
Abstract
Introduction
Proximal junctional kyphosis (PJK) of the cervicothoracic spine is a deformity that can affect patients who have undergone long thoracolumbar instrumented fusion. Preoperative hyperkyphosis of the thoracic spine and changes of more than 30° in lumbar lordosis are independent risk factors for the onset of PJK.
Methods
When PJK occurs in the cervicothoracic spine, extension of the fusion with eventual application of osteotomy techniques is frequently necessary to treat symptomatic patients or in case a neurological deficit occurs. Ponte osteotomy and pedicle subtraction osteotomy (PSO) are the two most used techniques to restore a good cervicothoracic alignment, although they are still demanding procedures even for expert surgeons. In junctional fractures, a vertebral column resection can be performed to support the anterior column. Ponte osteotomy ideally restores 10° at each treated level, while PSO allows a segmental correction up to 30°–35°. Adequate preoperative planning is fundamental for outlining the correct surgery and choosing the appropriate osteotomy.
Conclusions
The aim of corrective surgery is to restore the cervicothoracic alignment, obtaining an adequate postoperative sagittal balance and decreasing the risk of further complications and new revision surgeries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Proximal junctional kyphosis (PJK) is a deformity that occurs in adults and adolescents after scoliosis and kyphosis surgery [1–4]. After a long thoracolumbar instrumented fusion, an increased junctional stress concentration overloads the upper instrumented vertebra (UIV) or the immediate cranial segment, producing a PJK in some patients [5, 6]. This can be due to disc degeneration and consequent kyphosis or to a fracture of the UIV or first noninstrumented vertebra. The prevalence of this phenomenon varies in the literature according to different studies, reaching values of 39 % at long-term follow-up after long spinal fusions in adult spinal deformity patients [7]. It has been demonstrated that preoperative hyperkyphosis of the thoracic spine and changes of more than 30° in lumbar lordosis are independent risk factors for the onset of PJK [8]. Other risk factors include increased age, fusion to the sacrum, UIV at T1–T3 and inadequate restoration of global spine alignment [9]. Surgery-related risk factors can be related to the disruption of the posterior tension band of the spine due to intraoperative lesions of the inter- and supraspinous ligament or to an excessive dissection of the paraspinal muscles during spinal exposure, especially in the region immediately cranial to the hardware implant.
In severe cases, PJK can lead to compromised outcomes and neurological impairment, requiring a revision surgery to correct the junctional deformity [10]. The aims of this kind of surgery are to reestablish a good sagittal balance and an adequate regional kyphosis. If neurological impairment occurs, a laminectomy is mandatory. Compression of the spinal cord can frequently happen when a fracture of the UIV or of the first cranial noninstrumented vertebra occurs. Cephalad extension of the instrumentation and vertebral osteotomies are frequently used techniques in this kind of pathology, even if corrective procedures performed at the cervicothoracic junction are complex even in the hands of expert surgeons. The major vascular elements and fundamental structures, such as the esophagus and trachea, located ventrally to the cervicothoracic junction, make an anterior approach to the spine difficult, while the small pedicle diameters and presence of the vertebral arteries raise the risk of complications performing a posterior approach. However, recent advances in anesthesiology and surgical techniques, combined with more efficient posterior hardware, have made the posterior techniques and approaches to the spine more feasible, although these procedures remain complex and demanding for both surgeons and patients.
Indications for surgery and preoperative evaluation
A cranial extension of the instrumented fusion associated with spinal osteotomies for cervicothoracic PJK is generally indicated in the following cases: UIV or first noninstrumented vertebral fracture; symptomatic PJK without response from conservative or medical treatment; progression of the deformity or instability; neurological impairment or cord compression with myelopathy. In all these cases, a correction of the junctional kyphosis is mandatory.
Appropriate preoperative planning must be performed in order to choose the proper surgery. All patient candidates for a corrective osteotomy of the cervicothoracic junction should undergo a complete preoperative radiological evaluation that includes full spine X-rays, CT scan and MRI. Full-standing X-rays are useful to determine the global sagittal alignment of the patient and to measure spinal and pelvic parameters. The choice between the types of osteotomies depends on the expected degrees of correction of the cervicothoracic junction. A preoperative CT scan is useful to evaluate eventual fusions of the anterior structures and to measure pedicle and lateral mass sizes. Finally, MRI is needed to evaluate the course of vertebral arteries and their correct entrance through the transverse foramen of the C6 vertebra. Neurological structures such as the cord and nerve roots are also evaluated on MRI. In the presence of myelopathy signs due to cord compression, a laminectomy is mandatory to remove any bony constriction.
