
Abstract
The conservative and operative treatment strategies of hematogenous spondylodiscitis in septic patients with multiple risk factors are controversial. The present series demonstrates the outcome of 18 elderly patients (median age, 72 years) with septic hematogenous spondylodiscitis and intraspinal abscess treated with microsurgical decompression and debridement of the infective tissue, followed by posterior stabilization and interbody fusion with iliac crest bone graft in one or two lumbar segments. The majority of the patients were unsuccessfully treated with intravenous antibiotics prior to the operation. Antibiotic therapy was continued for more than 6 weeks postoperatively. Morbidity and early mortality amounted to 50 and 17%, respectively. Three patients died in the hospital from internal complications after an initial postoperative improvement of the inflammatory clinical signs and laboratory parameters. Fifteen patients recovered from the spinal infection. Three of them died several months after discharge (cerebral hemorrhage, malignancy and unknown cause). Twelve patients had excellent or good outcomes during the follow-up period of at least 1 year. The series shows that operative decompression and eradication of the intraspinal and intervertebral infective tissue with fusion and stabilization via a posterior approach is possible in septic patients with multiple risk factors and leads to good results in those patients, who survive the initial severe stage of the septic disease. However, the morbidity and mortality suggest that this surgical treatment is not the therapy of first choice in high-risk septic patients, but may be considered in patients when conservative management has failed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
During the last few decades, infections of the spine have been diagnosed with increasing frequency [2, 32]. The clinical features of spinal infections vary between long-lasting, localized and slowly progressive backache and nearly acute, septic and life-threatening courses with severe back pain and rapidly progressive neurological deficits [29, 36].
Hematogenous spinal infections frequently present as spondylodiscitis, leading to neurological deficits due to secondary epidural abscesses in a considerable number of cases [7, 29, 31, 35]. Many patients with hematogenous spinal infections suffer from multiple predisposing conditions, [5, 7, 16, 17, 27, 29, 30], and preceding non-spinal infections are common [16, 17, 27, 29]. Staphylococcus aureus is the predominant causative organism [29].
The early recognition of pyogenic spinal infections is very important, because specific treatment can lead to a significant improvement of morbidity and mortality [4, 16, 29]. The majority of spondylodiscitis without neurological deficits or severe progressive symptoms respond well to conservative treatment by intravenous antibiotics and spinal external immobilization [3, 4, 9, 26, 29, 34, 36]. Surgical decompression is mandatory in the presence or development of significant neurological deficits [16, 26, 29, 36], and operative treatment is also indicated in patients with disabling back pain [16, 26, 36] as well as in cases refractory to conservative treatment [4, 26, 28, 36]. The operation has to be followed by administration of bacteria-specific intravenous antibiotics for several weeks [26, 28, 36].
Different surgical strategies are possible in severe cases of spondylodiscitis. Some authors prefer minimally invasive or endoscopic surgical debridement and decompression without fusion and instrumentation [19, 25]. Others describe good results of dorsal instrumentation without eradication of the infected tissue [6, 13]. However, most surgeons recommend additional fusion and internal fixation [7, 16, 26, 28, 29]. Anterior, posterior or combined approaches in single- or two-staged procedures are used, each of them harboring advantages and disadvantages [8, 11, 15, 20, 21, 23, 24, 26, 28, 30].
