
Abstract
Hallux rigidus is a condition characterized by pain and restriction in motion of the first metatarsophalangeal joint (MTPJ), especially in dorsiflexion. Although various causes have been proposed for hallux rigidus, its exact etiology has yet to be elucidated. Both dynamic and structural factors of the MTPJ itself and the surrounding tissues have been involved, in spite of trauma or osteochondritis dissecans that themselves may damage the articular surfaces of the MTPJ.
Physical examination reveals a painful swollen MTP joint with restriction of dorsiflexion. The patient usually reports a history of pain and stiffness that worsens with activities involving an MTPJ dorsiflexion, such as stairs or running.
Conservative care is the first indication for patients with hallux rigidus, depending on the extent of arthritis and symptoms. The measures commonly used include foot orthoses, modification in shoe-wear, limitations in activity, physical therapy, and injections with corticosteroid or sodium hyaluronate.
Surgical correction of hallux rigidus is indicated when conservative treatment fails to relieve pain. At the most basic level, the surgical options involve either preservation or destruction of the articular surfaces. At moderate stages, joint-preserving procedures constitute a more rational approach. Newer techniques in constant development have focused on procedures that maintain range of motion and allow patients to weight-bear immediately following surgery.
Arthroplasty has been proposed as an alternative surgical option. The main advantage of arthroplasty over arthrodesis is the preservation of movement without the risk of malunion or nonunion. Still, first MTPJ fusion represents today the mainstay of surgical care for high-grade, advanced hallux rigidus. Improvement of pain is achieved by eliminating residual degenerated cartilage layers.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Hallux rigidus
- Degenerative arthritis
- First metatarsophalangeal joint arthrodesis
- First metatarsophalangeal joint arthroplasty
1 Introduction
Hallux rigidus is a condition characterized by pain and restriction in motion of the first metatarsophalangeal joint (MTPJ), especially in dorsiflexion. Symptoms commonly associated with degenerative arthritis of the first MTPJ were initially reported by Davies-Colley in 1887, although Cotterill is credited with proposing the term hallux rigidus. According to the etiology, hallux rigidus can be classified as primary or secondary [1].
2 Etiology
Although various causes have been proposed for hallux rigidus, its exact etiology has yet to be elucidated [1]. Trauma or osteochondritis dissecans may damage the articular surfaces of the MTPJ. Several biomechanical and structural factors may play a role in the development of hallux rigidus.
2.1 Functional Hallux Limitus or the Role of the Dynamic Factor
Functional hallux limitus is a clinical condition in which the first MTPJ motion is impaired on weight-bearing conditions but not when unloaded. That means that the joint moves in an open kinetic chain, but not in a closed chain [2]. Its etiology serves as an explanation of the influence of the soft tissue structures in the genesis of the first metatarsophalangeal degenerative arthritis.
The range of motion in a weight-bearing condition depends on structures that are not within the joint itself. Among these structures, the so-called Achilles-calcaneal-plantar system and the medial column of the foot are mainly responsible for optimally setting the first MTPJ in order to provide anteromedial support of the foot during the third rocker or propulsive phase of gait; this requires adequate passive dorsiflexion of the joint while the hallux is purchasing the ground and the verticalized first metatarsal is axially loading the hallux-sesamoid complex [2]. Failure to achieve first metatarsal plantar flexion or an increase in tensile stress at the plantar fascia will limit passive first MTPJ dorsiflexion in the transition from the second rocker (plantigrade support) to the third one (forefoot support). These can impede the ideal gliding contact pattern at the first MTPJ, producing rolling contact on the dorsal margin of the joint [2].
During the second rocker, the tibia must glide forward on the ankle to allow the body’s center of mass to progress from an initial position posterior to the supporting foot to a final position anterior to it. A restriction to ankle passive dorsiflexion during the second rocker (derived from a contractured gastrocnemius) will increase dorsiflexing moments at the forefoot, thus increasing tensile stress at the plantar soft tissues due to the truss and beam mechanism of the plantar vault support [2].
A cadaveric study conducted by Viehofer et al. [3] demonstrated that increased tension of the plantar fascia results in a decrease of first MTPJ dorsiflexion, and this also provides a plausible explanation for the development of functional hallux limitus.
2.2 The Structural Factor
The anatomy of the first metatarsal is unique, and its shape has been proposed to play a significant role in the development of hallux rigidus [4]. The first metatarsal head is a large transversely flattened quadrilateral structure with dorsoplantar diameter smaller than transverse [5]. The normal MTPJ has a range of motion of 110 degrees, with a plantar flexion of 35 degrees and dorsiflexion of 75 degrees. The consistency and three-dimensional geometry of the articular surfaces confer stability to the center of rotation of the joint [6].
In a normal foot, the centers of rotation are constant in motion and are on the metatarsal head, but in hallux rigidus they are located eccentrically to the metatarsal head [7]. The proximal phalanx moves gradually into a plantar position relative to the metatarsal head, resulting in progressive displacement of the center of rotation [7]. This displacement causes dorsal impingement of the joint during dorsiflexion. Cartilage lesions occur on the dorsal aspect of the first metatarsal head because of repeated compression under high stresses. This compression eventually leads to the development of dorsal osteophytes and joint degeneration [6].
Although in most patients with hallux rigidus it may be possible to objectively detect an elevation of the first metatarsal with respect to the second metatarsal in a lateral weight-bearing radiograph, in others this is not possible. In some cases, there is evidence of instability of the first metatarsocuneiform joint on the sagittal plane during clinical examination, but this may not be evident radiographically [2].
