
Abstract
Aim
To determine the prevalence of low back pain (LBP) among health sciences students and to identify the associated factors.
Methods
Cross-sectional study was conducted among 1163 students from five health sciences colleges during the academic year 2016–2017. Self-administered questionnaire was conducted and included 4 sections: demographic characteristics, risk factors, Nordic musculoskeletal questionnaire and Oswestry disability questionnaire. Data were analyzed using SPSS.
Results
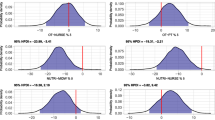
Mean age was 20.74 ± (1.59 years). 70.9% of students were female. Lifetime prevalence of LBP was 56.6%, 12-month prevalence 48.8%, and point prevalence 21.2%. Dentistry students had highest lifetime prevalence of LBP (67.6%) with significant p value (<0.001). Male were found to have higher lifetime prevalence compared to female (p ≤ 0.001). Spending more than 10 h on computer or tablet was significantly associated with LBP (OR 2.19; 95% CI 1.30–3.70; p = 0.003). Feeling discomfort on bed was associated with LBP (OR 1.81; 95% CI 1.38–2.38; p ≤ 0.001). Uncomfortable college furniture was associated with LBP (OR 1.40; 95% CI 1.09–1.79; p = 0.008). Using heavy backpack was found to be associated with LBP (OR 1.49; 95% CI 1.01–2.03; p = 0.011). Most of students LBP (90.3%) found to cause minimal disability on Oswestry scale.
Conclusion
This study has shown high prevalence of LBP among future healthcare provider. These risk factors should be well established to minimize the prevalence of LBP among future health sciences students. Dentistry students at higher risk of developing LBP compared to other students.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Low back pain (LBP) is one of the prevalent complaints among all age groups [1]. At least 90% of population experienced low back pain once in their life [2, 3]. Low back pain is commonly recognized “non-specific” as no organic source was found to cause the pain [4]. Frequent initial onset of back pain appears in age of 30 years, and the peak is between 45 and 60 years [5].
“Low back pain is no longer a disease of old” [5]. Although it is unusual for young population to visit physicians due to back pain, it has been reported that the percentage of adolescence population complaining of back pain varies between 13.5 and 39.8% in population aged between 18 and 24 years [5,6,7]. In population below 45 years, most prevalent cause to limit activities is back pain [8]. Also, low back pain has an impact on psychological aspect of the young population as it may lead to depression, anxiety and irritability [7].
Health science students are vulnerable to stress and prolonged time of studying and training which will make them predisposed for having LBP [2, 9]. Reported overall prevalence of LBP in health science students ranges from 40.1 to 57.9%, but there is controversy about which college has highest prevalence of LBP [1, 2]. According to Nordic classification of LBP, lifetime prevalence, 1-year prevalence and point prevalence of LBP among: medical students were 73.4, 46.1–59.9 and 27.2%; physical therapy students 69.2–82.3, 63.2–73.7 and 27.6%; and nursing students 79, 71 and 30%, respectively [1, 2, 5, 9,10,11,12]. LBP might be chronic, and this will affect future health professionals in the provision of health care to patients [9]. Studies have shown conflicting results on the effect of identifiable risk factors in health science students on LBP. Identified risk factors for LBP included gender, age, weight, general health status, socioeconomic status, smoking, year of study, psychosocial factors (feeling very sad, overwhelmed, exhausted), history of back pain, history of back trauma, family history of treated back pain, use of heavy backpack, physical fitness, prolonged sitting time, bad postural habits, short sleep hours, discomfort in bed and college furniture [1, 2, 5,6,7, 9, 12]. If risk factors are well recognized and understood, this would help in establishing preventive measures of LBP and modifying risk factors which will lead to better quality of life for future health professionals [1, 9].
No studies have been done in our region about the prevalence of low back pain among health science students. Further risk factors will be tested in this study. Aim of this study is to determine the prevalence of LBP among health science students and to identify the association between risk factors and LBP.
Methods
Quantitative cross-sectional study was conducted at 5 health science colleges (medicine, dentistry, pharmacy, nursing and college of applied medical sciences “physical therapy, occupational therapy, clinical laboratory and clinical nutrition”) at King Saud University, Riyadh, Saudi Arabia, which was conducted during the academic year 2016–2017. The study included 1163 students and excluded students who have spinal deformities or had undergone back surgery. Ethical approval was obtained from institutional review board at medical college, King Saud University.
Self-administered questionnaire was distributed during the lunch break of students. Instruction was explained by one of the authors and the data collector who was well informed about all the parts of questionnaire. Completeness of questionnaires was checked by the authors. The questionnaire contains 52 questions in 3 pages divided into 4 sections: demographic characteristics such as age, gender, weight, height, college, year at college. Risk factors included smoking, physical activity, coffee drinking, hours spent on using computer, position while studying, sleeping hours, comfort of bed to back, comfort of college furniture to bed, using heavy backpack, being overwhelmed, feeling exhausted and feeling sad. LBP was assessed using Nordic musculoskeletal questionnaire. Disability was classified based on Oswestry questionnaire. Nordic and Oswestry questionnaires were previously tested for validity and reliability [13, 14].