The choice of osteotomy level is significant, especially when a pedicle subtraction osteotomy (PSO) is indicated. Osteotomies are performed in the region of the kyphosis or at the site of maximal deformity [11]. If a vertebral fracture is the cause of PJK, PSO has to be performed at this level. Usually C7 and T1 are the preferred levels to perform a PSO. This is because the local anatomy is favorable for an osteotomy since vertebral arteries remain anterior to the transverse processes and do not enter the transverse foramen until C6. Second, C8 roots are mobile and can be better manipulated, and any eventual unwanted damage of these nervous roots will be less harmful to hand function. Finally, the spinal canal at these levels is wider and reduces the risks of entrapment of the spinal cord during osteotomy closure.
Cervicothoracic osteotomies
The cervicothoracic region is a peculiar area of the spine since it represents the passage from an extremely flexible spine to a rigid and kyphotic one. It usually refers to the region between C6 to T4 [12].
Different osteotomies can be performed in the cervicothoracic spine to treat PJK. The choice among these techniques depends on the entity of the local kyphosis, level and type of PJK, and grades that should be restored in order to achieve an adequate sagittal alignment. This can prevent further complications, such as hardware loosening or rod breakage, with subsequent revision surgery (see Fig. 2a–e as an exemplary case).
The main osteotomies performed at the cervicothoracic junction are the Ponte osteotomy and PSO. While the first ideally corrects 10° per treated level, PSO is used to restore up to 30°–35° per treated level. More rarely, in severe PJKs with a cervicothoracic fracture, a vertebral column resection (VCR) of the fractured vertebral body is performed to restore correct alignment and give support to the anterior column.
All patients undergoing a corrective surgery with osteotomies for a cervicothoracic PJK must be controlled during the whole procedure with neuromonitoring. This technique allows observing the nervous conduction to the four limbs in order to notice any change during the surgical maneuvers and spine corrections immediately.
Ponte osteotomies and PSOs are performed with a posterior incision, with the patient lying prone on a Jackson table or on a Risser frame. Each technique has specific aspects and steps that should be followed in order to obtain the optimal correction and decrease the risk of neurological injury. Many surgeons prefer the use of halo or Mayfield traction during surgery to manipulate the head and avoid the compression of the face on pad supports. This can reduce the facial and periorbital edema. If intraoperative traction is preferred, the halo ring should be the first choice when the traction is supposed to continue in the postoperative period.
In the past, instead of a traditional prone position of the patients, some surgeons preferred a sitting position when performing cervicothoracic corrective osteotomies [13]. There are however some difficulties in the procedure when this position is used. Furthermore, when a halo ring is used to maintain traction, the operating field is reduced, limiting distal fixation procedures. Nowadays, thanks to anesthesiology and surgical improvements, the preferred position is with the patient lying prone on a Jackson table.
Ponte osteotomy
Ponte osteotomy is a V-shape osteotomy of the thoracic spine first described in 1984 [14]. It represents an osteotomy of the posterior column and can restore up to 10° per treated level. In the preoperative planning, an accurate evaluation of the anterior structures should be made. Ponte osteotomy works as a posterior closing-anterior opening osteotomy, with a distraction of the anterior structures (disc, ligaments) in order to obtain the desired correction. This is performed acting as a hinge on the posterior longitudinal ligament. A nonrigid kyphosis without anterior ankylosing is mandatory to obtain a correction with Ponte osteotomies. After making a posterior longitudinal incision, a subperiosteal dissection of the paraspinal muscles is performed, with exposition of the previously implanted hardware. The caps and rods of the preexisting hardware are then removed. Lateral mass screws are placed in the cervical vertebrae, and pedicle screws are used in the thoracic area. Sublaminar bands can also be used in this procedure in order to decrease the risk of complications related to screw placement (Fig. 1a–d). After hardware positioning, Ponte osteotomy can be performed. It consists of the removal of the inferior portion of the lamina with a V-shape. The two grooves are directed laterally and cranially to reach the articular facets. Once the osteotomy has been performed on a single or multiple levels (depending on the required correction), a gentle extension of the spine produces a closure of the posterior elements. Once a complete correction has been obtained, rods can be fixed to the screws to maintain the restoration of the correct spinal alignment.

