
Abstract
Purpose
Several studies have revealed that robot-assisted technique might improve the pedicle screw insertion accuracy, but owing to the limited sample sizes in the individual study reported up to now, whether or not robot-assisted technique is superior to conventional freehand technique is indefinite. Thus, we performed this systematic review and meta-analysis based on randomized controlled trials to assess which approach is better.
Methods
Electronic databases including PubMed, EMBASE, CENTRAL, ISI Web of Science, CNKI and WanFang were systematically searched to identify potentially eligible articles. Main endpoints containing the accuracy of pedicle screw implantation and proximal facet joint violation were evaluated as risk ratio (RR) and the associated 95% confidence intervals (95% CIs), while radiation exposure and surgical duration were presented as mean difference (MD) or standard mean difference (SMD). Meta-analyses were performed using RevMan 5.3 software.
Results
Six studies involving 158 patients (688 pedicle screws) in robot-assisted group and 148 patients (672 pedicle screws) in freehand group were identified matching our study. The Grade A accuracy rate in robot-assisted group was superior to freehand group (RR 1.03, 95% CI 1.00, 1.06; P = 0.04), but the Grade A + B accuracy rate did not differ between the two groups (RR 1.01, 95% CI 0.99, 1.02; P = 0.29). With regard to proximal facet joint violation, the combined results suggested that robot-assisted group was associated with significantly fewer proximal facet joint violation than freehand group (RR 0.07, 95% CI 0.01, 0.55; P = 0.01). As was the radiation exposure, our findings suggested that robot-assisted technique could significantly reduce the intraoperative radiation time (MD − 12.38, 95% CI − 17.95, − 6.80; P < 0.0001) and radiation dosage (SMD − 0.64, 95% CI − 0.85, − 0.43; P < 0.00001). But the overall surgical duration was longer in robot-assisted group than conventional freehand group (MD 20.53, 95% CI 5.17, 35.90; P = 0.009).
Conclusions
The robot-assisted technique was associated with equivalent accuracy rate of pedicle screw implantation, fewer proximal facet joint violation, less intraoperative radiation exposure but longer surgical duration than freehand technique. Powerful evidence relies on more randomized controlled trials with high quality and larger sample size in the future.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pedicle screws have revolutionized the spinal surgery since their introduction to clinical application [1]. The success of robust fixation relies on the perfect insertion of the screws inside the pedicle. However, the procedure for accurate pedicle screw placement is challenging because of the complex anatomical structures surrounding the spine and widely morphologic variations of individual pedicles [2,3,4,5]. By means of conventional techniques, pedicle screws were implanted according to anatomical landmarks and intraoperative fluoroscopy. But the screw misplacement cannot be neglected, a literature had reported the percentage of misplaced screws ranging from 8.3 to 50.3% with conventional fluoroscopy [6]. Even though severe complications including vascular, neurological or visceral injuries just occur to a small number of patients after pedicle screws’ malposition, the complications can be potentially life and limb threatening.
To address the issue of pedicle screws’ malposition, image guidance system was explored and applied to spine surgery [7, 8]. Theoretically, the new technique can prevent complications by providing more precise anatomic guidance, but Verma et al.’s meta-analysis based on former studies did not favor computer-assisted navigation over conventional techniques [9]. Besides, with the more widespread application of image-guided techniques, issues such as reduction of radiation exposure, the operating time and cost-effectiveness need to be addressed as well [8]. The unsatisfactory issues in spine surgeries inspired the emergence of robot-guided pedicle screw insertion. Recently, a miniature robot has been devised for the purpose of improving the accuracy of pedicle screw placement, decreasing potential complications and reducing intraoperative radiation exposure [10,11,12]. Since 2006, a number of studies have reported the results of robot-assisted and conventional freehand pedicle screw placement techniques. However, the results remain inconsistent.
By far, two meta-analyses [13, 14] comparing robot-assisted and conventional freehand pedicle screw implantation have been published, but neither was based on RCTs, which will lead to less powerful results compared to study purely based on RCTs. Furthermore, in these two previously published studies, only accuracy of pedicle screws was combined using meta-analysis, other outcomes such as intraoperative radiation exposure, surgical duration and proximal facet joint violation were not combined. Thus, it is increasingly necessary to perform an updated meta-analysis based on RCTs. Our systematic review and meta-analysis were performed with the aim of investigating the difference of pedicle screw positioning accuracy, radiation exposure, surgical time and proximal facet joint violation between robot-assisted and conventional freehand technique based on RCTs.
