
Abstract
Odontoid fractures are common in the elderly following minor falls. Almost all of them have osteoarthritis of the cervical spine below the axis vertebra. As a result, there is increased stress on the spared upper cervical spine, resulting in a higher incidence of injuries. As movement in the upper cervical spine involves participation of five joints, degeneration in any one particular joint may affect the biomechanics of loading of the upper cervical spine. We aimed to analyse the relationship of odontoid fractures to the pattern of upper cervical spine osteoarthritis in the elderly. We studied the CT-scan images of the cervical spine in 23 patients who were over the age of 70 years and had odontoid fractures. In each patient, the type of odontoid fracture and the characteristics of the degenerative changes in each joint were analysed. Twenty-one of 23 patients had Type -II odontoid fractures. The incidence of significant atlanto-odontoid degeneration in these individuals was very high (90.48%), with relative sparing of the lateral atlantoaxial joints. Osteoporosis was found in 13 of 23 patients at the dens-body junction and in seven of 23 patients at the odontoid process and body of the axis. With ageing, progressively more severe degenerative changes develop in the atlanto-odontoid joint. These eventually obliterate the joint space and fix the odontoid to the anterior arch of the atlas. In contrast, the lateral atlantoaxial joints are hardly affected by osteoarthritis. Thus, ultimately, atlantoaxial movements including atlantoaxial rotation are markedly limited by osteoarthritis of the atlanto-odontoid joint. However, there is still potential for movement in the lateral atlantoaxial joints, as they remain relatively free of degenerative change. The vulnerability of the atlantoaxial segment is further increased by markedly limited rotation below the axis vertebra due to severe facet-joint degeneration. As a consequence, a relatively low-energy trauma to the lateral part of the face, for instance by a fall, will induce forced atlantoaxial rotation. This, with the marked limitation of movement at the atlanto-odontoid joint, will produce a torque force at the base of the odontoid process leading to a Type II fracture.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Above the age of 70 years, fracture of the odontoid process is the most common cervical spine injury [8, 9]. Unlike the younger population, in whom odontoid process fractures are caused by high-energy injuries, in the elderly population they are frequently caused by low-energy trauma like falls [8, 10]. The classification system detailed by Anderson and D’ Alonzo for odontoid process fractures is widely accepted and describes three types of fractures [1]. Type I injuries are oblique fractures in the upper portion of the dens; Type II fractures occur at the junction of the dens with the central body of the axis; and Type III fractures are through the upper body of the axis in the cancellous bone.
The unique and complex atlantoaxial articulation includes the two lateral atlantoaxial joints and the median atlanto-odontoid joint. The tip of the odontoid process rotates on itself between the anterior arch of the atlas and the transverse ligament of the atlas. As age increases, the incidence of degeneration in the cervical spine increases. Friedenberg and Miller found roentgenographic degenerative changes in the cervical spine in 75% of individuals over the age of 60 years [2]. Zapletal et al., in their computed tomography (CT) study, showed that obliteration of the joint space in the atlanto-odontoid joint was a frequent coincidental finding in patients referred for CT examination of the brain or paranasal sinuses [16].
As there are many articulations in the upper cervical spine, each contributing to different planes of motion, degeneration and, hence, restriction of motion in any one particular joint may adversely affect the movement and distribution of force across that segment of the spine. This uneven distribution of force together with the osteoporosis may dictate the pattern of fracture of the odontoid process in the elderly.
The purpose of our study is to analyse the types of fracture of the odontoid process in the elderly and to find the relationship between the degenerative changes in different joints of the upper cervical spine and the pattern of fracture of the odontoid process.
Clinical material and methods
Between July 1999 and March 2003, 185 patients had CT scans of the cervical spine for cervical spine injuries. Twenty-three out of 47 patients over the age of 70 years had odontoid process fractures. In the remaining 24 patients, only 13 had CT scans of the upper cervical spine, as there was no indication for imaging the upper cervical spine in the others. The median age of the patients was 79 years (range 71–100). The CT examinations were performed on a GE Lightspeed scanner, using helical acquisition. Slices 1.25 mm thick with a 0.6 mm overlap with bone and standard algorithm were acquired, allowing reformatting in the sagittal, coronal and axial planes. In each scan, we studied:
-
1.
The type of fracture of the odontoid process
-
2.
The angulation of the fracture without displacement, and the amount of displacement of the fracture with or without angulation
-
3.
The severity of degeneration in each joint viz., atlanto-occipital joints, lateral atlantoaxial joints, atlanto-odontoid joint, and facet joints below the axis vertebra
-
4.
Ossification of the anterior atlanto-occipital ligament
-
5.
Evaluation of osteoporosis at the dens-body junction, and in the odontoid process and the body of axis
The fracture of the odontoid process was classified according to the recommendation by Anderson and D’ Alonzo into three types. The displacement was either anterior, posterior, or lateral, and the amount of displacement measured in millimetres. The severity of the osteoarthritis was graded as none, mild, moderate and severe in each joint. Table 1 shows the classification of the severity of degenerative changes in the atlanto-odontoid joint, and Table 2 shows the same for the atlanto-occipital and the lateral atlantoaxial joints. Ossification of the anterior atlanto-occipital membrane was noted partially or completely bridging the atlas to the basiocciput. In addition the prevalence of calcification of the transverse ligament of the atlas was evaluated. Table 3 shows the classification of the severity of osteoporosis of the axis vertebra at the dens-body junction, and in the odontoid process and the body of axis.
The statistical analysis of the obliterated atlanto-odontoid joint space between the patients with Type II odontoid fractures and the remaining patients was performed using chi-square test. While performing the statistical analysis, only moderate and severe degenerative changes were considered, as, by definition, only they had obliterated joint space.
Results
Of the 23 odontoid fractures, one was type I; 21 were type II and one was of type III. Of the 21 Type II fractures, four showed no displacement or angulation at all; nine showed posterior angulation without displacement, seven posterior displacement with or without angulation (average displacement, 3.37 mm, range 2–7 mm), six lateral angulation without displacement (four towards the right side and two towards the left side), and four showed lateral displacement with or without angulation (range 1.6–5.4 mm; two towards the right side and two towards the left side). Three patients had additional injuries of the upper cervical spine—one anterior arch fracture, one posterior arch fracture and one lateral mass fracture of the atlas.
In the remaining 13 patients, two had fractures of the anterior arch of the atlas with lateral mass fracture on the left side, and eleven patients had no bony injury.
Fig. 1 shows the degree of degenerative changes in the atlanto-occipital joints, the lateral atlantoaxial joints, the atlanto-odontoid joint and the facet joints below the level of axis vertebra in the patients with Type II odontoid fractures. Fig. 2 shows the degenerative changes in the remaining 15 patients, including the patients with Type I and Type III odontoid process fractures.

