
Abstract
As an increase in gastroesophageal reflux disease (GERD) has been reported in Japan, and public interest in GERD has been increasing, the Japanese Society of Gastroenterology published the Evidence-based Clinical Practice Guidelines for GERD (1st edition) in 2009. Six years have passed since its publication, and there have been a large number of reports in Japan concerning the epidemiology, pathophysiology, treatment, and Barrett’s esophagus during this period. By incorporating the contents of these reports, the guidelines were completely revised, and a new edition was published in October 2015. The revised edition consists of eight items: epidemiology, pathophysiology, diagnosis, internal treatment, surgical treatment, esophagitis after surgery of the upper gastrointestinal tract, extraesophageal symptoms, and Barrett’s esophagus. This paper summarizes these guidelines, particularly the parts related to the treatment for GERD. In the present revision, aggressive proton pump inhibitor (PPI) maintenance therapy is recommended for severe erosive GERD, and on-demand therapy or continuous maintenance therapy is recommended for mild erosive GERD or PPI-responsive non-erosive GERD. Moreover, PPI-resistant GERD (insufficient symptomatic improvement and/or esophageal mucosal break persisting despite the administration of PPI at a standard dose for 8 weeks) is defined, and a standard-dose PPI twice a day, change in PPI, change in the PPI timing of dosing, addition of a prokinetic drug, addition of rikkunshito (traditional Japanese herbal medicine), and addition of histamine H2-receptor antagonist are recommended for its treatment. If no improvement is observed even after these treatments, pathophysiological evaluation with esophageal impedance-pH monitoring or esophageal manometry at an expert facility for diseases of the esophagus is recommended.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With global interest in gastroesophageal reflux disease (GERD) increasing since the 1980s, efforts to formulate an international consensus about GERD have been made. The first international consensus about GERD was reached in 1988 at the Genval Workshop [1] and was reconstituted as the Montreal Definition in 2006 [2]. In the United States, the American College of Gastroenterology (ACG) assembled the ACG Guidelines in 1995 [3] and revised them in 1999 [4] and 2005 [5]. In the Asian-Pacific region, the Asian-Pacific Consensus was established in 2004 [6].
Since GERD is a disease influenced by meals and obesity, formulation of guidelines for the Japanese population was necessary in consideration of differences in dietary intake, dietary contents, and physique compared to Western populations. As GERD was also reported to be increasing in Japan, and more attention began to be directed towards GERD, the Japanese Society of Gastroenterology (JSGE) decided to draft Evidence-based Clinical Practice Guidelines for GERD in 2006. The first edition of the Evidence-based Clinical Practice guidelines for GERD, based on the evidence published from 1983 to 2007, was published in 2009. During the last 6 years, much progress and many changes have occurred in the diagnosis and treatment of GERD. Particularly, epidemiological data and information concerning adverse drug reactions have been accumulated, and a large number of papers have been published. Also, due to increasing knowledge about Barrett’s esophagus, differences between Japan and Western countries have been clarified. While newly reported evidence has been checked annually after the publication of the guidelines, and supplementation in the form of annual reviews has been made if there was evidence that delivered a major impact on clinical activities, complete revision has finally become necessary. Drafting of the present revised edition was initiated to incorporate progress in GERD research after the publication of the first edition based on the evidence published between 1983 and June 2012.
It was decided that the present edition would be drafted according to the GRADE (grading of recommendations assessment, development, and evaluation) system [7], which is becoming a new standard for the preparation of guidelines. In the GRADE system, more importance is attached to references in which evaluation items of greater clinical significance are used. Also, in the assessment of literature-based evidence, the evidence level is determined by preparing a risk of bias table to evaluate not only the research design but also research contents, such as the validity of allocation, presence or absence of blinding, number of lost cases, number of subjects, presence or absence of various biases, consistency and magnitude of the effect, and clinical significance. Moreover, it is clearly stated that not only evidence but also the patient’s preferences, feasibility, adverse events, and cost should be taken into consideration in the determination of the recommendation grade. Thus, the GRADE system is considered to be a fundamentally evidence-based, but also a flexible standard for the preparation of guidelines convenient for use in clinical situations.
Concerning clinical questions (CQs), 53 CQs about six items (epidemiology, pathophysiology, diagnosis, medical treatment, surgical treatment, postoperative esophagitis, and extraesophageal symptoms) were prepared in the first edition, but, for the revised edition, proposals of CQs concerning seven items, with the addition of Barrett’s esophagus, were evaluated by the guideline writing committee. Those that are the same as the first edition, those that needed modification, and those that should be deleted were selected first, and those that should be newly added were prepared. Attention was paid to prepare new CQs in line with the principle of PICO (patients, intervention, comparison, outcome). As a result, a total of 60 CQs consisting of five concerning epidemiology, eight concerning pathophysiology, 11 concerning diagnosis, nine concerning medical treatment, seven concerning surgical treatment, eight concerning postoperative esophagitis, six concerning extraesophageal symptoms, and six concerning Barrett’s esophagus were formulated. This addition of seven CQs made the new edition more substantial. Of these CQs, most of those related to Barrett’s esophagus were newly prepared for this revision. While the pathophysiology of postoperative esophagitis basically differs from that of GERD, many of its symptomatologic and endoscopic features are common with those of reflux esophagitis. Therefore, postoperative esophagitis, which was mentioned in the first edition of the guidelines of the JSGE, was included in the revised edition. After the original draft of CQs was determined by the guideline writing committee, it was evaluated by the guideline assessment committee, and modified by the guideline writing committee according to the comments made by the guideline assessment committee.
Thereafter, a systematic search of the literature was performed, and new references not adopted in the first edition were collected and evaluated. Concerning newly prepared and revised CQs, the literature published between 1983 and June 2012 was collected. For CQs maintained from the first edition, the literature that appeared between 2007 and June 2012 was searched. Concerning the literature collected, structured abstracts were prepared, risk of bias tables were also prepared for papers including randomized controlled trials, and they were used as references for the determination of evidence levels. In the present guidelines, some references published not in the search period (before 1982 and after July 2012) were added as necessary in the preparation of the Comments on the Statements concerning the CQ.
Next, in consideration of not only such literature-based evidence but also the patient’s preferences and feasibility, a statement concerning each CQ was prepared. The evidence level of all references related to the statement (overall evidence) and recommendation grade were determined by repeating anonymous voting after sufficient discussion among the guideline writing committee members. Then, the algorithms for the diagnosis and treatment of GERD were prepared, explanatory notes of the statements were drafted, and they were modified according to discussions by the guideline writing committee and checked by the guideline assessment committee. Subsequently, after final modifications were made by the guideline writing committee, public comments were invited from the members of the JSGE on its website. On the basis of the contributed public comments, part of the statements and comments were modified, and the revised Evidence-based Clinical Practice Guidelines for GERD were published in October 2015. All funding for guideline preparation was provided by the JSGE.
Also, in Japan, vonoprazan, a new type of potassium competitive acid blocker that can be used for initial as well as maintenance therapy for reflux esophagitis, was clinically applied. With accumulation of data and publication of papers concerning the clinical use of vonoprazan, the preparation of a supplement or early revision of the present guidelines in mind will become necessary.
This paper is the English version of the Evidence-based Clinical Practice Guidelines for GERD 2015. It presents summaries of the items of the epidemiology, pathophysiology, diagnosis, and Barrett’s esophagus and entire CQs, statements, and comments concerning medical and surgical treatment in the guidelines. By also presenting the algorithms for the diagnosis and treatment of GERD, it aims to disseminate the guidelines worldwide.
Definitions of terms used in the present guideline
GERD
GERD is a condition in which gastroesophageal reflux (GER) causes either esophageal mucosal break, or annoying symptoms, or both. It is classified into “erosive GERD” with esophageal mucosal break and “non-erosive GERD” with symptoms alone.
GER
GER is classified into “acidic-GER” and “non-acidic (weakly acidic, alkaline) GER”.
Proton pump inhibitor (PPI)-resistant GERD
Defined as a condition in which (1) esophageal mucosal break did not heal and/or (2) reflux symptoms considered to be due to GERD are not sufficiently mitigated even after oral administration of PPI at a standard dose for 8 weeks.
Postoperative esophagitis
Postoperative esophagitis includes esophagitis developed after gastrectomy (including total gastrectomy), esophagectomy, or anti-reflux operations for GERD but not after anti-obesity surgery.
Barrett’s esophagus
Presently, the definition of Barrett’s esophagus is not standardized in Japan or abroad (whether or not biopsy has been performed, length of Barrett’s mucosa, judgment about the esophagogastric junction), and standardization of definition is necessary for the future. In the present guidelines, the definition, “the esophagus with Barrett’s mucosa (columnar epithelium that extends continuously from the stomach to the esophagus regardless of the presence or absence of intestinal metaplasia)”, by the Japanese Esophageal Society (The Japanese Classification of Esophageal Cancer, 10th edn.) was applied.
Algorithms for the diagnosis and treatment of GERD
Figure 1 shows algorithms for the diagnosis and treatment of GERD. They are based on a consensus reached by the members of the guideline writing committee and the guideline assessment committee, taking into consideration statements obtained using the GRADE method.

Algorithm for diagnosis and treatment of gastroesophageal reflux disease (GERD). a Diagnosis of GERD, b initial treatment for GERD, c long-term treatment strategy for GERD and therapeutic strategy for proton pump inhibitor (PPI)-resistant GERD
Diagnosis: When GERD is suspected, the patient is clinically evaluated by a questionnaire and the PPI test. If GERD is highly suspected, two types of algorithms are proposed: (i) administration of standard-dose PPI, which is the first-line treatment option of GERD, is started first without endoscopy (therapy at clinics without endoscopy equipment), (ii) endoscopy is performed first before PPI therapy. If symptomatic resolution was obtained with PPI before endoscopy, they are regarded as transient symptoms, and treatment should be discontinued. If the symptoms persist or are relapsed, endoscopy needs to be performed. When PPI is started before endoscopy, erosive GERD and non-erosive-GERD cannot be differentiated by the endoscopy even if it is done afterward. Endoscopy before PPI is the only way to diagnose erosive GERD or non-erosive GERD.