Methods
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement [15].
Literature search strategy
Six electronic databases including PubMed, EMBASE, CENTRAL, ISI Web of Science, CNKI and WanFang were systematically searched to identify potentially eligible articles. All the above databases were searched from inception to the latest issue (May 2017), without language restriction. Medical Subject Headings (MeSH) and free text words were combined to retrieve all the potential studies. MeSH were modified based on the specifications of each database. The following search strategy was used for the literature search in PubMed, CENTRAL and ISI Web of Science: (“Robotics”[Mesh] or robot or robotics or robotic) and (“Pedicle Screws”[Mesh] or “Bone Screws”[Mesh] or “Spine”[Mesh] or pedicle or screw or spine or bone screws) and (randomized controlled trial or randomized controlled trial or RCT or RCTs). For CNKI and WanFang, search terms were “ji qi ren” and “zhui gong gen”. In addition, the bibliographies of relevant systematic reviews were manually searched.
Inclusion criteria
We established the inclusion and exclusion criteria based on the PICOS principle. (1) Types of participants: patients presenting with lumbar spinal stenosis, degenerative lumbar disorders or other lumbar diseases that scheduled to undergo pedicle screw placement were included in our study, no specific indications were imposed. (2) Interventions: patients in experimental groups received robot-assisted pedicle screw implantation surgery. (3) Control: patients in control groups received pedicle screw surgery with the conventional freehand approach. (4) Outcome measurements: the primary outcome of our systematic review was the accuracy of pedicle screw replacement, assessed by Gertzbin–Robbins classification [16], Rampersaud scale [17] along with other well-established criteria. Secondary outcomes included radiation exposure, surgical time and proximal facet joint violation between robot-assisted and conventional freehand technique. (5) Types of publication: only randomized controlled trials (RCTs) could be included in our systematic review. Cohort studies, reviews articles, case reports or expert experience reports were excluded.
Data extraction
Two investigators (Z. Lv and S. Gao) screened each article independently and were blinded to the findings of the other reviewer. According to the predetermined inclusion criteria, two reviewers performed a strict screening to identify qualified articles independently, and they extracted data from these eligible articles using a standardized data collection form, which included first author, year of the publication, number of patients and number of screws implanted in different groups, robot type, assessment of screw accuracy, clinical outcome assessments. Any disagreement between the two reviewers was resolved through discussion until a consensus was reached. The third review author (H. Fang) was consulted if a consensus could not be reached.
Quality assessment
The Cochrane Collaboration’s tool was utilized to assess the risk of bias in the selected RCTs, which was based on seven items: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. Two reviewers assessed the risk of bias among studies independently, the results were compared afterwards. Disagreements regarding the risk of bias assessment were settled by discussion and consensus between reviewers.
Data synthesis and analysis
Risk ratio (RR) and the associated 95% confidence intervals (CIs) were calculated for accuracy of pedicle screw implantation and proximal facet joint violation. The mean difference (MD) or standard mean difference (SMD) in the continuous variables was calculated using the same methodology. The Chi-squared test and the Higgins I 2 test were used to assess the heterogeneity among studies (P > 0.1 and I 2 indicate acceptable heterogeneity). We used fixed-effect model if no obvious heterogeneity existed. Otherwise, a random-effect model was utilized. Forest plot and funnel plot were generated via RevMan 5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
In case that significant heterogeneity existed, subgroup-analysis by risk of bias of included studies was conducted. Begg’s rank correlation test and Egger’s linear regression test were used to evaluate the publication bias (StataCorp LP, USA).
