
Abstract
Aim
Preclinical studies suggested that insulin, incretin and thiazolidinediones had effect on regulation of bone metabolism. But clinical evidence is limited. We assessed the effects of these antihyperglycemic agents on bone metabolism in patients with newly diagnosed type 2 diabetes.
Methods
The present study was a two-center, randomized, parallel-group clinical trial. Sixty-two newly diagnosed and drug-naïve patients with type 2 diabetes were randomized to exenatide (EXE, n = 20), mixed protamine zinc recombinant human insulin lispro injection (25R; INS, n = 21) or pioglitazone (PIO, n = 21) group for a 24-week treatment. Glycosylated hemoglobin A1c (HbA1c), body weight, body mineral density (BMD) and fasting serum concentration of bone turnover markers including osteocalcin (OC), C-telopeptide of type I collagen (CTX) and tartrate-resistant alkaline phosphatase 5b (TRAcP5b) were assessed at baseline and week 24.
Results
Baseline characteristics were similar among groups. At week 24, HbA1c improved in all patients (EXE:−2.4 ± 0.3 %, INS:−2.4 ± 0.3 %, PIO:−2.0 ± 0.2 %; p > 0.05 among groups). Patients treated with exenatide lost body weight remarkably (−4.7 ± 0.8 kg). In spite of the amelioration of glucose control, no significant improvement of OC, CTX or TRAcP5b was observed at week 24 (EXE: OC −0.619 ± 0.728 ng/ml, CTX 0.147 ± 0.046 ng/ml, TRAcP5b 0.302 ± 0.149 U/L;INS: OC 0.637 ± 0.787 ng/ml, CTX −0.012 ± 0.074 ng/ml, TRAcP5b 0.124 ± 0.395 U/L; PIO: OC −0.150 ± 0.691 ng/ml, CTX 0.073 ± 0.094 ng/ml, TRAcP5b 0.586 ± 0.183 U/L; p > 0.05), as well as BMD measurement, regardless of the treatments.
Conclusions
Twenty-four-week treatment with exenatide, insulin and pioglitazone improved glucose control in patients with newly diagnosed type 2 diabetes, but had no impact on bone turnover markers or BMD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
A low bone mineral density (BMD) has been consistently observed in type 1 diabetes, while in type 2 diabetes BMD is similar to or even higher than age-matched nondiabetic controls [1]. However, type 2 diabetes mellitus is still associated with an increased risk of bone fractures [2–4]. Contributing factors include chronic hyperglycemia, impaired vitamin D metabolism, peripheral and autonomic neuropathy, and falls resulting from hypoglycemia (Maggi et al. [5, 6]). The impaired skeletal strength in type 2 diabetes is only in part reflected by a variation in BMD.
It is known that hyperglycemia exerts negative effects on both bone formation and bone resorption [7]. Accordingly, antihyperglycemic agents may theoretically counter the detrimental effects of diabetes on bone health. Preclinical data have suggested that insulin and glucagon-like peptide (GLP)-1 receptor agonist play an important role on anabolic action on bone metabolism in addition to their beneficial effects on glucose [8, 9], while clinical evidence of these two categories of agents on bone health is still limited. On the other hand, recent studies suggest that thiazolidinedione (TZD) treatment is associated with an increased risk of bone fractures in patients with type 2 diabetes, especially in postmenopausal female patients [10]. These findings emphasize the need to investigate the effect of antihyperglycemic agents on bone metabolism.
To date, comparative effect of insulin, GLP-1 receptor agonist and TZDs on bone metabolism, especially in patients with newly diagnosed type 2 diabetes, is still lacking. This present study was therefore designed to assess the effects of 24-week treatment of these three antihyperglycemic agents on both glucose control and bone metabolism in patients with newly diagnosed type 2 diabetes.
