
Abstract
Some studies have demonstrated that physiotherapists have a high prevalence of low back pain (LBP). The association between physiotherapy students, who are potentially exposed to the same LBP occupational risks as graduates, and LBP has never been demonstrated. The objective of the study is to evaluate the association between undergraduate physiotherapy study and LBP. The study design includes a cross-sectional study. A questionnaire-based study was carried out with physiotherapy and medical students. LBP was measured as lifetime, 1-year and point prevalence. Bivariate and multivariate analyses were performed to find the factors associated with LBP. Bivariate analyses were also performed to assess differences between LBP characteristics in the two courses. 77.9% of the students had LBP at some point in their lives, 66.8% in the last year and 14.4% of them reported they were suffering from LBP at the moment of answering the questionnaire. Physiotherapy students reported a higher prevalence of LBP when compared with the medical students in all measures. In the logistic regression model, physiotherapy students (A-OR 2.51; 95% CI 1.35–4.67; p = 0.003), and being exposed to the undergraduate study for more than four semesters (A-OR 2.55; 95% CI 1.43–4.55; p = 0.001) were independently associated with LBP. There were no differences between the courses concerning pain intensity and disability. As it was a cross-sectional study, we were not able to observe accurately if there is an increasing incidence of LBP during the course. Also, we did not intend to identify which activities in the course were associated with the development of LBP. This study clearly demonstrated an association between undergraduate physiotherapy study and LBP. The length of course exposure is also associated with LBP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Low back pain (LBP) is the leading cause of disability and inability to work, and expected to affect up to 90% of people at some point in their lives [1]. Many studies have attempted to identify and evaluate the contribution of different demographic, physical, socioeconomic, psychological, and occupational factors to the development of spinal pain. It is interesting that 37% of LBP worldwide are attributable to occupational risk factors, which represent many potentially preventable sources of pain [2].
Some studies have demonstrated that physiotherapists have a high prevalence of LBP [3–7]. The activities of these professionals are related to the development of this pain [3, 4, 7]. It is estimated that up to 60% of LBP events in this group occur as a consequence of work-related injuries [3–7]. Many physiotherapists report the onset of LBP during undergraduate course [7]. In fact, physiotherapy students are potentially exposed to the same LBP occupational risks as graduates, such as poor working postures and frequent manual handling activities, often undertaken in difficult environments and with variable training regarding personal safety.
In order to evaluate the association between undergraduate physiotherapy study and LBP, we developed a prevalence study with physiotherapy and medical students, analyzing the possible confounding factors in a logistic regression model. We also aimed to verify if LBP is more severe and disabling in physiotherapy students.
Method
Design and sample
This cross-sectional study was carried out at the University of Caxias do Sul, a private university in the state of Rio Grande do Sul, Brazil. A self-administered questionnaire was completed by medical and physiotherapy students. The students were invited to become involved in the study during their classes. All classes of both courses were visited by the researchers during the data collection period. After accepting to participate in the study and signing the letter of consent they completed the questionnaire, which took approximately 20 min.
The study was submitted to the Ethics and Research Committee of the University of Caxias do Sul and began after approval (n. 074/08) and no funds were received in support of this work.
Instrument
With the structured questionnaire, the following variables were collected: gender, age, program, length of study (in numbers of semesters), height, weight, tobacco use, physical activity, depressive symptoms, presence of LBP and its features. The students were asked about their height and weight; the body mass index (BMI) was calculated with these two variables.
The Beck Depression Inventory was used to evaluate the presence and severity of depressive symptoms among the students. This instrument consists of 21 questions, each question scores 0–3 with a total scoring from 0 to 63. It considers depression if the total score is >14, which has a 93% true-positive rate and 18% false-positive rate [8].
The International Physical Activity Questionnaire (IPAq) was used to classify the level of physical activity. This instrument was developed by the World Health Organization and it is frequently used worldwide. Its advantage is that IPAq evaluates physical activity in many aspects of the daily routine rather than only in one isolated aspect (i.e. leisure time). The IPAq evaluates the daily activity in four dimensions: professional, domestic, during transportation and leisure. Therefore, we were able to classify the physical activity as low, moderate or high [9, 10].
The students were asked if they have ever suffered LBP at some point of their lives (lifetime prevalence), if they suffered LBP in the last year (1-year prevalence), and if they were suffering LBP at the moment they were fulfilling the questionnaire (point prevalence). LBP was defined as pain in the area from below the ribs to the hips [11, 12]. People who had presented LBP in the last year were asked about duration of the pain, and it was classified as acute, if less than 3 weeks; sub acute, from 3 weeks to 3 months; and chronic, if >3 months [12]. It was also asked if the pain irradiated to the lower limbs (sciatica) or stayed only in the lumbar region [12].
Pain intensity was assessed by the numerical rating scale, ranging from zero (no pain) to ten (worst pain) [12]. Medication use and seeking care due to LBP were also assessed with the questionnaire. Disability was verified by four questions of the Oswestry Disability Index (ODI), i.e., lifting, walking, sitting and standing [13, 14].