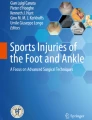
The role of metatarsus primus elevatus (MPE) in the pathogenesis of hallux rigidus has been debated since its first description by Lambrinudi in 1938, although a recent study hypothesized that with a higher grade of hallux rigidus, the plantar fascia windlass mechanism no longer works. The hallux plantar plate contracts, thus limiting hallux dorsiflexion and forcing the first metatarsal into MPE as a secondary phenomenon [8]. It has been widely debated whether the elevation of the head of the first metatarsal (Fig. 1) is the primary mechanical anomaly or whether the increase in tension in the plantar aponeurosis is the culprit [2, 9]. In the presence of either alteration, the other may end up occurring: an elevation of the head of first metatarsal will increase the tension in the plantar aponeurosis by reducing the vault’s anticollapse moment arm, while an abnormal increase in the tension of the fascia will impede the gliding motion in the first MP joint, increasing the dorsal compressive forces in the joint [2]. It changes the first MP joint motion from a gliding to a hinging type.

Picture and radiograph depicting the elevated first metatarsal in advanced hallux rigidus patient
Flat foot as a cause of hallux rigidus has been implicated in several studies, but no demographic data were reported in any of these studies to substantiate the notion. This concept may arise from a 1948 study that reported on 3619 normal military recruits and noted that 15% of the patients had an asymptomatic depression of the longitudinal arch [10]. In a case series evaluated by Coughlin et al., 11% of 140 patients had pes planus and/or excess heel valgus.
The exact role of a long first metatarsal as an associated factor in this particular entity is still controversial. Coughlin and Shurnas [10] found that a long first metatarsal was no more common in patients with hallux rigidus than in the general population. The author’s perspective has been that those flat or chevron-shaped first MTPJs will be exposed to an axial overload during gait that might be the trigger factor of the degenerative process. We believe this is far more significant than the metatarsal length [11].
An increased hallux valgus interphalangeus angle has been evaluated as an associated radiographic and clinical finding of hallux rigidus [12]. This association was seen 90% of the time in the series by Coughlin and Shurnas [5, 10].
Development of degenerative changes can also be secondary to repetitive stress or inflammatory or metabolic conditions such as gout, rheumatoid arthritis [13]. Coughlin and Shurnas [10] found in their study on etiology that adolescent patients with unilateral disease are likely to have reported acute trauma. They also found in the same study that if trauma was reported, the disease was unilateral in 78% of patients regardless of age [5]. A hyperextension injury to the plantar plate and sesamoid complex (so-called turf toe) and a hyperplantar flexion injury may create compression or shear forces that then lead to chondral or osteochondral injury, capsular damage, synovitis, and adhesions and thus have been linked to the development of hallux rigidus [6].
3 Anatomy and Radiological Findings
In 1988 Hattrup and Johnson published the most common classification system used in orthopedic literature. It is based on radiographic changes of the first MTPJ on standing anteroposterior and lateral radiographic examination of the foot. Grade 1 changes consist of mild to moderate osteophyte formation with preservation of joint space. Grade 2 changes exist if there is less than 50% narrowing of joint space, subchondral sclerosis, and moderate osteophyte formation. Grade 3 changes result when there is marked osteophyte formation and more than 50% loss of visible joint space, with or without subchondral cyst formation [1]. Lately Coughlin and Shurnas have introduced a new classification method, adding a grade 4 stage, using clinical information to classify the pathology. This classification includes the assessment of pain patterns. According to this, late stages are characterized for pain in the midrange of motion of the 1 MTPJ [10] (Table 1).
Beeson et al. [14] conducted a systematic review to critically evaluate the various classification systems for hallux rigidus. The authors criticized hallux rigidus grading systems because none had undergone independent testing to assess reliability and validity. Despite this, the Coughlin and Shurnas grading scale for hallux rigidus is the most commonly used and cited. It has been suggested to be prognostic of the severity of great toe arthritis and used to guide treatment [15,16,17].
Baumhauer et al. studied the relationship among the clinical factors making up this most commonly used hallux rigidus grading scale, in patients with hallux rigidus, and to explore the correlation of these factors to grade selection [15]. They failed to find a positive correlation between active dorsiflexion ROM and VAS pain scales at baseline with the Coughlin grade. More important, the Coughlin grade was only weakly correlated with the presence of remaining cartilage as observed within the joint and did not predict the success or failure of clinical treatment.
4 Diagnosis
4.1 Clinical Findings
Physical examination reveals a painful swollen MTP joint (Fig. 2) with restriction of dorsiflexion. The patient usually reports a history of pain and stiffness that worsens with activities involving an MTP dorsiflexion, such as stairs or running. Pain during walking occurs above all in lift-off phase of the gait [18]. Moreover, the patient can report numbness on the medial border of the great toe for the impingement of the medial branch of the superficial peroneal nerve from the dorsal osteophytes [17].

Clinical picture demonstrating the swollen MTPJ
At this point it is particularly important to determine if pain occurs at the midrange of motion or in maximum dorsiflexion. Pain at midrange of passive motion refers to pain that is elicited not only at the extremes of passive dorsiflexion and plantar flexion of the metatarsophalangeal joint but also in between [10].
This aspect must be considered to determine the appropriate surgical technique for the patient. Osteophytes around the joint may cause a superficial bursitis, neuritis, or skin ulceration. It is possible to observe an interphalangeal joint hyperextension as compensation of restricted MTPJ dorsiflexion [1]. This could eventually lead to nail disorders due to the continuous trauma with the toe box of the shoe. Pain at the tarsometatarsal joint may also occur because of this same mechanical compensation.
The inability to effectively dorsiflex the hallux during the swing phase, transfer the load to the second and probably third metatarsal. In that case complaints that lead to seek medical advice could be those of transfer metatarsalgia. When this phenomenon takes place in a load transfer could even take place in the fifth metatarsal head, producing a mixed second and third rocker hyperkeratosis. This phenomenon can also be observed when the patient adopts an antalgic supinated gait due to overpulling of the anterior tibial tendon.
