
Abstract
Hallux rigidus is a painful condition of the great toe characterized by restriction of the metatarsophalangeal range of motion and progressive osteophyte formation. Many etiologies have been postulated including excessive length of the first ray, trauma, abnormally elevated first metatarsal and a positive family history. However, most cases are likely idiopathic. Plain radiographs are used to grade the severity of hallux rigidus. The more comprehensive grading is represented by Coughlin and Shurnas’ system that introduced a four-grade classification. When nonoperative treatment fails to provide relief, surgery should be performed. The goal of surgery is to relieve pain, maintain stability of the first metatarsophalangeal joint and improve function and quality of life. Operative treatments can be divided into joint sparing (e.g., cheilectomy with or without associated osteotomies) versus joint sacrificing (e.g., arthroplasty or arthrodesis). There are a variety of osteotomies available for treatment of hallux rigidus (phalanx and/or metatarsal osteotomies). Newer techniques of interpositional arthroplasty as well as new hemi-arthroplasty designs, including synthetic cartilage implants, offer promising options for preservation of motion. The choice of procedure is based on the condition of the joint, patient’s goals and expectations of the surgical outcome, and patient’s motivation. This article discusses various procedures along with clinical outcomes and complications. The advantages and disadvantages of each procedure are discussed.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
Hallux rigidus (HR), Latin for stiff toe, is characterized by an osteoarthritic degeneration of the first metatarsophalangeal joint (FMTPJ) and metatarsosesamoidal joint. It was first mentioned in 1887 [1]. Since then, a multitude of terms have been used referring the same disease. FMTPJ osteoarthritis hallux rigidus is the most common arthritic condition in the foot. Of all patients aged over 50 years, 2.5% report degenerative arthritis of the FMTPJ, termed “hallux rigidus” [2]. The FMTPJ plays an important functional role during the gait cycle as it carries approximately 119% of an individual’s body weight with each step. Osteophyte formation and degeneration of the cartilage occur dorsally in early stages of the disease and progress to involve the entire FMTPJ. Consequently, individuals with hallux rigidus experience joint pain and decreased range of motion (ROM) in the sagittal plane. This leads to altered gait mechanics and significant reduction in activity and quality of life for patients [3].
Anatomy and pathophysiology
Anatomy of the FMTPJ is complex, and kinematics studies showed significant motion range in normal subjects: a mean dorsoplantar range of motion of 111° with a pure dorsiflexion of 76° [4]. Precise etiology remains under debate with trauma being often cited in the literature [5]. Development of degenerative changes can also be secondary to repetitive stress or inflammatory or metabolic conditions such as gout, rheumatoid arthritis. Biomechanical and structural factors, such as long first metatarsal, metatarsus elevates and metatarsus adductus, can also lead to increased risk of hallux rigidus [6, 7]. However, most cases are likely idiopathic.
Clinical evaluation
Hallux rigidus (HR) is rare in young subjects. HR rather reaches the man after the fifth decade. This double osteoarthritis presents different clinical presentations. The main complaints are pain especially during movement and a limited range of motion of the great toe. The restricted metatarsophalangeal range of motion is a hallmark clinical finding with dorsiflexion affected earlier. Patients may report limitations on wearing certain types of shoes due to dorsal osteophytes on the first metatarsal head and proximal phalanx. Patients also may present with altered gait patterns (lift-off gait phase) or pain of the great toe. Osteophytes can compress on the dorsomedial cutaneous nerve (medial branch of the superficial peroneal nerve) and lead to neurological pain [3].
Radiographic examination
Weight-bearing anteroposterior (AP), lateral and oblique views of the affected foot should be obtained. Multiple different grading systems for hallux rigidus have been introduced differentiating between two and five different grades [8, 9]. In 1986, Regnauld in France classified hallux rigidus in three grades. Today, probably the more comprehensive grading is represented by Coughlin and Shurnas’ system that introduced a four-grade classification. This classification system by Coughlin et al. is considered as a “gold standard” [10].
When conservative management fails, there are a variety of surgical treatment options available. These techniques can be divided into joint sparing or joint sacrificing techniques. The goal of surgery is to relieve pain, improve function and improve quality of life. Choice of surgical options depends on the etiology and grading of the deformity.