Methods
Patients and study design
This study is an ancillary study of CONFIDENCE study (registered at Clinical Trials.gov with Number NCT01147627). Detailed methods and results of the CONFIDENCE study have been published previously [11]. Briefly, the present study is a 24-week, two-center (the Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, and Drum Tower Hospital Affiliated to Nanjing University Medical School, Nanjing), randomized controlled trial. Treatment-naïve patients with newly diagnosed type 2 diabetes, aged 30–70 years, were recruited. Inclusion criteria were glycosylated hemoglobin A1c (HbA1c) 7.0–10.0 % (53–86 mmol/mol), body mass index (BMI) 20–35 kg/m2 and stable body weight for ≥3 months. Exclusion criteria were acute or severe chronic diabetic complications or illness (ketoacidosis, hyperosmotic state, lactic acidosis, severe micro- and macrovascular complications, neuropathy, retinopathy, nephropathy, hepatic dysfunction); the presence of glutamic acid decarboxylase antibodies; use of drugs affecting bone metabolism, gastrointestinal motility, weight and glycemia; a history of preexisting osteoporosis or pathologic fracture; a history of secondary osteoporosis; a history of pancreatitis; or triglycerides (TG) ≥5 mmol/L.
The study protocol was approved by each site’s ethical review committee in accordance with the Declaration of Helsinki. All participating patients gave their written informed consent prior to screening.
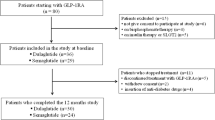
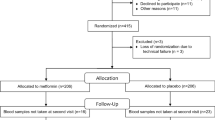
In total, 62 drug-naïve patients with newly diagnosed type 2 diabetes were enrolled from August 2010 to August 2012. With a randomization list generated using statistics analysis system (SAS; SAS Institute Inc., Cary, NC, USA), the patients were randomly assigned to exenatide (n = 20), insulin (n = 21) or pioglitazone group (n = 21).
Exenatide (Amylin Pharmaceuticals, Inc., San Diego, CA, USA) was injected subcutaneously at a dose of 5 μg twice daily, increasing to 10 μg twice daily after 4 weeks. Premixed insulin [mixed protamine zinc recombinant human insulin lispro injection (25R); Eli Lilly and Company, Indianapolis, IN, USA] was injected twice daily at an initial dose of 0.4 IU/kg daily, with 50 % administered 15 min before breakfast and the remaining 50 % administered 15 min before dinner. Thereafter, doses were titrated based on self-monitored blood glucose levels (Table S1). Pioglitazone (Deyuan Pharmacy, Jiangsu, China) was initially administered at 30 mg daily, increasing to 45 mg daily after 4 weeks.
All patients received diabetes information and lifestyle counseling at enrollment, with reinforcement throughout the study.
Measurements
At baseline, anthropometric data were recorded. Fasting venous blood samples were collected at 7:00 a.m.–9:00 a.m. to measure fasting plasma glucose (FPG), HbA1c, lipids, insulin (FINS), fasting serum concentration of bone formation marker osteocalcin (OC) and bone resorption markers, including C-telopeptide of type I collagen (CTX) and tartrate-resistant alkaline phosphatase 5b (TRAcP5b). A mixed meal test was performed with blood samples collected 120 min after injection to determine glucose (PPG) and insulin level. Samples were left to clot at room temperature for 30 min and then centrifuged. Aliquots of the serum supernatant were frozen and stored at –80 °C and subsequently thawed and analyzed in one batch for measurement of bone turnover markers. After 24-week treatment, all measurements at baseline were repeated with patients instructed to stop all antihyperglycaemic therapy 2 days before hand to avoid any acute drug effects on the collected data. BMD was measured at baseline and week 24.
Homeostasis model assessment was used to assess β-cell function [HOMA-β = (20 × FINS)/(FPG − 3.5)] and insulin resistance [HOMA-IR = (FPG × FINS)/22.5]. Area under the curve for glucose (AUCglu) is calculated by using trapezoidal rule. FPG and PPG were assessed by GOD-POD method, while HbA1c was measured by high-pressure liquid chromatography (HPLC), whereas insulin level by electrochemiluminescence assay. OC, CTX and TRAcP5b were assessed using standard enzyme-linked immunosorbent assays (ELISAs, IDS, UK). BMD was measured by dual-energy X-ray absorptiometry (DXA) (Discovery A, Hologic, USA).