Initial treatment: We recommend standard-dose PPI for 8 weeks as an initial treatment (Recommendation 1 (100 %), evidence level A). Additional treatments to PPI including: lifestyle modifications, alginate or antacids for temporal symptom relief (Recommendation 2 (100 %), evidence level B), and the use of a prokinetic drug, mosapride, and a traditional Japanese herbal medicine, rikkunshito (Recommendation 2 (100 %), evidence level C) are proposed.
Long-term strategy: As for a long-term strategy for GERD patients who responded to the standard dose of PPI, among the GERD patients who need long-term treatment, aggressive maintenance therapy using PPI (Recommendation 1 (100 %), evidence level B) is recommended for patients with GERD, or surgery (Recommendation 2 (100 %), evidence level B) is proposed for those with severe erosive GERD, but on-demand therapy or continuous maintenance therapy is proposed for those with mild erosive GERD (Recommendation 2 (100 %), evidence level B) or PPI-responsive non-erosive GERD (Recommendation 2 (92.3 %), evidence level B).
Therapeutic strategy for PPI-resistant GERD: For those symptoms and/or mucosal breaks refractory to 8 weeks of standard regiment of PPI, we recommend twice dosing of the standard PPI regimen (Recommendation 1 (92.3 %), evidence level: A). Also, changing the type of PPI, additional administration of a prokinetic drug (mosapride), additional administration of a traditional Japanese herbal medicine (rikkunshito), and additional administration of a histamine H2-receptor antagonist (H2RA) before sleep are proposed (Recommendation 2 (100 %), evidence level C).
If the condition persists after these treatments, evaluation of pathophysiology by esophageal multi-channel impedance and pH monitoring and/or esophageal manometery are recommended to see the relationship between symptoms and esophageal pathophysiology. If a relationship between GER and symptoms has been established, medical treatment by an expert or surgical treatment is an alternative.
Summary of epidemiology
The prevalence of erosive GERD in Japanese was approximately 10 % [8–10] in studies involving 1000 or more subjects after 2008. Although only a small number of reports described the endoscopic severity of erosive GERD, the frequency of severe erosive GERD (grade C or D of Los Angeles (LA) classification) cases was reported to be only 3 % [9], similar to that in previous reports, and the prevalence of GERD has been reported to reach an about two times higher level when heartburn symptoms are taken into account in the diagnosis [11].
In a systematic review [12] of changes in the prevalence of GERD in Japanese, the prevalence of GERD on endoscopy in outpatients was 1.6 % in the 1980s, but it started to rise in the latter half of 1990 and reached 13.1 % in 2000 to 2010. The rate of health check-up examinees with GERD symptoms was 10.3 % in the 1990s, but it increased to 18.9 % in 2000–2010, suggesting that the prevalence of GERD is increasing in Japanese.
Regarding factors related to the prevalence of GERD, a significantly higher BMI in erosive GERD patients than in control groups has been reported, but BMI was not associated in non-erosive GERD [10, 13]. In addition, the incidence of hiatal hernia in erosive GERD was high in many reports [12, 13], and the odds ratio of hiatal hernia in erosive GERD patients was significantly higher on multivariate analysis [10, 13], suggesting a close association between erosive GERD and hiatal hernia.
Summary of pathophysiology
Esophageal mucosal break in erosive GERD was characterized by excessive esophageal acid exposure and esophageal acid exposure significantly increased according to the severity of erosive GERD [14–16]. The main mechanisms of day- [17] and night-time [18] acid-GER are transient lower esophageal sphincter (LES) relaxation (abrupt LES relaxation not accompanied by swallowing) in both healthy subjects and reflux esophagitis patients. The main mechanism of acidic-GER is transient LES relaxation in healthy subjects [14, 17] and most mild erosive GERD patients [14], whereas acid-GER due to low LES pressure is also observed in severe erosive GERD patients [14, 17].
Primary peristalsis is important for acid clearance from the esophagus and its impairment causes excessive esophageal acid exposure. The presence of esophageal hiatal hernia also increases acidic-GER due to low LES pressure [19] and impairs esophageal acid clearance [20], inducing excessive esophageal acid exposure.
Non-erosive GERD patients have some clinical characteristics, such as more frequent in females, less complicated by hiatal hernia, and lower patients’ body weight compared to erosive GERD [21]. In the esophageal motor function study, a defective triggering of secondary peristalsis in non-erosive GERD patients is observed, compared to that in healthy subjects [22]. Regarding studies on GER, the esophageal impedance and pH monitoring contributed to the elucidation of the pathophysiology of non-erosive GERD, and it has been reported that not only acid-GER but also non-acid-GER is associated with the development of reflux symptoms [23], and proximal GER is likely an important factor in symptomatic GER [24].
Esophageal perception, it has been reported that symptoms in response to acid and saline infusion into the esophagus were severer in non-erosive GERD than erosive GERD patients [25, 26], and they were hypersensitive to acid infusion into the proximal esophagus [27], indicating the presence of esophageal hypersensitivity in non-erosive GERD patients.
Associations between esophageal hypersensitivity, increase in transient receptors potential vanilloid 1 (TRPV1) expression, and dilated intercellular space in non-erosive GERD patients have been reported. Some non-erosive GERD patients may have the pathophysiology of a mild type of erosive GERD, however, there is a certain group of non-erosive GERD patients with a heterogeneous pathophysiology different from the mild type of erosive GERD.
Summary of diagnosis
The typical symptoms of GERD are heartburn and regurgitation, but patients may not necessarily accurately understand their symptoms [28]. Thus, in addition to asking typical symptoms of GERD, a careful interview with different expressions may be helpful. GER may cause not only typical symptoms but also extraesophageal symptoms (chronic cough, bronchial asthma, discomfort of the pharyngolarynx, pharyngalgia, and non-cardiac chest pain). Since extraesophageal symptoms may be the only symptoms of GER, it is important to take them into consideration when diagnosing GERD.
The LA classification is widely used to evaluate mucosal break because it covers response to treatment, and correlation with the risk of recurrence during PPI maintenance therapy [16, 29, 30]. However, symptoms are not severe despite severe reflux esophagitis being observed on endoscopy in some cases. Therefore, severity judgment based on the symptoms alone should be carefully performed [31].
Other diagnostic methods of GERD include self-administered questionnaires. The mean sensitivity and specificity of the diagnosis of GERD made using them has been reported to be approximately 70 %, and they are useful to make the initial diagnosis of GERD and judge the treatment effect [32, 33]. The PPI test is also useful to diagnose GERD and extraesophageal symptoms. The sensitivities for erosive GERD [34] and non-erosive GERD [35] treated with a high dose of PPI were 74 and 66 %, respectively. In a meta-analysis of studies in which GERD patients were diagnosed based on 24-h esophageal pH monitoring [36], the sensitivity and specificity were 78 and 54 %, respectively, showing its usefulness to make the initial diagnosis of GERD and judge the treatment effect. However, the dose and duration of administration of PPI for the PPI test have not been standardized.
As pathogenesis of PPI-resistant GERD, several factors are proposed in addition to insufficient inhibition of gastric acid secretion. Proposed factors are: non-acidic GER [23], eosinophilic esophagitis, esophageal motility disorders [37], functional heartburn, and psychological factors [38]. Esophageal impedance combined with pH monitoring might be helpful for evaluating pathophysiology.
Summary of Barrett’s esophagus
The definition of Barrett’s esophagus has yet to be standardized internationally. The presence of specialized intestinal metaplasia is considered an essential condition of Barrett’s esophagus in Western countries except the United Kingdom.
In Japan, the definition of Barrett’s esophagus by the Japanese Esophageal Society (The Japanese Classification of Esophageal Cancer, 10th edn) is well accepted: ‘Barrett’s esophagus represents an esophagus in which Barrett’s mucosa (columnar epithelium that continues from the stomach to esophagus regardless of the presence or absence of intestinal metaplasia) is present’. The reasons for the absence of a standard definition of Barrett’s esophagus are differences in the endoscopic diagnosis of the esophago-gastric junction (EGJ) and the length of Barrett’s mucosa, which is diagnosed as Barrett’s esophagus in Japan and abroad, in addition to the presence or absence of specialized intestinal metaplasia on biopsy. In Japan, the landmark of the EGJ in endoscopic diagnosis is the distal end of the palisade vessels, whereas the endoscopic landmark for EGJ in Western consensus is defined as the proximal margin of the gastric fold in a minimally distended condition.
The national prevalence of Barrett’s esophagus in Japan is not reported yet. The subjects for annual health check-ups by employers or the local government show conflicting data, especially for short-segment Barrett’s esophagus. The mean prevalence of short-segment Barrett’s esophagus, < 3 cm in length, is 17.9 % (1.2–59.0 %). This indicates that each endoscopist may have a different diagnostic definition in the measurement of the length. Mean prevalence of long-segment Barrett’s esophagus, 3 cm or more, is 0.4 %, varying from 0.2 to 1.4 %.
In Western countries, the incidence of Barrett’s adenocarcinoma has been dramatically rising in the last 25 years, climbing more than sixfold [39], and the proportion among all esophageal malignancies might exceeded 50 %, especially among male Caucasians. On the other hand, 95 % or more of esophageal malignancies in Japan is reported to be squamous cell carcinoma, and adenocarcinoma is still rare. However, the number of adenocarcinomas of the esophagus are gradually increasing in Japan. Endoscopic follow-up of Barrett’s esophagus may also be useful based on reports from Western countries, but the incidence of carcinogenesis is markedly lower than that in Western countries, and the accurate incidence is unclear. Therefore, at present, the necessity of endoscopic follow-up for Japanese Barrett’s esophagus patients is unclear.