Comparison of severity of degenerative changes in different joints in the cervical spine in patients with Type II odontoid fractures

Comparison of severity of degenerative changes in different joints in the cervical spine in 15 patients with no Type II odontoid fractures (including patients with Type I and Type III odontoid fractures)
Of the 23 patients with odontoid fractures, eight showed degenerative changes in the atlanto-occipital joints on both sides, eight in the lateral atlantoaxial joints on both sides and twenty in the atlanto-odontoid joint. All the patients had degeneration of the facet joints below the level of axis vertebra.
Seventeen of the 21 patients with Type II odontoid fractures showed obliterated joint space in the atlanto-odontoid joint (Fig. 3 and Fig. 4) and two in the lateral atlantoaxial joints on both sides. Degenerative changes were absent in the atlanto-occipital and lateral atlantoaxial joints in 15 out of 21 patients. In the patient with Type III odontoid fracture, the atlanto-odontoid joint space was normal. In the patient with Type I fracture, severe atlanto-odontoid degeneration with moderate atlantoaxial and atlanto-occipital degeneration was noted.

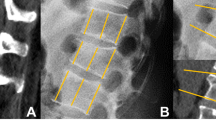
Sagittal CT reconstruction showing Type II odontoid fracture with backward displacement and backward angulation, and severe degeneration of the atlanto-odontoid joint

Axial CT scan showing severe degeneration of the atlanto-odontoid joint with complete obliteration of the joint space
In the 13 patients with no odontoid fracture, obliteration of the joint space was found in six patients in the atlanto-odontoid joint, three patients in the lateral atlantoaxial joints on both sides, four patients in the atlanto-occipital joints on both sides, and 12 patients in the facet joints below the level of axis vertebra.
Statistical analysis showed that the obliteration of atlanto-odontoid joint space was significant in patients with Type II odontoid fracture, compared with those with no Type II odontoid fracture (χ2=4.63; df=1; p<0.05).
Of the 21 patients with Type II odontoid fracture, the anterior atlanto-occipital membrane was partially ossified in 16 patients and completely ossified in four patients. In the remaining fifteen patients, anterior atlanto-occipital membrane was partially ossified in four patients and completely ossified in four. Also, alar ligament calcification was found in two patients with no odontoid fracture. Calcification of the transverse ligament was seen in six patients with Type II odontoid fracture and in one patient with no odontoid process fracture.
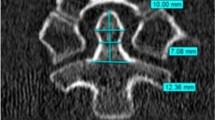
Fig. 5 shows the prevalence and severity of osteoporosis at the dens-body junction, and in the odontoid process and the body of axis in patients with Type II odontoid fracture. Fig. 6 shows the same for the remaining 15 patients. In six of 21 patients with Type II dens fracture, the loss of trabeculae in the dens-body junction (Fig. 7) was marked relative to the body and odontoid process of the axis. Severe osteoporosis was seen in the body and odontoid process of the axis in the patient with Type III dens fracture. Moderate osteoporosis was found in the entire axis vertebra in the patient with Type I fracture.