In infections of the lumbar spine, posterior interbody fusion with bone graft and instrumentation with a pedicle screw–rod system is, to our knowledge, performed in many hospitals. However, only a few series are published [24, 28, 30]. No series have been published on posterior lumbar interbody fusion in high-risk patients with multiple concomitant diseases suffering from hematogenous spondylodiscitis associated with septic symptoms. The optimal treatment strategies of spondylodiscitis with secondary intraspinal abscess in septic, severely ill patients are not known. Yet, no published data clarify whether a conservative treatment or one of the possible operative managements has to be preferred. We suppose that spinal infection has to be addressed as the main focus that maintains the general septic infection in the majority of these patients. Thus, the spinal location of the infection has to be thoroughly debrided [4, 29] to control sepsis. Since its description in the treatment of spinal tuberculosis [18], fusion with bone graft [2, 10] has been commonly performed to treat pyogenic spondylodiscitis [7, 24, 26, 28–30, 36]. Additional instrumentation of the involved segment and the consecutive early mobilization of the patients have been supposed to lead to lower rates of postoperative complications [26]. Many authors favor anterior approaches to achieve a direct access to the infected intervertebral tissue and perform additionally an anterior [11, 12] or posterior stabilization [8, 11, 15, 21] in one-staged [11, 21, 23, 33] or two-staged [1, 8, 15] operations. However, if the vertebral bodies are not destroyed by the inflammatory process, the debridement of the intraspinal and intervertebral infectious tissue as well as the instrumentation can be achieved by a single-staged posterior approach [24, 28, 30].
We present a series of decompression and thorough debridement of the infected tissue (to control the source of the sepsis), posterior lumbar interbody fusion and dorsal instrumentation (to facilitate early mobilization) in severely diseased patients with septic hematogenous spondylodiscitis and associated epidural abscess.
Patients and operative methods
The medical records of the patients were retrospectively reviewed. Usually, all patients who undergo spinal instrumentation in our clinic are observed during a follow-up period between 1.5 and 2 years. Those patients, who did not return to the outpatient department were recalled for follow-up examination for the purpose of this study. We classified the outcome as excellent (return to previous activities with little or no complaints), good (return to previous activities, but occasionally with recurrent back pain after activities), fair (reduction of previous activities necessary) and poor (no return to previous activities possible) [22, 24]. Paresis was classified according to the Frankel Neurological Performance Scale (A: sensation and voluntary motor function absent, E: sensation and motor function normal) [14].
Between 2004 and 2008, posterior lumbar interbody fusion with pedicle screws and autogenous bone was performed in 22 patients with spondylodiscitis. Eighteen of these patients (11 female, 7 male) were included in this retrospective analysis, because all of these patients suffered from hematogenous septic spondylodiscitis with associated epidural abscesses. In all 18 patients, the intraspinal abscesses were located ventrally, in direct contact with the involved intervertebral disc (Fig. 1). Sixteen patients were unsuccessfully treated with antibiotics in other hospitals for a period between 3 and 28 days, prior to transfer to the department of neurosurgery. In these 16 patients, the C-reactive protein (CRP) levels exceeded 100 mg/l and they had leucocytosis. No patient underwent a spinal invasive procedure prior to the infection.

Septic hematogenous spondylodiscitis with intraspinal epidural empyema in an 84 year-old patient (patient 7) in the segment L1/2. T-1- and T-2-weighted MRI. Contrast medium was not applied due to renal failure
All patients had multiple predisposing risk factors: besides arterial hypertension (16 patients), 13 patients suffered from diabetes mellitus, 10 from variable cardiac diseases, 10 from renal failure and 9 from extreme obesity. Six patients had malignant tumors, five had lung diseases and four had peripheral arterial or venous insufficiencies. Seven patients had a paresis in the lower extremities. The median age was 72 years (range 65–87). Thirteen Patients were older than 70 years and four older than 80 years.
The putative infection sources were skin infections of the feet in two cases, joint infections in two cases and a persistent perianal wound after cancer operation (1 patient), meningitis after glioma operation (1 patient), endocarditis (1 patient), skin laceration (1 patient), urinary infection (2 patients) and prior extraspinal operations (gynecological and forearm operations, 2 patients). In six patients, the infective causes could not be found.
Staphylococcus aureus was the causative pathogen in seven patients and Escherichia coli could be isolated in four patients. Other infectious agents were Staphylococcus haemolyticus (1 patient), Staphylococcus epidermidis (1 patient) and Streptococcus bovis (1 patient) (Tables 1, 2).
Conservative treatment was considered to have failed when disabling pain and a reduced general condition due to the sepsis rendered the mobilization impossible (all patients). Additionally, hemodynamic instability (1 patient), beginning or deteriorating renal failure due to the sepsis (6 patients) and deteriorating or severe neurological deficits (7 patients) were indications of surgery (Table 1).