Joint-preserving surgical procedures
Cheilectomy
For patients with grade 1 or 2 hallux rigidus, a cheilectomy is a good option. First described in 1959 by DuVries, cheilectomy is a joint-sparing technique that involves resection of 20 to 30% of the dorsal metatarsal head and removing dorsal osteophytes of the metatarsal head and proximal phalanx [11]. It is a relatively simple procedure that preserves FMTPJ motion, allowing for faster return to daily activities (Fig. 1a, b).

Cheilectomie
It is typically performed for patients in the earlier stages of hallux rigidus presenting with dorsal pain and dorsiflexion stiffness in the absence of through-range symptoms, rest pain and plantar pain and with negative result on grind test. Several studies report good results in early-stage HR (grades 1 and 2) and poorer results in more advanced stages [10].
A recent study by Nicolesi suggested that cheilectomy offers long-term satisfaction for patients with hallux rigidus and is an acceptable alternative to the joint destructive procedure of first metatarsophalangeal arthrodesis with a mean follow-up period of 7.14 years (range 39 weeks to 14.87 years) [12]. The mean patient age was 55.71 ± 9.51 years, and 37 (65%) of the patients were female. The mean percentage of success with this operation was 87.69%.
New approaches techniques such as percutaneous and arthroscopic have been described recently with good results [13]. The use of arthroscopy in the treatment of HR is an emerging technique used for grade 1 and 2 HR when joint motion still remains [14]. Cheilectomy can be performed arthroscopically as an alternative to open cheilectomy [15]. Advantages include smaller incisions, less operative morbidity and reduced pain. Nevertheless, arthroscopy of the FMTPJ needs a learning curve with additional surgical training.
Osteotomies
In order to restore an acceptable ROM of the great toe, especially dorsiflexion, several osteotomies have been described. We can distinguish phalangeal osteotomies on the one hand and metatarsal osteotomies on the other hand. Osteotomies of the proximal phalanx and first metatarsal have been described mainly in the podiatric literature; they have shown good outcomes in small patient groups with short-term follow-up. Proper patient selection is critical to obtaining favorable outcomes with any of the joint-sparing procedures [16]. The main goal of these procedures is to obtain a decompression of the joint.
Phalangeal osteotomies
-
Proximal phalange osteotomy (Moberg) A Moberg osteotomy consists of a dorsiflexion osteotomy of the proximal phalanx and was first described by Bonney and Macnab [17]. It is a closing wedge osteotomy and acts to shift the arc of motion of the first MTP joint into more dorsiflexion by sacrificing plantarflexion. First indication is represented by limited dorsiflexion with normal plantar flexion and moderate degeneratives stages (grades 1 and 2).
Moberg’s osteotomy can be associated with cheilectomy (Fig. 2). Waizy [18] published a prospective study of 60 patients with symptomatic HR. In cases with intraoperative dorsiflexion of less than 70 degrees after the cheilectomy, an additional Kessel–Bonney osteotomy was done. In 51.4% of the patients, the Kitaoka score was higher than 70.4 points. The joint-preserving operation in patients with grade 1 and 2 hallux rigidus shows an increase in dorsiflexion and decrease in daily pain. The long-term follow-up shows a persistent pain reduction and satisfaction of the patients.

Moberg osteotomy and cheilectomy
Regnauld in 1986 [19] described an enclavement procedure, a “peg-in-hole” technique. It consisted of removing the base of the proximal phalanx and resecting a cylinder of bone. The remaining exposed end of the proximal phalanx was then reduced so that the base with the removed cylinder would fit snugly on the proximal phalanx, and the two were then pieced together. Regnauld initially described 3 graft shapes: hat, cork and inverted (Fig. 3).
Fig. 3 
Regnauld osteotomies

Metatarsal osteotomies
-
Dorsal closing wedge osteotomy Watermann was the first to report in 1927 a dorsal closing wedge trapezoidal osteotomy of the distal first metatarsal bone [20] (Fig. 4). It was designed to relocate the viable plantar cartilage to a more dorsal location, allowing more dorsiflexion of the hallux. It further causes a joint decompression. Few studies evaluated this technique. The major disadvantage is that the osteotomy is relatively unstable due to the perpendicular orientation of the osteotomy and the resulting difficult fixation. It is contraindicated in metatarsus primus elevatus as it may exacerbate the disorder.
