model, we examined the interaction between age × group; for the quadratic model, we examined the interactions between age × group and age2 × group; and for potential cubic growth curves, we examined the interactions between age × group, age2 × group, and age3 × group. This approach allowed us to examine between-group differences and age × group interactions for both linear and more complex age terms. Corrections for multiple comparisons across the whole brain were performed using random-field theory (RFT)-based cluster-corrected analysis for non-isotropic images using a p < 0.05 (two tailed) cluster significance threshold (Worsley et al. 1999).
Results
Subject demographics
There were no significant differences between individuals with ASD and controls in age [t(152) = 1.32, p = 0.186] or full-scale IQ [t(152) = −1.73, p = 0.085]. There were also no significant between-group differences in mean cortical thickness [t(152) = −0.91, p = 0.361] or total surface area [t(152) = 0.23, p = 0.813]. We therefore did not covary for total brain measures in the statistical analysis of cortical thickness and surface area.
Nested model comparisons
For measures of cortical thickness, we found that the quadratic model provided a significantly better goodness of fit than the linear model in several spatially distributed clusters across the cortex (see Fig. 1a for individual regions). However, there was no significant improvement in fit when comparing the quadratic with the more complex cubic model, and no clusters survived correction for multiple comparisons (RFT-based, cluster-corrected, p < 0.05) (Fig. 1b). Thus, we selected the quadratic model as the most parsimonious model for examining between-group differences in cortical thickness (i.e., model with the smallest number of predictors), which also allowed us to investigate age × group interactions for the linear and quadratic age term.

Nested model comparisons for cortical thickness. a Linear vs. quadratic model. b Quadratic model vs. cubic model. Left panel shows the difference map resulting from the model comparison (F statistic, unthresholded). F values (green to blue) indicate voxels where the more complex model fits better than the more reduced model. Right panel indicates random-field theory (RFT)-based, cluster-corrected (p < 0.05) difference maps indicating regions where the more complex model provides a significant better goodness of fit than the simpler model
For vertex-based estimates of surface area, we found that neither quadratic nor cubic age term significantly increased the goodness of fit overall, and there were no clusters in which the more complex models (quadratic or cubic) provided a significantly better fit than the linear model (Fig. 2). Thus, we selected the linear model as the most parsimonious model for examining between-group differences in surface area and the interaction between age × group.

Nested model comparison for surface area. a Linear vs. quadratic model. b Quadratic model vs. cubic model. Left panel shows the difference map resulting from the model comparison (F statistic, unthresholded). F values (green to blue) indicate voxels where the more complex model fits better than the more reduced model. Right panel indicates random-field theory (RFT)-based, cluster-corrected (p < 0.05) difference maps indicating regions where the more complex model provides a significant better goodness of fit than the simpler model
Between-group differences in cortical thickness and interactions with age terms
Based on the outcome of the nested model comparison, a quadratic model was used to examine the effects of group, age, and their interactions on measures of cortical thickness. We found significant reductions in cortical thickness in ASD across the cortex when controlling for the effects of age (linear and quadratic terms), as well as for interactions between group and age terms. Relative to controls, individuals with ASD had significantly reduced cortical thickness (Table 2) in several large frontal lobe clusters (RFT-based cluster-corrected, cluster threshold p < 0.05), which included (1) the right medial orbitofrontal and rostral middle frontal lobe (approximate Brodmann area [BA] 10/11/12/46), (2) medial and lateral superior frontal regions (BA8/9), and (3) in the pars triangularis of the dorsolateral prefrontal cortex (BA44/45). Furthermore, we observed reduced cortical thickness in ASD in a cluster located in the bilateral postcentral gyrus (BA6), the bilateral superior parietal cortex (BA7), the right lingual gyrus (BA19/37), the right inferior and middle temporal lobe (BA20/21), and in the left precentral gyrus (BA4). There were no brain regions in which individuals with ASD showed a significant increase in cortical thickness relative to controls (Fig. 3).