5 Conservative Treatment
Conservative care is the first indication for patients with hallux rigidus, depending on the extent of arthritis and symptoms. The measures commonly used include foot orthoses, modification in shoe-wear, limitations in activity, physical therapy, and injections with corticosteroid or sodium hyaluronate [1].
Foot orthoses and modified shoe-wear are used to reduced motion and impingement at maximum dorsiflexion [19]. One clinical study found that 47% of patients responded to custom orthoses alone, while another 10% responded to simple shoe modifications [20] (Level IV evidence).
Shoe modifications include using low-heeled shoes and toe boxes that allow for accommodation of the first MTPJ.
Injections with corticosteroid or sodium hyaluronate may provide temporary relief of symptoms. Pons and colleagues [21] prospectively compared the effects of injections with either corticosteroid or sodium hyaluronate. Clinical improvement was observed in both groups at 3 months.
The results of these studies suggest that conservative treatment relieves pain associated with daily activities and constitute fair evidence (grade B recommendation).
An insole with a Morton extension [22] is commonly used in the management of hallux rigidus. Made of either spring steel or carbon graphite composite, these extensions are embedded between the layers of the sole, extending from the heel to the toe. They can be placed in nearly any type of shoe and can be used together with a rocker sole to enhance its function. The Morton extension also acts as a splint, preventing the shoe from bending and in the process limiting dorsiflexion of the big toe during gait and decreasing the forces acting through the midfoot and forefoot. The rocker sole is one of the most prevalent modifications, the main function of which is to rock the foot from heel strike to toe-off without requiring the shoe or foot to bend. A high toe box can also be used to prevent direct contact between the dorsal osteophyte and shoe [23].
Functional orthoses have been designed to reverse the windlass mechanism, allowing the first metatarsal to achieve sufficient plantar flexion in preparation for propulsion. First-ray cutouts, designed to allow plantar flexion of the first ray and pronate the forefoot and forefoot postings are other functional orthotic modifications that have been used to improve first-ray function and reduce pain [6]. In contrast, accommodative orthoses are adopted for the immobilization and for the alteration of the magnitude and temporal loading patterns of the first MTPJ. Accommodative orthoses include custom orthoses with a navicular pad and Morton extensions [6].
Physical therapy involves joint mobilization, manipulation, improving range of motion, muscle reeducation, and strengthening of the flexor hallucis longus muscles as well as the plantar intrinsic muscles of the feet to improve the stability of the first MTPJ. Gait training, together with rest, ice, compression, and elevation, has also been advocated in the reduction of pain and inflammation [6].
6 Surgical Treatment
Surgical correction of hallux rigidus is indicated when conservative treatment fails to relieve pain. At the most basic level, the surgical options involve either preservation or destruction of the articular surfaces, and the decision to pursue one option over the other hinges on the degree of articular cartilage degeneration. At moderate stages, joint-preserving procedures constitute a more rational approach. Different techniques have been proposed, but the optimal surgical procedure has yet to be defined [11].
6.1 Joint-Preserving Procedures
6.1.1 Cheilectomy
Dorsal cheilectomy can be performed for patients in early stages of hallux rigidus. This can result in good relief of their symptoms provided that it mainly consist of impingement pain and stiffness in the absence of mid-range pain and a negative grind test. It is popular as an initial treatment for hallux rigidus as it improves pain, preserves joint movement, maintains joint stability, and keeps future secondary options open [24, 25]. The traditional open dorsal cheilectomy involves removing dorsal osteophytes from both the metatarsal and phalangeal side of the joint and up to 30% of the joint surface, in order to achieve dorsiflexion of greater than 45 degrees [26].
In Coughlin and Shurnas’s landmark series of 93 feet undergoing cheilectomy with a mean follow-up of 9.6 years, they noted a 92% success rate in terms of pain relief and function [10]. In a more recent investigation, Sidon et al. reported a 69% rate of patient satisfaction with a 29% of failure rate [27].
The main difficulty is selecting the correct patient suitable for dorsal cheilectomy. Most authors agree that mid-range pain with passive motion (Coughlin and Shurnas grade 4) is a contraindication for dorsal cheilectomy [25]. Easley et al. [28] reported in their series that 90% of the patients were satisfied with increased range, and there was a 40-point improvement in American Orthopaedic Foot and Ankle Society (AOFAS) score following cheilectomy at mean follow-up of 63 months. Of the 58 patients in the series of Nicolosi et al. [29], 51 (87.9%) experienced no limitations in their daily activities at an average follow-up of 7.1 years, with two patients (3.3%) subsequently requiring an arthrodesis. Teoh et al. [25] reported on a cohort of 89 patients (98 feet) which underwent minimally invasive cheilectomy followed for a mean of 50 months, with considerable improvement of VAS and self-reported outcome scores. Authors reported a 10% of grades 2 and 3 patients went onto an arthrodesis at a mean of 15 (range, 8–30) months after initial surgery, and this could be due to the fact that they offer MIS cheilectomy to a series of grade 3 patients.
6.1.2 Osteotomies
6.1.2.1 Metatarsal Osteotomies
Watermann was the first to report in 1927 a dorsal closing wedge trapezoidal osteotomy of the distal first metatarsal bone [13]. It was designed to relocate the viable plantar cartilage to a more dorsal location, allowing more dorsiflexion of the hallux. This was a relatively unstable osteotomy due to its perpendicular orientation and the resulting difficult fixation.
Decompressive osteotomy would theoretically be able to alleviate pain and improve function. A modification of this technique is the Green-Watermann, which involves decompression and offers a more stable configuration of the osteotomy. Finally, the long-arm decompression osteotomy was proposed by Robinson and Frank as an intermediate to the distal decompression osteotomies and more proximal plantarflexory osteotomies. They reported that it offered the possibility of greater shortening and greater plantar flexion than its more distal counterparts and was also more stable than the proximal osteotomies [11].