Results
Literature search
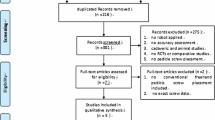
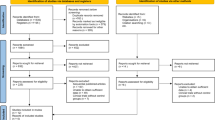
The literature selection process is presented in Fig. 1. The initial literature search yielded 155 potentially eligible records including 17 from PubMed, 21 from EMBASE, 10 from ISI Web of Science, 9 from CENTRAL, 44 from Wanfang and 54 from CNKI. 54 records were removed because they were duplicated for retrieval, the remaining 101 studies were screened with titles and abstracts. After the stage of title and abstract screening, eight articles were downloaded for full-text screening. One study [18] was removed because it was an editorial, one study [19] was deleted because it was duplicated. Finally, 6 RCTs [20,21,22,23,24,25] were deemed eligible and included in the meta-analysis.

Flowchart of literature selection
Main characteristics of included studies
Six studies involving 158 patients (688 pedicle screws) in robot-assisted groups and 148 patients (672 pedicle screws) in conventional freehand groups were included in our study. Each study was conducted in a single center, three studies [20,21,22] were performed in South Korea, two [23, 24] were conducted in Germany, the remaining one study [25] was performed in China. All the RCTs used post-operative thin-cut CT to evaluate the accuracy of pedicle screw implantation, and the scale used to assess the accuracy of pedicle screw was consistent across studies. The main characteristics of included RCTs are summarized in Table 1.
Quality assessment
The Cochrane’s tool was employed for appraisal of risk of bias for included RCTs. All the studies claimed randomization, but two studies [23, 24] failed to report the method of random sequence generation. Allocation concealment was well conducted in four studies [20,21,22, 25]. Regarding the blinding of personnel and participants, it was unfeasible to blind the spinal surgeons in our included studies so it was judged to high risk of bias in all selected RCTs. Two articles [20, 24] failed to report the blinding of outcome assessment, and they were judged to unclear risk of bias. When it comes to the incomplete outcome data and selective reporting, the Roser et al. study [24] was judged to high risk of bias because Roser et al. reported their preliminary results of 37 patients, with fewer patients undergoing fluoroscopy-guided (n = 10) than robot-assisted techniques (n = 18), and Roser et al. did not perform statistical analysis due to limited statistical power. The reviewers’ judgments about each risk of bias item for each included RCT is presented in Fig. 2.

Risk of bias summary: review authors’ judgements about each risk of bias item for each included study
Meta-analysis results
Pedicle screw placement accuracy
The comparison of accuracy of pedicle screw implantation between robot-assisted and conventional freehand according to Gerztbein–Robbins Classification (Grade A, 0 mm) is shown in Fig. 3. The heterogeneity between studies were significant (P = 0.07, I 2 = 51%), thus the random-effect model was used for statistical analysis. The combined results showed that robot-assisted pedicle screw placement was not significantly different from conventional freehand technique (τ 2 = 0.00, χ 2 = 10.28, df = 5; RR 1.02, 95% CI 0.98, 1.06). Fig. 4 presents the comparison of accuracy according to the Gertzbein–Robbins Grade A + B criteria. Random-effect model was employed due to obvious between-study heterogeneity (P = 0.002, I 2 = 73%), pooled results indicated that robot-assisted pedicle screw placement was not prior to freehand approach (τ 2 = 0.00, χ 2 = 18.69, df = 5; RR 1.00, 95% CI 0.97, 1.02).

Forest plot of robot-assisted versus conventional freehand technique: accuracy of screw according to Grade A criteria

Forest plot of robot-assisted versus conventional freehand technique: accuracy of screw according to Grade A + B criteria
Proximal facet joint violation
Proximal facet joint violation was reported by two RCTs [20, 22], and the facet joint violation was evaluated using post-operative fine-cut CT. The combined results suggested that robot-assisted pedicle screw placement was associated with significantly fewer proximal facet joint violation than conventional freehand technique (χ 2 = 1.12, I 2 = 0%; RR 0.07, 95% CI 0.01, 0.55) (Fig. 5).

Forest plot of robot-assisted versus conventional freehand technique: proximal facet joint violation
Radiation exposure
Three studies reported intraoperative radiation exposure as secondary endpoints, but only two studies [20, 24] provided detailed data on radiation exposure time and radiation dosage. The combined intraoperative radiation time showed that robot-assisted pedicle screw placement could significantly reduce the radiation time than conventional freehand pedicle screw implantation (MD − 12.38, 95% CI − 17.95, − 6.80; I 2 = 84%) (Fig. 6). Furthermore, robot-assisted pedicle screw placement was associated with significantly fewer intraoperative radiation dosage (SMD − 0.64, 95% CI − 0.85, − 0.43; I 2 = 10%) (Fig. 7).