Between-group differences and age-by-group interactions for measures of cortical thickness. a Clusters with significantly reduced cortical thickness measures (RFT-based, cluster-corrected, p < 0.05) in ASD compared to controls while controlling for the effects of age and age-related interactions (i.e., main effect of group). b Clusters with significant interactions between age × group (RFT-based, cluster-corrected, p < 0.05). c Clusters with significant interactions between age2 × group (RFT-based, cluster-corrected, p < 0.05)
Four out of 10 clusters with a significant between-group difference in cortical thickness also displayed a significant linear and quadratic interaction effect of age × group (i.e., age × group, age2 × group, respectively). The clusters in the right superior frontal lobe and in the left superior parietal cortex showed only a significant linear, but not quadratic, age × group interaction. No significant age × group interactions were observed in the right pars triangularis, the left precentral gyrus, the right superior parietal lobe, and in the right lingual gyrus. There were no brain regions with a significant age × group interaction term, but no significant between-group difference in cortical thickness.
In regions with significant age × group interactions, individuals with ASD tend to have reduced cortical thickness during childhood, but increased cortical thickness in adulthood relative to controls (Fig. 5a, b).
Between-group differences in surface area and age × group interactions
Based on the outcome of the nested model comparison, a linear model was used to examine the effects of group, age, and their interactions on vertex-based measures of surface area. Across groups, we found that vertex-based measures of surface area increased significantly with increasing age (i.e., from 7 to 25 years) overall, with strongest correlations being observed in the bilateral anterior inferior temporal lobes, the medial orbitofrontal cortex, the anterior cingulate cortex, and the medial prefrontal cortex (see Figure Supplementary Material). There were no significantly clusters where measures of surface area decreased with age.
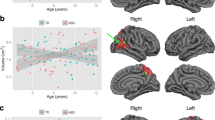
Individuals with ASD had significant reductions in surface area relative to controls, when controlling for the effect of age and for the interaction between age × group. Regions of reduced surface area in ASD included a large frontal cluster (t max = 3.07, N vertices = 4,217, p cluster = 0.005), including the right anterior cingulate gyrus (BA32/33) and the right medial orbitofrontal and rostral middle frontal lobe (BA10/12). We also observed reduced surface area in ASD in the left temporal pole (BA38) (t max = 3.04, N vertices = 3,864, p cluster = 0.023). There were no brain regions in which individuals with ASD showed a significant increase in surface area relative to controls (Fig. 4).

Between-group differences and age-by-group interactions for vertex-based measures of surface area. a Clusters with significantly reduced surface area (RFT-based, cluster-corrected, p < 0.05) in ASD compared to controls while controlling for the effects of age and age-related interactions (i.e., main effect of group). b Clusters indicating significant interactions between age × group (RFT-based, cluster-corrected, p < 0.05)
Furthermore, none of the regions with a significant between-group difference in surface area also displayed a significant age × group interaction. Instead, a significant linear age × group interaction was observed in the postcentral gyrus (BA6) of the left (t max = 4.27, N vertices = 10,007, p cluster = 0.0013) and right hemisphere (t max = 3.10, N vertices = 4,535, p cluster = 0.0025). In these regions, individuals with ASD show reduced measures of surface area during childhood and increased surface area during adulthood compared with controls (see Fig. 5c).