a Preoperative lateral X-ray of a 66-year-old woman affected by PJK after a T3-pelvis fusion. b Intraoperative view after a Ponte osteotomy and sublaminar band implant. c Postoperative X-rays with a complete correction of the deformity. d Detail of the cervicothoracic junction
Pedicle subtraction osteotomy
Pedicle subtraction osteotomy is a powerful technique that allows 30°–35° correction per treated level. It is a three-column shortening osteotomy with a resulting cancellous bone-on-bone contact, thus promoting fusion. This technique is widely used in the treatment of lumbar kyphotic deformities, but can also be applied at the cervicothoracic junction in order to correct local kyphosis. With the patient in a prone position, a midline skin incision and dissection of the paraspinal muscles are performed. The exposure of the implanted hardware is followed by the removal of caps and bilateral rods. Lateral mass and pedicle screws are then implanted in the cervical and thoracic region, respectively. Since PSO is a three-column osteotomy and creates extreme instability at the treated level, in older osteoporotic patients a fusion cephalad at least up to C2 is recommended in order to obtain solid bicortical screw placement. In younger patients with a good bone quality, two levels cranial to the PSO are sufficient if good hardware fixation has been provided, preferably using pedicle screws (Fig. 2a–e). A complete laminectomy is performed at the level of the osteotomy, including the removal of the facet joints. A partial removal of the adjoining laminae and spinous processes is performed in order to obtain better visualization of the structures inside the canal and better closure after the osteotomy. An accurate foraminotomy of the upper and lower levels is then performed in order to visualize the four exiting roots. When the PSO is complete, these roots will exit from the spine through a large foramen created by the union of these two. At this point, bilateral transverse processes and the corresponding ribs are resected. After the isolation of the pedicles at the selected level, apposite rongeurs are used to flatten the pedicles and expose the cancellous bone. Taps of increasing size are then inserted in the vertebral body, creating two cavities that will progressively connect on the midline. Osteotomes and curettes are then used to enlarge the cavity and obtain a wedge shape. Homeostatic agents and collagen sponges are used to control bleeding, which can become very abundant and in some cases be life threatening. Lateral aspects of the vertebral body are then carefully exposed, and a rongeur or an osteotome is used to remove a triangular portion corresponding to the wedge cavity. An appropriate instrument is then inserted between the dural sac and the residual posterior wall that is removed. Particular attention must be given to ensure a symmetrical removal of bone during each step of the PSO in order to obtain correct closure of the osteotomy and avoid rotational or lateral malalignments. The PSO is now complete, and a gentle extension of the neck is needed to close the osteotomy, while any dural or root entrapment is observed and avoided. For this reason, a further posterior decompression could be necessary. Once the bony elements are in contact, two rods are placed and fixed with caps to the screws in order to maintain the correction.

a PJK in a 36-year-old male treated with a T2–L2 instrumented fusion for Scheuermann disease. The junctional kyphosis produced a fracture of T2 bilateral laminae and mobilization of the sublaminar bands. b Postoperative lateral X-ray: an extension of the instrumentation without osteotomies was performed cephalad to C7. c Failure of the hardware and new onset of PJK 4 months after revision surgery. d Second revision surgery with T3 PSO and T1 and T2 pedicle screw implant. No further complications occurred in a 1-year follow-up. e Detail of the cervicothoracic junction at the final control
Vertebral column resection (VCR)
Vertebral column resection consists of the removal of the vertebral body. It is usually performed using a posterior approach in the thoracic spine (posterior vertebral column resection, PVCR) and has a great potential in restoring lordosis with the implant of an expandable intersomatic cage. In rare cases, when an acute angular deformity occurs, an anterior approach can be the preferable option (Fig. 3a–f). A midline incision and subperiosteal paraspinal muscle dissection are performed. After the screw implant, temporary rods are placed bilaterally to maintain orientation and stabilize the spine. VCR is a very destructive technique that disrupts the continuity of the spine, causing potentially hazardous instability. This is why the positioning of two temporary rods is required during this procedure. At this point, bilateral transverse processes and the corresponding ribs are resected. With a costotransversectomy approach, inferior and superior facets and pedicles are removed on both sides, and the vertebral body is gradually removed with appropriate curettes and rongeurs once the discs are found. These are dissected and the endplates scraped from the cartilaginous layer. Finally, the posterior wall is removed with the impaction technique. Once the vertebral body removal is complete, an expandable cage is implanted. Autologous bone graft from the removed vertebral body is used to fill the cage. Definitive rods are then connected to the screws and fixed with caps.