Forest plot of robot-assisted versus conventional freehand technique: radiation time

Forest plot of robot-assisted versus conventional freehand technique: radiation dosage
Surgical duration
Three RCTs [20, 22, 25] mentioned the overall surgical time from skin to skin, the findings of these studies were pooled using meta-analysis, with only one study favoring robot-assisted procedure. The combination of surgical time suggested that the overall surgical duration from skin to skin differed significantly between robot-assisted and conventional freehand pedicle screw implantation (MD 20.53, 95% CI 5.17, 35.90; I 2 = 10%) (Fig. 8).

Forest plot of robot-assisted versus conventional freehand technique: surgical time
Subgroup-analysis and publication bias
In the comparison of accuracy of pedicle screw implantation, obvious heterogeneity was detected regardless of using Gertzbein–Robbins Grade A criteria or Gertzbein–Robbins Grade A + B criteria. We performed subgroup analysis according to the methodological quality of included studies. Ringel et al. and Roser et al. study failed to report the random sequence generation and allocation concealment, so the aforementioned studies were assigned into the “without random sequence generation and allocation concealment” subgroup. According to the Gertzbein–Robbins Grade A (0 mm) criteria, there was no obvious heterogeneity between studies that reported random sequence generation and allocation concealment (P = 0.90, I 2 = 0%), and the combined results favored robot-assisted pedicle screw placement (RR 1.03, 95% CI 1.00, 1.06; P = 0.04). Similarly, according to the Gertzbein–Robbins Grade A + B criteria (2 mm), no obvious between-study heterogeneity existed in RCTs that reported random sequence generation and allocation concealment (P = 0.71, I 2 = 0%). The meta-analysis results showed that there was no significant difference between robot-assisted and conventional freehand pedicle screw placement (RR 1.01, 95% CI 0.99, 1.02; P = 0.29).When removing the studies without random sequence generation and allocation concealment, the heterogeneity in comparison of accuracy of pedicle screw placement was not significant, thus we removed Roser et al. study and Ringel et al. study from our meta-analyses.
Begg’s test (Grade A: z = 0.34, P = 0.73; Grade A + B: z = − 0.34, P = 1.00) and Egger’s test (Grade A: t = 0.99, P = 0.43; Grade A + B: t = 2.36, P = 0.14) revealed no significant publication bias in the accuracy of pedicle screw placement.
Discussion
To the best of our knowledge, this is the first meta-analysis and systematic review to compare robot-assisted and freehand pedicle screw implantation purely based on RCTs with the consideration of heterogeneity across included studies. In two previously published meta-analyses [13, 14], no definite conclusions could be drawn to unequivocally recommend one surgical technique over the other. The major methodological concern in above studies was the inclusion of both RCTs and cohort studies for meta-analysis, which could lead to less powerful results. The way screw accuracy was defined and measured was also noted to vary among their included studies. Another methodological flaw to be considered was the absence of an investigation of publication bias, publication bias might arise because only articles published in English were included by aforementioned meta-analyses.
In our current study, only RCTs that featured to compare robot-assisted and conventional freehand pedicle screw placement were included for meta-analysis. The definition of accuracy of pedicle screw was consistent across all the selected studies, namely the Gerztbein–Robbins Classification [16]. Roser et al. [24] did not perform statistical analysis on their preliminary results due to limited statistical power, although a trend towards increased pedicle screw accuracy in robot-assisted group was observed. Ringel et al. [23] for the first time compared the screw position accuracy between robot-assisted and conventional freehand technique using a randomized controlled design; however, they failed to report the method of random sequence generation and details about allocation concealment. Regardless of using Grade A or Grade A + B, the between-study heterogeneity was statistically significant, thus subgroup-analysis according to methodological quality was conducted. The combination of data from studies that reported adequate randomization and allocation concealment suggested that robot-assisted pedicle screw placement was superior to freehand technique when using Grade A (test for heterogeneity: P = 0.90, I 2 = 0%), but was similar to conventional freehand approach using Grade A + B (test for heterogeneity: P = 0.71, I 2 = 0%).