Fig. 4 
Watermann osteotomy
-
Watermann Green The Watermann Green involves a 2-arm osteotomy in the metatarsal head (Fig. 5) with the dorsal arm being parallel to the long axis of the bone and the plantar arm being parallel to the weight-bearing surface. A dorsal cheilectomy is frequently performed during the procedure. The name Waterman Green is misleading as the procedure originally was not designed to rotate the articular cartilage compared to the original Watermann procedure. It is difficult to delineate this technique from the Youngswick osteotomy.
Fig. 5 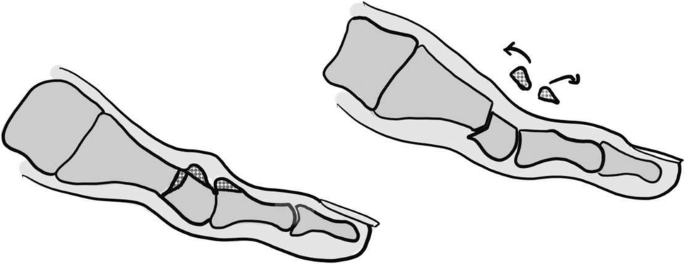
Watermann Green osteotomy
-
Youngswick This procedure was described by Youngswick in 1982 as a modification of the Chevron osteotomy [21]. The Youngswick has become one of the most popular distal metatarsal osteotomies used in hallux rigidus. First a V-shaped osteotomy is performed with the apex directed distally, and two diagonal arms are directed dorsal proximal and plantar proximal at a 60° angle. A second osteotomy is performed parallel to the dorsal limb of the first osteotomy (Fig. 6). This results in a shortening of the first metatarsal leading to a decompression of the joint. Fixation is similar to the Austin bunionectomy and offers the advantage of being stable in all three cardinal planes when one point of fixation is used.
Fig. 6 
Youngswick



Its main indications include metatarsus primus elevatus and/or long first metatarsal bone, in order to relax the joint space reducing pain and increasing mobility.
Reverdin Green The Reverdin Green osteotomy is a modification of the Youngswick procedure. After performing the V-shaped osteotomy, a second osteotomy is performed parallel to the dorsal limb of the V-shaped osteotomy and the excised bone block is implanted in the plantar limb of the osteotomy to further translate the metatarsal head plantarwards (Fig. 7). Kilmartin [22] performed 30 procedures in a prospective study aiming to compare 3 different types of metatarsal osteotomies, but due to complications they instead continued with a plantar proximal displacement osteotomy. Authors did not report clear clinical results, but Reverdin procedure was stopped due to high rate of complications.
Fig. 7 
Reverdin Green osteotomy
Distal oblique sliding osteotomy (Weil/Mau osteotomy) It is characterized by a single, dorsal distal to plantar proximal oriented osteotomy line, beginning just proximal to the articular surface. Osteotomy angle is about 35°–45° (Fig. 8). Lundeen [23] initially described this procedure for treatment of hallux limitus, but it has been adopted for treatment of hallux rigidus only. Ronconi et al. [24] studied 26 patients on whom both the Weil and an aggressive cheilectomy were performed with 84% having good-to-excellent results. Malerba et al. [25] retrospectively analyzed 20 patients treated with a distal oblique sliding osteotomy with an average follow-up of 11 years. The average AOFAS score increased from 44 (range 14–68) to 82 (range 80–100). Good-to-excellent results were achieved in 19 patients. The mean passive dorsiflexion of the FMTPJ improved from 8° (range 5°–10°) to 44° (range 15°–55°). No patient underwent subsequent surgery. The authors did not comment on metatarsalgia of the lesser toes.
Fig. 8 
Distal oblique sliding osteotomy
Sagittal Z osteotomy This osteotomy is performed creating 2 parallel arms perpendicular to the long axis of the metatarsal bone. Distal arm exits laterally and proximal arm exits medially, linked by a central arm running the long axis perpendicular to the weight-bearing line (Fig. 9). The sagittal Z osteotomy aims at shortening and thereby decompressing the FMTPJ. It allows plantar flexion of the MTPJ. The advantage is represented by high cross-sectional area for bone healing, stability and low risk of bone necrosis. The evidence of this procedure is slow. Viegas [26] evaluated 11 patients treated with this osteotomy. There were eight excellent results (73%) and three good results (27%). There were no fair or poor results. The authors did not acquire objective measurements and consequently could not perform statistical analysis.