Safety and tolerability were assessed at each visit by the investigators. Minor hypoglycemia was defined as symptoms confirmed by a blood glucose concentration <3.9 mmol/L, with prompt recovery after self-administered carbohydrate. Major hypoglycemia was defined as an event requiring the assistance of another person to administer carbohydrate, glucagon or other resuscitative treatment.
Statistical analysis
The primary end point of the study was the change in OC, the marker of bone formation. Eighteen patients per group were required to provide 80 % power at the 5 % significance level to detect differences of at least 90 % of 1 standard deviation (SD) among different treatments [8]. The estimated dropout rate was 10 %, and thus, 60 patients were required for enrollment.
HOMA-β and HOMA-IR were logarithmically transformed prior to statistical analysis. All outcome measures were analyzed using mixed-model repeated-measures analysis of covariance (ANCOVA) to estimate the change in variables, with treatment (exenatide/insulin/pioglitazone), center (Guangzhou/Nanjing), baseline HbA1C and the pretreatment variable of the corresponding dependent variable as covariates. Pearson’s correlation analysis was used to evaluate the correlations between the change in BMD or bone turnover markers from week 24 to baseline and the change in metabolic parameters from week 24 to baseline in all the patients. Statistical analysis was performed using SPSS 17.0 (SPSS, USA). All inferential statistical tests were conducted at a significant level of 0.05 (two-sided). Unless otherwise stated, data are presented as mean ± SEM.
Result
Overall, 62 patients were enrolled and assigned randomly in a 1:1:1 ratio to exenatide (n = 20), insulin (n = 21) or pioglitazone group (n = 21). All patients completed the 24-week follow-up. Baseline clinical characteristics were similar among treatment groups (Table 1).
FPG, PPG and HbA1c decreased significantly in all patients throughout the study (Table 2). The AUCglu during MMT was also decreased at the end of the study compared to that at baseline (Table 2). No between-treatment differences at week 24 were found regarding glucose improvement. As shown in Table 2, HOMA-β was significantly improved after 24-week treatment with insulin compared to other treatments. Exenatide and pioglitazone treatments improved HOMA-IR at week 24, but no between-treatment difference was observed. After adjusting by HOMA-IR, no between-treatment difference of HOMA-β was noted (p = 0.066).
Changes in body weight are presented in Table 2. At week 24, exenatide, as compared to insulin and pioglitazone treatments, significantly decreased body weight and BMI. No significant body weight gain was observed in insulin or pioglitazone group.
At week 24, changes in bone turnover markers from baseline were similar in three groups. No significant effect on bone turnover markers was observed, regardless of any treatments (Table 3). These results did not change even after adjusting by age, gender, menopause or not, baseline BMI and baseline HbA1c. Similar with bone turnover markers, BMD also remained unaffected following 24-week treatments (Table 3).
To further analyze the association between bone turnover markers and metabolic parameter, correlation analysis was applied. A statistically significant negative correlation was found between the change in CTX and the change in weight from baseline [correlation coefficient (r) = −0.30, p = 0.02], as well as the change in BMI [correlation coefficient (r) = −0.28, p = 0.03] with Pearson’s correlation analysis.
Exenatide, insulin and pioglitazone treatments were generally well tolerated. Adverse events are shown in Table S2. Gastrointestinal reactions were the most frequently reported adverse events in exenatide group. No bone fractures were reported during the follow-up period. There were no major hypoglycemia and serious adverse event occurring in this study. Incidences of minor hypoglycemia were 5 % in exenatide group, 9.5 % in insulin group and 4.8 % in pioglitazone group.
Discussion
The most recent set of guidelines encourages a patient-centric approach that takes into account the specific role of each drug and patient factors, which raises attention to effects of antihyperglycemic agents on not only glucose-lowering efficacy but also other actions beyond glucose, such as bone metabolism. To our knowledge, the present study is the first study directly comparing the effects of exenatide, insulin and pioglitazone on both glucose and bone metabolism in drug-naïve patients with newly diagnosed type 2 diabetes. Our results indicated that 24-week treatment with exenatide, insulin and pioglitazone improved glucose control, but not yet affected bone turnover markers and BMD.