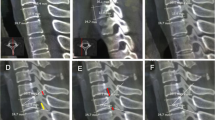
a Preoperative lateral X-ray of a 74-year-old man affected by Parkinson's disease and suffering from global kyphosis deformity according to the Lamartina-Berjano sagittal classification. b Immediate postoperative correction with a T2-pelvis fusion and L3 PSO. Postoperative spinopelvic values were the following: pelvic incidence = 60°, pelvic tilt = 12°, lumbar lordosis = 71° and thoracic kyphosis = 55°. c PJK with T1 fracture and angular kyphosis. On the left, lateral X-ray image; sagittal MRI on the right. d Skin lesion with hardware exposure. e Postoperative lateral X-ray with cranial extension to C6 and T1 anterior corpectomy. An expandable cage and plate were implanted using an anterior approach. A halo vest was worn for the first 3 postoperative months. f Clinical preoperative (left) and follow-up (right) pictures
All the previously described osteotomies are followed by autograft bone displacement on the decorticated spine in order to obtain solid fusion. Drains are placed, and the fascia, underskin layer and skin are sutured. The postoperative course includes the maintenance of a halo vest or a Minerva cervicothoracic brace for the first 3 months. While this last orthosis can be used in younger patients where a solid instrumentation has been obtained, a halo vest is required in older osteoporotic patients to obtain rigid spinal support.
When the fusion is extended cranially including the whole cervical spine, a slight flexion of the head is preferable. This still requires the patients to look straight, but also allows them to see things placed at a lower level, such as the floor when they are walking or a keyboard or a book located on a desk.
Personal casuistry
Twelve revision surgeries for PJK after thoracolumbar fusion were carried out in our division in the past years. Five patients (41.7 %) underwent primary corrective surgery for thoracic hyperkyphosis in Scheuermann’s disease, while seven (58.3 %) suffered from combined lumbar and thoracic kyphosis. According to the Lamartina and Berjano classification of sagittal deformities [15], these patients were classified into two groups, those with thoracic kyphosis (TK) and global kyphosis (GK), respectively. Patients in the TK group had a mean age of 29 years (range 18–40), with a preoperative thoracic kyphosis of 89° (range 78°–95°). The primary corrective surgery was extended to T2 in all cases and provided a reduction of thoracic kyphosis to 39° (range 33°–44°). When PJK occurred, an increase of mean thoracic kyphosis of 23° was observed (average 62°, range 58°–66°). No neurological deficits were observed. A revision surgery with a T3 PSO and restoration of thoracic kyphosis (mean 24°, range 20°–33°) was performed in all the cases. At an average 3-year follow-up (range 1–6 years), no complications or PJK recurrence were observed.
Considering the seven patients in the GK group, the mean age was 67 years (range 55–80), with a preoperative global kyphosis (T1–S1) of 85° (range 78°–95°). After the first corrective surgery more than 35° of lumbar lordosis was restored in each case, while the postoperative thoracic kyphosis had a mean value of 49° (range 39°–52°). The UIV was T2 in all cases. When PJK occurred, thoracic kyphosis increased to a mean value of 58° (range 55°–60°). In this group we observed two cases of myelopathy (28.6 %) due to spinal cord compression. Three patients were revised with a T3 PSO, while four patients underwent Ponte osteotomies, with a decrease of thoracic kyphosis to a value of 36° (range 30°–40°). At a mean 1.9-year follow-up (range 1–3 years), no complications or PJK recurrence was observed. One complete and one partial recovery of the two neurological deficits were observed.
The overall mean time of revision surgery was 240 min, with an average blood loss of 1,600 ml. In our patients, one implant failure and one skin lesion (Fig. 3d) were observed.