Different types of age × group interactions. a Quadratic interaction between age × group for cortical thickness in left medial orbitofrontal cluster, extending into the rostral middle frontal lobe. b Linear interaction between age × group for cortical thickness in the left superior frontal lobe. c Linear interaction between age × group for surface area in the right postcentral gyrus
Discussion
We report the results of a cross-sectional structural neuroimaging study examining age-related differences in cortical thickness and surface area in a large and well-characterized sample of male adults with ASD, and matched neurotypical controls, between 7 and 25 years of age. Based on prior knowledge of the typical developmental trajectory of gray matter maturation, we examined linear, quadratic, and cubic effects of age in order to identify the statistical model that best predicted developmental trajectories in our sample. We found that measures of cortical thickness were best predicted by a quadratic model, which included a linear and a quadratic age term, while a simple linear model was best suited to predict measures of surface area. When controlling for age effects, individuals with ASD showed significant reductions in cortical thickness across the cortex, and particularly in fronto-temporal regions. In most of these regions, we also observed significant group × age and group × age2 interactions, indicating that individuals with ASD tend to have thinner cortices during childhood but increased cortical thickness during adulthood. Last, we found that individuals with ASD had significant reductions in surface area, in addition to a significant age × group interaction. Thus, our study confirms that there are region-specific between-group differences in cortical thickness and surface area in ASD in addition to age-related interactions and that the direction of differences between groups (i.e., increased or decreased in ASD) heavily depends on the particular age-group of the investigated sample.
Our finding of reduced cortical thickness in ASD—when controlling for age-related effects—agrees with previous studies employing a similar approach in comparable samples (e.g., Raznahan et al. 2010; Wallace et al. 2010; Scheel et al. 2011). However, while previous studies report that age-related cortical thinning is mostly restricted to temporal and parietal regions, our study extends these findings by also reporting extensive reductions in cortical thickness in several areas of the frontal cortex. For example, we found reduced cortical thickness in ASD in the medial and rostral dorsolateral prefrontal cortices, which play a crucial role in the typical development of social cognition and empathy (Lombardo et al. 2007; Blakemore 2008). Moreover, these regions have also been linked to atypical theory of mind (ToM) (Castelli et al. 2002) and self-referential cognition in ASD (Lombardo et al. 2010). One aspect that sets our study apart from others is that we also considered quadratic interactions between group and age in our statistical model, while previous investigations modeled linear effects exclusively (Raznahan et al. 2010; Wallace et al. 2010). It is known from longitudinal studies examining brain maturation in healthy controls that the neurodevelopmental trajectory of cortical thickness is nonlinear in most regions across the cortex, but also includes complex age terms (i.e., cubic and quadratic) resulting in a typical inverted U-shape (Shaw et al. 2006). Thus, our quadratic model, which included a quadratic and linear age term, is expected to be statistically more powerful in comparison with the simple linear model and may explain our finding of cortical thinning in the frontal lobe in ASD. Also, our sample of 77 individuals per group (N total = 154) that are well matched in terms of age, FSIQ, and gender offers increased statistical power in comparison with existing studies, which mostly investigated smaller samples of individuals. Due to the large sample size, we were also able to examine complex interactions between group × age and group × age2. Such complex age × group interactions were predominantly observed in the anterior temporal and prefrontal lobe where individuals with ASD tent to have reductions in cortical thickness during childhood, but increased cortical thickness during adulthood. Thus, it is important to consider such complex age × group interactions when interpreting between-group differences in neuroanatomy in ASD.
Furthermore, we observed a significant reduction in vertex-based measures of surface area in the medial orbitofrontal and anterior temporal lobe in ASD. Anterior temporal lobe abnormalities have previously been linked to the core symptoms of ASD, which center on deficits in language, emotional, and social behavior. For instance, the temporal pole is crucial for high-level social cognitive processes, such as mentalizing (e.g., ToM) and semantic processing (Patterson et al. 2007). Functional MRI studies on ASD also suggest that the recruitment of the anterior temporal lobe is atypical across social cognitive tasks with mentalizing demands such as irony processing (Wang et al. 2009), emotional introspection (Silani et al. 2008), attributing mental states to geometric shapes (Castelli et al. 2002), and language tasks with semantic demands (Gaffrey et al. 2007). Also, we observed reductions in surface area of the anterior cingulate in ASD, which is part of the extended neural system processing emotions (Pessoa 2008), and also plays a major role in general executive functioning that mediate the capacity to shift attention between social and non-social goals and representation (Mundy et al. 2010). Our finding of reduced surface area in these brain regions thus further corroborates their importance in mediating autism-related neurocognitive impairments, particularly in the social domain.