Pedicle screw position deviations up to 2 mm can be accepted by clinicians since minor deviations rarely injury vital vessels and nerves [26]. The included studies, with the exception of Ringel et al’s [23], had a higher accuracy of screw insertion in the robot-assisted group. The poorly positioned implants were partially attributed to the bed mount by Ringel et al. [23], but Roser et al. [24] did not encounter a similar inaccuracy with the same bed mount. When using grading A as the standard of accuracy, robot-assisted technique tends to overmatch freehand technique (RR 1.03, 95% CI 1.00, 1.06; P = 0.04). While using Grade A + B, robot-assisted technique is not superior to freehand technique (RR 1.01, 95% CI 0.99, 1.02; P = 0.29). The explanations could be summarized as below: first, spine surgeon relies upon a steady hand and meticulous skills during surgery. The surgical procedures are tedious and laborious, predisposing the surgeon to both physical and mental exhaustion, which may decrease the accuracy [27]. But robots are capable of performing the repetitive tasks and holding tools for long periods with accuracy and precision devoid of the limitations of human manual errors [28]. Besides, a preoperative CT scan of the surgical region is beneficial to select optimal screw size and plan an ideal entry position and trajectory. The robot-assisted system guides the surgeon to the desired position but leaves the actual execution of the surgical procedure in the surgeon’s hands, which also help the surgeon improve accuracy. What is more, the robot-assisted setting fixed firmly to the spine, monitoring and coordinating with the patient’s movements, reinforces its reliability. Last but not the least, the solid floor-flexible base and firm robotized arm of the robot device could help reduce the risk of secondary motion, thus guaranteeing the dependability of the entry point and trajectory [29]. Less than 2 mm deviation can be achieved by well-trained and experienced surgeons, but the 0 mm deviation which needs more accurate and precise movements enable the robot-assisted system to perform better than their human counterparts.
Reducing radiation exposure is especially important because large doses of radiation can contribute to an increasing risk of delayed effects such as malignancy [30, 31]. Ringel et al. [23] reported that total intraoperative radiation in freehand group was similar to robot-assisted group but freehand group required an additional radiation exposure for planning. Roser et al. [24] found the radiation in freehand group is nearly two times than robot-assisted group. Hyun et al.’s study [20] showed fluoroscopy time for per screw in freehand group was almost four times than the robot-assisted group. A latest study led by Alaid et al. also indicated a significant reduction of radiation exposure using robotic guidance for the treatment of pyogenic spondylodiscitis with pedicle screw fixation [32]. One valuable advantage of robot-assisted system is to lessen reliance on intraoperative fluoroscopy. With robot-assisted technique, simply anterior–posterior and lateral fluoroscopy images are necessary for image matching between patient and robot. C-arm can be taken away after registration, surgeons insert the screws along previously planned trajectories [33], thus limiting additional radiation exposure. Besides, robot-guided procedures require significantly shorter imaging sessions, exposing the patients and staffs to less radiation. Keric et al. reported that surgeons with more experience in conventional spinal instrumentation procedures might suffer less radiation exposure using the same robot-assisted technique [34].
Shah et al. initially reported the incidence of proximal facet joint violation, which might accelerate the occurrence of adjacent segment degeneration [35], was more than 30% of involved patients [36]. Factors including body mass index (BMI), age, type of pedicle screw and fusion procedure, number of fused segments may contribute to proximal facet joint violation [37]. A latest study led by Levin et al. reported that through no obvious impact on reoperation rate or post-operative quality of life at 1-year follow-up, the reoperation rate was considerably higher in the proximal facet joint violation patients compared with non-PFJV subjects at 2- and 3-year follow-up [38]. Among the included studies, Hyun et al. and Kim et al. mentioned proximal facet joint violation, the pooled data indicated that robot-assisted technique allowed surgeons to reduce proximal facet joint violation. Freehand technique largely relies on intraoperative C-arm fluoroscopy images for screw insertion, requiring the surgeon’s own judgment to harmonize the trajectory in three dimensions, while the robot-assisted system guides the surgeon to the preoperatively planned trajectory directly. By selecting optimal screw trajectory on the planning scheme, it was possible to keep screws away from the facets. The robot-assisted system implements the plan precisely during the operation, regardless of the surgeon’s proficiency [22].