Fig. 9 
Sagittal Z osteotomy
Drago osteotomy Drago et al. [27] described a double osteotomy consisting of a Watermann procedure and a proximal plantar flexing osteotomy (Fig. 10). The idea was to perform a major grade of plantar flexioning correction compared to distal osteotomy alone. No study has yet evaluated the results of this technique.
Fig. 10 
Drago osteotomy




In summary, there are numerous osteotomies available for treatment of hallux rigidus. The advantages and disadvantages of each procedure need to be weighed with the expectations of both the surgeon and the patient.
Joint sacrificing techniques
Valenti procedure
In 1987, Valente Valenti presented a personal communication regarding a surgical alternative treatment for hallux rigidus. Valenti described a 80° sagittal plane “V” resection of the FMTPJ with preservation of the first ray length, the plantar portion of the first metatarsal head and first proximal phalangeal base, conserving also the flexor hallucis brevis and the sesamoid function [28]. Few studies reporting this procedure have been published in the literature. Recently, Colo [29] retrospectively evaluated 38 patients (40 feet) who underwent a Valenti procedure with a mean follow-up of 132 months. The authors found a significant improvement of the mean values of the visual analog scale (VAS) (p < 0.0001) and AOFAS Hallux Metatarsophalangeal Interphalangeal Scale Assessment (p < 0.0001) at the latest follow-up visit. Complications of the Valenti procedure were a progressive worsening of joint stiffness, but no sesamoiditis, metatarsalgia overload were documented.
Resection arthroplasty
The Keller resection arthroplasty consists of removal of the base of the proximal phalanx to decompress the joint and increase dorsiflexion while sacrificing joint stability. While some reports have demonstrated effective pain relief, complications include weakness with toe-off, transfer metatarsalgia and cock-up deformity of the great toe. This profile makes this procedure a less desirable option for most patients [30].
Arthrodesis
Arthrodesis of the FMTPJ is the current “gold standard” of treatment for advanced arthritis of the great toe and has demonstrated consistently good results in the literature. Arthrodesis yielded better reduction of pain, better functional satisfaction, shorter hospital stays, lower revision rates and faster return to normal activity [31].
There are multiple techniques (Fig. 11) to achieve fusion (plates, screws, wires and staples). Politi et al. [32] compared the strength of fixation of different commonly used procedures to achieve FMTPJ fusion and found that the most stable technique was the combination of an oblique lag screw and a dorsal plate. This procedure is typically performed as open surgery although few recent studies have demonstrated a percutaneous approach [33, 34].

Hallux arthrodesis: plating or screwing
Arthrodesis is performed under regional or general anesthesia with or without tourniquet. The surgery can be performed through a dorsal or medial approach. Several techniques have been described to remove the cartilage, including use of burrs, flats cuts or conical reamers. Flat cuts are more demanding and have an increased risk of shortening the first ray. Dome-cup pair configuration allows for high degrees of adjustability in a 3-dimensional plane, making final alignment of the hallux easier. Optimal position of the FMTPJ is 5°–15° of valgus and 10°–20° of dorsiflexion with neutral rotation [2].
Post-surgery protocol includes either nonweight bearing or weight bearing in a postoperative shoe to avoid high pressure under the metatarsophalangeal joint.
Recent studies have reported high fusion rates (between 77 and 100%) with dorsal plating and screw fixation [35]. Numerous comparative studies have reported good results of arthrodesis compared with arthroplasty. In all series, the results of arthrodesis were either equivalent or superior with fewer complications [36,37,38]. Complications include infection, osteonecrosis, implant protrusion or failure, nonunion and malunion, the latter 2 each occurring in approximately 6% of cases [39].
The rate of satisfaction with arthrodesis has been reported to be over 80% [40]. Arthrodesis has been shown to improve propulsion power and stability during gait. Given the good results reported in level II to IV studies, there is good evidence (grade B) to support arthrodesis in symptomatic advanced hallux rigidus.
Arthroplasty
As first metatarsophalangeal joint arthrodesis is generally considered to be a successful procedure for the treatment of hallux rigidus, many surgeons question the usefulness of FMTPJ arthroplasty. Unlike arthrodesis in which the joint motion is sacrificed, arthroplasty is a procedure intended to relief pain while preserving the mobility of the FMTPJ.