Comparison of severity of osteoporosis between the dens-body junction and the odontoid process and body of the axis in patients with Type II odontoid fractures

Comparison of severity of osteoporosis between the dens-body junction and the odontoid process and body of the axis in 15 patients with no Type II odontoid fractures (including patients with Type I and Type III odontoid fractures)

Axial CT scan at the level of dens-body junction showing absence of trabeculae (three holes), involving nearly 50% of the transverse diameter of the bone
Discussion
Type II fracture at the junction of dens and body of the axis accounts for 95% of odontoid process fractures in the elderly [8], as compared with 60% in the general population [3]. The population of the mobile elderly is rising steadily, and ,hence, the number of low-energy traumatic events resulting from accidental falls is increasing. Falls from standing or seated height can produce cervical spine injuries in the elderly, commonly involving the atlantoaxial complex [7]
The relative horizontal orientation of the facet joints between the atlas and the axis allows excellent rotation. Around 40–70% of total neck rotation takes place in the atlantoaxial articulation [5, 14]. The initial rotation is performed in the atlantoaxial articulation, and the facet joints below the level of axis vertebra contribute at the extremes of rotation. The atlantoaxial rotational movement includes not only the two lateral atlantoaxial joints but also the atlanto-odontoid joint, where the odontoid process rotates behind the anterior arch of the atlas. For a wide range of atlantoaxial rotation of 69.25° (range 45–88.5°) available in the normal person, the instantaneous axis of rotation is found to be located within the odontoid peg [12].
In the cervical spine, degenerative osteoarthritis primarily affects the facet joints below the level of the axis vertebra [2, 6]. As these segments become less mobile in the elderly, the atlantoaxial articulation becomes the most mobile portion [14]. This results in increased upper cervical spine injuries, as shown in the study of 225 cervical spine injuries in 149 consecutive patients 65 years and older, performed by Lomoschitz et al [7]. The incidence of degenerative changes in the lateral atlantoaxial joints in the normal elderly population varied from 4% to 18.2% in the literature [4, 15]. The incidence of degenerative changes in the atlanto-odontoid joint in the normal population is quite high, with 42% in the seventh decade and 60.9% in the eighth decade, resulting in obliteration of atlanto-odontoid joint space [16]. Our series showed an increased incidence of degeneration of the atlanto-odontoid joint in patients with odontoid process fractures (90.48%) as compared with the normal population. In the patients with Type II odontoid fractures, it was also noted that in nine patients with severe degeneration of the atlanto-odontoid joint (Figs. 3 and 4) there was no significant degenerative change in the lateral atlantoaxial articulations (Fig. 8). In addition, in eight patients with moderate degeneration of the atlanto-odontoid joint, only one patient had significant degeneration of the lateral atlantoaxial joints, while two others had mild degeneration of the lateral atlantoaxial joints. Interestingly, a cadaver study of cervical spine flexion–extension motion from youth to old age by ten Have [13] demonstrated general increase of atlanto-occipital motion at the expense of general decrease of atlantoaxial motion, total craniovertebral flexion–extension remaining about the same (40.3° at 15–24 years, 38.8° at 75–84 years). This decrease in atlantoaxial motion may well have been caused by atlanto-odontoid osteoarthritis, which was very evident from the elderly specimens, in contrast with the practical absence of degenerative changes of the lateral atlantoaxial joints. The above cadaveric findings are supported by the radiologic study performed by authors more recently [4, 15, 16].