Hyun et al. [20] reported the overall surgical time had no difference in robot-assisted and freehand group. But Ringel et al. [23], Tian et al. [25] and Kim et al. [22] reported a longer surgical time in robot-assisted group. The robot-assisted technique is in its early stage of clinical application. And a new technique always involves a learning curve before reaching to a proficient and steady state. The increase in surgical time can be partly attributed to the learning curve. Besides, the intraoperative preparation phase may also contribute to the longer surgical time with robot-assisted technique.
Several limitations to our study should be taken into account. First, although Begg’s test and Egger’s test indicated no significant publication bias in the accuracy of pedicle screw placement, the number of included studies was still limited, additional RCTs with larger sample size within different cultural contexts are needed. Second, as most studies used the Mazor robot, the findings of our present study may not represent the surgical robots as a whole. Additionally, all of our included studies restricted their participants to patients undergoing lumbar pedicle screw placement, considering the anatomical differences between the lumbar and thoracic vertebrae, whether or not robot-assisted technique is superior to conventional freehand remains to be addressed by future studies. Despite these aforementioned limitations, our present meta-analysis represents the highest level of evidence.
Conclusion
Taken together, the findings of the present meta-analysis suggested that robot-assisted pedicle screw implantation was as accurate as conventional freehand techniques, robot-assisted approach was associated with fewer proximal facet joint violation, less intraoperative radiation exposure but longer surgical duration than freehand technique. Although robotics in spinal surgeries holds promise for future spinal instrumentation, the effectiveness of robotics has been researched less than might be anticipated. To validate the beneficial role of robotics in spinal surgery, more RCTs with rigorous design and larger sample size are encouraged.
References
Gaines RW Jr (2000) The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. J bone Jt Surg Am 82-A:1458–1476
Panjabi MM, Goel V, Oxland T, Takata K, Duranceau J, Krag M, Price M (1992) Human lumbar vertebrae. Quantitative three-dimensional anatomy. Spine 17:299–306
Panjabi MM, Takata K, Goel V, Federico D, Oxland T, Duranceau J, Krag M (1991) Thoracic human vertebrae. Quantitative three-dimensional anatomy. Spine 16:888–901
Tan SH, Teo EC, Chua HC (2004) Quantitative three-dimensional anatomy of cervical, thoracic and lumbar vertebrae of Chinese Singaporeans. Eur Spine J 13:137–146. https://doi.org/10.1007/s00586-003-0586-z
Panjabi MM, Duranceau J, Goel V, Oxland T, Takata K (1991) Cervical human vertebrae. Quantitative three-dimensional anatomy of the middle and lower regions. Spine 16:861–869
Mason A, Paulsen R, Babuska JM, Rajpal S, Burneikiene S, Nelson EL, Villavicencio AT (2014) The accuracy of pedicle screw placement using intraoperative image guidance systems. J Neurosur Spine 20:196–203. https://doi.org/10.3171/2013.11.spine13413
Nolte LP, Visarius H, Arm E, Langlotz F, Schwarzenbach O, Zamorano L (1995) Computer-aided fixation of spinal implants. J Image Guid Surg 1:88–93. doi:10.1002/(SICI)1522-712X(1995)1:2<88::AID-IGS3>3.0.CO;2-H
Tjardes T, Shafizadeh S, Rixen D, Paffrath T, Bouillon B, Steinhausen ES, Baethis H (2010) Image-guided spine surgery: state of the art and future directions. Eur Spine J 19:25–45. https://doi.org/10.1007/s00586-009-1091-9