Although it was initially conceived for a long first metatarsal, Youngswick osteotomy (Figs. 3 and 4) showed good results in both harmonic and nonharmonic formulas, at alleviating pain and improving function over the short and intermediate terms [30]. Its rationale is to obtain a longitudinal decompression of the joint by proximal translation of the metatarsal head and plantarflexing it as desired by moving the apex of the osteotomy plantarly, allowing the surrounding soft tissues to relax and remodel. Concerns may arise about survival of this joint-preserving procedures although Slulitell et al. published in 2019 a report zero cases of progression to MTPJ arthrodesis despite of progressive worsening (recurrence of dorsal osteophyte and joint space narrowing) of the radiographic appearance in a cohort of 61 patients followed through a mean of 54.8 months [30].

Youngswick osteotomy. Placed in order to obtain a longitudinal decompression of the joint by proximal translation of the metatarsal head and plantarflexing it by moving the apex of the osteotomy plantarly

Youngswick osteotomy. Placed in order to obtain a longitudinal decompression of the joint by proximal translation of the metatarsal head and plantarflexing it by moving the apex of the osteotomy plantarly
6.1.2.2 Phalangeal Osteotomies
Dorsiflexion phalangeal osteotomy, as first described by Kessel and Bonnie in 1958, is an effective procedure for remodeling an arthritic first MTPJ, restoring pain-free movement to the joint, and alleviating the pain associated with footwear irritation of dorsal and medial osteophytes of the metatarsal head [31].
Roukis conducted a systematic review of 11 studies of cheilectomy and phalangeal dorsiflexion osteotomy, with a mean follow-up period of 12 months. In 374 procedures, pain was relieved in 89%, and 77% of the patients were satisfied or very satisfied with their outcomes. Just under 5% of the patients required revision surgery [32].
This osteotomy intends to gaining dorsiflexion at the expense of plantar flexion [33] by changing the orientation of the hallux in relation to the first metatarsal for a given angle between the metatarsal and proximal phalanx and may therefore change the direction or distribution of forces at the joint [33]. In a cadaveric study by Kim et al. [33], Moberg osteotomy proved to shift the center of contact pressure plantar an average of 0.7 mm, but did not decrease the peak pressure therefore offloading the diseased cartilage of the dorsal aspect of the joint. The Moberg osteotomy has been studied in patients with advanced hallux rigidus, showing a reduction in pain and improved range of motion 2–4 years after surgery [34]. Probably the main reason for the good results obtained with this technique is that less dorsiflexion is needed at the metatarsophalangeal joint, thus not producing any dorsal metatarsal impingement.
6.2 Joint-Sacrificing Techniques
6.2.1 Metatarsophalangeal Arthroplasty
Arthroplasty has been proposed as an alternative surgical option. The main advantage of arthroplasty over arthrodesis is the preservation of movement without the risk of malunion or nonunion.
Cook and Carpenter et al. [35, 36] divided the prosthetic implants of the first MTP joint into four categories:
-
First generation: silicone implants.
-
Second generation: silicone implants with grommets.
-
Third generation: metal implants with press-fit fixation.
-
Fourth generation: metal implants with threaded stem fixation.
Silastic implants using a silicone and plastic hybrid were introduced in the 1960s, to improve the outcome of the Keller’s arthroplasty [37]. They were originally single-stemmed hemi-implants. Initial studies in the 1980s, however, reported extremely high rates of complications and failure, including synovitis, migration, osteolysis, granulomas, and lymphadenopathy [38]. However those studies evaluated single-stemmed Silastic implants which are no longer commercially available.
Biomechanically, the Silastic implant is designed to act as a sloppy hinged dynamic spacer but has no inbuilt ability to correct deformity or maintain correction. It is not directly attached to the bone, allowing self-alignment in the axis of the joint. This, combined with its low modulus of elasticity, reduces stress-shielding and promotes bone loading, preventing bone reabsorption and fractures. It has viscoelastic properties and high resistance to fatigue. It is a single component; hence once encapsulation occurs, backside wear is not seen [37]. Cautions and contraindications for Silastic implants should be the same as for any arthroplasty. We would not recommend its use when there is a sizeable associated deformity such as valgus or in rheumatoid disease where the bone may be soft and/or cystic [39].
A recent systematic review suggested that arthroplasty leads to similar outcomes, satisfaction, rate of complications, and reoperation as arthrodesis [38, 39]. Despite several subsequent studies in the 1990s reporting good outcomes with the new implant with high satisfaction rates (80–90%), low rates of complication, failure, and revision [39, 40], it continues to be rarely used and remains a controversial surgical option for patients with end-stage HR [41].
There are several Silastic implants, with different stems length and angulation.
A 2020 study [39] on double stemmed Silastic implants reported a 97.2% implant survivorship at a mean 5.3 years follow-up in a 108 hallux rigidus patient population, with high satisfaction rates and considerable improvement in self-reported outcome measures. Three patients require revision (one infection and two implant fractures). A total of 25 patients (23.1%) had a complication, most were minor, responding to simple treatment, and authors stated that this did not affect the outcome. In the same scenario Van Duijvenbode et al. [42] described the results of 43 implants in 36 patients at a mean follow-up of 19 years. There was a 4% revision/reoperation rate, with one revision to a further Silastic implant at 9 years and two revisions to a Keller’s procedure at 13 and 17 years. They report good to excellent patient-reported outcome measures (PROM) scores and a median satisfaction rate of 10.
