
Abstract
Purpose
To identify predictors of both intermediate and long-term unfavorable outcomes after first time, uncomplicated lumbar disc surgery.
Methods
Patients (n = 120) who had undergone lumbar disc surgery were followed up 1.5 and 12 years thereafter. Baseline assessments were carried out 5–8 days after surgery. Clinical outcome was assessed in both follow-ups using the Low Back Pain Rating Scale. Statistical analysis included binary logistic and linear regression.
Results
Unfavorable outcomes were found in 50.5 % (1.5 years) and 52.6 % (12 years) of patients available for follow-up examination. Low pre-operative physical activity and severe pain in the first week after surgery were predictive of an unfavorable post-operative outcome at both follow-ups.
Conclusions
Identified predictors suggest that particular emphasis should put on comprehensive post-operative care at large and encouragement to adapt a physically active lifestyle in particular in rehabilitation concepts after first time uncomplicated lumbar disc surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
About 7400 and 342,000 lumbar discectomy surgeries are performed every year in Austria and in the US, respectively [1, 2]. Despite reported high success rates of this procedure of up to 90 %, there seems to be a considerable amount of patients who complain about pain and disability several months or even years after surgery [3, 4]. Loupasis et al. [5] reported unfavorable results in one-third of these patients seven to 20 years after lumbar discectomy.
If patients with an increased risk for an unsatisfying intermediate and long-term outcome after first time lumbar disc herniation surgery could be identified prior to the intervention or within the first post-operative week, early comprehensive pre- and post-operative management intended to improve overall back related health of these patients in the long-term could be provided. Items potentially modifiable by a multidisciplinary management approach seem of particular interest. In fact, compelling evidence suggests several socio-demographic, clinical, work-related, and psychological variables to be associated with less satisfying short- and intermediate-term outcomes after lumbar disc surgery [6]. However, so far only few studies have investigated predictors of an unfavorable outcome in the long-term [4, 7, 8]. Only one study seems to exist that has ever compared intermediate with long-term predictive factors for an inferior outcome after lumbar disc surgery [8]. Findings of this research suggested only one out of several prognostic factors to be predictive of an unfavorable intermediate and long-term outcome: time on sick leave. However, this study has several flaws e.g., inclusion of patients who suffered from chronic low back pain before disc surgery, a fact that per se seems to be associated with an inferior post-surgical outcome [9]. Other potentially relevant variables such as physical activity and/or improvement of symptoms immediately after surgery were not assessed.
This communication is reporting on the 12 years’ follow-up of a cohort of participants of an RCT, whose pre-operative complaints had lasted less than 3 months, and which were subjected to uncomplicated first time lumbar disc surgery with either discectomy or a microdiscectomy procedure. Particular focus has been put on the potential of a range of variables to predict an unfavorable outcome both 1.5 and 12 years after lumbar disc surgery. We were interested to see whether there are variables that could predict a poor outcome at both the intermediate and long-term.
Methods
Study design
The original, primary study was an RCT into the effectiveness of post-operative physiotherapy after first-time uncomplicated lumbar disc surgery [10]. Patients qualified for participation, if they presented with acute or subacute lumbar radicular symptoms, while spinal stenosis or spondylolisthesis, chronic pain disorders of the musculoskeletal system, defined neurological or psychiatric disorders were exclusion criteria. 120 patients had been randomly assigned after lumbar disc surgery (discectomy or microdiscectomy without a segmental fusion) to 12 weeks physiotherapy, “sham” neck massage, or no treatment and were evaluated before, 6, 12 weeks and 1.5 years after randomization. The study had taken place at the XXX, and had included a 1.5 years’ follow-up. Now a second follow-up should be performed overlooking a mean follow-up period of 12 years since surgical intervention. Formally, the design of this study is explorative in nature.
Both the original study and the actual follow-up study were approved by the Ethics Committee of the Medical University of XXX, and included patients had provided written informed consent for either study.