Spinal computed tomography (CT) was performed in all patients pre- and postoperatively. Additionally, a preoperative magnetic resonance imaging (MRI) was performed in all patients except in one female patient due to the presence of a cardiac pacemaker. Further controls were done using conventional spinal radiography. Clinical symptoms and inflammatory markers such as body temperature, CRP and white blood cell (WBC) counts were obtained at least daily in the early postoperative period; ESR is not determined routinely in our hospital.
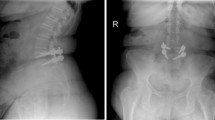
Several pieces of tricortical iliac bone crest as well as spongiosa graft were obtained via the same operative approach (in the cases of spondylodiscitis in the lower lumbar segments) or via a separate incision (infections of the upper lumbar spine) under general anesthesia. The transpedicular screws were placed under fluoroscopic control. Meticulous removal of the intraspinal infective tissue and discectomy were performed via hemilaminectomy or laminectomy. Thereafter, interbody fusion with the autograft and fixation of the rods under slight compression of the segment were performed (Fig. 2). The wound drainage persisted for 1 or 2 days. Interbody fusion and instrumentation were performed in one lumbar segment (11 patients) or in two segments (in three patients both levels were infected; three patients had adjacent spinal stenosis or instability; in one patient the instrumentation had to be exceeded due to intraoperative problems: see “Results”).

CT scan of the same patient (Fig. 1) after the operation. Posterior interbody fusion with iliac crest bone graft and stabilization with transpedicular screw–rod system
The patients were supervised in the intensive care unit for at least one night. The mobilization into the sitting or standing position started at the intensive care unit or at the neurosurgical ward on the first postoperative day after CT control except in two patients because of pulmonary complications (cases 8 and 14). An external orthosis was applied for about 4 weeks. Intravenous antibiotics were administered until normalization of the CRP or for a period of 6–8 weeks, followed by oral antibiotics for about 4 weeks. Before getting the results of the antibiogram, the initial antibiotic therapy (Table 1) was continued. In those two patients who did not receive antibiotics preoperatively, clindamycin was administered until the antibiogram was obtained.
Results
Mortality
Three patients died in the hospital after an initial postoperative improvement of the inflammatory clinical and laboratory symptoms (mortality 17%): One patient died from multi-organic failure, one patient from pneumonia and one from endocarditis.
Morbidity
Morbidity amounted to 50% (9 from 18 cases). In three patients, a superficial debridement at the site of the iliac crest became necessary because of superficial wound infection. After the revisions, uncomplicated wound healing could be achieved. One patient required spinal superficial wound revision due to secretion without evidence of superficial or deep wound infection. One patient had to be re-operated because of a displaced screw, another because of a screw pullout (see below).
Transitory complications were urinary tract infection (2), cerebral ischemia with transient slight hemiparesis (1) and diarrhea (1).
There was one intraoperative complication: in a female patient (operation in the L3/4 segment), one pedicle screw in L4 could not be fixed. Thus, the operating surgeon decided to extend the instrumentation to the L4–L5 segment. The infected disc was removed and replaced by iliac crest bone graft; however, the intact disc in the L4/5 segment was left in place. After initial recovery, this patient experienced recurrent backache as well as clinical and laboratory infection signs. Radiographs and CT scans demonstrated secondary lucencies around the pedicle screws and slight screw pullouts. This patient was re-operated. After multisegmental posterior fixation from L1 to the sacrum, a corporectomy of L3 and L4 and the reconstruction with an expandable titanium ring cage, filled with autologous iliac bone, was performed via an anterolateral approach. The patient recovered from the infectious symptoms and could be discharged after 6 weeks. She died several months later at home. She suffered from several severe concomitant diseases including vulva carcinoma.