Medical treatment
CQ: What are the purpose and endpoint of management of GERD patients?
-
The main purpose of long-term management of GERD patients is to prevent complications, in addition to control symptoms and to improve patients’ health-related quality of life (HR-QOL). Prevention of acid regurgitation improves QOL of GERD patients.
Comments:
-
(1)
Symptoms of GERD and HR-QOL
Either by medical treatment or surgical treatment, QOL of GERD patients improves after complete control of GERD symptoms [40–42]. When GERD symptoms disappear, QOL of GERD patients improves to a level equal to or above that of healthy subjects [4]. Manifestation of symptoms once or more times a week seriously influences QOL of GERD patients. Full disappearance of symptoms is important to improve QOL [43]. As to medical treatment, PPIs are more effective in improving QOL than H2RAs or prokinetic drugs [44, 45]. Acid regurgitation during night-time could induce sleep disturbance and non-cardiac pain. Heartburn at night-time is one of the most serious causes of QOL impairment [46]. When night-time acid regurgitation is controlled by PPI administration, patients’ HR-QOL is improved through improved sleep disturbance and absence of chest pain [47].
-
(2)
GERD treatment and prevention of complications
The main goals of GERD treatment are to heal mucosal break, relieve symptoms, maintain remission, improve HR-QOL, and prevent complications. GERD patients with severe reflux esophagitis or complications, such as peptic stricture, should be treated and maintained by PPIs [48]. Complications of GERD include anemia, bleeding, esophageal stenosis, Barrett’s esophagus, and adenocarcinoma [49]. Anemia, bleeding, and esophageal stenosis are serious complications of esophagitis caused by esophageal erosion or ulcer. Effective and strong acid suppression induces rapid healing of esophagitis and protects from complications because the severity of reflux esophagitis is correlated with the duration of esophageal acid exposure [50]. Therefore, PPI administration is required in GERD patients with complications. The most serious complication of GERD is adenocarcinoma. Adenocarcinoma is quite rare among Japanese GERD patients, whereas the incidence has doubled during the past 20 years and has become more prevalent than squamous cell carcinoma in Europe and the United States [49]. GERD increases the risk for esophageal adenocarcinoma. Among symptoms, the duration, severity and frequency of heartburn are reported to be independent risk factors for adenocarcinoma [49]. Patients complicated by severe heartburn for more than 20 years have a relative risk of adenocarcinoma 43.5 times higher than that of patients with no symptoms [51]. However, no report has indicated that either medical or surgical treatment can restrain the risk of adenocarcinoma in GERD patients [49, 51].
CQ: Is lifestyle modification effective for the treatment of GERD?
-
Lifestyle modification along with PPI therapy is effective because lifestyle factors cause acid GER. However, there is little evidence that lifestyle modification alone improves reflux symptoms.
Comment: Tobacco, chocolate, carbonated beverages, alcohol, and fatty foods may reduce LES pressure and/or prolong acid exposure duration [52]. Right lateral decubitus or recumbent position also either reduce LES pressure or prolong acid exposure time [52]. Clinical experience shows that tobacco, alcohol, and recumbent position exacerbate reflux symptoms [52]. Lifestyle intervention studies have shown that left lateral decubitus raises LES pressure, and that body weight reduction and head-of-bed elevation reduce the duration of esophageal acid exposure and improve reflux symptoms [52]. Lifestyle modification alone does not improve symptoms satisfactorily, but those who have lifestyle modification along with PPI therapy may have a significant improvement in reflux symptoms and HR-QOL [53].
CQ: Is an acid suppressant effective for the treatment of GERD?
-
A potent acid suppressant is recommended for the treatment of GERD because of its efficacy.
Comment: The degree of esophageal mucosal injury of erosive GERD patients depends on the duration of esophageal acid exposure and pH of the refluxate [54]. Treatment with a more potent and more sustained acid suppressant is associated with higher healing rates and faster symptom relief [54–56]. PPIs are significantly more effective than H2RAs [54–56]. However, there are still unmet clinical needs. More prompt and full 24-h control of gastric acid secretion might lead to more efficacious clinical improvement.
PPIs are the most effective drugs in non-erosive GERD treatment [57], but the symptomatic response rate for PPI therapy in patients with non-erosive GERD has been approximately 20 % lower than that in patients with erosive GERD [58]. It is thought that various patient conditions, such as heartburn by non-acid GER or functional heartburn without GER, are present in non-erosive GERD without mucosal break [59].
CQ: Are sodium alginate and antacid effective for the treatment of GERD?
-
Sodium alginate and antacid are effective for temporary improvement of GERD symptoms, and we recommend the use of these drugs for GERD patients.
Comment: The significant inhibition effect of sodium alginate for GER has been demonstrated [60–62], and the drug is effective for GERD symptoms [63–66]. However, to achieve effective results, it is necessary to use the drug more than four times a day. Thus, the drug is not suitable for severe cases [65]. Though the endoscopic healing rate for erosive GERD by frequent dosing of antacid has been reported to be no better than placebo [67, 68], the relief rate for GERD symptoms is significantly better than that of a placebo [63, 69]. Antacid is a neutralizer of acid and is effective immediately. Even a large amount of antacid does not maintain a neutralizing effect of more than 30 min, as continuously secreted gastric acid overweighs its neutralizing effect [64]. Therefore, antacid alone for patients with frequent symptoms and impaired HR-QOL is unrealistic.
CQ: Are PPIs the first-line drugs in the treatment of GERD?
-
As the primary treatment of GERD, PPIs have a superior effect on symptom resolution and mucosal healing over other drugs and are cost-effective. PPIs are recommended as the first-line drugs in the treatment of GERD.
Comment: PPIs have a superior effect in terms of heartburn symptom relief and mucosal healing over H2RAs and prokinetic drugs for the primary treatment of erosive GERD [55, 70, 71]. PPIs are more cost-effective for the treatment of GERD than H2RAs or step-up therapy starting from H2RA [72, 73]. PPIs have a superior effect in terms of heartburn symptom relief over H2RAs or alginate for the treatment of GERD diagnosed by symptoms [66, 74]. PPIs have a superior effect in terms of heartburn symptom relief than H2RAs or prokinetic drugs for the treatment of non-erosive GERD [75]. The addition of a prokinetic drug, mosapride, to omeprazole is not more effective than omeprazole alone for the treatment of non-erosive GERD [76].
Among PPIs, the treatment efficacy is not different, and the potential at the onset of GERD symptom relief during the early days of treatment might not be different, but the data are controversial [55, 77, 78]. Therapeutic efficacy of 8 weeks of PPI (lansoprazole and omeprazole) in severe esophagitis is weaker than that in mild esophagitis [79]. Therapeutic efficacy of lansoprazole, and probably of omeprazole, on mucosal healing of erosive GERD may be influenced by patients’ CYP2C19 genotype [80, 81].
CQ: Are there any medications, such as prokinetic drugs or traditional Japanese herbal medicines, which are expected to have additional benefits with a PPI in the treatment of GERD?
-
There is no evidence which shows the efficacy of prokinetic drugs or traditional Japanese herbal medicine alone; however, some medications with a PPI are reported to provide an additional benefit in the improvement of GERD symptoms. Therefore, their use with a PPI has been proposed.
Comment: There has been no report that has recommended the use of prokinetic drugs or traditional Japanese herbal medicine alone for the treatment of GERD [55]. The standard dose of a PPI plus cisapride (withdrawn from clinical use due to a cardiac adverse effect) is reported to have no significant additional benefit in curing or relieving symptoms of GERD [82]. A Japanese study showed the possibility of an additional benefit of mosapride with a PPI [76]. Combination therapy of rikkunshito, a traditional Japanese herbal medicine, with the standard dose of a PPI is reported to have an equivalent effect of a double dose of a PPI in PPI-resistant GERD patients, showing a possible additional benefit of rikkunshito [83]. Adding these prokinetic drugs or traditional Japanese herbal medicines to a PPI is of significance when a PPI alone does not have a satisfactory effect.
CQ: What should be done if the effect of a PPI is insufficient at the standard dose?
-
To those who did not respond to standard PPI treatment either in healing of mucosal break or intense symptoms, a double dose of PPI twice a day is recommended.
-
To those who did not respond to standard PPI treatment, there are options to switch to another PPI or addition of prokinetic drug, mosapride, or a Japanese herbal medicine, rikkunshito, or add on of H2RA before bedtime.
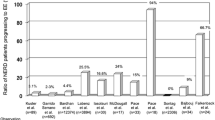
Comment: Persistent and intense GERD symptoms despite PPI therapy have a significant and negative impact on both QOL and healthcare resource utilization [84]. A randomized clinical trial (RCT) from Japan revealed that rabeprazole at 20 mg and 10 mg twice dosing for 8 weeks is more effective than 20 mg once dosing in resolution of persistent symptoms and endoscopically confirmed healing in patients with erosive GERD refractory to a standard PPI [84]. Addition of an H2RA before bedtime with a PPI is known to reduce nocturnal acid breakthrough. This treatment is effective for long-term control of refractory reflux esophagitis [85]. In contrast, in a study using pH testing, this impact rapidly disappeared in 1 week because of H2RA tachyphylaxis [86]. There have been some open-label RCTs for refractory GERD as described below. A study reported that two different kinds of double-dose PPIs are equally effective in patients refractory to a standard-dose PPI [87]. A study from Japan concluded that rikkunshito combined with standard-dose PPI therapy is equally effective to a double-dose PPI; however, in subgroup analysis between erosive and non-erosive GERD, rikkunshito was more efficacious in male non-erosive GERD than the other groups [83]. Symptoms refractory to standard PPI may improve with increasing the dose of PPI [88], switching to other PPI [89], addition of mosapride [90], or baclofen [91].