However, while the typical neurodevelopmental trajectory of cortical thickness is well established across the early human life span (see Shaw et al. 2006), there is currently no comparable data indicating the growth trajectory of vertex-based measures of surface area. Here, we found that age × group interactions for surface area were best modeled by a simple linear model, thus suggesting that the neurodevelopmental trajectory of surface area may be different from the neurodevelopmental trajectory of cortical thickness. This agrees with the previous notion that differences in cortical thickness and surface area in ASD may represent neurobiologically distinct mechanisms that are mediated by different sets of genes (Panizzon et al. 2009), distinct phylogenies (Rakic 1995), and also relate to different aspects of the neural architecture. For instance, it has been suggested that both measures originate from different types of progenitor cells, which divide in the ventricular zone to produce glial cells and neurons. Cortical thickness has been related primarily to intermediate progenitor cells (neurogenic transient amplifying cells in the developing cerebral cortex) (Pontious et al. 2008), which divide symmetrically at basal (non-surface) positions of the ventricular surface and only produce neurons (Noctor et al. 2004; Miyata et al. 2004). These neurons then migrate along radial glial fibers to form ontogenetic columns (i.e., radial units). According to the radial unit hypothesis (RUH) (Rakic 1995), cortical thickness depends on the neuronal output from each radial unit—amplified by intermediate progenitor cells—and therefore reflects the number of neurons produced in each unit. On the other hand, surface area has mainly been related to radial unit progenitor cells, which divide at the apical (ventricular) surface. The early proliferation of radial unit progenitor cells leads to an increase in the number of proliferation units, which in turn results in an increase in SA (Pontious et al. 2008). In other words, surface area is related to the number of ontogenetic columns. Our findings therefore suggest that the brain in ASD differs from neurotypical controls in terms of neuronal numbers and the number of cortical minicolumns, which has also been demonstrated by histological studies (e.g., Courchesne et al. 2011; Casanova et al. 2006). In addition to these abnormalities that influence early brain maturation, atypical growth curves of the brain in ASD may also result from abnormalities to mechanisms mediating late brain maturation. For instance, it has been shown that the brain continues to mature until late childhood and/or early adolescence, particularly in temporal and frontal lobes (Giedd et al. 1999). Late brain maturation seems to be driven by a combination of progressive and recessive events including synaptic proliferation, synaptic pruning, and myelination (Huttenlocher and Dabholkar 1997; Paus 2005). Thus, atypical neurodevelopment in ASD may be driven by different aspects of pathology occurring during early and/or late brain maturation.
Notably, age × group interactions in surface area were not observed in regions where we also found a significant between-group difference. For example, we found significant age × group interactions in the bilateral postcentral gyrus (BA6) where surface area did not differ between individuals in ASD and controls overall. Our study is also the first study to report significant age × group interactions for vertex-based estimates of cortical thickness while others, using a similar approach, did not report any significant interactions (e.g., Raznahan et al. 2010; Wallace et al. 2013). This discrepancy may partially be due to differences in sample size and issues of matching and clinical characterization between groups. For instance, participants with ASD were not matched to controls on FSIQ in the study by Raznahan et al. (2010), and not all participants with ASD were diagnosed using ADOS or ADI-R diagnostic criteria (Raznahan et al. 2010). However, significant between-group differences in surface area and age × group interactions have previously been noted by Doyle-Thomas et al. (2013), who found that surface area in the right cingulate was significantly different in ASD, and decreased more rapidly with age in ASD than in controls (Doyle-Thomas et al. 2013). It is thus important for future studies to examine surface area at different stages of development in order to elicit reliable and interpretable differences in ASD.