Outcome
Three patients died early on after an initial improvement (see above). Three patients were cured from the spinal infection, but died several months after the discharge during the follow-up period: one patient died of an unknown cause at home; one patient died during therapy in a rehabilitation clinic from cerebral hematoma; and one patient died from malignancy and multimorbidity at home.
Twelve patients were cured from the sepsis and spondylodiscitis with normalization of the laboratory infection markers in follow-up controls. After at least 1 year, 11 of them had an excellent outcome and were painless for most of the time. One patient had a good outcome, but complained of moderate backache from time to time. Seven patients suffered from paraparesis prior to the operation. Two of these patients died. In the surviving five patients, neurological deficits improved completely (Tables 1 and 2).
Discussion
Different and obviously contradictory surgical approaches have been successfully used in the treatment of severe spondylodiscitis: minimally invasive [25] and endoscopic [19] approaches without fusion and instrumentation versus posterior instrumentation combined with anterior bone grafting [8, 11, 15, 21] or posterior instrumentation combined with anterior insertion of a titanium cage [21, 23]; an anterior approach with bone grafting and without instrumentation [10, 12, 20] or with anterior instrumentation [11, 12] versus a posterior approach and instrumentation with discectomy and interbody bone graft [24, 28, 30] or without eradication of the infected tissue and interbody fusion [6, 13]; two-staged [1, 8, 15] versus one-staged [11, 21, 23, 33] dorsoventral operations in variable sequential procedural orders.
Prospective, controlled clinical studies comparing the different methods are necessary, but would be difficult because of: the rareness of the disease, the apparently comparable results of different operative therapies, and the individual preferences of spinal surgeons when choosing the operative technique. Thus, prospective, controlled studies do not exist, and surgeons treating spinal infections have to refer to retrospective comparisons and empirical results that have been reported in a large number of publications.
Though the posterior lumbar approach in the treatment of spondylodiscitis is, to our knowledge, used in many neurosurgical and orthopedic hospitals, only a few series have been published on the outcomes of patients after posterior lumbar instrumentation and interbody fusion (PLIF).
Rath et al. [30] compared retrospectively the results of debridement and posterior internal fixation. A high percentage of the patients suffered, like those in the present study, from associated illnesses and were in a reduced general condition. The overall good outcome suggested that a posterior approach in a single-staged procedure using a transpedicular screw–rod system, which could be left in place, and autologous bone is nearly always sufficient and does not bear a higher risk of persistence or recurrence of the infection. The study combined data of postprocedural and spontaneous spondylodiscitis and of tuberculous and non-specific infections as well as thoracic and lumbar operative interventions. The mean age of the patients was somewhat lower than in this present study.
Przybylski et al. [28] showed, that a single-staged operation using iliac autograft is an effective procedure for the treatment of infection and the stabilization of the spine, with sufficient pain reduction and facilitation of early mobilization. The authors reported two lethal outcomes during the first postoperative week owing to medical complications. The authors presented 12 patients with postinterventional or hematogenic lumbar spondylodiscitis. The patients were younger than those in the presented study, and they had less associated risk factors. The presence of intraspinal abscesses or septic signs was not mentioned.
Lee et al. [24] presented their results on 18 patients with pyogenic lumbar spondylodiscitis, operated by means of posterior lumbar interbody fusion using a pedicle screw system and intervertebral iliac crest autograft as well as a posterolateral graft. The authors reported an effective control over the infection and good outcomes with no lethal complication. The mean age of the patients was younger than in our report, and the number of concomitant diseases was considerably lower. Both facts are explained in the origin of the spondylodiscitis, which was presumably caused by spinal interventions in 13 of 18 patients.