RCT conducted in Japan with rebamipide to PPI refractory NERD did not show superiority to placebo in symptomatic resolution. Observational studies from Japan showed symptomatic improvement with dosing increase of PPI, and also mosapride added on standard PPI dosing [92, 93].
For the evaluation of the origin of PPI refractory GERD symptoms, pathophysiological investigation under sufficient medication should be performed.
CQ: What is the long-term treatment strategy for GERD? Should we use maintenance, intermittent, on-demand, or step-down therapy?
-
PPI maintenance therapy is the most efficient and cost-effective. PPIs are recommended for maintenance therapy for GERD (Recommendation 1 (100 %), evidence level A)
-
Affirmative PPI maintenance therapy is recommended for severe erosive GERD (Recommendation 1 (100 %), evidence level B)
-
Some patients with mild erosive GERD are well controlled by on-demand therapy with a PPI. For long-term management, the dosage of PPI should be minimized as much as possible with careful symptom evaluation (Recommendation 2 (100 %), evidence level B)
-
On-demand therapy with a PPI for the long term is proposed for patients with non-erosive GERD responding to a PPI as an initial therapy (Recommendation 2 (92.3 %), evidence level B)
-
The view of patients on efficacy, safety, cost, preference of medication and frequency should be taken in consideration in long-term strategies (Recommendation 2 (100 %), evidence level C).
Comment: PPIs are recommended for maintenance therapy of GERD because PPI maintenance therapy is the most cost-effective therapy both in symptomatic and endoscopic improvement in GERD [94–97]. Among GERD patients, affirmative PPI maintenance therapy is mandatory to control patients with severe erosive GERD, because it is liable to recur without such therapy [98, 99]. On the other hand, some patients with mild reflux esophagitis and some patients with non-erosive GERD responding to a PPI as an initial therapy are well controlled by on-demand therapy with a PPI [100–104]. Therefore, the dose of PPI should be limited to as minimal as required in the long-term management of GERD, especially in the viewpoint of medical economics [105–109]. Furthermore, consideration of the patient’s view on treatment efficacy, safety, cost, preference of medication, and frequency should be taken in long-term strategies. Reports on patients’ satisfaction show that PPIs are superior to other strategies both in initial and long-term treatment [110, 111].
CQ: What are the potential risks of long-term acid inhibition? What is the overall safety of long-term PPI therapy?
-
Maintenance treatment with PPIs is generally safe. However, careful observation is mandatory in long-term use. We propose that PPIs should be administered at the lowest effective dose. (Recommendation 2 (84.6 %), evidence level C)
Comment: Concerns continue to be expressed about potential adverse effects of PPI therapy due to its potent acid suppressing effect, especially in long-term use.
-
(1)
Gastric carcinoid tumors
A few cases in which carcinoid tumors were detected after the initiation of PPI therapy have been reported [112, 113]. However, causal association is unclear. There is no evidence to support increased incidence of carcinoid tumors in long-term PPI therapy [114, 115].
-
(2)
Gastric cancer
In the presence of H. pylori, PPIs will enhance the development of corpus-predominant gastritis and possibly accelerate development of atrophic gastritis. Eradication of H. pylori induces regression of gastritis and possibly of atrophy without stopping PPIs [116, 117]. However, there is no evidence of an increased incidence of gastric cancer related to PPI use either with or without H. pylori [118, 119]. Whether H. pylori infection should be screened for before starting PPI therapy remains controversial.
-
(3)
Colorectal cancer
Hypergastrinemia may increase the risk of colorectal cancer. However, case–control studies have not identified an increased risk with PPI use [120, 121].
-
(4)
Enteric infection
A systematic review [122] showed that PPI use is associated with an increased risk of bacterial enterocolitis (pooled OR = 3.33; 95 % CI = 1.84–6.02). Another systematic review [123] demonstrated that PPI use is associated with an increased risk of Clostridium difficile infection (pooled OR = 2.15; 95 % CI, 1.81–2.55). Although the absolute risks appear to be small, PPIs should be used with care in patients with risks.
-
(5)
Community-acquired pneumonia
A systematic review [124] showed that current PPI use is associated with an increased risk of community-acquired pneumonia (CAP) (pooled OR = 1.39; 95 % CI = 1.09–1.76). Short duration of use is associated with an increased risk (pooled OR = 1.65; 95 % CI = 1.25–2.19), whereas chronic use is not (pooled OR = 1.10; 95 % CI = 1.00–1.21). Association of PPI use and CAP may have been confounded by the presence of GERD as a reason for PPI therapy.
-
(6)
Calcium and bone fracture
A systematic review [125] showed that PPI use is associated with an increased risk of hip fracture (pooled OR = 1.25; 95 % CI = 1.14–1.72) and spine fracture (pooled OR = 1.50; 95 % CI = 1.32–1.72). With regard to hip fracture, short duration of use (<1 year) is associated with a significantly increased risk (pooled OR = 1.24; 95 % CI = 1.19–1.28), whereas long-term use (3–10 years) is not (pooled OR = 1.30; 95 % CI = 0.98–1.70). PPI therapy may increase the risk slightly. The risk of osteoporosis and hip fracture is substantial in elderly patients irrespective of PPI use.
-
(7)
Microscopic colitis
Microscopic colitis (MC) [collagenous colitis (CC)/lymphocytic colitis (LC)] causes diarrhea. Cases of CC related to the use of lansoprazole have been increasingly reported, especially in Japan [126–128]. In CC patients in Japan, 51.1–69.8 % [126, 127] are reported to take lansoprazole with some reason, and discontinuation of lansoprazole resolved the CC in 90.4 % of patients [126]. A case–control study [129] showed that PPI use is associated with an increased risk for MC. When seeing an intractable diarrhea patient under PPI medication, especially lansoprazole, MC (CC/LC) should be considered as a differential diagnosis. Discontinuation or a switch to another PPI may resolve the MC symptoms.
-
(8)
Concomitant use with clopidogrel
The competition of clopidogrel with a PPI at CYP2C19 may reduce the biological activity of clopidogrel. Early retrospective studies showed conflicting results, with some studies suggesting an increased risk of cardiovascular events and others showing a lack of effect. However, prospective studies [130, 131] and RCTs [132–134] have not identified an increased risk with PPI use. A systematic review [135] indicated that the data from RCTs do not support an adverse effect, and that confounding factors may explain the differences in results between observational studies.
-
(9)
Other potential risks
There have been case reports regarding the deficiency of vitamin B12, iron, or magnesium associated with PPI use [136]. However, true incidences and causal associations are unclear. Several studies have suggested the development of gastric fundic gland polyp during PPI therapy [137, 138]. However, a causal relationship is unclear, and the clinical significance appears to be limited.
The benefits of PPI treatment seem to outweigh the above-mentioned potential risks in the large majority of patients if PPI use is based on appropriate indications. The clinical risk/benefit should be evaluated for each patient, and PPIs should be used at the lowest effective dose.
Anti-reflux surgery
CQ: Who should have anti-reflux surgery?
-
Anti-reflux surgery is recommended for PPI-resistant GERD patients (Recommendation 2 (100 %), evidence level B)
-
Anti-reflux surgery is proposed for erosive GERD patients on long-term PPI treatment (Recommendation 2 (100 %), evidence level C)
Comment: Anti-reflux surgery may be indicated to GERD patients who are refractory to medication with lifestyle modification. Many reports discussed the indication of anti-reflux surgery to PPI-refractory GERD [139, 140].
-
A majority of the papers show the superiority of anti-reflux superiority over PPI treatment, while some report conflicting results, suggesting publication bias on this topic. We need more intensive surveys.
Although PPI is effective for many GERD patients, long-term treatment is necessary for most patients. Recent studies compared therapeutic efficacies between long-term PPI medication and laparoscopic anti-reflux surgery, leading to the conclusion of the superiority of surgical approaches in the majority of cases [141, 142]. Recent studies also seek risk factors for the post-operative recurrence of GERD [143, 144]. The majority of papers show the superiority of anti-reflux surgery over PPI treatment, while some report conflicting results, suggesting publication bias on this topic [145]. We need a more intensive survey.
CQ: Is the long-term outcome of antireflux surgery better than that of PPI treatment?
-
Laparoscopic fundoplication for erosive GERD significantly improves QOL scores and symptoms for at least 1 year more than PPI treatment (Recommendation NA, evidence level B)
Comment: In Western countries, there have been many clinical trials that compared treatment effects between medication and laparoscopic surgery [146]. In a systematic review, laparoscopic fundoplication significantly improved QOL scores and symptoms for at least 1 year [147]. Moreover, airway symptoms and sleeping difficulties associated with GERD symptoms [148], acid reflux in esophageal impedance-pH monitoring [149, 150], intestinal metaplasia in Barrett’s esophagus on endoscopy [149], and bile reflux [150] were also significantly improved by laparoscopic fundoplication compared to medication.
CQ: Is the cost-effectiveness of surgical treatment better than that of PPI treatment?
-
The cost-effectiveness of surgical treatment is sometimes better than that of medical therapy. Because outcomes depend heavily on the method of investigation, the medical insurance system, and drug costs, this issue is now controversial (Recommendation NA, evidence level B)
Comment: In Western countries, comparative studies on the cost-effectiveness of both treatments have been performed [151], but it has not been sufficiently investigated in Japan [152]. In an RCT comparing laparoscopic fundoplication and PPI treatment [152], it was suggested that the cost-effectiveness of laparoscopic surgery for GERD with long-term medication is better than that of medical therapy. Nevertheless, outcomes of comparative studies on cost-effectiveness depend on the method of investigation, the medical insurance system, and drug costs. This issue is now controversial.