Our findings should be interpreted in light of a number of methodological considerations. First, we investigated surface-based neuroanatomy in a sample of high-functioning male individuals with ASD (and neurotypical controls), whose diagnostic status was confirmed using the ADI-R. The ADI-R rather than ADOS scores were chosen as exclusion criteria because current symptoms assessed in adult samples can often be masked by coping strategies developed across the life span and can also be alleviated by treatments/interventions (e.g., social skills training). Hence, it is not uncommon for individuals to meet ADI-R (i.e., diagnosis of childhood autism) but not ADOS diagnostic criteria during adulthood. Our sample thus represents a subpopulation of the autistic phenotype, and our results may not generalize to other groups on the autism spectrum (e.g., individuals with intellectual disability) or females with ASD. Second, we employed a cross-sectional design to investigate age-related differences in brain anatomy between groups. While this design enabled us to investigate neuroanatomy across a relatively large age range, it did not allow us to determine neurodevelopmental trajectories for cortical thickness and surface area within individuals. Longitudinal studies are therefore needed to replicate our findings by also taking into account intra-individual variations, and to identify the individual growth trajectories for cortical thickness and surface area. Also, we did not covary for total brain volume as it is a rather ‘convoluted’ measure, which can be further subdivided into distinct neuroanatomical features, e.g., total gray matter volume is a product of total surface area and cortical thickness. Moreover, total brain volume is the sum of total gray and total white matter and thus contains a third component (i.e., white matter) that may not necessarily be correlated with the dependent variable (e.g., one would not expect a significant between-group difference in regional cortical thickness to be driven by differences in total white matter volume). Accordingly, including total brain volume as a covariate may remove not only global effects directly related to the dependent variable, but also eliminate unspecific and indirect effects that would alter the scientific question under investigation. Last, did we not compare the neurodevelopmental trajectories for cortical thickness and surface area directly, but rather indirectly via the nested model comparison. Future research is, however, required to directly compare the individual growth curves for both measures (e.g., via cross-correlation analysis) in order to establish their distinct genetic and neurobiological underpinnings.
To sum up, our cross-sectional study suggests that there are age-related changes in cortical thickness and surface area of the brain across childhood and early adulthood in ASD. We observed significant reductions in cortical thickness and surface area in ASD relative to controls when controlling for the effect(s) of age mainly in fronto-temporal regions. In these regions, we also found significant interactions between group and age terms (linear and quadratic) predominantly for measures of cortical thickness. Our findings thus support the hypothesis that the brain in ASD undergoes an atypical trajectory of brain maturations and that the regions maturing last during typical brain development are also the regions most affected in ASD.
References
Amaral DG, Schumann CM, Nordahl CW (2008) Neuroanatomy of autism. Trends Neurosci 31:137–145. doi:10.1016/j.tins.2007.12.005
Blakemore S-J (2008) The social brain in adolescence. Nat Rev Neurosci 9:267–277. doi:10.1038/nrn2353