Thus, the patients enrolled in the studies of Rath, Przybylski and Lee and co-authors cannot be compared with the cases in our report. We show the results of posterior lumbar interbody fusion and instrumentation in selected high-risk patients of advanced age with spontaneous spondylodiscitis and secondary intraspinal abscesses. All patients suffered from sepsis and multiple predisposing diseases. The best way to treat spondylodiscitis in septic patients with multiple risk factors is not known, and studies comparing conservative and surgical management in those high-risk patients do not exist. A conservative management would avoid severe intra- and postoperative complications. However, a conservative antibiotic therapy was given in other hospitals in all but two of our patients, but remained unsuccessful with regard to laboratory parameters and clinical symptoms (backache and, in some patients, development of neurological deficits). Hence, we regarded an invasive procedure as obligatory. A mere decompression of the spinal canal would not lead to eradication of the infective focus. Therefore, our operative goals were to (1) decompress the neural structures, (2) control the source of sepsis by a thorough removal of the infective tissue from the spinal canal and the intervertebral space and (3) render an early mobilization possible by operative fusion and internal fixation to avoid secondary complications due to long-term immobilization.
In a recent study, Liljenqvist et al. [23] demonstrated the efficacy of a single-staged procedure with posterior transpedicular fixation over several segments and empyema removal, followed by anterior decompression and column reconstruction with an expandable titanium cage filled with autologous bone. Two severely ill patients died several weeks after the operation. Like a number of other authors [8, 11, 12, 15, 21], the authors confirm that the use of metallic implants is safe and does not lead to persistence or recurrence of infection. Comparable to those in our report, most of the patients had advanced age and severe associated risk factors.
We preferred the posterior operation to the anterior approach due to its putatively lower risks of perioperative complications in these severely diseased patients. Generally, we use the anterior or circumferential approach reported by Liljenqvist et al. [23] with corporectomy, fusion with titanium cage and posterior internal stabilization only in patients with severe vertebral destruction and spinal deformation. However, this was only thrice the case during the period of the presented series.
An initial postoperative recovery from spondylodiscitis was seen in all patients. Fifteen patients could be cured from the infection. Three of these patients died several months after the operation (cerebral hemorrhage, malignancy and polymorbidity, and unknown cause). Twelve patients had an excellent or good outcome with no or tolerable backache during the follow-up period of at least 1 year.
Three patients died in the hospital. Two of these three patients died from severe internal complications, and one patient from the initial infection (endocarditis). In no case was a direct causative relation between death and spinal operation proved. However, these early lethal outcomes amounted to a perioperative mortality of 17%; the perioperative morbidity was 50%. This high morbidity and mortality are putatively related to the poor primary clinical conditions of the patients. It suggests that the aggressive operation including thorough debridement, fusion and instrumentation is not the therapy of first choice in high-risk septic patients. However, the recovery from infection in 83% and the good long-term results in two-thirds of the patients implicate that this operative approach may be taken into consideration in patients who underwent an unsuccessful preceding conservative treatment and who suffer from progressive neurological deficits.
A retrospective statistical comparison between patients with a good outcome and those who died during few months after the operation is not appropriate. The causes of lethal outcomes were miscellaneous and could not be directly related to the operative therapy.
The concomitant diseases, especially diabetes mellitus, can lead to postoperative infections. The low number of infections (two urinary and one iliac crest wound infections) in patients with diabetes mellitus may be explained by the continuous intravenous antibiotic therapy.
In one female patient, intraoperative problems occurred. The posterior instrumentation was extended to an adjacent segment without removal of the intact intervertebral disc. This was the only patient where a failure of the fusion and instrumentation was observed. After initial recovery, the patient suffered from recurrent symptoms of infection. Radiography and CT scans showed a loosening of the pedicle screws. The patient had to be re-operated on by means of corporectomy and circumferential instrumentation. The failure of the instrumentation may be explained by a residual segmental mobility due to the intact disc in a morbidly obese patient, who was mobilized early on. The complication in this single case where the instrumentation bridged a remaining intervertebral disc corroborates the necessity for a rigid internal stabilization when early mobilization is intended.
Conclusion
The posterior approach with fusion and stabilization in elderly high-risk patients with spondylodiscitis, intraspinal abscesses and signs of septic complications is feasible and leads to a good outcome in all patients who survive the first few months of the septic disease. However, the morbidity and mortality suggest that this surgical treatment is not the therapy of first choice in high-risk septic patients, but may be considered in patients when conservative management had failed.