There are other possibilities when replacing the first MTPJ surface. A metallic proximal phalangeal resurfacing was evaluated in a recent review which included a total of 97 implants reported survival rates of 85.6% and rates of satisfaction of 75% at a median follow-up of 5.4 years. Causes of failure included osteolysis and deep infection but most commonly persistent pain. The authors concluded that this implant should be used with caution in younger patients due to the high revision rate [43].
Some three-component implants are available. There are studies showing good early results for these implants [44]. Titchener et al., however, reported alarming results in a series of 86 Toefit-Plus implants in 73 patients with a 9.3% intraoperative fracture rate and 24% revision rate at a mean follow-up of 33 months (2–72) [45]. Gupta and Masud [46] reported the results of 47 Toefit-Plus implants with a 21% (10/47) revision rate and a further 23% (11/47) complaining of ongoing pain at a mean follow-up of 11.1 years. This field is still of ongoing investigation although some results are promising in terms of preserving first MTPJ motion for those patients with severe HR.
6.2.2 Metatarsophalangeal Hemiarthroplasty
Hemiarthroplasty consists of a unipolar implant designed to replace the articular surface of the head of the metatarsal or the proximal phalanx base. This procedure requires less bone resection and maintains the length of the first ray. Moreover, if a conversion to arthrodesis becomes necessary, it should be technically easier. Meriç et al. [47], with a mean follow-up of 24.2 ± 7.2 months, reported an improvement from a preoperative AOFAS score of 33.9 ± 9.8 points to a final follow-up score of 81.6 ± 10.1 points, VAS diminished from 8.4 ± 0.9 to 1.21 ± 1.2 and first MTPJ ROM improved from 22.8° to 69.6°. There was no implant loosening at follow-up and only one case of revision in arthrodesis due to pain and immobility.
Mermerkaya and Adli [48] have retrospectively compared outcomes of total joint arthroplasty and hemiarthroplasty of the metatarsal component to a mean follow-up of 27.1 ± 7.5 months and 29.9 ± 5.2 months, respectively. Authors have observed significant improvement in AOFAS scores and significant decreases in VAS in both groups at follow-up, with no significant between-group difference, at last, follow-up. No implant loosening, radiolucency, or subsidence was found in the cases treated.
6.2.3 Polyvinyl Alcohol Implant
Historically , the most commonly performed procedure in patients with moderate to severe HR is arthrodesis; however, this procedure leaves the patient with no motion through the first MTPJ [49]. Newer techniques have focused on procedures that maintain range of motion (ROM) and allow patients to weight-bear immediately following surgery [50].
A novel polyvinyl alcohol (PVA) hydrogel implant has recently been developed [51]. This synthetic material has water content comparable to healthy cartilage and a compressive modulus and tensile strength similar to human articular cartilage. Therefore it can withstand shear and axial load forces beyond those experienced in the great toe, without fragmentation. These biomechanical features make it an ideal material for use in hemiarthroplasty of the first MTPJ [50].
The efficacy and safety of this small PVA hydrogel implant in comparison to first MTPJ arthrodesis was recently evaluated in a prospective, randomized, clinical trial conducted at 12 centers in Canada and the United Kingdom. At the 2-year follow-up, the implant hemiarthroplasty demonstrated equivalent pain relief and functional outcomes to first MTPJ arthrodesis, with no cases of implant fragmentation, wear, or bone loss [52].
An additional study evaluated the 5-year outcome of 27 grade 2, 3, and 4 HR patients treated in 3 different centers, which were assigned to the PVA implant in a random manner and reported clinically and statistically significant improvements in patient-reported outcome measures (VAS, SF-36 FAAM-ADL) and 65% of patients rating their overall function level as normal, with a 96% implant survivorship [50]. Interestingly, range of motion through the MTP joint improved following hemiarthroplasty with the PVA hydrogel implant compared with baseline, which represents an additional benefit to these patients.
Cassinelli et al. [53], in a non-designer study, reported less favorable results in a series of 64 implants in 60 patients with 38% (24/64) being “unsatisfied” or “very unsatisfied,” a 20% (13/64) reoperation rate, and an 8% (5/64) rate of conversion to arthrodesis , at a mean follow-up of 18.5 months (12–30).
6.2.4 Metatarsophalangeal Arthrodesis
First MTPJ fusion today represents the mainstay of surgical care for high-grade, advanced hallux rigidus [54]. Improvement of pain is achieved by eliminating residual degenerated cartilage layer, overstepping the subchondral bone and sacrificing the joint motion. Preparation of the surfaces may lead to the creation of complementary bone interfaces, through flat or conical molding of the metatarsal and phalangeal portions [54].
Fusion rates have been observed between 53% and 100%, depending on the type of fixation and type of pathoanatomy [55]. Chraim et al. [56] reported the long-term outcome of first MTPJ fusion using a transarticular screw and dorsal non-locked plate, with 93.3% of fusion rate and 6.7% of painless nonunion with no needed additional surgery.
Arthrodesis is particularly indicated in younger patients, with mid- or high-performance requests or more active patients, in severe pathologies, such as salvage procedure in recurrences or failed motion-sparing procedures (Fig. 5a–c). Recommended fixation of the hallux is 10°–15° of dorsiflexion and 10°–15° of valgus [57, 58].

First MTPJ arthrodesis as a procedure to save a failed hemiarthroplasty that was in an unacceptable hyperextension. (a) Radiograph depicting the hemiarthroplasty implant in position. Note the osteolysis around the implant stem. (b) Photograph demostrating the hyperextension of the MTPJ tha caused pain with shoe wearing. (c) Correct aligmnent after MTPJ arthrodesis
Different fixation techniques have been described to achieve fusion [59]. Recent plating techniques yielded significant improvements in fixation stability and union rates. While plating techniques are highly successful, they necessitate a relatively large dorsal incision, which can lead to postoperative complications. The plates can also be bulky, creating subsequent symptoms during activities and showing wear over time. In contrast, arthroscopic fusion requires smaller incisions, which may result in less swelling, less pain, and fewer complications. The evolution of minimally invasive techniques and instruments has enabled the arthroscopic preparation of an arthritic hallux MTPJ for arthrodesis. Fixation for arthroscopic MTPJ fusion can be achieved by crossing compression lag screw [60].