The questionnaire was piloted on 10 students to ensure the clarity of information and determine the time needed to fill the questionnaire. Feedback from pilot study was modified on last draft of questionnaire. Data from pilot study were not included in the study.
Data were analyzed by using Statistical Package for Social Studies (SPSS 22; IBM Corp., New York, NY, USA). Continuous variables were expressed as mean ± standard deviation, and categorical variables were expressed as percentages. The t-test was used for continuous variables, and Chi-square test was used for categorical variables. Odds ratio (OR) with their 95% confidence interval (CI) was used for assessing the risk factors for LBP using the univariate analysis. A p value <0.05 was considered statistically significant.
Consent form was provided for each participant which included the purpose of study and the right of participant to withdraw at any time without completing the questionnaire. Participants’ anonymity was assured by assigning each participant with a code number for the purpose of analysis only. No incentives or rewards were given to participants.
Results
One thousand and fifty-two participants out of 1163 were enrolled in this study. Exclusion of participants was due to incomplete questionnaire, history of back surgery or deformity, pain location outside low back demarcation of Nordic questionnaire. Mean age of participants ± (standard deviation) was 20.74 ± (1.59 years). Majority of participants were female (70.9%). Demographic characteristics are shown in Table 1.
Overall lifetime prevalence of LBP among health sciences undergraduate was 56.6%, 12-month prevalence 48.8%, and point prevalence 21.2%. Dentistry students had significantly highest lifetime, 12-month and point prevalence compared to other students (Table 2). Males had significantly higher lifetime prevalence of LBP than females (Table 3).
Risk factors associated significantly with point prevalence of LBP are hours spent on using computer or tablet (p = 0.002), sleeping on uncomfortable bed (p < 0.001), uncomfortable college furniture (p = 0.005), using heavy backpack (p = 0.01), feeling overwhelmed (p < 0.001), feeling sad (p < 0.001), previous history of back trauma (p < 0.001) and family history of low back pain treated by a doctor (p < 0.001).
Majority of students complaining of LBP are having pure LBP, not sciatic pain; most of them did not use medication for their back pain, but it has been shown that highest percentage of students taking medication are nursing students compared to other students, and based on Oswestry disability scale, LBP is causing minimal disability on undergraduates. Characteristics of LBP classified by colleges are show in Table 4.
In multivariable logistic regression model, factor associated significantly with point prevalence are using computer or tablet more than 10 h per day, sleeping on uncomfortable bed, uncomfortable college furniture and using heavy backpack (Table 5).
Discussion
The overall lifetime prevalence of LBP among undergraduates was found to be high (56.6%), which is within the range of previous studies (40.1–57.9%) [1, 2]. Further, 1-year prevalence was reported to be 48.8% and point prevalence 21.2%, which is higher than the results reported in Hafeez et al.’s study (21%, 13.1%) [2].
Yucel et al. [15] reported that medical students had the highest prevalence of LBP compared to dentistry, pharmacology and health sciences students. In our study, dentistry students showed significantly highest lifetime, 1-year and point prevalence of LBP compared to other students. This could be attributed to the nature of their clinical training which makes them to sit on a chair for prolonged time [16].
Incidence of LBP increased with age, but the result was not significant. In opposite to the findings of the literature, males had higher lifetime prevalence with very significant result than females [1, 2, 9, 15]. Majority of males (56.7%) are more than or equal to 22 years, but the females are younger which might explain why male have higher prevalence of LBP. BMI was not significantly associated with LBP, which is consistent with previous studies [1, 15]. No significant association was found between incidence of LBP and smoking. Coffee consumption increased in students having LBP, but in this study no significant correlation was found between coffee consumption and LBP [17]. Most of students (61.4%) are physically inactive, and no significant association was found between physical activity and LBP. A study involving undergraduates from sport and physical education institute reported that some sports are significantly associated with LBP [18]. In this study, recreational sports (football, basketball, volleyball and swimming) had no association with LBP.
It is reported that prolonged sitting time using computer or tablet is strongly associated with LBP [1, 2]. In this study, the result is consistent with the literature and it shows significantly higher point prevalence among students spending more than 10 h using computer or tablet compared with other groups. Prolonged sitting increases compression load on the spine [2]. Position while studying and sleeping hours were not associated with incidence of LBP. Students who stated that their mattress is uncomfortable were very significantly associated with point prevalence (p < 0.001), and this could be attributed to the use of soft mattress by the students. Uncomfortable college chairs were also found to be significantly associated with point prevalence (p = 0.005). In a study conducted on health education students, they found that backpack more than 4 KG is associated with LBP [19]. In this study, heavy backpack was found to be associated significantly with LBP (p = 0.01). Carrying laptop, tablets and health sciences books might justify the association [5]. Psychological factors were identified to contribute to development of LBP [7, 15]. In this study, being overwhelmed and sad is associated significantly with point prevalence of LBP (p < 0.001). Students who feel exhausted had higher incidence of LBP compared to who did not feel exhausted, but with no significant result. Hafeez and Yucel found an association between LBP and history of trauma of back, but it was not significant [2, 15]. In contrast, Alshagga reported significant association between trauma and family history of musculoskeletal disorders with LBP [9]. In this study, previous history of trauma of back and family history of treated LBP were strongly associated with incidence of LBP (p < 0.001).