The effect of exenatide, insulin and pioglitazone on glycemic control in the present study is similar with those observed in CONFIDENCE study previously reported [11] and other studies [12–14]. Significant weight reduction was found in patients treated with exenatide. No weight change was observed in patients treated with insulin or pioglitazone, probably because of the lifestyle modification under diabetes education and the relatively short-term interventions.
Previous studies in type 2 diabetes have shown the decreased levels of bone turnover markers in type 2 diabetic patients compared to nondiabetic control subjects [15, 16]. And some studies indicated that improved glycemic control in diabetic patients resulted in change in bone turnover markers [17–19], which is not found in the present study. Although it is well accepted in cross-sectional studies that serum OC is inversely related to glycemic control [20–23], effects of improved glycemic control on OC observed in longitudinal studies are still inconsistent. Several studies reported an increase in OC in diabetic patients who entered each study with poorly controlled glycemia and achieved improved control [17–19, 24]. But another 1-year study found that improving glycemic control reduced OC levels [25]. And similar to our result, Hong et al. [26] and Poomthavorn et al. [27] showed that changes in serum total OC level were not associated with the changes in glucose, although the interventions in these two studies were bisphosphonate and vitamin D2, respectively. It is still not clear what factors induce these controversial results. What should be addressed is that bone turnover markers levels were shown to be correlated with diabetes duration [15]. The subjects in our study are patients with newly diagnosed type 2 diabetes and were treated with monotherapy of hypoglycemic agents for 6 months, who are quite different with those patients enrolled in other studies. It may be inferred that the difference in patients’ diabetes duration between our study and other studies partly contributes to the inconsistency. Moreover, ethnic differences in bone turnover markers levels reported in other studies might explain in part the discrepancy of our results and others [28]. More details about the association between changes in serum OC levels and changes in glycemic status are needed to be investigated in well-designed, long-term, prospective, longitudinal clinical trial.
More recent basic research data support that GLP-1 is involved in bone metabolism [29]. It has been demonstrated that incretin hormones can stimulate osteoblastogenesis indirectly via increasing insulin secretion as well as through a direct action on osteoblasts. Moreover, incretin hormones can inhibit osteoclastogenesis by stimulating calcitonin production in diabetes mellitus, which is independent of glycemic control [30]. A three-day GLP-1 administration exerted osteogenic effects in type 2 diabetic rat models with increased bone formation markers OC and osteoprotegerin (OPG), and reduced bone structure anisotropy assessing with microcomputerized tomography [31, 32]. The accumulating experimental data raise an interesting hypothesis that GLP-1 could be a useful therapeutic agent for improving the deficient bone formation and bone structure in addition to its glucose efficiency. However, the potential improvement of bone metabolism by exenatide was not yet confirmed in clinical settings.
The effect of exenatide and insulin treatments on bone metabolism presented in this study is in agreement with other studies. A 44-week study conducted in metformin-treated patients showed that neither exenatide nor insulin glargine as add-on therapy has influence on bone density, despite different effect on body weight [33]. And 1-year treatment with a dipeptidylpeptidase-4 inhibitor vildaglptin, another incretin-based drug, was not associated with changes in bone resorption markers in drug-naïve patients with type 2 diabetes whose baseline HbA1c was 6.0 % [34].