FMTPJ arthroplasty began historically in the 1950s with silastic implants similar to those used in the hand and progressed to all-metal implants and, more recently, to synthetic cartilage implants [41]. Silastic implants have been found to be associated with high rates of osteolysis with implant subsidence and immune reactions [42].
Unlike arthrodesis in which joint motion is sacrificed to improve pain, arthroplasty is a surgical option intended to relief pain while preserving the mobility of the FMTPJ. Both total joint arthroplasty and hemiarthroplasty of the phalanx or metatarsal have been described.
Total joint replacement of the hallux metatarsophalangeal joint has not enjoyed the same success as hip and knee arthroplasties. The first generation of implants used a constrained polyethylene phalangeal component with a metal metatarsal component. Results from this implant experienced high rates of failure due to loosening [43]. The third generation of implants used either metal or ceramic components that were press fit with or without cement to anchor into the bone [42]. But multiple complications were reported in the literature including implant failure and aseptic loosening. The reports of high complication rates and poor survival have led surgeons to become cautious with this procedure. Fourth-generation implants now use either threaded stems with a Morse taper or press-fit design to secure the bearing surface. Actually, most of the designs use titanium stems that are porous coated for press-fit or cemented implantation with a Co–Cr articulating surface on ultra-high-weight molecular polyethylene. Mixed results have been reported on the long-term outcomes of various types of implants [44].
Similar to total joint arthroplasty, hemiarthroplasty also helps maintain the motion of the FMTPJ but requires less bone resection in comparison with total arthroplasty. As a result, conversion to arthrodesis would be easier if a revision becomes necessary. Like total arthroplasty, studies on hemiarthroplasty have shown mixed results [45, 46]. In a recent study, Stibolt et al. [47] showed that the mean postoperative AOFAS scores in patients undergoing hemiarthroplasty improved by 50.7 points, whereas the mean AOFAS score improvement in total joint arthroplasty patients was 40.6 points. Mean postoperative FMTPJ range of motion improved by 43.0° in hemiarthroplasty patients, which exceeded the mean range of motion improvement of 32.5° found in total joint arthroplasty. They concluded that hemisurface implants in MTPJ arthroplasty may improve postoperative AOFAS and ROM results to a greater extent than total-toe devices.
Interpositional arthroplasty
Range of motion sparing techniques such as interpositional arthroplasty (IA) can preserved joint function and can be therefore preferred in some patients.
IA consists of combining a limited Keller resection with placement of a biological spacer into the joint. The spacer is made of allograft, autograft, or synthetic biological material. IA procedure described in the literature interposes the dorsal capsule, tendons of extensor digitorium, extensor hallucis brevis, plantaris, gracilis or facia lata. For some authors, regenerative collagen matrix can be used [48].
Retrospective studies using IA demonstrate moderate results and complications included metatarsalgia (13.6–57%), loss of ground contact, weakness of great toe, diminished push off power, etc. [49, 50]. In a recent meta-analysis, Patel et al. [48] compared outcomes between allograft versus autograft. In summary, there was no significant difference in the preoperative AOFAS scores, but the postoperatives scores in the autograft group were significantly higher than in the allograft group (p = 0.003). There were significant improvements from the preoperative to postoperative scores in both groups. Patients desiring MTP joint movement may opt for interposition arthroplasty to avoid the movement restrictions of arthrodesis. IA gives acceptable clinical outcomes in patients with moderate to severe HR who prefer to maintain ROM and accept the risk of complications.
Synthetic cartilage and chondral engineering
Baumhauer et al. [41] described the use of a synthetic cartilage implant as an allograft interpositional spacer. This synthetic cartilage implant of 8 or 10 mm in diameter requires minimal bone resection. The authors prospectively evaluated in a multicenter study 152 HR treated with this hydrogel implant compared with an arthrodesis group. At 2-year follow-up, both groups had similar functional improvement, SF 36 score and VAS score. Cassinelli [51] described the use of a synthetic cartilage implant (SCI, Cartiva) for treatment of HR with neutral patient satisfaction, mild pain and physical dysfonction at early follow-up.
Glazebrook [52] demonstrated in a prospective, randomized noninferiority clinical trial of synthetic cartilage implant hemiarthroplasty, functional outcomes and safety equivalent to FMTPJ arthrodesis at 24 months. Patient-reported outcomes at 24 months were maintained at 5.8 years in patients who were not revised. 93.4% of patients would have the procedure again according to the authors.