CQ: Is the outcome of antireflux surgery influenced by surgeons’ experience and skill?
-
The outcome of antireflux surgery is sometimes influenced by surgical experience and skill (Recommendation NA, evidence level C)
Comment: Anti-reflux surgery requires knowledge and trained skills. However, skill levels vary from surgeon to surgeon. A direct study has not been conducted on this topic. The recent introduction of endoscopic surgery, in which views of the surgical field can be shared and recorded, has made surgical procedures reproducible and various technical assessments possible. Regarding antireflux surgery in particular, reports discussing the results of the acquisition of skills from the viewpoint of a learning curve have also appeared. However, there have not been any reports with a high evidence level. One paper reported that the clinical outcome of antireflux surgery is influenced by the learning curve [153], and other reports have found no significant differences [154–157].
CQ: Is laparoscopic fundoplication useful compared with open fundoplication?
-
Laparoscopic fundoplication is more useful than open fundoplication, and is recommended (Recommendation 1 (100 %), evidence level A)
Comment: Most recent anti-reflux surgeries have been performed laparoscopically, although the open approach was more prevalent previously. Laparoscopic fundoplication has been shown not only to reduce postoperative pain, shorten the hospital stay, promote early return to normal life, and reduce the overall cost, but also to enable sharing of views of the surgical field and improves safety [158–162]. There have been no randomized clinical trials in Japan, but the findings of Western countries are generally applicable to Japan.
CQ: Is Nissen fundoplication superior to Toupet fundoplication as an antireflux surgery?
-
Nissen fundoplication, full circumferential, is better for prevention of GER, while Toupet fundoplication, 3/4 circumferential, is better in avoiding the early postoperative complications of dysphagia and bloating. The early clinical outcome of Toupet fundoplication is superior to that of Nissen fundoplication, but longer follow-up data are needed to confirm its long-term outcome (Recommendation NA, evidence level A)
Comment: The goal for anti-reflux surgery is to achieve secure antireflux effects and minimize complications such as dysphagia and bloating. Two meta-analysis showed no significant difference between two procedures in terms of anti-reflux effect, but less postoperative dysphagia and bloating with Toupet fundoplication compared to Nissen fundoplication [163, 164]. In addition, there are no significant differences in long-term outcome over 5 years between these procedures [165]. Laparoscopic Toupet fundoplication is proposed as a standard procedure for antireflux surgery.
CQ: Is endoscopic treatment effective for GERD?
-
Various methods of endoscopic treatment for GERD have been proposed. Most of them have been shown to be safe and effective. Although the long-term outcome is still unclear, short-term effectiveness was confirmed (Recommendation NA, evidence level B)
Comment: Endoscopic treatments for GERD have been actively performed in Western countries since 2003. They are classified into three categories. The first is a method to generate plication on cardia [166–170]. The second involves alteration of muscle layer on LES [171], and the third involves insertion of foreign bodies into LES [172, 173]. The short-term effectiveness of most of these techniques has been confirmed, but the long-term outcome is still unclear. Long-term follow-up for these techniques and development of novel methods which are safe and effective are necessary.
References
Dent J, Brun J, Fendric AM, et al. An evidence-based appraisal of reflux disease management the Genval Workshop Report. Gut. 1998;44(Suppl 2):S1–16.
Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–20.
DeVault KR, Castell DO. Guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Practice Parameters Committee of the American College of Gastroenterology. Arch Intern Med. 1995;155:2165–73.
DeVault KR, Castell DO. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. The Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol. 1999;94:1434–42.
DeVault KR, Castell DO. American College of Gastroenterology Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Am J Gastroenterol. 2005;100:190–200.
Fock KM, Talley N, Hunt R, et al. Report of the Asia-Pacific consensus on the management of gastroesophageal reflux disease. J Gastroenterol Hepatol. 2004;19:357–67.
Yoshida M, Kinoshita Y, Watanabe M, JSGE Clinical Practice Guidelines. standards, methods, and process of developing the guidelines. J Gastroenterol. 2014;2015(50):4–10.
Mizuta A, Adachi K, Furuta K, et al. Different sex-related influences of eating habits on the prevalence of reflux esophagitis in Japanese. J Gastroenterol Hepatol. 2011;26:1060–4.
Yasuhara H, Miyake Y, Toyokawa T, et al. Large waist circumference is a risk factor for reflux esophagitis in Japanese males. Digestion. 2010;81:181–7.
Murao T, Sakurai K, Mihara S, et al. Lifestyle change influences on GERD in Japan: a study of participants in a health examination program. Dig Dis Sci. 2011;56:2857–64.
Kusano M, Kouzu T, Kawano T, et al. Nationwide epidemiological study on gastroesophageal reflux disease and sleep disorders in the Japanese population. J Gastroenterol. 2008;43:833–41.
Fujiwara Y, Arakawa T. Epidemiology and clinical characteristics of GERD in the Japanese population. J Gastroenterol. 2009;44:518–34.
Mishima I, Adachi K, Arima N, et al. Prevalence of endoscopically negative and positive gastroesophageal reflux disease in the Japanese. Scand J Gastroenterol. 2005;40:1005–9.
Iwakiri K, Kawami N, Sano H, et al. Mechanisms of excessive esophageal acid exposure in patients with reflux esophagitis. Dig Dis Sci. 2009;54:1686–92.
Adachi K, Fujishiro H, Katsube T, et al. Predominant nocturnal acid reflux in patients with Los Angeles grade C and D reflux esophagitis. J Gastroenterol Hepatol. 2001;16:1191–6.
Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut. 1999;45:172–80.
Hayashi Y, Iwakiri K, Kotoyori M, et al. Mechanisms of acid gastroesophageal reflux in the Japanese population. Dig Dis Sci. 2008;53:1–6.
Kuribayashi S, Kusano M, Kawamura O, et al. Mechanism of gastroesophageal reflux in patients with obstructive sleep apnea syndrome. Neurogastroenterol Motil. 2010;22(611–7):e172.
van Herwaarden MA, Samsom M, Smout AJPM. Excess gastroesophageal reflux in patients with hiatus hernia is caused by mechanisms other than transient LES relaxations. Gastroenterology. 2000;119:1439–46.
Sloan S, Kahrilas PJ. Impairment of esophageal emptying with hiatal hernia. Gastroenterology. 1991;100:596–605.
Fass R. Erosive esophagitis and nonerosive reflux disease (NERD): comparison of epidemiologic, physiologic, and therapeutic characteristics. J Clin Gastroenterol. 2007;41:131–7.
Iwakiri K, Hayashi Y, Kotoyori M, et al. Defective triggering of secondary peristalsis in patients with non-erosive reflux disease. J Gastroenterol Hepatol. 2007;22:2208–11.
Iwakiri K, Kawami N, Sano H, et al. Acid and non-acid reflux in Japanese patients with non-erosive reflux disease with persistent reflux symptoms, despite taking a double-dose of proton pump inhibitor: a study using combined pH-impedance monitoring. J Gastroenterol. 2009;44:708–12.
Iwakiri K, Sano H, Tanaka Y, et al. Characteristics of symptomatic reflux episodes in patients with non-erosive reflux disease who have a positive symptom index on proton pump inhibitor therapy. Digestion. 2010;82:156–61.
Miwa H, Minoo T, Hojo M, et al. Oesophageal hypersensitivity in Japanese patients with non-erosive gastro-oesophageal reflux diseases. Aliment Pharmacol Ther. 2004;20(Suppl 1):112–7.
Nagahara A, Miwa H, Minoo T, et al. Increased esophageal sensitivity to acid and saline in patients with nonerosive gastro-esophageal reflux disease. J Clin Gastroenterol. 2006;40:891–5.
Thoua NM, Khoo D, Kalantzis C, et al. Acid-related oesophageal sensitivity, not dysmotility, differentiates subgroups of patients with non-erosive reflux disease. Aliment Pharmacol Ther. 2008;27:396–403.
Manabe N, Haruma K, Hata J, et al. Differences in recognition of heartburn symptoms between Japanese patients with gastroesophageal reflux, physicians, nurses, and healthy lay subjects. Scand J Gastroenterol. 2008;43:398–402.
Ghoshal UC, Chourasia D, Tripathi S, et al. Relationship of severity of gastroesophageal reflux disease with gastric acid secretory profile and esophageal acid exposure during nocturnal acid breakthrough: a study using 24-h dual-channel pH-metry. Scand J Gastroenterol. 2008;43:654–61.
Fujimoto K, Hongo M. Risk factors for relapse of erosive GERD during long-term maintenance treatment with proton pump inhibitor: a prospective multicenter study in Japan. J Gastroenterol. 2010;45:1193–200.
Fennerty MB, Johnson DA. Heartburn severity does not predict disease severity in patients with erosive esophagitis. MedGenMed. 2006;8:6.
Kusano M, Shimoyama Y, Sugimoto S, et al. Development and evaluation of FSSG: frequency scale for the symptoms of GERD. J Gastroenterol. 2004;39:888–91.
Jones R, Junghard O, Dent J, et al. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Aliment Pharmacol Ther. 2009;30:1030–8.
Johnsson F, Weywadt L, Solhaug JH, et al. One-week omeprazole treatment in the diagnosis of gastro-oesophageal reflux disease. Scand J Gastroenterol. 1998;33:15–20.
Schenk BE, Kuipers EJ, Klinkenberg-Knol EC, et al. Omeprazole as a diagnostic tool in gastroesophageal reflux disease. Am J Gastroenterol. 1997;92:1997–2000.
Numans ME, Lau J, de Wit NJ, et al. Short-term treatment with proton-pump inhibitors as a test for gastroesophageal reflux disease: a meta-analysis of diagnostic test characteristics. Ann Intern Med. 2004;140:518–27.