Very different therapeutic strategies in the treatment of pyogenous spondylodiscitis have been successfully used worldwide. A multicentric prospective study would be necessary to verify the best surgical approaches in severe and life-threatening septic spondylodiscitis.
References
Arnold PM, Bak PN, Bernardi RJ, Luck E, Larson S (1997) Surgical management of nontuberculous thoracic and lumbar vertebral osteomyelitis: report of 33 cases. Surg Neurol 47:551–561
Cahill DW, Love LC, Rechtine GR (1991) Pyogenic osteomyelitis of the spine in the elderly. J Neurosurg 74:878–868
Carragee EJ (1997) Pyogenic vertebral osteomyelitis. J Bone Joint Surg 79:874–880
Chen W-H, Jiang L-S, Dai L-Y (2007) Surgical treatment of pyogenic vertebral osteomyelitis with spinal instrumentation. Eur Spine J 16:1307–1316
Curry WT, Hoh BL, Amin-Hanjani S, Eskandar EN (2005) Spinal epidural abscess: clinical presentation, management, and outcome. Surg Neurol 63:364–371
Deininger MH, Unfried MI, Vougioukas VI, Hubbe U (2009) Minimally invasive dorsal percutaneous spondylodesis for the treatment of adult pyogenic spondylodiscitis. Acta Neurochir 151:1451–1457
Dietze DD, Fessler RG, Jacob RP (1997) Primary reconstruction for spinal infections. J Neurosurg 86:981–989
Dimar JR, Carreon LY, Glassman SD, Campbell MJ, Hartman MJ, Johnson JR (2004) Treatment of pyogenic osteomyelitis with anterior debridement and fusion followed by delayed posterior spinal fusion. Spine 29:326–332
Eismont FJ, Bohlman HH, Soni PL, Goldberg VM, Freehafer AA (1983) Pyogenic and fungal vertebral osteomyelitis with paralysis. J Bone Joint Surg 65:19–29
Emery SE, Chan DP, Woodward HR (1989) Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 14:284–291
Eysel P, Hopf C, Vogel I, Rompe J-D (2005) Primary stable anterior instrumentation or dorsoventral spondylodesis in spondylodiscitis? Results of a comparative study. Eur Spine J 6:152–157
Fang D, Cheung KM, Dos Remedios ID, Lee YK, Leong JC (1994) Pyogenic vertebral osteomyelitis: treatment by anterior spinal debridement and fusion. J Spin Disord 7:173–180
Frangen TM, Kälicke T, Gottwald M, Andereya S, Andress H-J, Russe OJ, Müller EJ, Muhr G, Schinkel C (2006) Surgical management of spondylodiscitis. An analysis of 78 cases. Unfallchirurg 109:743–753
Frankel HL, Hancock DO, Hyslop G, Melzakh J, Michaelis LS, Ungar GH, Vernon JD, Walsh JJ (1969) The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. Paraplegia 7:179–192
Fukuta S, Miyamoto K, Masuda T, Hosoe H, Kodama H, Nishimoto H, Sakaeda H, Shimizu K (2003) Two-stage (posterior and anterior) surgical treatment using posterior spinal instrumentation for pyogenic and tuberculotic spondylitis. Spine 28:E302–E308
Hadjipavlou AG, Mader JT, Necessary JT, Muffoletto AJ (2000) Hematogenous pyogenic spinal infections and their surgical management. Spine 25:1668–1679
Hlavin ML, Kaminski HJ, Ross JS, Ganz E (1990) Spinal epidural abscess: a ten-year perspective. Neurosurgery 27:177–184
Hodgson AR, Stock FE (1956) Anterior spinal fusion: a preliminary communication on the radical treatment of Pott’s disease and Pott’s paraplegia. Br J Surg 44:266–275
Ito M, Abumi K, Kotani Y, Kadoya K, Minami A (2007) Clinical outcome of posterolateral endoscopic surgery for pyogenic spondylodiscitis: results of 15 patients with serious comorbid conditions. Spine 32:200–206