Clinical studies about chondral engineering for HR are emerging. Future publications are promising, and it is necessary to wait for other high-level evidence series.
Conclusion
Operative options range from joint-preserving procedures to joint-altering procedures. The choice of procedure is based on the condition of the joint, patient’s goals and expectations of the surgical outcome. Early- to mid-stage hallux rigidus is best managed with isolated cheilectomy or cheilectomy associated with proximal phalanx or metatarsal osteotomies. For patients with severe hallux rigidus, the “gold standard” remains first MTP arthrodesis, where retrospective series as well as comparative studies have shown consistent success. Arthroplasty is an alternative to arthrodesis if we want to preserve joint mobility. Nevertheless, we must accept the significant complications in the short or medium term. For less active patients, a resection arthroplasty is also possible. Newer techniques of interpositional arthroplasty as well as new hemi-arthroplasty designs, including synthetic cartilage implants, offer promising options for preservation of motion. The evidence currently available investigating the different procedures is poor. Especially, the clinical heterogeneity and the low number of prospective trials are the reason why it is not possible to compare outcomes for patients undergoing the different surgical procedures. Long-term follow-up studies are needed to validate the available results.
References
Davies-Colley M (1887) Contraction of the metatarsophalangeal joint of the great toe. BMJ 1:728
Ho B, Baumhauer J (2017) Hallux rigidus. EFORT Open Rev 2:13–20. https://doi.org/10.1302/2058-5241.2.160031
Lam A, Chan JJ, Surace MF, Vulcano E (2017) Hallux rigidus: How do I approach it? World J Orthop 8:364–371. https://doi.org/10.5312/wjo.v8.i5.364
Shereff MJ, Bejjani FJ, Kummer FJ (1986) Kinematics of the first metatarsophalangeal joint. J Bone Jt Surg Am 68:392–398
Botek G, Anderson MA (2011) Etiology, pathophysiology, and staging of hallux rigidus. Clin Podiatr Med Surg 28(229–243):vii. https://doi.org/10.1016/j.cpm.2011.02.004
Migues A, Slullitel G (2012) Joint-preserving procedure for moderate hallux rigidus. Foot Ankle Clin 17:459–471. https://doi.org/10.1016/j.fcl.2012.06.006
Hamid KS, Parekh SG (2015) Clinical presentation and management of hallux rigidus. Foot Ankle Clin 20:391–399. https://doi.org/10.1016/j.fcl.2015.04.002
Karasick D, Wapner KL (1991) Hallux rigidus deformity: radiologic assessment. AJR Am J Roentgenol 157:1029–1033. https://doi.org/10.2214/ajr.157.5.1927789
Karasick D, Wapner KL (1990) Hallux valgus deformity: preoperative radiologic assessment. AJR Am J Roentgenol 155:119–123. https://doi.org/10.2214/ajr.155.1.2112832
Coughlin MJ, Shurnas PS (2003) Hallux rigidus. Grading and long-term results of operative treatment. J Bone Jt Surg Am 85:2072–2088
Duvries HL (1959) Surgery of the foot. Acad Med 34:1055
Nicolosi N, Hehemann C, Connors J, Boike A (2015) Long-term follow-up of the cheilectomy for degenerative joint disease of the first metatarsophalangeal joint. J Foot Ankle Surg 54:1010–1020. https://doi.org/10.1053/j.jfas.2014.12.035
Bauer T (2014) Percutaneous forefoot surgery. Orthop Traumatol Surg Res 100:S191–S204. https://doi.org/10.1016/j.otsr.2013.06.017
Hunt KJ (2015) Hallux metatarsophalangeal (MTP) joint arthroscopy for hallux rigidus. Foot Ankle Int 36:113–119. https://doi.org/10.1177/1071100714559728
Walter R, Perera A (2015) Open, arthroscopic, and percutaneous cheilectomy for hallux rigidus. Foot Ankle Clin 20:421–431. https://doi.org/10.1016/j.fcl.2015.04.005
Seibert NR, Kadakia AR (2009) Surgical management of hallux rigidus: cheilectomy and osteotomy (phalanx and metatarsal). Foot Ankle Clin 14:9–22. https://doi.org/10.1016/j.fcl.2008.11.002