Klinkenberg-Knol EC, Meuwissen SG. Combined gastric and oesphageal 24-hour pH monitoring and oeosphageal manometry in patients with reflux disease, resistant to treatment with omeprazole. Aliment Pharmacol Ther. 1990;4:485–95.
Nojkov B, Rubenstein JH, Adlis SA, et al. The influence of Co-morbid IBS and psychological distress on outcomes and quality of life following PPI therapy in patients with gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2008;27:473–82.
Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97:142–6.
Pace F, Negrini C, Wiklund I, et al. Quality of life in acute and maintenance treatment of non-erosive and mild erosive gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2005;22:349–56.
Velanovich V. Quality of life and severity of symptoms in Gastro-oesophageal reflux disease: a clinical review. Eur J Surg. 2000;166:516–25.
Robinson M, Fitzgerald S, Hegedus R, et al. Onset of symptom relief with rabeprazole: a community-based, open-label assessment of patients with erosive oesophagitis. Aliment Pharmacol Ther. 2002;16:445–54.
Bytzer P. Goals of therapy and guideline for treatment success in symptomatic gastroesophageal reflux disease patients. Am J Gastroentero1 2003; 98(Suppl):S31-9.
Meineche-Schmidt V, Hauschildt Juhl H, Østergaard JE, et al. Costs and efficacy of three different esomeprazole treatment strategies for long-term management of gastro-esophageal reflux symptoms in primary care. Aliment Pharmacol Ther. 2004;19:907–15.
Hongo M, Kinoshita Y, Miwa H, et al. Characteristics affecting health-related quality of life (HRQOL) in Japanese patients with reflux oesophagitis and the effect of lansoprazole on HRQOL. J Med Econ. 2009;12:182–91.
Nocon M, Labenz J, Jaspersen D, et al. Health-related quality of life in patients with gastro-oesophageal reflux disease under routine care: 5-year follow up results of the ProGERD study. Aliment Pharmacol Ther. 2009;29:662–8.
Talwar V, Wurm P, Bankart MJG, et al. Clinical trial: chest pain caused by presumed gastro-oesophageal reflux in coronary artery disease: controlled study of lansoprazole vs. placebo. Aliment Pharmacol Ther. 2010;32:191–9.
Richter JE. Long-term management of gastroesophageal reflux disease and its complications. Am J Gastroentero1 1997; 92(4 Suppl):30S-34S; discussion: 34S-35S.
Katelaris PH. An evaluation of current GERD therapy: a summary and comparison of effectiveness, adverse effects and costs of drugs, surgery and endoscopic therapy. Best Prac Res Clin Gastroenterol. 2004;18(Suppl):39–45.
Jones MP. Acid suppression in gastro-oesophageal reflux disease: why? how? How much and when? Post-grad Med J. 2002;78:465–8.
Jankowski JA, Anderson M. Review article: management of oesophageal adenocarcinoma– control of acid bile and inflammation in intervention strategies for Barrett’s oesophagus. Aliment Pharmacol Ther. 2004;20(Suppl 5):71–80.
Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach. Arch Intern Med. 2006;166:965–71.
Kinoshita Y, Ashida K, Miwa H, et al. The impact of lifestyle modification on the health-related quality of life of patients with reflux esophagitis receiving treatment with a proton pump inhibitor. Am J Gastroenterol. 2009;104:1106–11.
Hunt RH. Importance of pH control in the management of GERD. Arch Intern Med. 1999;159:649–57.
Khan M, Santana J, Donnellan C, et al. Medical treatments in the short term management of reflux oesophgitis (review). Cochrane Database Syst Rev 2007; (2):CD003244.
Hunt RH. The relationship between the control of pH and healing and symptom relief in gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 1995;9(Suppl 1):3–7.
van Pinxteren B, Numans ME, Bonis PA, et al. Short-term treatment with proton pump inhibitors, H2-receptor antagonists and prokinetics for gastro-oesophageal reflux disease-like symptoms and endoscopy negative reflux disease (review). Cochrane Database Syst Rev 2006; (3):CD002095.
Tack J, Fass R. Review article: approaches to endoscopic-negative reflux disease: part of the GERD spectrum of a unique acid-related disorder? Aliment Pharmacol Ther. 2004;19(Suppl. 1):28–34.
Fass R. Epidemiology and pathophysiology of symptomatic gastroesophageal reflux disease. Am J Gastroenterol. 2003;98(Suppl):S2–7.
Castell DO, Dalton CB, Becker D, et al. Alginic acid decreases postprandial upright gastroesophageal reflux. Comparison with equal-strength antacid. Dig Dis Sci. 1992;37:589–93.
Buts JP, Barudi C, Otte JB. Double-blind controlled study on the efficacy of sodium alginate (Gaviscon) in reducing gastroesophageal reflux assessed by 24 h continuous pH monitoring in infants and children. Eur J Pediatr. 1987;146:156–8.
Kwiatek MA, Roman S, Fareeduddin A, et al. An alginate-antacid formulation (Gaviscon Double Action Liquid) can eliminate or displace the postprandial ‘acid pocket’ in symptomatic GERD patients. Aliment Pharmacol Ther. 2011;34:59–66.
Tran T, Lowry AM, El-Serag HB. Meta-analysis: the efficacy of over-the-counter gastro-oesophageal reflux disease therapies. Aliment Pharmacol Ther. 2007;25:143–53.
Mandel KG, Daggy BP, Brodie DA, et al. Review article: alginate-raft formulations in the treatment of heartburn and acid reflux. Aliment Pharmacol Ther. 2000;14:669–90.
Poynard T, Vernisse B, Agostini H. Randomized, multicentre comparison of sodium alginate and cisapride in the symptomatic treatment of uncomplicated gastro-oesophageal reflux. Aliment Pharmacol Ther. 1998;12:159–65.
Pouchain D, Bigard MA, Liard F, et al. Gaviscon ® vs. omeprazole in symptomatic treatment of moderate gastroesophageal reflux. a direct comparative randomised trial. BMC Gastroenterol. 2012;12:18–26.
Graham DY, Patterson DJ. Double-blind comparison of liquid antacid and placebo in the treatment of symptomatic reflux esophagitis. Dig Dis Sci. 1983;28:559–63.
Grove O, Bekker C, Jeppe-Hansen MG, et al. Ranitidine and high-dose antacid in reflux oesophagitis. A randomized, placebo-controlled trial. Scand J Gastroenterol. 1985;20:457–61.
Weberg R, Berstad A. Symptomatic effect of a low-dose antacid regimen in reflux oesophagitis. Scand J Gastroenterol. 1989;24:401–6.
Chiba N, De Gara CJ, Wilkinson JM, et al. Speed of healing and symptom relief in grade II to IV gastroesophageal reflux disease: a meta-analysis. Gastroenterology. 1997;112:1798–810.
Habu Y, Kiyota K, Asada M, et al. Omeprazole versus famotidine for the treatment of lower-grade reflux esophagitis: a randomized controlled trial in Japan. Shin-yaku to Rinsho. 2000;49:1072–8 (in Japanese).
Habu Y, Maeda K, Kusuda T, et al. “Proton-pump inhibitor-first” strategy versus “step-up” strategy for the acute treatment of reflux esophagitis: a cost-effectiveness analysis in Japan. J Gastroenterol. 2005;40:1029–35.
Habu Y, Oyasu K, Wakamatsu T, et al. Cost-effectiveness of the treatment of reflux esophagitis: proton pump inhibitor versus histamine-2-receptor antagonist. Nihon Rinsho. 2000;58:1881–5 (in Japanese).
Haag S, Holtmann G. Onset of relief of symptoms of gastroesophageal reflux disease: post hoc analysis of two previously published studies comparing pantoprazole 20 mg once daily with nizatidine or ranitidine 150 mg twice daily. Clin Ther. 2010;32:678–90.
Sigterman KE, van Pinxteren B, Bonis PA, et al. Short-term treatment with proton pump inhibitors, H2-receptor antagonists and prokinetics for gastro-oesophageal reflux disease-like symptoms and endoscopy negative reflux disease. Cochrane Database Syst Rev. 2013; 5:CD002095.
Miwa H, Inoue K, Ashida K, et al. Randomised clinical trial: efficacy of the addition of a prokinetic, mosapride citrate, to omeprazole in the treatment of patients with non-erosive reflux disease—a double-blind, placebo-controlled study. Aliment Pharmacol Ther. 2011;33:323–32.
Klok RM, Postma MJ, van Hout BA, et al. Meta-analysis: comparing the efficacy of proton pump inhibitors in short-term use. Aliment Pharmacol Ther. 2003;17:1237–45.
Kinoshita Y, Miwa H, Kasugai K. Efficacy of esomeprazole compared with omeprazole in reflux esophagitis patients -a phase III, multicenter, randomized, double-blind, parallel-group trial-. Nihon Shokakibyo Gakkai Zasshi. 2013;110:234–42 (in Japanese).
Mee AS, Rowley JL. Rapid symptom relief in reflux oesophagitis: a comparison of lansoprazole and omeprazole. Aliment Pharmacol Ther. 1996;10:757–63.
Furuta T, Shirai N, Watanabe F, et al. Effect of cytochrome P4502C19 genotypic differences on cure rates for gastroesophageal reflux disease by lansoprazole. Clin Pharmacol Ther. 2002;72:453–60.
Kawamura M, Ohara S, Koike T, et al. The effects of lansoprazole on erosive reflux oesophagitis are influenced by CYP2C19 polymorphism. Aliment Pharmacol Ther. 2003;17:965–73.
von Rensburg CJ, Bardhan KD. No clinical benefit of adding cisapride to pantoprazole for treatment of gastro-oesophageal reflux disease. Eur J Gastroenterol Hepatol. 2001;13:909–14.