It is believed that the imbalance of bone turnover and osteoblast activity contribute to the impaired bone metabolism in type 2 diabetes, which may be detected much earlier than the change in BMD [35]. That is why assessments of not only BMD but also bone metabolism markers, including both bone formation markers and bone resorption markers, are even more clinically significant. Controversial to the animal studies, both formation marker (OC), resorption markers (CTX, TRAcP5b) and BMD remained unaffected following 24-week treatments in the present study, although fasting glucose and HbA1C decreased by GLP-1 agonist treatment. Consequently, there could be other factors associated with bone metabolism leading to this negative result even under optimal glucose control. Firstly, it was demonstrated that body weight reduction was associated with decreased BMD and increased bone resorption, especially in obese postmenopausal women [36, 37]. A decrease in total BMD was observed with the significant weight reduction 1 year after Roux-en-Y gastric bypass surgery [38]. And the reduced levels of bone turnover markers and abnormal vitamin D metabolism were found in obese women during the 5-year follow-up after short-term weight loss therapy [39]. It is also found in this study that the change in bone resorption marker CTX was negatively correlated with the change in weight from baseline. Abundant evidence of the weight-reduction effect of GLP-1 receptor agonist was cumulated in many clinical trials. However, no obvious weight change was induced in animal studies with short-term GLP-1 treatment, which may be the key reason leading to the difference between preclinical and clinical studies. In addition, experimental data from rodents suggested that administration of calcitonin, a peptide secreted from thyroid C cells, reduced bone resorption markers in urine [40]. And GLP-1 receptor agonist administration increased calcitonin gene expression in the thyroid of wild-type mice [40]. These findings indicate that GLP-1 receptor may have a role in bone resorption indirectly through a calcitonin-dependent pathway in thyroid C cells by stimulating calcitonin releasing [40, 41]. Nevertheless, important species-specific differences in C cell histology, namely a higher GLP-1 receptor expression in C cell related lesion in rodents than in humans, do exist [42, 43]. It is highly possible that this species-specific difference of GLP-1 receptor expression in C cell is also attributable to the inconsistent results between animal studies and clinical trials.
Although TZDs were indicated to lead to osteoporosis by inducing peroxisome proliferator-activated receptor γ in many clinical trials in type 2 diabetes [44–46], no negative effect of pioglitazone on BMD and bone turnover markers was found in this study. It is worthy to address that patients enrolled in the present study were all drug-naïve patients with newly diagnosed type 2 diabetes who may have better bone quality compared to those patients with relatively long diabetic durations in other studies indicating the association between TZDs and bone fracture.
The strengths of our study included the direct head-to-head comparison of monotherapy of antihyperglycemic agent in patients with newly diagnosed type 2 diabetes, maximally avoiding the confounding effects of other antihyperglycemic agents and different diabetic duration. And adopting bone turnover markers in addition to BMD could reveal the differences between treatments with regard to the early change in bone metabolism. Some limitations should also be addressed. First, undercarboxylated osteocalcin (ucOC) has been considered a novel and exciting regulator of glucose metabolism in recent years, although a distinct role for ucOC in skeletal health has not been clearly identified [47]. We did not find a relation between the glucose metabolism and OC in this study. Nevertheless, not measuring ucOC leads to the impossibility to establish the relationships among OC, ucOC, OC-to-ucOC ratio and glycemic index. Second, we did not measure serum levels of 25-hydroxyvitamin D, parathyroid hormone, calcium, magnesium, sex steroids and calcium content in the diet, which are known to influence bone turnover. And the 6-month follow-up duration is not long enough to prove the long-term effects of the interventions on bone health. Thus, well-designed, prospective and long-term randomized control trials are needed to shed light on the action of exenatide, insulin or pioglitazone on bone metabolism.
In conclusion, 24-week monotherapy with exenatide, insulin or pioglitzone improved glycemic control in patients with newly diagnosed type 2 diabetes. In spite of different effects on body weight change, 24-week treatment with exenatide, insulin or pioglitzone has no effects on bone turnover markers and BMD.