Assessment of potential predictors
Variables with an assumed predictive potential had first been assessed at the time of inclusion into the original study, 5–8 days after surgery. Overall, 28 potential predictors that had been assessed, and were sub-classified into anthropometric (weight, height, BMI), socio-demographic (gender, age, education, social status) work related (work status, pending retirement claim, and duration of pre-operative sick leave), clinical (“trauma”, pre-operative and post-operative paresis, pre-operative physical activity, pre-operative analgesic medication or use of physical therapy, duration of pre-operative complaints, alcohol consumption, nicotine use), and psychological variables [perceived overall quality of life (VAS 0-10), Spielberger State-Trait Anxiety Inventory [11] and the Giessen-Test (GT) [12]].
The STAI, which measures adult trait and state anxiety [11], encompasses two sub-scales each comprising of 20 items. One sub-scale describes the general feeling concerning stable anxiety and the other one describes the transient anxiety at a given moment. Items are scored on a Likert scale from 1 to 4 (“not at all” to “very much”) with higher scores indicating more pronounced anxiety. High test–retest reliability and construct validity has been demonstrated [13]. The GT [12] describes a person’s self image and is based on models of psychoanalysis and social psychology. The GT covers six dimensions: Social Resonance, Pliancy, Control, Depressiveness, Reservedness, and Social Potency. The reliability was found to be satisfactory except for the scales “Control and Pliancy” [14].
Furthermore, the patients’ subjective satisfaction with the treatment outcome was rated on a four-point Likert scale (very satisfied, satisfied, dissatisfied and very dissatisfied).
Assessment of clinical outcome at follow-up
Clinical outcome was evaluated 12 years after baseline evaluation in the same way as in the 1.5 years’ follow-up, i.e., using the German version of the Low Back Pain Rating Scale (LBPRS) [15]. This assessment tool measures a patient’s back related health and ranges from 130 (worst) to 0 (best). It is composed of three sub-scales, i.e., pain (60–0), physical function (40–0), and disability (30–0). High within and between reliability and satisfactory construct validity has been demonstrated [15].
Statistical analyses
Main outcome variable “unfavorable outcome”: A score of higher than 19.5 points on the total LBPRS (primary outcome parameter) and one exceeding 4.5 points on the LBPRS disability sub-scale (secondary outcome parameter) were considered as “unfavorable outcome”. A total LBPRS score of 19.5 points corresponds to approximately 35 % of the original baseline mean. Binary logistic and linear regression using univariate and multivariate models were applied to examine the potential of variables to differentiate between patients with a satisfactory or unsatisfactory post-operative outcome 1.5 and 12 years after surgery. LBPRS total (sum score of the LBPRS) served as dependent variable for the linear regression analysis, and the dichotomous variable LBPRS >19.5/≤19.5 points for the logistic regression analysis. For the multivariate models multi-collinearity analyses were calculated to identify correlations between the independent variables. A correlation matrix of the predictor variables was plotted and variance inflation factors (VIF) were calculated. Furthermore, associations between the patients’ subjective satisfaction with the treatment result and the actual outcome as assessed by the LBPRS were calculated by contingency tables and Spearman´s correlation coefficients.
Results
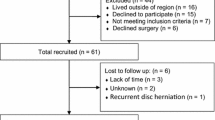
Ninety-nine and seventy-eight out of 120 patients who had originally been enrolled into the RCT could be included into the 1.5 and 12 years’ follow-up examinations. There was considerable overlap between those two cohorts, i.e., 70 of the 78 patients included in the 12 years’ follow up took also part in the 1.5 years’ follow-up. Among the 42 participants of the original study lost to the 12 years´ follow-up, contact addresses of 25 patients were unavailable, another three patients were deceased, and 14 patients denied participation in the actual examination.
Baseline values did not differ significantly between patients who completed the 1.5 years’ and the 12 years’ follow-up evaluations (Tab. 1). Results of the independent predictive variables in the first week after surgery and the results of the dependent variable LBPRS at baseline, 1.5 and 12 years´ follow-ups are presented in Tables 1, 2.
Outcomes classified as unfavorable were observed in 50 (50.5 %) and 41 (52.6 %) participants 1.5 and 12 years after surgery, respectively. In 45 patients the outcome (favorable or unfavorable) did not differ between the follow-ups. In 12 patients (12 %) an unfavorable outcome was present at the 1.5 years´ follow-up only and in another 12 patients (15 %) an unfavorable outcome was present at the 12 years´ follow-up only.