Limitations
The weakness is the study being cross-sectional. Since LBP was causing minimal disability to undergraduates, further longitudinal studies need to be conducted to evaluate long-term effect of LBP.
Conclusion
Health science students reported high prevalence of LBP. Dentistry students are at higher risk to develop LBP compared with other colleges. Prolonged sitting using computer or tablet, sleeping on uncomfortable mattress and using heavy backpack were found to be associated with LBP. Lectures about preventive measures should be included in health-related courses. Students should take a break during using computer or tablet and they should do stretching exercises to back. Students should be aware to use electronic version of books instead of paper based trying to not carry it on backpack. Further detailed studies should be conducted on the relation between quality of matters and LBP among undergraduates.
References
Nordin NAM, Singh DKA, Kanglun L (2014) Low back pain and associated risk factors among health science undergraduates. Sains Malays 43(3):423–428
Hafeez K, Ahmed Memon A, Jawaid M, Usman S, Usman S, Haroon S (2013) Back pain—are health care undergraduates at risk? Iran J Public Health 42(8):819–825
Falavigna A, Teles A, Mazzocchin T, de Braga G, Kleber F, Barreto F et al (2010) Increased prevalence of low back pain among physiotherapy students compared to medical students. Eur Spine J 20(3):500–505
Urquhart D, Berry P, Wluka A, Strauss B, Wang Y, Proietto J et al (2011) 2011 young investigator award winner. Spine 36(16):1320–1325
Anand T, Aggarwal N, Kishore J, Ingle G (2013) Low back pain and associated risk factors among undergraduate students of a medical college in Delhi. Educ Health 26(2):103
Mohammad W, El-Sais W (2013) Prevalence of non-specific self-reported back pain among adolescents at Hail Territory-KSA. J Asian Sci Res Asian Econ Social Soc 3(10):1036–1045
Kennedy C, Kassab O, Gilkey D, Linnel S, Morris D (2008) Psychosocial factors and low back pain among college students. J Am Coll Health 57(2):191–196
Al-Saleh SS, Alballa SR, Al-Dalaan AN, Bahabri SA, Al-Sekeit MA, Mousa MA (2003) How common is back pain in Al-Qaseem region. Saudi Med J 24(2):170–173
Alshagga M, Nimer A, Yan L, Ibrahim I, Al-Ghamdi S, Radman Al-Dubai S (2013) Prevalence and factors associated with neck, shoulder and low back pains among medical students in a Malaysian Medical College. BMC Res Notes 6(1):244
Nyland L, Grimmer K (2003) Is undergraduate physiotherapy study a risk factor for low back pain? A prevalence study of LBP in physiotherapy students. BMC Musculoskelet Disord 4(1):22
Leggat P, Smith D, Clark M (2008) Prevalence and correlates of low back pain among occupational therapy students in Northern Queensland. Can J Occup Ther 75(1):35–41
Moroder P, Runer A, Resch H, Tauber M (2011) Low back pain among medical students. Acta Orthop Belg 77:88–92
Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G et al (1987) Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon 18(3):233–237
Fairbank JC, Pynsent PB (2000) The Oswestry disability index. Spine 25(22):2940–2952 (discussion 52)
Hulya Yucel, Perihan Torun (2016) Incidence and risk factors of low back pain in students studying at a health university. Bezmialem Sci 4(1):12–18
Vijay S, Ide M (2016) Musculoskeletal neck and back pain in undergraduate dental students at a UK dental school—a cross-sectional study. BDJ 221(5):241–245
McPartland JM, Mitchell J (1997) Caffeine and chronic back pain. Arch Phys Med Rehabil 78:61–63
Triki M et al (2015) Prevalence and risk factors of low back pain among undergraduate students of a sports and physical education institute in Tunisia. Libyan J Med 10(1):26802
Heuscher Z et al (2010) The association of self-reported backpack use and backpack weight with low back pain among college students. J Manip Physiol Ther 33(6):432–437
Acknowledgements
The authors thank Hanan Alabdullah for her great effort in data collection.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
AlShayhan, F.A., Saadeddin, M. Prevalence of low back pain among health sciences students. Eur J Orthop Surg Traumatol 28, 165–170 (2018). https://doi.org/10.1007/s00590-017-2034-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-017-2034-5