Verma R, Krishan S, Haendlmayer K, Mohsen A (2010) Functional outcome of computer-assisted spinal pedicle screw placement: a systematic review and meta-analysis of 23 studies including 5,992 pedicle screws. Eur Spine J 19:370–375. https://doi.org/10.1007/s00586-009-1258-4
Barzilay Y, Liebergall M, Fridlander A, Knoller N (2006) Miniature robotic guidance for spine surgery–introduction of a novel system and analysis of challenges encountered during the clinical development phase at two spine centres. Int J Med Robot Comput Assist Surg MRCAS 2:146–153. https://doi.org/10.1002/rcs.90
Lieberman IH, Togawa D, Kayanja MM, Reinhardt MK, Friedlander A, Knoller N, Benzel EC (2006) Bone-mounted miniature robotic guidance for pedicle screw and translaminar facet screw placement: Part I-Technical development and a test case result. Neurosurgery 59:641–650. https://doi.org/10.1227/01.neu.0000229055.00829.5b (discussion 641–650)
Lieberman IH, Hardenbrook MA, Wang JC, Guyer RD (2012) Assessment of pedicle screw placement accuracy, procedure time, and radiation exposure using a miniature robotic guidance system. J Spinal Disord Tech 25:241–248. https://doi.org/10.1097/BSD.0b013e318218a5ef
Liu H, Chen W, Wang Z, Lin J, Meng B, Yang H (2016) Comparison of the accuracy between robot-assisted and conventional freehand pedicle screw placement: a systematic review and meta-analysis. Int J Comput Assist Radiol Surg 11:2273–2281. https://doi.org/10.1007/s11548-016-1448-6
Marcus HJ, Cundy TP, Nandi D, Yang GZ, Darzi A (2014) Robot-assisted and fluoroscopy-guided pedicle screw placement: a systematic review. Eur Spine J 23:291–297. https://doi.org/10.1007/s00586-013-2879-1
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Gertzbein SD, Robbins SE (1990) Accuracy of pedicular screw placement in vivo. Spine 15:11–14
Rampersaud YR, Simon DA, Foley KT (2001) Accuracy requirements for image-guided spinal pedicle screw placement. Spine 26:352–359
Cahill KS, Wang MY (2012) Evaluating the accuracy of robotic assistance in spine surgery. Neurosurgery 71:N20–N21
Kim HJ, Kang KT, Park SC, Kwon OH, Son J, Chang BS, Lee CK, Yeom JS, Lenke LG (2017) Biomechanical advantages of robot-assisted pedicle screw fixation in posterior lumbar interbody fusion compared with freehand technique in a prospective randomized controlled trial-perspective for patient-specific finite element analysis. Spine J 17:671–680. https://doi.org/10.1016/j.spinee.2016.11.010
Hyun SJ, Kim KJ, Jahng TA, Kim HJ (2017) Minimally invasive robotic versus open fluoroscopicguided spinal instrumented fusions: a randomized controlled trial. Spine 42(6):353–358. doi:10.1097/BRS.0000000000001778
Kim HJ, Lee SH, Chang BS, Lee CK, Lim TO, Hoo LP, Yi JM, Yeom JS (2015) Monitoring the quality of robot-assisted pedicle screw fixation in the lumbar spine by using a cumulative summation test. Spine 40(2):87–94. doi:10.1097/BRS.0000000000000680
Kim HJ, Jung WI, Chang BS, Lee CK, Kang KT, Yeom JS (2016) A prospective, randomized, controlled trial of robot-assisted vs freehand pedicle screw fixation in spine surgery. Int J Med Robot Comput Assist Surg MRCAS. https://doi.org/10.1002/rcs.1779
Ringel F, Stuer C, Reinke A, Preuss A, Behr M, Auer F, Stoffel M, Meyer B (2012) Accuracy of robot-assisted placement of lumbar and sacral pedicle screws: a prospective randomized comparison to conventional freehand screw implantation. Spine 37:E496–E501. https://doi.org/10.1097/BRS.0b013e31824b7767
Roser F, Tatagiba M, Maier G (2013) Spinal robotics: current applications and future perspectives. Neurosurgery 72(Suppl 1):12–18. https://doi.org/10.1227/NEU.0b013e318270d02c
Tian W, Fan MX, Han XG, Zhao JW, Liu YJ (2016) Pedicle screw insertion in spine: a randomized comparison study of robot-assisted surgery and fluoroscopy-guided techniques. J Clin Orthop Res 1:4–10. https://doi.org/10.3969/j.issn.2096-269X.2016.01.002