Bonney G, Macnab I (1952) Hallux valgus and hallux rigidus: a critical survey of operative results. J Bone Jt Surg Br 34:366–385
Waizy H, Czardybon MA, Stukenborg-Colsman C et al (2010) Mid- and long-term results of the joint preserving therapy of hallux rigidus. Arch Orthop Trauma Surg 130:165–170. https://doi.org/10.1007/s00402-009-0857-1
Freeman BL, Hardy MA (2011) Multiplanar phalangeal and metatarsal osteotomies for hallux rigidus. Clin Podiatr Med Surg 28:329–344. https://doi.org/10.1016/j.cpm.2011.03.002
Watermann H (1927) Die Arthritis deformans des grozehen-grungelenkes als selbstndiges krankheitsbild. Z Orthop Chir 48:346–355
Youngswick FD (1982) Modifications of the Austin bunionectomy for treatment of metatarsus primus elevatus associated with hallux limitus. J Foot Surg 21:114–116
Kilmartin TE (2005) Phalangeal osteotomy versus first metatarsal decompression osteotomy for the surgical treatment of hallux rigidus: a prospective study of age-matched and condition-matched patients. J Foot Ankle Surg 44:2–12. https://doi.org/10.1053/j.jfas.2004.11.013
Lundeen RO, Rose JM (2000) Sliding oblique osteotomy for the treatment of hallux abducto valgus associated with functional hallux limitus. J Foot Ankle Surg 39:161–167
Ronconi P, Monachino P, Baleanu PM, Favilli G (2000) Distal oblique osteotomy of the first metatarsal for the correction of hallux limitus and rigidus deformity. J Foot Ankle Surg 39:154–160
Malerba F, Milani R, Sartorelli E, Haddo O (2008) Distal oblique first metatarsal osteotomy in grade 3 hallux rigidus: a long-term followup. Foot Ankle Int 29:677–682. https://doi.org/10.3113/FAI.2008.0677
Viegas GV (1998) Reconstruction of hallux limitus deformity using a first metatarsal sagittal-Z osteotomy. J Foot Ankle Surg 37:204–211 (discussion 261-262)
Drago JJ, Oloff L, Jacobs AM (1984) A comprehensive review of hallux limitus. J Foot Surg 23:213–220
Harisboure A, Joveniaux P, Madi K, Dehoux E (2009) The Valenti technique in the treatment of hallux rigidus. Orthop Traumatol Surg Res 95:202–209. https://doi.org/10.1016/j.otsr.2009.02.004
Colò G, Alessio-Mazzola M, Dagnino G, Felli L (2019) Long-term results of surgical treatment of valenti procedures for hallux rigidus: a minimum ten-year follow-up retrospective study. J Foot Ankle Surg 58:291–294. https://doi.org/10.1053/j.jfas.2018.08.055
Coutts A, Kilmartin TE, Ellis MJH (2012) The long-term patient focused outcomes of the Keller’s arthroplasty for the treatment of hallux rigidus. Foot (Edinb) 22:167–171. https://doi.org/10.1016/j.foot.2012.02.008
McNeil DS, Baumhauer JF, Glazebrook MA (2013) Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int 34:15–32. https://doi.org/10.1177/1071100712460220
Politi J, John H, Njus G et al (2003) First metatarsal-phalangeal joint arthrodesis: a biomechanical assessment of stability. Foot Ankle Int 24:332–337. https://doi.org/10.1177/107110070302400405
Fanous RN, Ridgers S, Sott AH (2014) Minimally invasive arthrodesis of the first metatarsophalangeal joint for hallux rigidus. Foot Ankle Surg 20:170–173. https://doi.org/10.1016/j.fas.2014.03.004
Bauer T (2017) Percutaneous first metatarsophalangeal joint fusion. Open Orthop J 11:724–731. https://doi.org/10.2174/1874325001711010724
Chraim M, Bock P, Alrabai HM, Trnka H-J (2016) Long-term outcome of first metatarsophalangeal joint fusion in the treatment of severe hallux rigidus. Int Orthop 40:2401–2408. https://doi.org/10.1007/s00264-016-3277-1
Gibson JNA, Thomson CE (2005) Arthrodesis or total replacement arthroplasty for hallux rigidus: a randomized controlled trial. Foot Ankle Int 26:680–690. https://doi.org/10.1177/107110070502600904