Carper RA, Courchesne E (2005) Localized enlargement of the frontal cortex in early autism. Biol Psychiatry 57:126–133. doi:10.1016/j.biopsych.2004.11.005
Casanova MF, van Kooten IAJ, Switala AE et al (2006) Minicolumnar abnormalities in autism. Acta Neuropathol 112:287–303. doi:10.1007/s00401-006-0085-5
Castelli F, Frith C, Happé F, Frith U (2002) Autism, Asperger syndrome and brain mechanisms for the attribution of mental states to animated shapes. Brain 125:1839–1849
Courchesne E, Pierce K (2005) Brain overgrowth in autism during a critical time in development: implications for frontal pyramidal neuron and interneuron development and connectivity. Int J Dev Neurosci 23:153–170. doi:10.1016/j.ijdevneu.2005.01.003
Courchesne E, Mouton PR, Calhoun ME et al (2011) Neuron number and size in prefrontal cortex of children with autism. JAMA 306:2001–2010. doi:10.1001/jama.2011.1638
Dale AM, Fischl B, Sereno MI (1999) Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage 9:179–194. doi:10.1006/nimg.1998.0395
Doyle-Thomas KAR, Kushki A, Duerden EG et al (2013) The effect of diagnosis, age, and symptom severity on cortical surface area in the cingulate cortex and insula in autism spectrum disorders. J Child Neurol 28:732–739. doi:10.1177/0883073812451496
Ecker C, Suckling J, Deoni SC et al (2012) Brain anatomy and its relationship to behavior in adults with autism spectrum disorder: a multicenter magnetic resonance imaging study. Arch Gen Psychiatry 69:195–209. doi:10.1001/archgenpsychiatry.2011.1251
Ecker C, Ginestet C, Feng Y et al (2013a) Brain surface anatomy in adults with autism: the relationship between surface area, cortical thickness, and autistic symptoms. JAMA Psychiatry 70:59–70. doi:10.1001/jamapsychiatry.2013.265
Ecker C, Ronan L, Feng Y et al (2013b) Intrinsic gray-matter connectivity of the brain in adults with autism spectrum disorder. Proc Natl Acad Sci USA. doi:10.1073/pnas.1221880110
Fischl B, Sereno MI, Dale AM (1999a) Cortical surface-based analysis. II: inflation, flattening, and a surface-based coordinate system. Neuroimage 9:195–207. doi:10.1006/nimg.1998.0396
Fischl B, Sereno MI, Tootell RB, Dale AM (1999b) High-resolution intersubject averaging and a coordinate system for the cortical surface. Hum Brain Mapp 8:272–284
Gaffrey MS, Kleinhans NM, Haist F et al (2007) Atypical [corrected] participation of visual cortex during word processing in autism: an fMRI study of semantic decision. Neuropsychologia 45:1672–1684. doi:10.1016/j.neuropsychologia.2007.01.008
Geschwind DH, Levitt P (2007) Autism spectrum disorders: developmental disconnection syndromes. Curr Opin Neurobiol 17:103–111. doi:10.1016/j.conb.2007.01.009
Giedd JN, Blumenthal J, Jeffries NO et al (1999) Brain development during childhood and adolescence: a longitudinal MRI study. Nat Neurosci 2:861–863. doi:10.1038/13158
Hardan AY, Muddasani S, Vemulapalli M et al (2006) An MRI study of increased cortical thickness in autism. Am J Psychiatry 163:1290–1292. doi:10.1176/appi.ajp.163.7.1290
Hardan AY, Libove RA, Keshavan MS et al (2009) A preliminary longitudinal magnetic resonance imaging study of brain volume and cortical thickness in autism. Biol Psychiatry 66:320–326. doi:10.1016/j.biopsych.2009.04.024
Hazlett HC, Poe MD, Gerig G et al (2011) Early brain overgrowth in autism associated with an increase in cortical surface area before age 2 years. Arch Gen Psychiatry 68:467–476. doi:10.1001/archgenpsychiatry.2011.39
Huttenlocher PR, Dabholkar AS (1997) Regional differences in synaptogenesis in human cerebral cortex. J Comp Neurol 387:167–178
Hyde KL, Samson F, Evans AC, Mottron L (2010) Neuroanatomical differences in brain areas implicated in perceptual and other core features of autism revealed by cortical thickness analysis and voxel-based morphometry. Hum Brain Mapp 31:556–566. doi:10.1002/hbm.20887