References
de Liefde II, van der Klift M, de Laet CE, van Daele PL, Hofman A, Pols HA (2005) Bone mineral density and fracture risk in type-2 diabetes mellitus: the Rotterdam study. Osteoporos Int 16:1713–1720
Vestergaard P (2007) Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes—a meta-analysis. Osteoporos Int 18:427–444
Hamilton EJ, Rakic V, Davis WA, Paul Chubb SA, Kamber N, Prince RL, Davis TME (2012) A five-year prospective study of bone mineral density in men and women with diabetes: the fremantle diabetes study. Acta Diabetol 49:153–158
Saller A, Maggi S, Romanato G, Tonin P, Crepaldi G (2008) Diabetes and osteoporosis. Aging Clin Exp Res 20:280–289
Maggi S, Siviero P, Brocco E, Albertin M, Romanato G, Crepaldi G (2014) Vitamin D deficiency, serum leptin and osteoprotegerin levels in older diabetic patients: an input to new research avenues. Acta Diabetol 51:461–469
Khazai NB, Beck GR Jr, Umpierrez GE (2009) Diabetes and fractures: an overshadowed association. Curr Opin Endocrinol Diabetes Obes 16:435–445
Clowes JA, Allen HC, Prentis DM, Eastell R, Blumsohn A (2003) Octreotide abolishes the acute decrease in bone turnover in response to oral glucose. J Clin Endocrinol Metab 88:4867–4873
Ferron M, Wei J, Yoshizawa T, Del Fattore A, DePinho RA, Teti A, Ducy P, Karsenty G (2010) Insulin signaling in o Guillermo E. Umpierrez, osteoblasts integrates bone remodeling and energy metabolism. Cell 142:296–308
Asmar M, Holst JJ (2010) Glucagon-like peptide 1 and glucose-dependent insulinotropic polypeptide: new advances. Curr Opin Endocrinol Diabetes Obes 17:57–62
Wei W, Wan Y (2011) Thiazolidinediones on PPARgamma: the roles in bone remodeling. PPAR Res 2011:867180
Xu W, Bi Y, Sun Z, Li J, Guo L, Yang T, Wu G, Shi L, Feng Z, Qiu L, Li Q, Guo X, Luo Z, Lu J, Shan Z, Yang W, Ji Q, Yan L, Li H, Yu X, Li S, Zhou Z, Lv X, Liang Z, Lin S, Zeng L, Yan J, Ji L, Weng J (2015) Comparison of the effects on glycaemic control and b-cell function in newly diagnosed type 2 diabetes patients of treatment with exenatide, insulin or pioglitazone: a multicenter randomized parallel-group trial (the confidence study). J Intern Med 277:137–150
Bunck MC, Diamant M, Cornér A, Eliasson B, Malloy JL, Shaginian RM, Deng W, Kendall DM, Taskinen MR, Smith U, Yki-Järvinen H, Heine RJ (2009) One-year treatment with exenatide improves beta-cell function, compared with insulin glargine, in metformin-treated type 2 diabetic patients: a randomized, controlled trial. Diabetes Care 32:762–768
Meloni AR, DeYoung MB, Han J, Best JH, Grimm M (2013) Treatment of patients with type 2 diabetes with exenatide once weekly versus oral glucose-lowering medications or insulin glargine: achievement of glycemic and cardiovascular goals. Cardiovasc Diabetol 12:48
Russell-Jones D, Cuddihy RM, Hanefeld M, Kumar A, González JG, Chan M, Wolka AM, Boardman MK, DURATION-4 Study Group (2012) Efficacy and safety of exenatide once weekly versus metformin, pioglitazone, and sitagliptin used as monotherapy in drug-naive patients with type 2 diabetes (DURATION-4): a 26-week double-blind study. Diabetes Care 35:252–258
Reyes-García R, Rozas-Moreno P, López-Gallardo G, García-Martín A, Varsavsky M, Avilés-Perez MD, Muñoz-Torres M (2013) Serum levels of bone resorption markers are decreased in patients with type 2 diabetes. Acta Diabetol 50:47–52
Gerdhem P, Isaksson A, Akesson K, Obrant KJ (2005) Increased bone density and decreased bone turnover, but no evident alteration of fracture susceptibility in elderly women with diabetes mellitus. Osteoporos Int 16:1506–1512
Rosato MT, Schneider SH, Shapses SA (1998) Bone turnover and insulin-like growth factor I levels increase after improved glycemic control in noninsulin-dependent diabetes mellitus. Calcif Tissue Int 63:107–111