Compression lag screws were previously compared with standard dorsal plates, and standard plates were shown to be mechanically superior. Fully threaded headless screws may provide superior stability when compared with compression lag screws because the threads engage the cortex in three places, the outer cortex at the site of insertion and both cortices at the MTPJ. Standard compression lag screw threads, however, do not always engage cortical bone, depending on surgeon technique. Fully threaded screws may provide a more stable construct to allow early weight-bearing, particularly if the subchondral plate is preserved.
In a cadaveric study which compared the mechanical stability of the current generation of locking plates used in conjunction with a single compression lag screw to fully threaded headless compression screws, there was a significant difference in mean stiffness in favor of the plate plus lag screw construct; however, no significant difference was found when examining mean load to failure [60].
6.2.5 Resection and Interposition Arthroplasty
A simple resection technique of the first phalangeal base has been described in 1904 by Keller and Menger [61], for treatment of hallux valgus associated with osteoarthritis of the first metatarsophalangeal joint, without replacement of the joint space with non-tissue implants. Actually, this technique is used for decompression and restoration of range of motion of high-grade hallux rigidus, especially in those patients that refuse arthrodesis. Complications described include first MTPJ instability, cock-up deformity and transfer metatarsalgia [54]. This procedure is usually reserved for older and low demand patients.
When a traditional resection arthroplasty is combined with the insertion of a biologic spacer into the joint, it is called interposition arthroplasty. Its rationale is given by the reduction in bone loss from the proximal phalangeal base, the maintenance of length, and improving joint stability and motion. Various tissues have been utilized and described: capsular autograft, meniscus allograft, regenerative tissue matrix, and tendon autograft [62, 63].
7 Summary
Hallux rigidus is still a complex entity in which optimal treatment has yet to be defined. New developments and techniques should be in the direction of joint and motion preservation, especially in high demand or younger patients.
References
Migues A, Slullitel G. Joint-preserving procedure for moderate hallux rigidus. Foot Ankle Clin. 2012;17(3):459–71. https://doi.org/10.1016/j.fcl.2012.06.006.
Maceira E, Monteagudo M. Functional hallux rigidus and the Achilles-calcaneus-plantar system. Foot Ankle Clin. 2014;19(4):669–99. https://doi.org/10.1016/j.fcl.2014.08.006.
Viehöfer AF, Vich M, Wirth SH, Espinosa N, Camenzind RS. The role of plantar fascia tightness in hallux limitus: a biomechanical analysis. J Foot Ankle Surg. 2019;58(3):465–9. https://doi.org/10.1053/j.jfas.2018.09.019.
Coughlin MJ, Shurnas PS. Hallux rigidus: grading and long term results of operative treatment. J Bone Joint Surg Am. 2003;85:2072–88.
Lucas DE, Hunt KJ. Hallux rigidus: relevant anatomy and pathophysiology. Foot Ankle Clin. 2015;20(3):381–9. https://doi.org/10.1016/j.fcl.2015.04.001.
Kunnasegaran R, Thevendran G. Hallux rigidus: nonoperative treatment and orthotics. Foot Ankle Clin. 2015;20(3):401–12. https://doi.org/10.1016/j.fcl.2015.04.003.
Flavin R, Halpin T, O’Sullivan R, et al. A finite-element analysis study of the metatarsophalangeal joint of the hallux rigidus. J Bone Joint Surg Br. 2008;90(10):1334–40.
Cheung ZB, Myerson MS, Tracey J, Vulcano E. Weightbearing CT scan assessment of foot alignment in patients with hallux rigidus. Foot Ankle Int. 2018;39:67–74. https://doi.org/10.1177/1071100717732549.
Roukis TS. Metatarsus primus elevatus in hallux rigidus. Fact or fiction? J Am Podiatr Med Assoc. 2005;95(3):221–8.
Coughlin MJ, Shurnas PS. Hallux rigidus: demographics, etiology, and radiographic assessment. Foot Ankle Int. 2003;24(10):731–43. https://doi.org/10.1177/107110070302401002.
Slullitel G, López V, Seletti M, Calvi JP, Bartolucci C, Pinton G. Joint preserving procedure for moderate hallux rigidus: does the metatarsal index really matter? J Foot Ankle Surg. 2016;55(6):1143–7. https://doi.org/10.1053/j.jfas.2016.06.003.
Hunt K, Anderson R. Biplanar proximal phalanx closing wedge osteotomy for hallux rigidus. Foot Ankle Int. 2012;33(12):1043–50.
Galois L, Hemmer J, Ray V, Sirveaux F. Surgical options for hallux rigidus: state of the art and review of the literature. Eur J Orthop Surg Traumatol. 2020;30(1):57–65. https://doi.org/10.1007/s00590-019-02528-x.
Beeson P, Phillips C, Corr S, Ribbans W. Classification systems for hallux rigidus: a review of the literature. Foot Ankle Int. 2008;29(4):407–14.
Baumhauer JF, Singh D, Glazebrook M, et al. Prospective, randomized, multi-centered clinical trial assessing safety and efficacy of a synthetic cartilage implant versus first metatarsophalangeal arthrodesis in advanced hallux rigidus. Foot Ankle Int. 2016;37(5):457–69. https://doi.org/10.1177/1071100716635560.
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012;20(6):347–58.