Langen M, Durston S, Staal WG et al (2007) Caudate nucleus is enlarged in high-functioning medication-naive subjects with autism. Biol Psychiatry 62:262–266. doi:10.1016/j.biopsych.2006.09.040
Langen M, Leemans A, Johnston P et al (2011) Fronto-striatal circuitry and inhibitory control in autism: findings from diffusion tensor imaging tractography. Cortex. doi:10.1016/j.cortex.2011.05.018
Lombardo MV, Barnes JL, Wheelwright SJ, Baron-Cohen S (2007) Self-referential cognition and empathy in autism. PLoS One 2:e883. doi:10.1371/journal.pone.0000883
Lombardo MV, Chakrabarti B, Bullmore ET et al (2010) Atypical neural self-representation in autism. Brain 133:611–624. doi:10.1093/brain/awp306
Lord C, Rutter M, Goode S et al (1989) Autism diagnostic observation schedule: a standardized observation of communicative and social behavior. J Autism Dev Disord 19:185–212
Lord C, Rutter M, Le Couteur A (1994) Autism diagnostic interview-revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord 24:659–685
Mak-Fan KM, Taylor MJ, Roberts W, Lerch JP (2011) Measures of cortical grey matter structure and development in children with autism spectrum disorder. J Autism Dev Disord. doi:10.1007/s10803-011-1261-6
McAlonan GM, Cheung V, Cheung C et al (2005) Mapping the brain in autism. A voxel-based MRI study of volumetric differences and intercorrelations in autism. Brain 128:268–276. doi:10.1093/brain/awh332
Miyata T, Kawaguchi A, Saito K et al (2004) Asymmetric production of surface-dividing and non-surface-dividing cortical progenitor cells. Development 131:3133–3145. doi:10.1242/dev.01173
Mundy P, Gwaltney M, Henderson H (2010) Self-referenced processing, neurodevelopment and joint attention in autism. Autism 14:408–429. doi:10.1177/1362361310366315
Noctor SC, Martínez-Cerdeño V, Ivic L, Kriegstein AR (2004) Cortical neurons arise in symmetric and asymmetric division zones and migrate through specific phases. Nat Neurosci 7:136–144. doi:10.1038/nn1172
Nordahl CW, Scholz R, Yang X et al (2012) Increased rate of amygdala growth in children aged 2 to 4 years with autism spectrum disorders: a longitudinal study. Arch Gen Psychiatry 69:53–61. doi:10.1001/archgenpsychiatry.2011.145
Panizzon MS, Fennema-Notestine C, Eyler LT et al (2009) Distinct genetic influences on cortical surface area and cortical thickness. Cereb Cortex 19:2728–2735. doi:10.1093/cercor/bhp026
Patterson K, Nestor PJ, Rogers TT (2007) Where do you know what you know? The representation of semantic knowledge in the human brain. Nat Rev Neurosci 8:976–987. doi:10.1038/nrn2277
Paus T (2005) Mapping brain maturation and cognitive development during adolescence. Trends Cogn Sci (Regul Ed) 9:60–68. doi:10.1016/j.tics.2004.12.008
Pessoa L (2008) On the relationship between emotion and cognition. Nat Rev Neurosci 9:148–158. doi:10.1038/nrn2317
Pontious A, Kowalczyk T, Englund C, Hevner RF (2008) Role of intermediate progenitor cells in cerebral cortex development. Dev Neurosci 30:24–32. doi:10.1159/000109848
Rakic P (1995) A small step for the cell, a giant leap for mankind: a hypothesis of neocortical expansion during evolution. Trends Neurosci 18:383–388
Raznahan A, Toro R, Daly E et al (2010) Cortical anatomy in autism spectrum disorder: an in vivo MRI study on the effect of age. Cereb Cortex 20:1332–1340. doi:10.1093/cercor/bhp198
Raznahan A, Shaw P, Lalonde F et al (2011) How does your cortex grow? J Neurosci 31:7174–7177. doi:10.1523/JNEUROSCI.0054-11.2011
Redcay E, Courchesne E (2008) Deviant functional magnetic resonance imaging patterns of brain activity to speech in 2-3-year-old children with autism spectrum disorder. Biol Psychiatry 64:589–598. doi:10.1016/j.biopsych.2008.05.020