Raikin SM, Ahmad J, Pour AE, Abidi N (2007) Comparison of arthrodesis and metallic hemiarthroplasty of the hallux metatarsophalangeal joint. J Bone Jt Surg Am 89:1979–1985. https://doi.org/10.2106/JBJS.F.01385
Stone OD, Ray R, Thomson CE, Gibson JNA (2017) Long-term follow-up of arthrodesis vs. total joint arthroplasty for hallux rigidus. Foot Ankle Int 38:375–380. https://doi.org/10.1177/1071100716682994
Rammelt S, Panzner I, Mittlmeier T (2015) Metatarsophalangeal joint fusion: Why and how? Foot Ankle Clin 20:465–477. https://doi.org/10.1016/j.fcl.2015.04.008
Ellington JK, Jones CP, Cohen BE et al (2010) Review of 107 hallux MTP joint arthrodesis using dome-shaped reamers and a stainless-steel dorsal plate. Foot Ankle Int 31:385–390. https://doi.org/10.3113/FAI.2010.0385
Baumhauer JF, Singh D, Glazebrook M et al (2016) Prospective, randomized, multi-centered clinical trial assessing safety and efficacy of a synthetic cartilage implant versus first metatarsophalangeal arthrodesis in advanced hallux rigidus. Foot Ankle Int 37:457–469. https://doi.org/10.1177/1071100716635560
Johnson MD, Brage ME (2016) Total toe replacement in the United States: what is known and what is on the horizon. Foot Ankle Clin 21:249–266. https://doi.org/10.1016/j.fcl.2016.01.004
Weil LS, Pollak RA, Goller WL (1984) Total first joint replacement in hallux valgus and hallux rigidus. Long-term results in 484 cases. Clin Podiatry 1:103–129
Horisberger M, Haeni D, Henninger HB et al (2016) Total arthroplasty of the metatarsophalangeal joint of the hallux. Foot Ankle Int 37:755–765. https://doi.org/10.1177/1071100716637901
Gheorghiu D, Coles C, Ballester J (2015) Hemiarthroplasty for hallux rigidus: mid-term results. J Foot Ankle Surg 54:591–593. https://doi.org/10.1053/j.jfas.2014.11.001
Voskuijl T, Onstenk R (2015) Operative treatment for osteoarthritis of the first metatarsophalangeal joint: arthrodesis versus hemiarthroplasty. J Foot Ankle Surg 54:1085–1088. https://doi.org/10.1053/j.jfas.2015.06.019
Stibolt RD, Patel HA, Lehtonen EJ et al (2019) Hemiarthroplasty versus total joint arthroplasty for hallux rigidus: a systematic review and meta-analysis. Foot Ankle Spec 12:181–193. https://doi.org/10.1177/1938640018791017
Patel HA, Kalra R, Johnson JL et al (2018) Is interposition arthroplasty a viable option for treatment of moderate to severe hallux rigidus? A systematic review and meta-analysis. Foot Ankle Surg. https://doi.org/10.1016/j.fas.2018.07.006
Lau JT, Daniels TR (2001) Outcomes following cheilectomy and interpositional arthroplasty in hallux rigidus. Foot Ankle Int 22:462–470
Coughlin MJ, Shurnas PJ (2003) Soft-tissue arthroplasty for hallux rigidus. Foot Ankle Int 24:661–672. https://doi.org/10.1177/107110070302400902
Cassinelli SJ, Chen S, Charlton TP, Thordarson DB (2019) Early outcomes and complications of synthetic cartilage implant for treatment of hallux rigidus in the United States. Foot Ankle Int. https://doi.org/10.1177/1071100719855049
Glazebrook M, Blundell CM, O’Dowd D et al (2019) Midterm outcomes of a synthetic cartilage implant for the first metatarsophalangeal joint in advanced hallux rigidus. Foot Ankle Int 40:374–383. https://doi.org/10.1177/1071100718815469
Acknowledgements
The authors thank Dr. P. Pasquier M.D. for preparation of the figures.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest with this manuscript.
Ethical standards
This study complies with the current laws of the country in which it was conducted.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Galois, L., Hemmer, J., Ray, V. et al. Surgical options for hallux rigidus: state of the art and review of the literature. Eur J Orthop Surg Traumatol 30, 57–65 (2020). https://doi.org/10.1007/s00590-019-02528-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-019-02528-x