Hamid KS, Parekh SG. Clinical presentation and management of hallux rigidus. Foot Ankle Clin. 2015;20(3):391–9.
Ho B, Baumhauer J. Hallux rigidus. EFORT Open Rev. 2017;2:13–20. https://doi.org/10.1302/2058-5241.2.160031.
Smith RW, Katchis SD, Ayson LC. Outcomes in hallux rigidus patients treated nonoperatively: a long-term follow-up study. Foot Ankle Int. 2000;21(11):906–13.
Horton GA, Parks YW, Myerson MS. Role of metatarsus primus elevatus in the pathogenesis of hallux rigidus. Foot Ankle Int. 1999;20(12):777–80.
Pons M, Alvarez F, Solana J, et al. Sodium hyaluronate in the treatment of hallux rigidus. A single-blind, randomized study. Foot Ankle Int. 2007;28(1):38–42.
Sammarco VJ, Nichols R. Orthotic management for disorders of the hallux. Foot Ankle Clin. 2005;10(1):191–209.
Janisse DJ, Janisse E. Shoe modification and the use of orthoses in the treatment of foot and ankle pathology. J Am Acad Orthop Surg. 2008;16(3):152–8.
Walter R, Perera A. Open, arthroscopic, and percutaneous cheilectomy for hallux rigidus. Foot Ankle Clin. 2015;20(3):421–31.
Teoh KH, Tan WT, Atiyah Z, Ahmad A, Tanaka H, Hariharan K. Clinical outcomes following minimally invasive dorsal cheilectomy for hallux rigidus. Foot Ankle Int. 2019;40(2):195–201. https://doi.org/10.1177/1071100718803131.
Stevens R, Bursnall M, Chadwick C, Davies H, Flowers M, Blundell C, Davies M. Comparison of complication and reoperation rates for minimally invasive versus open cheilectomy of the first metatarsophalangeal joint. Foot Ankle Int. 2020;41(1):31–6. https://doi.org/10.1177/1071100719873846.
Sidon E, Rogero R, Bell T, McDonald E, Shakked RJ, Fuchs D, Daniel JN, Pedowitz DI, Raikin SM. Long-term follow-up of cheilectomy for treatment of hallux Rigidus. Foot Ankle Int. 2019;40(10):1114–21. https://doi.org/10.1177/1071100719859236.
Easley ME, Davis WH, Anderson RB. Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int. 1999;20(3):147–52. https://doi.org/10.1177/107110079902000302.
Nicolosi N, Hehemann C, Connors J, Boike A. Long-term follow-up of the cheilectomy for degenerative joint disease of the first metatarsophalangeal joint. J Foot Ankle Surg. 2015;54(6):1010–20.
Slullitel G, López V, Calvi JP, D'Ambrosi R, Usuelli FG. Youngswick osteotomy for treatment of moderate hallux rigidus: thirteen years without arthrodesis. Foot Ankle Surg. 2019:S1268-7731(19)30208-5. https://doi.org/10.1016/j.fas.2019.11.008.
Coutts A, Kilmartin TE. Dorsiflexory phalangeal osteotomy for grade II hallux rigidus: patient-focused outcomes at eleven-year follow-up. J Foot Ankle Surg. 2019;58(1):17–22. https://doi.org/10.1053/j.jfas.2018.06.004.
RoukisTS. Outcomes after cheilectomy with phalangeal dorsiflexory osteotomy for hallux rigidus:a systematic review. J Foot Ankle Surg. 2010;49:479–87.
Kim PH, Chen X, Hillstrom H, Ellis SJ, Baxter JR, Deland JT. Moberg osteotomy shifts contact pressure plantarly in the first metatarsophalangeal joint in a biomechanical model. Foot Ankle Int. 2016;37(1):96–101. https://doi.org/10.1177/1071100715603513.
O’Malley MJ, Basran HS, Gu Y, et al. Treatment of advanced stages of hallux rigidus with cheilectomy and phalangeal osteotomy. J Bone Joint Surg Am. 2013;95:606–5. https://doi.org/10.2106/JBJS.K.00904.
Cook KD. Capsular interposition for the Keller bunionectomy with the use of soft-tissue anchors. J Am Podiatr Med Assoc. 2005;95(2):180–2. https://doi.org/10.7547/0950180.
Carpenter B, Smith J, Motley T, Garrett A. Surgical treatment of hallux rigidus using a metatarsal head resurfacing implant: mid-term follow-up. J Foot Ankle Surg. 2010;49:321–5. https://doi.org/10.1053/j.jfas.2010.04.007.
Swanson AB, Lumsden RM, Swanson GD. Silicone implant arthroplasty of the great toe. A review of single stem and flexible hinge implants. Clin Orthop Relat Res. 1979;142:30–43.
Clough TM, Ring J. Silastic first metatarsophalangeal joint arthroplasty for the treatment of end-stage hallux rigidus. Bone Joint J. 2020;102-B(2):220–6. https://doi.org/10.1302/0301-620X.102B2.BJJ-2019-0518.R2.
Park YH, Jung JH, Kang SH, Choi GW, Kim HJ. Implant arthroplasty versus arthrodesis for the treatment of advanced hallux rigidus: a meta-analysis of comparative studies. J Foot Ankle Surg. 2019;58(1):137–43.
Ter Keurs EW, Wassink S, Burger BJ, Hubach PC. First metatarsophalangeal joint replacement: long-term results of a double stemmed flexible silicone prosthesis. Foot Ankle Surg. 2011;17(4):224–7.
Majeed H. Silastic replacement of the first metatarsophalangeal joint:historical evolution, modern concepts and a systematic review of the literature. EFORT Open Rev. 2019;4(3):77–84.
van Duijvenbode DC, Bulstra GH, Nijsse BA. Nineteen-year follow-up of the silastic double stemmed hinge prosthesis of the first metatarsophalangeal joint. Foot Ankle Surg. 2013;19(1):27–30.