Scheel C, Rotarska-Jagiela A, Schilbach L et al (2011) Imaging derived cortical thickness reduction in high-functioning autism: key regions and temporal slope. Neuroimage 58:391–400. doi:10.1016/j.neuroimage.2011.06.040
Schumann CM, Barnes CC, Lord C, Courchesne E (2009) Amygdala enlargement in toddlers with autism related to severity of social and communication impairments. Biol Psychiatry 66:942–949. doi:10.1016/j.biopsych.2009.07.007
Schumann CM, Bloss CS, Barnes CC et al (2010) Longitudinal magnetic resonance imaging study of cortical development through early childhood in autism. J Neurosci 30:4419–4427. doi:10.1523/JNEUROSCI.5714-09.2010
Ségonne F, Dale AM, Busa E et al (2004) A hybrid approach to the skull stripping problem in MRI. Neuroimage 22:1060–1075. doi:10.1016/j.neuroimage.2004.03.032
Shaw P, Lerch J, Greenstein D et al (2006) Longitudinal mapping of cortical thickness and clinical outcome in children and adolescents with attention-deficit/hyperactivity disorder. Arch Gen Psychiatry 63:540–549. doi:10.1001/archpsyc.63.5.540
Silani G, Bird G, Brindley R et al (2008) Levels of emotional awareness and autism: an fMRI study. Soc Neurosci 3:97–112. doi:10.1080/17470910701577020
Waiter GD, Williams JHG, Murray AD et al (2004) A voxel-based investigation of brain structure in male adolescents with autistic spectrum disorder. Neuroimage 22:619–625. doi:10.1016/j.neuroimage.2004.02.029
Wallace GL, Dankner N, Kenworthy L et al (2010) Age-related temporal and parietal cortical thinning in autism spectrum disorders. Brain 133:3745–3754. doi:10.1093/brain/awq279
Wallace GL, Robustelli B, Dankner N et al (2013) Increased gyrification, but comparable surface area in adolescents with autism spectrum disorders. Brain 136:1956–1967. doi:10.1093/brain/awt106
Wang K, Zhang H, Ma D et al (2009) Common genetic variants on 5p14.1 associate with autism spectrum disorders. Nature 459:528–533. doi:10.1038/nature07999
Wechsler D (1999) Wechsler abbreviated scale of intelligence (WASI). Harcourt Assessment, San Antonio
Wing L (1997) The autistic spectrum. Lancet 350:1761–1766. doi:10.1016/S0140-6736(97)09218-0
Winkler AM, Sabuncu MR, Yeo BTT et al (2012) Measuring and comparing brain cortical surface area and other areal quantities. Neuroimage. doi:10.1016/j.neuroimage.2012.03.026
Worsley KJ, Andermann M, Koulis T et al (1999) Detecting changes in nonisotropic images. Hum Brain Mapp 8:98–101
Acknowledgments
This work was supported (1) by the Medical Research Council UK (G0400061 and G0800298), (2) by the Dr. Mortimer and Theresa Sackler Foundation, (3) by the EU-AIMS project (European Autism Interventions—a Multicentre Study for developing New Medications) receiving support from the Innovative Medicines Initiative Joint Undertaking under grant agreement no. 115300, which includes financial contributions from the EU Seventh Framework Programme (FP7/2007-2013), (4) by the NIHR Biomedical Research Centre for Mental Health at King’s College London, Institute of Psychiatry, and (5) by the South London & Maudsley NHS Foundation Trust. We are also grateful to those who agreed to be scanned and who gave their time so generously to this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
C. Ecker and A. Shahidiani contributed equally to the manuscript.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

{kind=link}
Cite this article
Ecker, C., Shahidiani, A., Feng, Y. et al. The effect of age, diagnosis, and their interaction on vertex-based measures of cortical thickness and surface area in autism spectrum disorder. J Neural Transm 121, 1157–1170 (2014). https://doi.org/10.1007/s00702-014-1207-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00702-014-1207-1