Statistical analysis
All statistical analyses were conducted with SPSS 16.0 (SPSS, Chicago, IL, USA). The categorical variables were presented as proportion. The continuous variables were submitted to the Kolmogorov–Smirnov test to verify normal distribution and were presented as mean plus standard deviation or median plus interquartile interval, depending on distribution.
In order to verify factors associated with the presence of LBP currently among the students, bivariate analysis was performed using the chi-square test. The variables tested were gender, age, program, length of study, tobacco use, BMI, depression, and level of physical activity. The continuous variables such as age, phase of course, and BMI were transformed as categorical variables. All variables that achieved a level of significance in the bivariate analyses were inserted into a logistic regression model, in order to observe their independence from each other. The results were presented in adjusted odds ratio and confidence interval for 95%. Statistical significance was accepted at the level of p < 0.05.
Bivariate analyses were also performed to assess differences between LBP characteristics in the two programs using the chi-square test for categorical variables and Mann–Whitney test for continuous variables.
Results
Four hundred and sixteen students were evaluated, 207 (49.76%) being medical and 209 (50.24%) physiotherapy students. The majority of the students were women (73.1%), and the mean age was 21.68 years. Table 1 demonstrates the general characteristics of the sample and the comparisons between the programs. It is observed that the proportion of the female is higher in the physiotherapy program than in the medical program, the physiotherapy students are slightly younger than medical students, and prevalence of tobacco use is higher in physiotherapy.
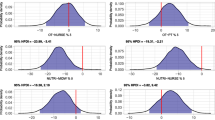
Overall, 77.9% of the students had LBP at some point in their lives, 66.8% in the last year and 14.4% of them reported that they were suffering from LBP at the time they answered the questionnaire. Physiotherapy students reported higher prevalence of LBP compared with the medical students (Fig. 1).

Prevalence of LBP
Table 2 demonstrates bivariate analyses concerning the factors associated with LBP. Program, duration of exposure to the program, and gender were the variables associated with LBP. The other variables did not achieve a level of significance during this phase of analysis. In the logistic regression model with these three variables, only the physiotherapy program and more exposure to the course were independently associated with pain (Table 3). Physiotherapy students were 2.51 times more likely to have LBP (95% CI 1.35–4.67; p = 0.003). Besides, subjects exposed to more than four semesters of the undergraduate study had 2.55 times more chance of having LBP (95% CI 1.43–4.55; p = 0.001).
Table 4 presents the characteristics of LBP between the programs. In relation to duration of pain in the last year, 11.5% experienced chronic LBP (p = 0.445). It was observed that the physiotherapy students are more likely to have sciatica than medical students (p = 0.003). Concerning the severity of pain, there were no differences between programs in the numerical rating scale (p = 0.445) and the four questions of ODI (p = 0.290). Use of medication for pain relief was mentioned by 33.3% of the students (p = 0.812). Differences were observed between programs in relation to seeking care because of LBP: medical students were less likely to seek care compared with physiotherapy students; and physiotherapy students were more likely to seek care from physiotherapists than medical students (p = 0.025).
Discussion
This cross-sectional study aimed to verify the existence of a higher prevalence of LBP in physiotherapy students. For this, medical students were chosen as a comparative group. First, we noted that the prevalence of LBP was higher in physiotherapy students compared with medical students. When the variables course, length of study and female gender were put into a logistic regression model, we observed that undergraduate physiotherapy study was independently associated with having LBP. To the best of our knowledge, this was the first study that clearly demonstrated the association between undergraduate physiotherapy study and LBP.
There are many reports in the literature concerning the burden of work-related musculoskeletal injuries in physiotherapists [3–7]. West and Gardner [7] reported that 16% of physiotherapists first experienced their injury as students, whereas 56% reported their worst injury to have occurred within the first 5 years of working as a physiotherapist. The most common region of injury is the low back [3, 4, 6, 7]. In our study, only 17.7% of physiotherapy students had never experienced LBP.
Nyland and Grimmer [15] carried out a cross-sectional study to evaluate the prevalence of LBP among physiotherapy students. They found a 1 week LBP prevalence of 27%, 1 month of 44%, 1 year of 63% and lifetime of 69% [15]. Also, they concluded that, compared to the first year students, students at all other levels of study incurred a significantly elevated risk for LBP [15]. Finally, the authors compared their results with other prevalence studies and discussed the possibility of the undergraduate physiotherapy study being a risk factor for LBP [15]. Our study clearly demonstrated this association, observing that the undergraduate physiotherapy program involves 2.51 times greater chance of experiencing LBP.