Of the 28 potentially predictive variables assessed, a total of eight were significant predictors at the 1.5 years´ follow-up, and another four variables at the 12 years´ follow-up. Significantly more likely to have an unfavorable outcome at respective follow-ups were:
-
At the 1.5-year follow-up, patients positive for (a) no physical exercise before surgery, (b) severe post-operative back pain, (c) extended pre-operative sick leave, (d) a pre-operative therapy with analgesics (alone or in combination with other conservative interventions), (e) a pending retirement claim, and (f) suffering from anxiety or depressive mood.
-
At the 12-year follow-up, patients with “no physical exercise before surgery”, “severe post-operative leg pain”, “low stature”, and “female gender”.
Thus “low pre-operative physical activity status” and “high pain intensity in the first week after the intervention” significantly predicted an unfavorable outcome both at 1.5 and 12 years after surgery (see Table 3).
There was a strong association between the patients’ satisfaction with their treatment outcome and their outcome on the LBPRS after 1.5 years (r = 0.668, p < 0.01). In contrast, no such association was observed at the 12-year follow-up (r = 0.228, p < 0.05).
Discussion
Findings from this study suggest that (1) variables with a significant predictive value for an unfavorable post-operative outcome at 1.5 years were not consistent with those at 12 years, and (2) patients with lumbar disc herniation syndrome who had reported to exercise regularly before surgery or who had reported lower pain levels in the first week after surgery, revealed a better back related health outcome at both the 1.5 and 12-year follow-up examinations.
In our sample the rate of unfavorable outcome 1.5 years (50.5 %) and 12 years after surgery (52.6 %) was higher than previously reported (Woertgen et al. 30 % [16], Atlas et al. 31 % [4], Loupasis et al. 36 % [5]), which may, for instance, relate to differences in the classification criteria of an unfavorable outcome or the assessment instruments used [4, 5, 8, 16]. Independent of the differences in the cut-off points defined for classifying an outcome as unfavorable, predictive variables were similar between all three studies, and also well matching with those identified in this research.
Of the apparent predictors at our 1.5 years´ follow-up, extended pre-operative sick leave and pending retirement claims, are well comparable with findings from previous studies [6, 8, 17–19], while less is known about our potential predictor anxiety. One might speculate that after surgery anxiety may negatively interfere with patients’ expectations and motivation, thereby facilitating depression and inhibiting full post-operative recovery from symptoms and complaints, thus interfering with the capacity of regaining optimum functioning in the intermediate and long-term. In fact, anxiety has elsewhere been identified as an important intermediate predictor of unfavorable post-operative outcomes [6]. Consistent with findings from previous research, depression was found to be a predictor for unfavorable outcome in this study, too [20]. In young patients, low pre-operative mental health state was found to be associated with low subjective satisfaction 1 year after lumbar disc surgery [21]. Also, pre-operative treatment with analgesics and/or physical therapy seemed to be related to a negative post-operative outcome 1.5 years after surgery, well in line with Hebert et al. [22], who reported an association between pre-operative physical and injection therapy and impaired improvement in leg pain intensity 10 weeks after lumbar disc surgery. In a recent review by Koerner et al. [23], prior injections and depression emerged as important patient-related outcome variables in patients included in the Spine Patient Outcomes Research Trial (SPORT). One might be tempted to speculate that either (unsuccessful) pre-operative physical therapy may affect post-surgical outcome or that pre-operative physical therapy may be an indicator for a pronounced problem. Interestingly, the objective outcome parameter for evaluation of back health (LBPRS) correlated well with subjective ratings of the patients concerning their satisfaction with the treatment outcome at the 1.5 years´ follow-up, which may be indicative of good external validity of our set of objective assessment instruments.
In the 12-year follow-up, female gender and short stature were found to be predictive of an unfavorable long-term outcome. Whereas findings of most studies seem to be in line with our findings and suggest female gender as predictive of an unfavorable outcome in the intermediate [24, 25] or long-term [5] after disc herniation surgery [6], there is at least one study [26] that found a significant association between male sex and poor outcome 1 year after lumbar disc surgery. Elsewhere short stature was identified as a predictor for a poor clinical intermediate-term outcome [24]. Patients’ estimates of the post-operative success assessed 12 years after disc surgery was found not to be related with the simultaneous objective outcome assessment. One is tempted to speculate that this might be a consequence of patients having simply neglected/superseded either their primary health problems that led to acute back surgery and/or the surgical event itself, and/or that the objective results may predominantly reflect the natural history of the underlying degenerative process. This assumption also reflects the fact that the identified long-term predictors are similar to established predictors for the development of back problems in general.