Tominaga K, Iwakiri R, Fujimoto K, et al. Rikkunshito improves symptoms in PPI-refractory GERD patients: a prospective, randomized, multicenter trial in Japan. J Gastroenterol. 2012;47:284–92.
Kinoshita Y, Hongo M, Mitsui S, et al. Efficacy of twice-daily rabeprazole for reflux esophagitis patients refractory to standard once-daily administration of PPI: the Japan-based TWICE study. Am J Gastroenterol. 2012;107:522–30.
Adachi K, Komazawa Y, Mihara T, et al. Administration of H2 receptor antagonist with proton pump inhibitor is effective for long-term control of refractory reflux esophagitis. J Clin Gastroenterol. 2004;38:297–8.
Fackler WK, Ours TM, Vaezi MF, et al. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology. 2002;122:625–32.
Fass R, Murthy U, Hayden CW, et al. Omeprazole 40 mg once a day is equally effective as lansoprazole 30 mg twice a day in symptom control of patients with gastro- oesophageal reflux disease (GERD) who are resistant to conventional-dose lansoprazole therapy-a prospective, randomized, multi-centre study. Aliment Pharmacol Ther. 2000;14:1595–603.
Furuta T, Shimatani T, Sugimoto M, et al. Investigation of pretreatment prediction of proton pump inhibitor (PPI)-resistant patients with gastroesophageal reflux disease and the dose escalation challenge of PPIs-TORNADO study: a multicenter prospective study by the Acid-Related Symptom Research Group in Japan. J Gastroenterol. 2011;46:1273–83.
Sugimoto M, Nishino M, Kodaira C, et al. Characteristics of non-erosive gastroesophageal reflux disease refractory to proton pump inhibitor therapy. World J Gastroenterol. 2011;17:1858–65.
Miyamoto M, Haruma K, Takeuchi K, et al. Frequency scale for symptoms of gastroesophageal reflux disease predicts the need for addition of prokinetics to proton pump inhibitor therapy. J Gastroenterol Hepatol. 2008;23:746–51.
Koek GH, Sifrim D, Lerut T, et al. Effect of the GABA(B) agonist baclofen in patients with symptoms and duodeno-gastro-oesophageal reflux refractory to proton pump inhibitors. Gut. 2003;52:1397–402.
Futagami S, Iwakiri K, Shindo T, et al. The prokinetic effect of mosapride citrate combined with omeprazole therapy improves clinical symptoms and gastric emptying in PPI-resistant NERD patients with delayed gastric emptying. J Gastroenterol. 2010;45:413–21.
Miyamoto M, Manabe N, Haruma K. Efficacy of the addition of prokinetics for proton pump inhibitor (PPI) resistant non-erosive reflux disease (NERD) patients: significance of frequency scale for the symptom of GERD (FSSG) on decision of treatment strategy. Intern Med. 2010;49:1469–76.
Donnellan C, Sharma N, Preston C, et al. Medical treatments for the maintenance therapy of reflux oesophagitis and endoscopic negative reflux disease. Cochrane Database Syst Rev 2005; 2: CD003245.
Habu Y, Yoshino T, Shio S, et al. Evaluation of the efficacy and the cost-effectiveness of maintenance treatment of gastroesophageal reflux disease: proton pump inhibitor versus histamine-2-receptor antagonist. Nihon Rinsho. 2004;62:1504–9 (in Japanese).
Caos A, Breiter J, Perdomo C, et al. Long-term prevention of erosive or ulcerative gastro-oesophageal reflux disease relapse with rabeprazole 10 or 20 mg vs. placebo: results of a 5-year study in the United States. Aliment Pharmacol Ther. 2005;22:193–202.
Fujimoto K. Hongo M; Maintenance Study Group. Risk factors for relapse of erosive GERD during long-term maintenance treatment with proton pump inhibitor: a prospective multicenter study in Japan. J Gastroenterol. 2010;45:1193–200.
Carlsson R, Galmiche JP, Dent J, et al. Prognostic factors influencing relapse of oesophagitis during maintenance therapy with antisecretory drugs: a meta-analysis of long-term omeprazole trials. Aliment Pharmacol Ther. 1997;11:473–82.
Habu Y, Ikeura T, Shio S, et al. A cost-effectiveness analysis for the therapeutic strategy of reflux esophagitis based on endoscopic findings. Shoukakika. 2003;36:46–50 (in Japanese).
Lind T, Havelund T, Lundell L, et al. On demand therapy with omeprazole for the long-term management of patients with heartburn without oesophagitis: a placebo-controlled randomized trial. Aliment Pharmacol Ther. 1999;13:907–14.
Talley NJ, Lauritsen K, Tunturi-Hihnala H, et al. Esomeprazole 20 mg maintains symptom control in endoscopy-negative gastro-oesophageal reflux disease: a controlled trial of ‘on-demand’ therapy for 6 months. Aliment Pharmacol Ther. 2001;15:347–54.
Bytzer P, Blum A, De Herdt D, et al. Six-month trial of on-demand rabeprazole 10 mg maintains symptom relief in patients with non-erosive reflux disease. Aliment Pharmacol Ther. 2004;20:181–8.
Juul-Hansen P, Rydning A. On-demand requirements of patients with endoscopy-negative gastro-oesophageal reflux disease: H2-blocker vs. proton pump inhibitor. Aliment Pharmacol Ther. 2009;29:207–12.
Bigard MA, Genestin E. Treatment of patients with heartburn without endoscopic evaluation: on-demand treatment after effective continuous administration of lansoprazole 15 mg. Aliment Pharmacol Ther. 2005;22:635–43.
Tsai HH, Chapman R, Shepherd A, et al. Esomeprazole 20 mg on-demand is more acceptable to patients than continuous lansoprazole 15 mg in the long-term maintenance of endoscopy-negative gastro-oesophageal reflux patients: the COMMAND Study. Aliment Pharmacol Ther. 2004;20:657–65.
Habu Y, Maeda K, Kusuda T, et al. A cost-effectiveness analysis for the therapeutic strategy of non-erosive reflux disease. Shokakika. 2005;40:286–90 (in Japanese).
Szucs T, Thalmann C, Michetti P, et al. Cost analysis of long-term treatment of patients with symptomatic gastroesophageal reflux disease (GERD) with esomeprazole on-demand treatment or esomeprazole continuous treatment: an open, randomized, multicenter study in Switzerland. Value Health. 2009;12:273–81.
Tepes B, Stabuc B, Kocijancic B, et al. Maintenance therapy of gastroesophageal reflux disease patients with omeprazole. Hepatogastroenterology. 2009;56:67–74.
van der Velden AW, de Wit NJ, Quartero AO, et al. Pharmacological dependency in chronic treatment of gastroesophageal reflux disease: a randomized controlled clinical trial. Digestion. 2010;81:43–52.
Sato N, Ohkusa T, Mitachi Y, et al. Assessment of patient satisfaction after one-month administration of omeprazole tablets for repeated recurrence of reflux esophagitis: a patient satisfaction survey using self-reporting questionnaire. Yakuri to Chiryo. 2003;31:163–75 (in Japanese).
van Zanten SJ, Henderson C, Hughes N. Patient satisfaction with medication for gastroesophageal reflux disease: a systematic review. Can J Gastroenterol. 2012;26:196–204.
Haga Y, Nakatsura T, Shibata Y, et al. Human gastric carcinoid detected during long-term antiulcer therapy of H2 receptor antagonist and proton pump inhibitor. Dig Dis Sci. 1998;43:253–7.
Jianu CS, Fossmark R, Viset T, et al. Gastric carcinoids after long-term use of a proton pump inhibitor. Aliment Pharmacol Ther. 2012;36:644–9.
Freston JW, Hisada M, Peura DA, et al. The clinical safety of long-term lansoprazole for the maintenance of healed erosive oesophagitis. Aliment Phamacol Ther. 2009;29:1249–60.
Lundell L, Miettinen P, Myrvold HE, et al. Comparison of outcomes 12 years after antireflux surgery or omeprazole maintenance therapy for reflux esophagitis. Clin Gastroenterol Hepatol. 2009;7:1292–8.
Kuipers EJ, Nelis GF, Klinkenberg-Knol EC, et al. Cure of Helicobacter pylori infection in patients with reflux oesophagitis treated with long term omeprazole reverses gastritis without exacerbation of reflux disease: results of a randomised controlled trial. Gut. 2004;53:12–20.
Yang H-B, Sheu B-S, Wang S-T, et al. H. pylori eradication prevents the progression of gastric intestinal metaplasia in reflux esophagitis patients using long-term esomeprazole. Am J Gastroenterol. 2009;104:1642–9.
Tamim H, Duranceau A, Qi Chen L, et al. Association between use of acid-suppressive drugs and risk of gastric cancer: a nested case-control study. Drug Saf. 2008;31:675–84.
Poulsen AH, Christensen S, McLaughlin JK, et al. Proton pump inhibitors and risk of gastric cancer: a population-based cohort study. Br J Cancer. 2009;100:1503–7.
Robertson DJ, Larsson H, Friis S, et al. Proton pump inhibitor use and risk of colorectal cancer: a population-based, case-control study. Gastroenterology. 2007;133:755–60.
van Soest EM, van Rossum LG, Dieleman JP, et al. Proton pump inhibitors and the risk of colorectal cancer. Am J Gastroenterol. 2008;103:966–73.
Leonard J, Marshall JK, Moayyedi P. Systematic review of the risk of enteric infection in patients taking acid suppression. Am J Gastroenterol. 2007;102:2047–56.
Deshpande A, Pant C, Pasupuleti V, et al. Association between proton pump inhibitor therapy and Clostridium difficile infection in a meta-analysis. Clin Gastroenterol Hepatol. 2012;10:225–33.
Giuliano C, Wilhelm SM, Kale-Pradhan PB. Are proton pump inhibitors associated with the development of community-acquired pneumonia? A meta- analysis. Expert Rev Clin Pharmacol. 2012;5:337–44.