Okazaki R, Totsuka Y, Hamano K, Ajima M, Miura M, Hirota Y, Hata K, Fukumoto S, Matsumoto T (1997) Metabolic improvement of poorly controlled noninsulin-dependent diabetes mellitus decreases bone turnover. J Clin Endocrinol Metab 82:2915–2920
Kanazawa I, Yamaguchi T, Yamauchi M, Yamamoto M, Kurioka S, Yano S, Sugimoto T (2009) Adiponectin is associated with changes in bone markers during glycemic control in type 2 diabetes mellitus. J Clin Endocrinol Metab 94:3031–3037
Kindblom JM, Ohlsson C, Ljunggren O, Karlsson MK, Tivesten A, Smith U, Mellstrom D (2009) Plasma osteocalcin is inversely related to fat mass and plasma glucose in elderly Swedish men. J Bone Miner Res 24:785–791
Im JA, Yu BP, Jeon JY, Kim SH (2008) Relationship between osteocalcin and glucose metabolism in postmenopausal women. Clin Chim Acta 396:66–69
Kanazawa I, Yamaguchi T, Yamamoto M, Yamauchi M, Kurioka S, Yano S, Sugimoto T (2009) Serum osteocalcin level is associated with glucose metabolism and atherosclerosis parameters in type 2 diabetes mellitus. J Clin Endocrinol Metab 94:45–49
Kanazawa I, Yamaguchi T, Yamauchi M, Yamamoto M, Kurioka S, Yano S, Sugimoto T (2010) Serum undercarboxylated osteocalcin was inversely associated with plasma glucose level and fat mass in type 2 diabetes mellitus. Osteoporos Int 22:187–194
Sayinalp S, Gedik O, Koray Z (1995) Increasing serum osteocalcin after glycemic control in diabetic men. Calcif Tissue Int 57:422–425
Gregorio F, Cristallini S, Santeusanio F, Filipponi P, Fumelli P (1994) Osteopenia associated with non-insulin-dependent diabetes mellitus: what are the causes? Diabetes Res Clin Pract 23:43–54
Hong SH, Koo JW, Hwang JK, Hwang YC, Jeong IK, Ahn KJ, Chung HY, Kim DY (2013) Changes in serum osteocalcin are not associated with changes in glucose or insulin for osteoporotic patients treated with bisphosphonate. J Bone Metab 20:37–41
Poomthavorn P, Nantarakchaikul P, Mahachoklertwattana P, Chailurkit LO, Khlairit P (2014) Effects of correction of vitamin D insufficiency on serum osteocalcin and glucose metabolism in obese children. Clin Endocrinol (Oxf) 80:516–523
Finkelstein JS, Sowers M, Greendale GA, Lee ML, Neer RM, Cauley JA, Ettinger B (2003) Ethnic variation in bone turnover in pre- and early perimenopausal women: effects of anthropometric and lifestyle factors. J Clin Endocrinol Metab 87:3051–3056
Nuche-Berenguer B, Portal-Núñez S, Moreno P, González N, Acitores A, López-Herradón A, Esbrit P, Valverde I, Villanueva-Peñacarrillo ML (2010) Presence of a functional receotpr for GLP-1 in osteoblastic cells, independent of the cAMP-linked GLP-1 receptor. J Cell Physiol 225:585–592
Ng KW (2011) Regulation of glucose metabolism and the skeleton. Clin Endocrinol (Oxford) 75:147–155
Nuche-Berenguer B, Moreno P, Esbrit P, Dapía S, Caeiro JR, Cancelas J, Haro-Mora JJ, Villanueva-Peñacarrillo ML (2009) Effect of GLP-1 treatment on bone turnover in normal, type 2 diabetic, and insulin-resistant states. Calcif Tissue Int 84:453–461
Nuche-Berenguer B, Moreno P, Portal-Nuñez S, Dapía S, Esbrit P, Villanueva-Peñacarrillo ML (2010) Exendin-4 exerts osteogenic actions in insulin-resistant and type 2 diabetic states. Regul Pept 159:61–66
Bunck MC, Eliasson B, Cornér A, Heine RJ, Shaginian RM, Taskinen MR, Yki-Järvinen H, Smith U, Diamant M (2011) Exenatide treatment did not affect bone mineral density despite body weight reduction in patients with type 2 diabetes. Diabetes Obes Metab 13:374–377
Bunck MC, Poelma M, Eekhoff EM, Schweizer A, Heine RJ, Nijpels G, Foley JE, Diamant M (2012) Effects of Vildagliptin on postprandial markers of bone resorption and calcium homeostasis in recently diagnosed, well-controlled, type 2 diabetes patients. J Diabetes 4:181–185
Garnero P (2008) Biomarkers for osteoporosis management: utility in diagnosis, fracture risk prediction and therapy monitoring. Mol Diagn Ther 12:157–170
Jensen LB, Kollerup G, Quaade F, Sørensen OH (2001) Bone mineral changes in obese women during a moderate weight loss with and without calcium supplementation. J Bone Miner Res 16:141–147
Riedt CS, Cifuentes M, Stahl T, Chowdhury HA, Schlussel Y, Shapses SA (2005) Overweight postmenopausal women lose bone with moderate weight eduction and 1 g/day calcium intake. J Bone Miner Res 20:455–463
Carrasco F, Ruz M, Rojas P, Csendes A, Rebolledo A, Codoceo J, Inostroza J, Basfi-Fer K, Papapietro K, Rojas J, Pizarro F, Olivares M (2009) Changes in bone mineral density, body composition and adiponectin levels in morbidly obese patients after bariatric surgery. Obes Surg 19:41–46
Holecki M, Zahorska-Markiewicz B, Chudek J, Wiecek A (2010) Changes in bone mineral density and bone turnover markers in obese women after short-term weight loss therapy during a 5-year follow-up. Pol Arch Med Wewn 120:248–254
Yamada C, Yamada Y, Tsukiyama K, Yamada K, Udagawa N, Takahashi N, Tanaka K, Drucker DJ, Seino Y, Inagaki N (2008) The murine glucagonlike peptide-1 receptor is essential for control of bone resorption. Endocrinology 149:574–579
Antonopoulou M, Bahtiyar G, Banerji MA, Sacerdote AS (2013) Diabetes and bone health. Maturitas 76:253–259
Waser B, Beetschen K, Pellegata NS, Reubi JC (2011) Incretin receptors in non-neoplastic and neoplastic thyroid C cells in rodents and humans: relevance for incretin-based diabetes therapy. Neuroendocrinology 94:291–301
Gier B, Butler PC, Lai CK, Kirakossian D, DeNicola MM, Yeh MW (2012) Glucagon like peptide-1 receptor expression in the human thyroid gland. J Clin Endocrinol Metab 97:121–131
Lecka-Czernik B (2010) Bone loss in diabetes: use of antidiabetic thiazolidinediones and secondary osteoporosis. Curr Osteoporos Rep 8:178–184
Dormuth CR, Carney G, Carleton B, Bassett K, Wright JM (2009) Thiazolidinediones and fractures in men and women [J]. Arch Intern Med 169:1395–1402
Meier C, Kraenzlin ME, Bodmer M, Jick SS, Jick H, Meier CR (2008) Use of thiazolidinediones and fracture risk. Arch Intern Med 168:820–825
Motyl KJ, McCabe LR, Schwartz AV (2010) Bone and glucose metabolism: a two-way street. Arch Biochem Bioph 503:2–10
Acknowledgments
The authors would like to thank all the participating patients in the study. This study was supported by the Key Clinical Project from the Ministry of Health of China and investigator-initiated trial research funds from Eli Lilly and Co. and Amylin Pharmaceuticals, Inc. The sponsors had no role in the study design, collection, analysis and interpretation of data, or writing the report.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflict of interest.
Ethical standard
The study protocol has been reviewed by the ethics committee of the Third Affiliated Hospital of Sun Yat-sen University and Drum Tower Hospital Affiliated to Nanjing University Medical School, and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1964 Declaration of Helsinki.
Human and animal rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Informed consent
Informed consent was obtained from all patients for being included in the study.
Additional information
Managed by Antonio Secchi.
Renyuan Li, Wen Xu and Sihui Luo have contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Li, R., Xu, W., Luo, S. et al. Effect of exenatide, insulin and pioglitazone on bone metabolism in patients with newly diagnosed type 2 diabetes. Acta Diabetol 52, 1083–1091 (2015). https://doi.org/10.1007/s00592-015-0792-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-015-0792-2