Concerning the natural history of lumbar disc herniation it should be mentioned that regressions of 30 % of lumbar disc protrusions and 77 % of extrusions and sequestrations were reported by Chiu et al. [27]. Irrespective of the fact that a high percentage of herniated discs may subside with time without surgery [26], the patients included in our previous study and respective follow-ups suffered form an acute disc syndrome with severe neurologic findings that required surgical relief.
One might speculate that post-operative degeneration and instability of the herniated disc might have affected our intermediate and long-term outcomes. A recent study by our group found indeed the risk of instability and degeneration to be increased, however, not related to the patients’ outcome [27]. The surgical procedures for the treatment of disc herniation used in this study, like microdiscectomy, open sequestrectomy and open discectomy, are currently recommended by spine societies internationally. Notably, no differences in clinical outcome and re-operation rates seem to exist between these techniques [28, 29]. Thus, the choice of the surgical procedures considered in our study may not have biased our results to a relevant extent.
Variables with predictive potential at both follow-up evaluations (i.e., after 1.5 and 12 years) were regular physical activity before surgery, and severe post-operative pain emphasizing their importance. To our knowledge, this is the first study that investigated the impact of patients´ physical activity level before surgery on long-term post-operative outcome after lumbar disc herniation. Jansson et al. [30] reported a short pre-operative walking distance as predictor for poor outcome 1 year after lumbar disc surgery. Patients reporting low levels of physical activity had a 3–7 times higher risk for unfavorable treatment results. This is in line with a study dealing with pre-operative physical fitness and outcome after abdominal surgery [31]. Our findings reflect the importance of regular muscular exercise for spine stabilisation, movement and back health. This statement is supported by findings of Rantanen et al. [32], who described a correlation between pathological changes in patients´ multifidus muscles and the clinical outcome 5 years after lumbar disc surgery, and who recommended adequate surgical and physiotherapeutic treatment. Regular exercise is thought to optimize or maintain optimum neuromuscular functions important for spine stabilization and safe spine movements, to increase pain perception thresholds, to promote subjective well-being and to optimize cardiopulmonary capability, probably via adaptations to exercise inside and outside of the muscle [33, 34]. The concept associated with the predictive value of post-operative pain during the first few days clearly differs from previously published research where high pre-operative pain intensity was identified as a short- and intermediate-term predictor of an unfavorable outcome after disc surgery [6, 21]. Remarkably, Peters et al. also found an association between long-term unfavorable outcome and a high level of acute post-operative pain 4 days after different elective surgeries [35].
Two aspects in particular may have a positive impact on the reliability of the reported findings. First, this research builds on data of an RCT which had only included patients with a history of painful symptoms of less than 3 months before surgery (average duration 6 weeks), acknowledging evidence of the duration of complaints prior to surgery as a predictor for unfavorable outcomes [6] and a duration of leg pain less than 6 months as a predictive factor for sought results [8]. Second, the use of a comprehensive outcome parameter (LBPRS) comprising of evaluations of pain, disability and physical function made it possible to deal with one core variable for back health.
Clearly, this research has several limitations. The limited sample size has to be mentioned, even though, at the 1.5 and 12 years follow-up, data were available from 81 %, respectively, 65 % of all patients originally included into the RCT, which compares with the proportions of patients available for a follow-up in other studies (Loupasis 77 % [5], Kerr 63 % [7], Silverplats 81 % [8]).
This research identified predictive factors that were similar to previously reported ones. Moreover, assessment of back health was performed after surgery. We had considered evaluating return to work, but eventually excluded this variable, since factors other than the ones evaluated may also relevantly influence return to work (as, for instance, expectations and pressure at work as well as the social and economic impact of the respective country). Blood tests may also help identify individuals with an increased risk of unfavorable outcome. This may be true for plasminogen activator inhibitor 1 (PAI-1) [36] and/or other markers of inflammation, fibrinolysis, and genetic biomarkers, respectively, but their relevance will have to be validated in the future. In a recent observational study, elective vs non-elective surgery was not predictive of satisfaction with post-operative outcome 2 years after surgery [37]. For studies with an extensive set of data, innovative statistical procedures like the Fuzzy Logic-based fuzzy inference system [38] might be an option, for follow-up periods of about 6 months.