Clement ND, MacDonald D, Dall GF, et al. Metallic hemiarthroplasty for the treatment of end-stage hallux rigidus: mid-term implant survival, functional outcome and cost analysis. Bone Joint J. 2016;98-B(7):945–51.
Tunstall C, Laing P, Limaye R, et al. 1st metatarso-phalangeal joint arthroplasty with ROTO-glide implant. Foot Ankle Surg. 2017;23(3):153–6.
Titchener AG, Duncan NS, Rajan RA. Outcome following first metatarsophalangeal joint replacement using TOEFIT-PLUS™: a midterm alert. Foot Ankle Surg. 2015;21(2):119–24.
Gupta S, Masud S. Long term results of the Toefit-Plus replacement for first metatarsophalangeal joint arthritis. The Foot (Edinb). 2017;31:67–71.
Meriç G, Erduran M, Atik A, Köse Ö, Ulusal AE, Akseki D. Short-term clinical outcomes after first metatarsal head resurfacing hemiarthroplasty for late stage hallux rigidus. J Foot Ankle Surg. 2015;54(2):173–8. https://doi.org/10.1053/j.jfas.2014.10.016.
Mermerkaya MU. Adli H.a comparison between metatarsal head-resurfacing hemiarthroplasty and total metatarsophalangeal joint arthroplasty as surgical treatments for hallux rigidus: a retrospective study with short- to midterm follow-up. Clin Interv Aging. 2016;11:1805–13. https://doi.org/10.2147/CIA.S110865.
Yee G, Lau J. Current concepts review: hallux rigidus. Foot Ankle Int. 2008;29(6):637–46. https://doi.org/10.3113/FAI.2008.0637.
Daniels TR, Younger AS, Penner MJ, et al. Midterm outcomes of polyvinyl alcohol hydrogel hemiarthroplasty of the first metatarsophalangeal joint in advanced hallux rigidus. Foot Ankle Int. 2017;38(3):243–7. https://doi.org/10.1177/1071100716679979.
Younger ASE, Baumhauer JF. Polyvinyl alcohol hydrogel hemiarthroplasty of the great toe: technique and indications. Techn Foot Ankle Surg. 2013;12(3):164–9.
Baumhauer JF, Singh D, Glazebrook M, et al. Correlation of hallux rigidus grade with motion, VAS pain, intraoperative cartilage loss, and treatment success for first MTP joint arthrodesis and synthetic cartilage implant. Foot Ankle Int. 2017;38(11):1175–82. https://doi.org/10.1177/1071100717735289.
Cassinelli SJ, Chen S, Charlton TP, Thordarson DB. Early outcomes and complications of synthetic cartilage implant for treatment of hallux rigidus in the United States. Foot Ankle Int. 2019;40(10):1140–8.
Massimi S, Caravelli S, Fuiano M, Pungetti C, Mosca M, Zaffagnini S. Management of high-grade hallux rigidus: a narrative review of the literature. Musculoskelet Surg. 2020; https://doi.org/10.1007/s12306-020-00646-y.
Raikin SM, Ahmad J. Comparison of arthrodesis and metallic hemiarthroplasty of the hallux metatarsophalangeal joint: surgical technique. J Bone Joint Surg Am. 2008; https://doi.org/10.2106/JBJS.H.00368.
Chraim M, Bock P, Alrabai HM, Trnka HJ. Long-term outcome of first metatarsophalangeal joint fusion in the treatment of severe hallux rigidus. Int Orthop. 2016; https://doi.org/10.1007/s00264-016-3277-1.
Kelikian AS. Technical considerations in hallux metatarsophalangeal arthrodesis. Foot Ankle Clin. 2005;10(1):167–90.
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013;34(1):15–32. https://doi.org/10.1177/1071100712460220.
Migues A, Calvi J, Sotelano P, Carrasco M, Slullitel G, Conti L. Endomedullary screw fixation for first metatarsophalangeal arthrodesis. Foot Ankle Int. 2013;34(8):1152–7. https://doi.org/10.1177/1071100713483113.
Fuld RS 3rd, Kumparatana P, Kelley J, Anderson N, Baldini T, Younger ASE, Hunt KJ. Biomechanical comparison of low-profile contoured locking plate with single compression screw to fully threaded compression screws for first MTP fusion. Foot Ankle Int. 2019;40(7):836–44. https://doi.org/10.1177/1071100719837524.
Konkel KF, Menger AG. Mid-term results of titanium hemi-great toe implants. Foot Ankle Int. 2006;27(11):922–9.
Clews CNL, Kingsford AC, Samaras DJ. Autogenous capsular interpositional arthroplasty surgery for painful hallux rigidus: assessing changes in range of motion and postoperative foot health. J Foot Ankle Surg. 2015;54(1):29–36. https://doi.org/10.1053/j.jfas.2014.09.004.
Delacruz EL, Johnson AR, Clair BL. First metatarsophalangeal joint interpositional arthroplasty using a meniscus allograft for the treatment of advanced hallux rigidus: surgical technique and short-term results. Foot Ankle Spec. 2011;4(3):157–64. https://doi.org/10.1177/1938640011402821.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Slullitel, G., Lopez, V. (2022). Hallux Rigidus: A Comprehensive Review. In: Wagner Hitschfeld, E., Wagner Hitschfeld, P. (eds) Foot and Ankle Disorders. Springer, Cham. https://doi.org/10.1007/978-3-030-95738-4_18
Download citation
DOI: https://doi.org/10.1007/978-3-030-95738-4_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-95737-7
Online ISBN: 978-3-030-95738-4
eBook Packages: MedicineMedicine (R0)