Klöckner C, Valencia R (2003) Sagittal alignment after anterior debridement and fusion with or without additional posterior instrumentation in the treatment of pyogenic and tuberculous spondylodiscitis. Spine 28:1036–1042
Korovessis P, Petsinis G, Koureas G, Iliopoulos P, Zacharatos S (2006) Anterior surgery with insertion of titanium mesh cage and posterior instrumented fusion performed sequentially on the same day under one anesthesia for septic spondylitis of thoracolumbar spine: is the use of titanium mesh cages safe? Spine 31:1014–1019
Kirkaldy-Willis WH, Paine KW, Cauchoix J, McIvor G (1974) Lumbar spinal stenosis. Clin Orthop 99:30–50
Liljenqvist U, Lerner T, Bullmann V, Hackenberg L, Halm H, Winkelmann W (2004) Titanium cages in the surgical treatment of severe vertebral osteomyelitis. Eur Spine J 12:606–612
Lee JS, Suh KT (2006) Posterior lumbar interbody fusion with an autogenous iliac crest bone graft in the treatment of pyogenic spondylodiscitis. J Bone Joint Surg Br 88:765–770
Nagata K, Ohashi T, Ariyoshi M, Sonoda K, Imoto H, Inoue A (1998) Percutaneous suction aspiration and drainage for pyogenic spondylitis. Spine 23:1600–1606
Ogden AT, Kaiser MG (2004) Single-stage debridement and instrumentation for pyogenic spinal infections. Neurosurg Focus 17:E5, 1–5
Osenbach RK, Hitchon PW, Menezes AH (1990) Diagnosis and management of pyogenic vertebral osteomyelitis in adults. Surg Neurol 33(4):266–275
Przybylski GJ, Sharan AD (2001) Single-stage autogenous bone grafting and internal fixation in the surgical management pf pyogenic discitis and vertebral osteomyelitis. J Neurosurg (Spine) 94:1–7
Qinones-Hinojosa A, Jun P, Jacobs R, Rosenberg WS, Weinstein PR (2004) General principles in the medical and surgical management of spinal infections: a multidisciplinary approach. Neurosurg Focus 17:E1, 1–15
Rath SA, Neff U, Schneider O, Richter HP (1996) Neurosurgical management of thoracic and lumbar vertebral osteomyelitis and discitis in adults: a review in 43 consecutive surgically treated patients. Neurosurgery 38:933–938
Rezai AR, Woo HH, Errico TJ, Cooper PR (1999) Contemporary management of spinal osteomyelitis. Neurosurgery 44:1018–1026
Rigamonti D, Liem L, Sampath P, Knoller N, Numaguchi Y, Schreibman DL, Sloan MA, Wolf A, Zeidman S (1999) Spinal epidural abscess: contemporary trends in etiology, evaluation, and mangement. Surg Neurol 52:189–196
Safran O, Rand N, Kaplan L, Sagiv S, Floman Y (1998) Sequential or simultaneous, same-day anterior decompression and posterior stabilization in the management of vertebral osteomyelitis of the lumbar spine. Spine 23:1885–1890
Sapico FL (1996) Microbiology and antimicrobial therapy of spinal infections. Orthop Clin North Am 27:9–13
Soehle M, Wallenfang T (2001) Spinal epidural abscess: clinical manifestations, prognostic factors, and outcomes. Neurosurgery 51:79–87
Tandon N, Vollmer DJ (2004) Infections of the spine and spinal cord. In: Winn HR, Dacey RG (eds) Youman’s neurological surgery, 5th edn, Vol 4, Elsevier Inc., Philadelphia, pp 4363–4394
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hempelmann, R.G., Mater, E. & Schön, R. Septic hematogenous lumbar spondylodiscitis in elderly patients with multiple risk factors: efficacy of posterior stabilization and interbody fusion with iliac crest bone graft. Eur Spine J 19, 1720–1727 (2010). https://doi.org/10.1007/s00586-010-1448-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-010-1448-0