We conclude that low physical activity levels and perception of severe pain in the first week after surgery may negatively impact intermediate and long-term outcomes after lumbar disc surgery. For these patients, multidisciplinary rehabilitation programs including optimized pain management immediately after surgery, psychological treatment and intensive exercise as well as regular encouragement to adopt a physically active lifestyle before surgery should be provided.
References
Gesundheit Bf (2012) http://www.kaz.bmg.gv.at/fileadmin/user_upload/Leistungen/2_T_Leistungen.pdf. Accessed 21 Aug 2015
Survey NNHD (2010) http://www.cdc.gov/nchs/data/nhds/4procedures/2010pro4_numberrate.pdf. Accessed 27 July 2012
Ebenbichler GR, Inschlag S, Pfluger V et al (2015) Twelve-year follow-up of a randomized controlled trial of comprehensive physiotherapy following disc herniation operation. Clin Rehabil 29:548–560
Atlas SJ, Keller RB, Wu YA et al (2005) Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the maine lumbar spine study. Spine (Phila Pa 1976) 30:927–935
Loupasis GA, Stamos K, Katonis PG et al (1999) Seven- to 20-year outcome of lumbar discectomy. Spine (Phila Pa 1976) 24:2313–2317
den Boer JJ, Oostendorp RA, Beems T et al (2006) A systematic review of bio-psychosocial risk factors for an unfavourable outcome after lumbar disc surgery. Eur Spine J 15:527–536
Kerr D, Zhao W, Lurie JD (2015) What are long-term predictors of outcomes for lumbar disc herniation? A randomized and observational study. Clin Orthop Relat Res 473:1920–1930
Silverplats K, Lind B, Zoega B et al (2010) Clinical factors of importance for outcome after lumbar disc herniation surgery: long-term follow-up. Eur Spine J 19:1459–1467
Nygaard OP, Kloster R, Solberg T (2000) Duration of leg pain as a predictor of outcome after surgery for lumbar disc herniation: a prospective cohort study with 1-year follow up. J Neurosurg 92:131–134
Erdogmus CB, Resch KL, Sabitzer R et al (2007) Physiotherapy-based rehabilitation following disc herniation operation: results of a randomized clinical trial. Spine (Phila Pa 1976) 32:2041–2049
Spielberger CD (2010) State-trait anxiety inventory. In: Corsini Encyclopedia of Psychology. Wiley
Beckmann D, Brähler E, Richter H (1991) Der Gießen-Test (GT)(4., erweiterte und überarbeitete Aufl. mit Neustandardisierung). Huber, Bern
Mondolo F, Jahanshahi M, Grana A et al (2007) Evaluation of anxiety in Parkinson’s disease with some commonly used rating scales. Neurol Sci 28:270–275
Gunzelmann T, Schumacher J, Brahler E (2002) Normal values of the Giessen Test for over 60-year-old probands. Z Gerontol Geriatr 35:13–20
Nuhr MJ, Crevenna R, Quittan M et al (2004) Cross-cultural adaption of the Manniche questionnaire for German-speaking low back pain patients. J Rehabil Med 36:267–272
Woertgen C, Holzschuh M, Rothoerl RD et al (1997) Does the choice of outcome scale influence prognostic factors for lumbar disc surgery? A prospective, consecutive study of 121 patients. Eur Spine J 6:173–180
Kitze K, Winkler D, Gunther L et al (2008) Preoperative predictors for the return to work of herniated disc patients. Zentralbl Neurochir 69:7–13
Mannion AF, Elfering A (2006) Predictors of surgical outcome and their assessment. Eur Spine J 15(Suppl 1):S93–S108
Junge A, Dvorak J, Ahrens S (1995) Predictors of bad and good outcomes of lumbar disc surgery. A prospective clinical study with recommendations for screening to avoid bad outcomes. Spine (Phila Pa 1976) 20:460–468
Chaichana KL, Mukherjee D, Adogwa O et al (2011) Correlation of preoperative depression and somatic perception scales with postoperative disability and quality of life after lumbar discectomy. J Neurosurg Spine 14:261–267