Studies with physiotherapists who have already graduated reported a 1 year prevalence of LBP ranging from 22 to 62.5% [4, 6, 7]. These professionals routinely perform some activities that could be risk factors for development of back pain like manual therapy such as soft tissue mobilization, transferring dependent patients, assisting patients in gait, providing manual resistance, assisting with mat activities, and lifting heavy and cumbersome equipment. Campo et al. [3] conducted a 1-year prospective study with physiotherapists in order to verify the incidence of work-related musculoskeletal injuries in these professionals. They found a 1-year LBP incidence of 6.6%. Also, they observed that patient transfers and repositioning were the main risk factors for LBP. Our study showed the increased likelihood of LBP among the advanced students, who are more exposed to practical activities.
In relation to severity of LBP, there were no differences between pain intensity and disability measured by ODI comparing physiotherapy to medical students. However, some findings in this study suggest that LBP can be disabling in physiotherapy students. For example, its was observed that 33.9% of physiotherapy students reported taking medication due to LBP, 25.1% needed to seek care because of back pain, and 13.3% of them had chronic LBP. Interestingly, Cromie et al. [4] reported that one in six physiotherapists changed settings or left the profession due to work-related musculoskeletal injuries. These findings demonstrate the need for specific educational programs discussing the risk factors for developing LBP in the physiotherapy setting, as a way to prevent these events in this group.
One important limitation of our study is that, as it was a cross-sectional study, we were not able to observe accurately if there is an increasing incidence of LBP during the program. It was observed that students with five or more semesters had higher prevalence of LBP. This suggests that there is an increased risk for advanced students, who most often are exposed to practical activities. Also, we did not intend to identify which activities in the course were associated with the development of LBP. Finally, further studies could demonstrate if preventive activities and educational interventions can decrease the risk for developing LBP among these students.
Conclusion
The physiotherapy students are 2.51 times more likely to have LBP in a sample composed of medical and physiotherapy students. The length of course exposure also is associated with the presence of LBP, with a risk of 2.55 times. These findings suggest that preventive activities should be performed during the undergraduate physiotherapy program in order to alleviate or minimize the impact of LBP in these students.
References
Ehrlich GE (2003) Low back pain. Bull World Health Organ 81(9):671–676
Punnett L, Pruss-Utun A, Nelson DI et al (2005) Estimating the global burden of low back pain attributable to combined occupational exposures. Am J Ind Med 48(6):459–469
Campo M, Weiser S, Koenig KL, Nordin M (2008) Work-related musculoskeletal disorders in physical therapists: a prospective cohort study with 1-year follow-up. Phys Ther 88(5):608–619
Cromie JE, Robertson VJ, Best MO (2000) Work-related musculoskeletal disorders in physical therapists: prevalence, severity, risks, and responses. Phys Ther 80(4):336–351
Mierzejewski M, Kumar S (1997) Prevalence of low back pain among physical therapists in Edmonton, Canada. Disabil Rehabil 19(8):309–317
Molumphy M, Unger B, Jensen GM, Lopopolo RB (1985) Incidence of work-related low back pain in physical therapists. Phys Ther 65(4):482–486
West DJ, Gardner D (2001) Occupational injuries of physiotherapists in North and Central Queensland. Aust J Physiother 47(3):179–186
Gorenstein C, Andrade L, Vieira Filho AH, Tung TC, Artes R (1999) Psychometric properties of the Portuguese version of the Beck Depression Inventory on Brazilian college students. J Clin Psychol 55(5):553–562
Craig CL, Marshall AL, Sjostrom M et al (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35(8):1381–1395
Guedes DP, Lopes CC, Guedes JE (2005) Reprodutibilidade e validade do Questionário Internacional de Atividade Física em adolescentes. Rev Bras Med Esporte 11(2):151–158
Kuorinka I, Jonsson B, Kilbom A et al (1987) Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon 18(3):233–237
Dionne CE, Dunn KM, Croft PR et al (2008) A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine 33(1):95–103
Fairbank JC, Pynsent PB (2000) The Oswestry Disability Index. Spine 25(22):2940–2952 (discussion 2952)
Vigatto R, Alexandre NM, Correa Filho HR (2007) Development of a Brazilian Portuguese version of the Oswestry Disability Index: cross-cultural adaptation, reliability, and validity. Spine 32(4):481–486
Nyland LJ, Grimmer KA (2003) Is undergraduate physiotherapy study a risk factor for low back pain? A prevalence study of LBP in physiotherapy students. BMC Musculoskelet Disord 4:22
Acknowledgments
We gratefully acknowledge the undergraduate students of the Liga Acadêmica Multidisciplinar de Neurologia e Neurocirurgia da Universidade de Caxias do Sul: Maíra Cristina Velho, Bruna Steiner, Natália Laste Becknkamp, Bruna de Souza da Silva.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Falavigna, A., Teles, A.R., Mazzocchin, T. et al. Increased prevalence of low back pain among physiotherapy students compared to medical students. Eur Spine J 20, 500–505 (2011). https://doi.org/10.1007/s00586-010-1646-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-010-1646-9