Conclusions
Proximal junctional kyphosis after long thoracolumbar instrumented fusion is a deformity that occurs in adults who have undergone deformity corrective procedures. Cephalad extension of the fusion with the application of osteotomy techniques is frequently necessary to treat symptomatic patients or in case a neurological deficit occurs. Ponte osteotomy and PSO are the two most used techniques to restore good cervicothoracic alignment, even though they are still demanding procedures even for expert surgeons. However, current advances in intraoperative monitoring systems, implants for posterior fusion and surgical techniques help the surgeon in performing these procedures. Ponte osteotomy allows the restoration of 10° at each treated level, while PSO provides local correction up to 30°–35°. Adequate preoperative planning is fundamental to outline the correct surgery and choose the appropriate osteotomy. The aim of this surgery is to restore the cervicothoracic alignment, obtaining improvement of the T1 slope and adequate postoperative sagittal balance and decreasing the risk of further complications and new revision surgeries.
References
Arlet V, Aebi M (2013) Junctional spinal disorders in operated adult spinal deformities: present understanding and future perspectives. Eur Spine J 22(Suppl 2):S276–S295
Denis F, Sun EC, Winter RB (2009) Incidence and risk factors for proximal and distal junctional kyphosis following surgical treatment for Scheuermann kyphosis: minimum five-year follow-up. Spine Phila Pa (1976) 34:E729–E734
DeWald CJ, Stanley T (2006) Instrumentation-related complications of multilevel fusions for adult spinal deformity patients over age 65: surgical considerations and treatment options in patients with poor bone quality. Spine Phila Pa (1976) 31:S144–S151
Hart RA, Prendergast MA, Roberts WG et al (2008) Proximal junctional acute collapse cranial to multi-level lumbar fusion: a cost analysis of prophylactic vertebral augmentation. Spine J 8:875–881
Hollenbeck SM, Glattes RC, Asher MA et al (2008) The prevalence of increased proximal junctional flexion following posterior instrumentation and arthrodesis for adolescent idiopathic scoliosis. Spine Phila Pa (1976) 33:1675–1681
Watanabe K, Lenke LG, Bridwell KH et al (2010) Proximal junctional vertebral fracture in adults after spinal deformity surgery using pedicle screw constructs: analysis of morphological features. Spine Phila Pa (1976) 35:138–145
Kim YJ, Bridwell KH, Lenke LG et al (2008) Proximal junctional kyphosis in adult spinal deformity after segmental posterior spinal instrumentation and fusion: minimum five-year follow-up. Spine Phila Pa (1976) 33:2179–2184
Maruo K, Ha Y, Inoue S et al (2013) Predictive factors for proximal junctional kyphosis in long fusions to the sacrum in adult spinal deformity. Spine Phila Pa (1976) 38(23):E1469–E1476
Kim HJ, Lenke LG, Shaffrey CI et al (2012) Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery. Spine Phila Pa (1976) 37(22S):S144–S164
Glattes RC, Bridwell KH, Lenke LG et al (2005) Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: incidence, outcomes, and risk factor analysis. Spine Phila Pa (1976) 30:1643–1649
Wang MY, Berven SH (2007) Lumbar pedicle subtraction osteotomy. Neurosurgery 60(2 Suppl 1):ONS140–ONS146
Boyle JJ, Milne N, Singer KP (2002) Influence of age on cervicothoracic spinal curvature: an ex vivo radiographic survey. Clin Biomech (Bristol, Avon) 17:361–367
Simmons EH (1972) The surgical correction of flexion deformity of the cervical spine in ankylosing spondylitis. Clin Orthop 86:132–143
Ponte A, Vero B, Siccardi GL (1984) Surgical treatment of Scheuermann’s hyperkyphosis. In: Winter RB (ed) Kyphosis (progress in spinal pathology). Aulo Gaggi, Bologna, pp 75–80
Lamartina C, Berjano P (2014) Classification of sagittal imbalance based on spinal alignment and compensatory mechanisms. Eur Spine J 23:1177–1189
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cecchinato, R., Berjano, P., Bassani, R. et al. Osteotomies in proximal junctional kyphosis in the cervicothoracic area. Eur Spine J 24 (Suppl 1), 31–37 (2015). https://doi.org/10.1007/s00586-014-3654-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-014-3654-7