Ngamruengphong S, Leontiadis GI, Radhi S. Proton pump inhibitors and risk of fracture: a systematic review and meta-analysis of observational studies. Am J Gastroenterol. 2011;106:1209–19.
Hayashi T, Ogino H, Hirai S, et al. A case of collageneous colitis showing improvement by discontinuation of lansoprazole was reported with a review of 182 cases in Japan. Nihon Shokaki Naishikyo Gakkai Koushin-etsu Hokuriku Shibu Kikannshi, 27:30–6, 53 (in Japanese).
Abe K, Kurahara K, Sakai Y, et al. Clinical features of collageneous colitis. Clinics in Digestive Tract. 2012;17:101–6 (in Japanese).
Hotta K, Oyama T, Miyata Y, et al. Incidence of microscopic colitis in patients who presented with chronic diarrhea: outcome of retrospective study in Japan of colonoscopic random biopsies. Shoukaki Naishikyo. 2008;20:1357–61 (in Japanese).
Keszthelyi D, Jansen SV, Schouten GA, et al. Proton pump inhibitor use is associated with an increased risk for microscopic colitis: a case-control study. Aliment Pharmacol Ther. 2010;32:1124–8.
O’Donoghue ML, Braunwald E, Antman EM, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials. Lancet. 2009;374:989–97.
Simon T, Steg PG, Gilard M, et al. Clinical events as a function of proton pump inhibitor use, clopidogrel use, and cytochrome P450 2C19 genotype in a large nationwide cohort of acute myocardial infarction: results from the French Registry of Acute ST-Elevation and Non-ST-Elevation Myocardial Infarction (FAST-MI) registry. Circulation. 2011;123:474–82.
Bhatt DL, Cryer BL, Contant CF, et al. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med. 2010;363:1909–17.
Ren YH, Zhao M, Chen YD, et al. Omeprazole affects clopidogrel efficacy but not ischemic events in patients with acute coronary syndrome undergoing elective percutaneous coronary intervention. Chin Med J (Engl). 2011;124:856–61.
Hsu P-I, Lai K-H, Liu C-P, et al. Esomeprazole with clopidogrel reduces peptic ulcer recurrence, compared with clopidogrel alone, in patients with atherosclerosis. Gastroenterology. 2011;140:791–8.
Kwok CS, Jeevanantham V, Dawn B, et al. No consistent evidence of differential cardiovascular risk amongst proton-pump inhibitors when used with clopidogrel: meta-analysis. Int J Cardiol. 2013;167:965–74.
Ito T, Jensen RT. Association of long-term proton pump inhibitor therapy with bone fractures and effects on absorption of calcium, vitamin B12, iron, and magnesium. Curr Gastroenterol Rep. 2010;12:448–57.
Ally MR, Veerappan GR, Maydonovitch CL, et al. Chronic proton pump inhibitor therapy associated with increased development of fundic gland polyps. Dig Dis Sci. 2009;54:2617–22.
Hongo M, Fujimoto K, Yabana T, et al. Incidence and risk factor of fundic gland polyp and hyperplastic polyp in long-term proton pump inhibitor therapy: a prospective study in Japan. J Gastroenterol. 2010;45:618–24.
Stein HJ, Feussner H, Siewert JR. Antireflux surgery: a current comparison of open and laparoscopic approaches. Hepatogastroenterology. 1998;45:1328–37.
Ozawa S, Yoshida M, Kumai K, et al. New endoscopic treatments for gastroesophageal reflux disease. Ann Thorac Cardiovasc Surg. 2005;11:146–53.
Anvari M, Allen C, Marshall J, et al. A randomized controlled trial of laparoscopic Nissen fundoplication versus proton pump inhibitors for treatment of patients with chronic gastroesophageal reflux disease: one-year follow-up. Surg Innov. 2006;13:238–49.
Gillies RS, Stratford JM, Booth MI, et al. Does laparoscopic antireflux surgery improve quality of life in patients whose gastro-oesophageal reflux disease is well controlled with medical therapy? Eur J Gastroenterol Hepatol. 2008;20:430–5.
Broeders JA, Draaisma WA, de Vries DR, et al. The preoperative reflux pattern as prognostic indicator for long-term outcome after Nissen fundoplication. Am J Gastroenterol. 2009;104:1922–30.
Omura N, Kashiwagi H, Yano F, et al. Postoperative recurrence factors of GERD in the elderly after laparoscopic fundoplication. Esophagus. 2010;7:31–5.
Spechler SJ, Lee E, Ahnen D, et al. Long-term outcome of medical and surgical therapies for gastroesophageal reflux disease: follow-up of a randomized controlled trial. JAMA. 2001;285:2331–3.
Grant AM, Wileman SM, Ramsay CR, et al. Minimal access surgery compared with medical management for chronic gastro-oesophageal reflux disease: UK collaborative randomised trial. BMJ. 2008;337:2264–71.
Wileman SM, McCann S, Grant AM, et al. Medical versus surgical management for gastro-oesophageal reflux disease (GORD) in adults. Cochrane Database of Systematic Reviews. 2010;3:1–38.
Johannessen R, Petersen H, Olberg P, et al. Airway symptom and sleeping difficulties in operated and non-operated patients with gastroesophageal reflux disease. Scan J Gastroenterol. 2012;47:762–9.
Zaninotto G, Parante P, Salvador R, et al. Long-term follow-up of Barrett’s epithelium: medical versus antireflux surgical therapy. J Gastrointest Surg. 2012;16:7–15.
Brillantino A, Schettino M, Torelli F, et al. Laparoscopic Nissen-Rossetti fundoplication is a safe and effective treatment for both acid and bile gastroesophageal reflux in patients poorly responsive to proton pump inhibitor. Surg innovation. 2011;18:387–93.
Grant A, Wileman S, Ramsay C, et al. The effectiveness and cost-effectiveness of minimal access surgery amongst people with gastro-oesophageal reflux disease—a UK collaborative study. The REFLUX trial. Health Technol Assess. 2008;12:1–98.
Goeree R, Hopkins R, Marshall JK, et al. Cost-utility of laparoscopic Nissen fundoplication versus proton pump inhibitors for chronic and controlled gastroesophageal reflux disease: a 3-year prospective randomized controlled trial and economic evaluation. Value in Health. 2011;14:263–73.
Luostarinen ME, Isolauri JO. Surgical experience improves the long-term results of Nissen fundoplication. Scand J Gastroenterol. 1999;34:117–20.
Sandbu R, Khamis H, Gustavsson S, et al. Laparoscopic antireflux surgery in routine hospital care. Scand J Gastroenterol. 2002;37:132–7.
Contini S, Scarpignato C. Does the learning phase influence the late outcome of patients with gastroesophageal reflux disease after laparoscopic fundoplication? Surg Endosc. 2004;18:266–71.
Contini S, Bertile A, Nervi G, et al. Quality of life for patients with gastroesophageal reflux disease 2 years after laparoscopic fundoplication: evaluation of the results obtained during the initial evidence. Surg Endosc. 2002;16:1555–60.
Hwang H, Turner LJ, Blair NP. Examining the learning curve of laparoscopic fundoplication at an urban community hospital. Am J Surg. 2005;189:522–6.
Zaninotto G, Molena D, Ancona E. A prospective multicenter study of laparoscopic treatment of gastroesophageal reflux disease in Italy: type of surgery, conversions, complications, and early results. Surg Endosc. 2000;14:282–8.
Hakanson BS, Thor KB, Thorell A, et al. Open vs laparoscopic partial posterior fundoplication. Surg Endosc. 2007;21:289–98.
Velanovich V. Comparison of symptomatic and quality of life outcomes of laparoscopic versus open antireflux surgery. Surgery. 1999;126:782–9.
Juan RT, Sánchez TT, Martínez EM, et al. Surgery for gastroesophageal reflux disease: a comparative study between the open and laparoscopic approaches. Rev Esp Enferm Dis. 2005;97:328–37.
Franzén T, Anderberg B, Grahn LT, et al. Prospective evaluation of laparoscopic and open 360* fundoplication in mild and severe gastro-oesophageal reflux disease. Eur J Surg. 2002;168:539–54.
Tan G, Yang Z, Wang Z. Meta-analysis of laparoscopic total (Nissen) versus posterior (Toupet) fundoplication for gastro-oesophageal reflux disease based on randomized clinical trials. ANZ J Surg. 2011;81:246–52.
Broeders JA, Mauritz FA, Ahmed Ali U, et al. Systematic review and meta-analysis of laparoscopic Nissen (posterior total) versus Toupet (posterior partial) fundoplication for gastro-oesophageal reflux disease. Br J Surg. 2010;97:1318–30.
Hafez J, Wrba F, Lenglinger J, et al. Fundoplication for gastroesophageal reflux and factors associated with outcome 6–10 years after the operation: multivariate analysis of prognostic factors using the propensity score. Surg Endosc. 2008;22:1763–8.
Ozawa S, Kumai K, Higuchi K, et al. Short-term outcome of endoluminal gastroplication for the treatment of GERD: the first multicenter trial. J Gastroenterol. 2009;44:675–84.
Chen YK, Raijman I, Ben-Menachem T, et al. Long-term outcomes of endoluminal gastroplication: a US multicenter trial. Gastrointest Endosc. 2005;61:659–67.
von Renteln D, Brey U, Riecken B, et al. Endoscopic full-thickness placation (Plicator) with two serially placed implants improves esophagitis and reduced PPI use and esophageal acid exposure. Endoscopy. 2008;40:173–8.
Filipi CJ, Stadlhuber RJ. Initial experience with new intraluminal device for GERD Barrett esophagus and obesity. J Gastrointest Surg. 2010;14:121–6.
Testoni PA, