
Abstract
We present a rare and interesting case of a cerebellopontine angle cyst containing ectopic choroid plexus tissue in a 26 year-old female. Surgical resection was performed, and histological examination confirmed the presence of choroid plexus in the cyst wall. This is the first reported case of ectopic choroid plexus at the cerebellopontine angle in an adult. We present the case and review the literature.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Case report
A 26-year-old female who suffered from uncomplicated viral encephalitis as a young child presented with a 2-year history of rotational vertigo associated with a right-sided hearing loss and constant tinnitus. Her vertigo could last up to 90 min and occurred two to three times per month, at any time and in any position. She was otherwise well. Clinical examination was unremarkable, other than a sensorineural deafness on the right, confirmed by formal audiometry. She had no cerebellar signs, her gait and balance were normal, nor was there nystagmus, dysdiadokinesis or finger-nose dysmetria.
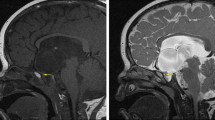
Magnetic resonance imaging revealed a 3.7 × 1.4-cm right-sided cerebellopontine angle cyst. There was no evidence of hydrocephalus or mass effect (Fig. 1)

High-resolution MRI illustrating preoperative cerebellopontine angle cyst extension
A right sub-occipital craniotomy was performed. The cyst was identified, with the 7th and 8th cranial nerve complex deep to it. This tissue was distinct and several centimetres away from the foramen of Luske, and separated by the cyst wall from surrounding structures. The lateral cyst wall was incised, revealing a cavity containing clear CSF, which was under moderate pressure. The cyst contained tissue within its wall that appeared macroscopically similar in morphology to normal choroid plexus (Fig. 2). All ectopic tissue was microsurgically resected, and the medial wall of the cyst was incised, allowing communication with the midline subarachnoid cisterns. Histological examination revealed papillary tissue comprising monolayered, bland cuboidal epithelium overlying fibrovascular cores, in keeping with normal choroid plexus (Fig. 3). There were no intra-operative complications. She made an uncomplicated recovery and was discharged home 3 days after surgery.

Intra-operative view after resection of the lateral wall of the cyst. Ectopic choroid plexus in the wall of the cyst indicated by the arrow. Cranial nerve 7 and 8 complex deep to the cyst wall (VII/VIII)

Microscopic examination of biopsies taken from the cyst shows papillary tissue comprising monolayered bland cuboidal epithelium overlying fibrovascular cores in keeping with histologically normal choroid plexus (H&E)
Discussion
Cystic lesions of the cerebellopontine angle include arachnoid cysts [6] as well as neoplastic lesions, including schwannomas of the seventh and eighth cranial nerves. Arachnoid cysts can occur anywhere in the central nervous system, and their aetiology is unknown. One possibility is that their formation derives from abnormal CSF flow causing splitting of the arachnoid membrane. They may be congenital and are commonly incidental findings in adults. Some have been linked to a post-traumatic or inflammatory aetiology [2, 6], but it is likely that the majority are not. Thus they may not represent a single aetiology, but rather a group of pathological processes, which may explain the variation in histological appearances [3].
One mechanism for cyst formation and growth is the presence of CSF-secreting choroid plexus within the cyst wall. Intracranial cysts that contain choroid plexus that are not in continuity with the ventricular system—i.e., they contain true ectopic choroid tissue—are rare. To our knowledge there are only five reported cases of intracranial cysts containing true ectopic choroid plexus; three were supratentorial [1, 5, 11], one was intramedullary [4], and a cerebellopontine angle cyst containing choroid plexus in a child has also been reported [12] (Table 1). There is also a reported case of extracranial ectopic choroid plexus causing cyst formation in the oropharynx of a neonate [8]. To our knowledge this is the first report of ectopic choroid plexus associated with a cerebellopontine angle cyst in an adult.
The choroid plexus develops from the ependyma and overlying vascular pia in the choroid fissures of the lateral ventricles. It also differentiates from the same cell types in the third and fourth ventricles [7]. The choroid plexus has been implicated in the development of the foetal brain, providing a chemical environment that promotes neuronal growth, as well as producing chemotactic and chemoprotective agents that aid neuronal migration as well as protecting sensitive foetal cells. This process has also been shown to occur in the developing neonatal and infant brain. It diminishes throughout life and may be a factor that predisposes to neurodegenerative disorders as humans age [9].
With this information, one could hypothesise that a biochemical insult to the developing brain, such as would occur from an encephalitis, may lead to an increase in cerebrospinal fluid production from developing choroid plexus. If this were true, it would also be conceivable that choroid plexus hyperplasia may also result. The same stimulus may promote choroid plexus differentiation from ependyma and vascular pia that maintained an element of pluripotency in other regions other than the ventricular system. Previous case reports of ectopic choroid plexus in the central nervous system do not mention if the patients suffered a neuro-inflammatory condition in infancy. This theory is entirely conjectural, but may help to explain the presence of choroid ectopia. A malformative origin is also plausible; however, a complete absence of any brain malformation in this case and all previous cases makes it unlikely.
Conclusion
We present the first case of ectopic choroid plexus causing cyst formation in the cerebellopontine angle of an adult. Cases of ectopic choroid plexus tissue are rare. We suggest, as have previous authors, that arachnoid cysts should be carefully inspected at the time of operation to exclude the presence of ectopic choroid plexus. It may, therefore, be more common than previously reported. We hypothesise that the formation of such ectopic tissue may be the result of a biochemical insult to the brain in infancy.
References
Azzam NI, Timperley WR (1981) Intracerebral cyst due to ectopic choroid plexus: case report. J Neurosurg 55(4):651–653
Choi J, Kim D (1998) Pathogenesis of arachnoid cyst: congenital or traumatic? Pediatr Neurosurg 29:260–266
Di Rocco C (1999) Arachnoid cysts of the posterior fossa (comment). Surg Neurol 51:376–382
Dwarakanath S, Suri A, Mahapatra AK, Mehta VS, Sharma MC (2005) Intramedullary ectopic choroid plexus: report of a rare case. Neurosurgery 56(4):E869
Iglesias JR, Sanjuanbenito L, Martinez-Cubells J, Lousa M, Redondo C (1981) Intracerebral arachnoid cyst containing choroid plexus. Case report. Acta Neurochir (Wien) 58:229–234
Jallo GI, Woo HH, Meshki C, Epstein FJ, Wisoff JH (1997) Arachnoid cysts of the cerebellopontine angle: diagnosis and surgery. Neurosurgery 40:31–38
Larsen WJ. 2001. Development of the brain and cranial nerves, from Human Embryology. 3rd Edn. Ed. Churchill Livingstone
Lasjaunias P, Ginisty D, Comoy J, Landrieu P (1985/1986) Ectopic secreting choroid plexus in the oropharynx. Pediatr Neurosci 12(4–5):205–207
Redzic ZB, Preston JE, Duncan JA, Chodobski A, Szmydynger-Chodobska J (2005) The choroid plexus-cerebrospinal fluid system: from development to aging. Curr Top Dev Biol 71:1–52
Rengachary SS, Watanabe I, Brackett CE (1978) Pathogenesis of intracranial arachnoid cysts. Surg Neurol 8:119–144
Rosich-Pla A, Smith BH, Sil R (1977) Congenital arachnoid cyst with unusual clinical, radiological and pathological findings. Ann Neurol 2:443–446
Schuhmann MU, Tatagiba M, Hader C, Brandis A, Samii M (2000) Ectopic choroid plexus within a juvenile arachnoid cyst of the cerebellopontine angle: cause of cyst formation or reason of cyst growth. Pediatr Neurosurg 32(2):73–76
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
Arachnoid cyst, generally speaking, remains an intriguing condition. In this unusual location, the presence of a small ectopic nest of choroid plexus gives a sound pathophysiological explanation to the growing of the cyst. Post-infectious or post-inflammatory septation of the subarachnoid spaces could be another hypothesis but more difficult to prove. According to the review presented by the authors, all these arachnoid cysts associated with ectopic choroid plexus were symptomatic, and the indication to operate was thus straightforward; complications were not reported, and prognosis is excellent.
Benedict Rilliet
Switzerland
Rights and permissions
About this article
Cite this article
Singleton, W.G.B., Lawrence, T., Green, A.L. et al. Cerebellopontine angle arachnoid cyst containing ectopic choroid plexus—case report. Acta Neurochir 152, 881–883 (2010). https://doi.org/10.1007/s00701-009-0516-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0516-x