Strömqvist F, Strömqvist B, Jönsson B, Gerdhem P, Karlsson MK (2016) Predictive outcome factors in the young patient treated with lumbar disc herniation surgery. J Neurosurg Spine 20:1–8
Hebert JJ, Fritz JM, Koppenhaver SL et al (2016) Predictors of clinical outcome following lumbar disc surgery: the value of historical, physical examination, and muscle function variables. Eur Spine J 25:310–317
Koerner JD, Glaser J, Radcliff K (2015) Which variables are associated with patient-reported outcomes after discectomy? Review of SPORT disc herniation studies. Clin Orthop Relat Res 473:2000–2006
Graver V, Ljunggren AE, Loeb M et al (1998) Background variables (medical history, anthropometric and biological factors) in relation to the outcome of lumbar disc surgery. Scand J Rehabil Med 30:221–225
Donceel P, Du Bois M (1999) Predictors for work incapacity continuing after disc surgery. Scand J Work Environ Health 25:264–271
Haugen AJ, Brox JI, Grovle L et al (2012) Prognostic factors for non-success in patients with sciatica and disc herniation. BMC Musculoskelet Disord 13:183
Chiu CC, Chuang TY, Chang KH et al (2015) The probability of spontaneous regression of lumbar herniated disc: a systematic review. Clin Rehabil 29:184–195
Schmid SL, Wechsler C, Farshad M et al (2016) Surgery for lumbar disc herniation: analysis of 500 consecutive patients treated in an interdisciplinary spine centre. J Clin Neurosci 27:40–43
Azarhomayoun A, Chou R, Shirdel S et al (2015) Sequestrectomy versus conventional microdiscectomy for the treatment of a lumbar disc herniation: a systematic review. Spine (Phila Pa 1976) 40:E1330–E1339
Jansson KA, Nemeth G, Granath F et al (2005) Health-related quality of life in patients before and after surgery for a herniated lumbar disc. J Bone Joint Surg Br 87:959–964
Dronkers JJ, Chorus AM, van Meeteren NL et al (2013) The association of pre-operative physical fitness and physical activity with outcome after scheduled major abdominal surgery. Anaesthesia 68:67–73
Rantanen J, Hurme M, Falck B et al (1993) The lumbar multifidus muscle five years after surgery for a lumbar intervertebral disc herniation. Spine (Phila Pa 1976) 18:568–574
Ebenbichler GR, Oddsson LI, Kollmitzer J et al (2001) Sensory-motor control of the lower back: implications for rehabilitation. Med Sci Sports Exerc 33:1889–1898
Tucker KJ, Hodges PW (2010) Changes in motor unit recruitment strategy during pain alters force direction. Eur J Pain 14:932–938
Peters ML, Sommer M, de Rijke JM et al (2007) Somatic and psychologic predictors of long-term unfavorable outcome after surgical intervention. Ann Surg 245:487–494
Elkan P, Sten-Linder M, Hedlund R et al (2016) Markers of inflammation and fibrinolysis in relation to outcome after surgery for lumbar disc herniation. A prospective study on 177 patients. Eur Spine J 25:186–191
Elkan P, Sjovie Hasserius J, Gerdhem P (2016) Similar result after non-elective and elective surgery for lumbar disc herniation: an observational study based on the SweSpine register. Eur Spine J 25:1460–1466
Shamim, Enam SA, Qidwai U (2009) Fuzzy Logic in neurosurgery: predicting poor outcomes after lumbar disk surgery in 501 consecutive patients. Surg Neurol 72:565–572 (discussion 572)
Acknowledgments
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
This work was a master thesis by Nora Salomon MD. She published the results of this research in her master thesis, Vienna Medical University in 2015.
Rights and permissions
About this article

Cite this article
Pieber, K., Salomon, N., Inschlag, S. et al. Predictors of an unfavorable outcome 1.5 and 12 years after a first, uncomplicated lumbar disc surgery. Eur Spine J 25, 3520–3527 (2016). https://doi.org/10.1007/s00586-016-4700-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-016-4700-4