Sagittal reconstruction showing preservation of the joint space in the atlanto-occipital and lateral atlantoaxial joints in the same patient as in Figs. 3 and 4. In the cervical spine proper, severe osteoarthritis of the facet joints is seen, with complete obliteration and fusion of the joint spaces
When a person falls hitting an immobile object with the side of his face, an axial rotation in the upper cervical spine is produced by the bending moment, along with the applied lateral force. Puttlitz et al. used the finite-element model to study the biomechanics of loading of the upper cervical spine to determine the various forces responsible for producing odontoid fractures [11]. They utilised the von Mises stress mapping to locate and calculate the magnitude of the maximum stresses for various force loadings in the Type I, Type II or Type III fracture region in the odontoid process [11]. They demonstrated that the finite-element model consistently implicated axial rotation in the production of high stresses in the odontoid’s Type II fracture region. Our study shows that it is likely that the degenerative cervical spine significantly alters the biomechanics of loading of the upper cervical spine in the elderly. Rotatory motion is affected in atlanto-odontoid osteoarthritis, as the tip of the odontoid is held relatively fixed by the degenerative process. If the lateral atlantoaxial joints are not affected, or only minimally affected, by osteoarthritis in an elderly patient with significant atlanto-odontoid osteoarthritis, the fall onto the side of the face initiates rotation in the lateral atlantoaxial joints, and as the tip of the odontoid is held relatively static due to the degenerative process, abnormal stress is created at the junction of body and odontoid process of the axis, in addition to the normal increased von Mises stress in the Type II fracture region of the odontoid. This results in a Type II fracture of the odontoid process and explains the higher incidence of Type II odontoid fractures in the elderly with significant atlanto-odontoid osteoarthritis even after minor falls.
The findings from our series show a definite causal relationship between the incidence of Type II odontoid fractures and the pattern of upper cervical-spine osteoarthritis. To the best of the authors’ knowledge, the significance of upper cervical-spine osteoarthritis in the incidence of Type II odontoid fractures has not been analysed until now.
Conclusions
Type II odontoid fracture is the commonest odontoid fracture in the elderly over the age of 70 years. There is a significant relationship between upper cervical-spine osteoarthritis and the incidence of Type II odontoid fractures. Significant atlanto-odontoid osteoarthritis in the presence of normal lateral atlantoaxial joints increases the risk of sustaining Type II odontoid fracture. Osteoporosis will play an additional role.
References
Anderson LD, D’Alonzo RT (1974) Fractures of the odontoid process of the axis. J Bone Joint Surg Am 56(8):1663–1674
Friedenberg ZB, Miller WT (1963) Degenerative disc disease of the cervical spine. A comparative study of asymptomatic and symptomatic patients. J Bone Joint Surg Am 45:1171–1178
Fujii E, Kobayashi K, Hirabayashi K (1988) Treatment in fractures of the odontoid process. Spine 13(6):604–609
Halla JT, Hardin JG (1987) Atlantoaxial (C1–C2) facet joint osteoarthritis; A distinctive clinical syndrome. Arthritis Rheum 30(5):577–582
Iai H, Goto S, Yamagata M et al (1993) Three-dimensional motion of upper cervical spine in rheumatoid arthritis. Spine 19:272–276
Lestini WF, Wiesel SW (1989) The pathogenesis of cervical spondylosis. Clin Orthop 239:69–93
Lomoschitz FM, Blackmore CC, Mirza SK, Mann FA (2002) Cervical spine injuries in patients 65 years old and older: epidemiologic analysis regarding the effects of age and injury mechanism on distribution, type, and stability of injuries. AJR Am Roentgenol 178(3):573–577
Muller EJ, Wick M, Russe O, Muhr G (1999) Management of odontoid fractures in the elderly. Eur Spine J 8(5):360–365
Nagashima H, Morio Y, Hasegawa K, Teshima R (2001) Odontoid fractures complicated by fractures of the posterior arch of the atlas in the elderly over 85 years with severe thoracic kyphosis secondary to osteoporosis. Injury 32(6):501–504
Pepin JW, Bourne RB, Hawkins RJ (1985) Odontoid fractures, with special reference to the elderly patient. Clin Orthop 193:178–183
Puttlitz CM, Goel VK, Clark CR, Traynelis VC (2000) Pathomechanisms of failures of the odontoid. Spine 25(22):2868–2876
Roche CJ, King SJ, Dangerfield PH, Carty HM (2002) The atlantoaxial joint physiological range of rotation on MRI and CT. Clin Radiol 57(2):103–108
ten Have HA (1978) Antero-posterior mobility and degenerative changes of the cervical spine (in Dutch). Thesis Leiden, Visdruk Alphen aan den Rijn
White AA, Panjabi MM (1978) Kinematics in spine. In: White AA, Panjabi MM (eds) Clinical biomechanics of the spine. Lippincott, Philadelphia, pp 87–125
Zapletal J, de Valois JC (1997) Radiologic prevalence of advanced lateral C1–C2 osteoarthritis. Spine 22(21):2511–2513
Zapletal J, Hekster RE, Straver JS, Wilmink JT (1995) Atlanto-odontoid osteoarthritis. Appearance and prevalence at computed tomography. Spine 20(1):49–53
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lakshmanan, P., Jones, A., Howes, J. et al. CT evaluation of the pattern of odontoid fractures in the elderly—relationship to upper cervical spine osteoarthritis. Eur Spine J 14, 78–83 (2005). https://doi.org/10.1007/s00586-004-0743-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-004-0743-z