Macke JJ, Woo R, Varich L (2016) Accuracy of robot-assisted pedicle screw placement for adolescent idiopathic scoliosis in the pediatric population. J Robot Surg 10:145–150. https://doi.org/10.1007/s11701-016-0587-7
Overley SC, Cho SK, Mehta AI, Arnold PM (2017) Navigation and robotics in spinal surgery: where are we now? Neurosurgery 80:S86–S99. https://doi.org/10.1093/neuros/nyw077
Joseph JR, Smith BW, Liu X, Park P (2017) Current applications of robotics in spine surgery: a systematic review of the literature. Neurosurg Focus 42:E2. https://doi.org/10.3171/2017.2.focus16544
Lonjon N, Chan-Seng E, Costalat V, Bonnafoux B, Vassal M, Boetto J (2016) Robot-assisted spine surgery: feasibility study through a prospective case-matched analysis. Eur Spine J 25:947–955. https://doi.org/10.1007/s00586-015-3758-8
Perisinakis K, Damilakis J, Theocharopoulos N, Papadokostakis G, Hadjipavlou A, Gourtsoyiannis N (2004) Patient exposure and associated radiation risks from fluoroscopically guided vertebroplasty or kyphoplasty. Radiology 232:701–707. https://doi.org/10.1148/radiol.2323031412
Mastrangelo G, Fedeli U, Fadda E, Giovanazzi A, Scoizzato L, Saia B (2005) Increased cancer risk among surgeons in an orthopaedic hospital. Occup Med (Oxf, Engl) 55:498–500. https://doi.org/10.1093/occmed/kqi048
Alaid A, von Eckardstein K, Smoll NR, Solomiichuk V, Rohde V, Martinez R, Schatlo B (2017) Robot guidance for percutaneous minimally invasive placement of pedicle screws for pyogenic spondylodiscitis is associated with lower rates of wound breakdown compared to conventional fluoroscopy-guided instrumentation. Neurosurg Rev. https://doi.org/10.1007/s10143-017-0877-1
Barzilay Y, Schroeder JE, Hiller N, Singer G, Hasharoni A, Safran O, Liebergall M, Itshayek E, Kaplan L (2014) Robot-assisted vertebral body augmentation: a radiation reduction tool. Spine 39:153–157. https://doi.org/10.1097/brs.0000000000000100
Keric N, Doenitz C, Haj A, Rachwal-Czyzewicz I, Renovanz M, Wesp DMA, Boor S, Conrad J, Brawanski A, Giese A, Kantelhardt SR (2017) Evaluation of robot-guided minimally invasive implantation of 2067 pedicle screws. Neurosurg Focus 42:E11. https://doi.org/10.3171/2017.2.focus16552
Kim HJ, Chun HJ, Kang KT, Moon SH, Kim HS, Park JO, Moon ES, Kim BR, Sohn JS, Ko YN, Lee HM (2012) The biomechanical effect of pedicle screws’ insertion angle and position on the superior adjacent segment in 1 segment lumbar fusion. Spine 37:1637–1644. https://doi.org/10.1097/BRS.0b013e31823f2115
Shah RR, Mohammed S, Saifuddin A, Taylor BA (2003) Radiologic evaluation of adjacent superior segment facet joint violation following transpedicular instrumentation of the lumbar spine. Spine 28:272–275. https://doi.org/10.1097/01.brs.0000042361.93572.74
Babu R, Park JG, Mehta AI, Shan T, Grossi PM, Brown CR, Richardson WJ, Isaacs RE, Bagley CA, Kuchibhatla M, Gottfried ON (2012) Comparison of superior-level facet joint violations during open and percutaneous pedicle screw placement. Neurosurgery 71:962–970. https://doi.org/10.1227/NEU.0b013e31826a88c8
Levin JM, Alentado VJ, Healy AT, Steinmetz MP, Benzel EC, Mroz TE (2017) Superior segment facet joint violation during instrumented lumbar fusion is associated with higher reoperation rates and diminished improvement in quality of life. Clin Spine Surg. https://doi.org/10.1097/bsd.0000000000000566
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Gao, S., Lv, Z. & Fang, H. Robot-assisted and conventional freehand pedicle screw placement: a systematic review and meta-analysis of randomized controlled trials. Eur Spine J 27, 921–930 (2018). https://doi.org/10.1007/s00586-017-5333-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-017-5333-y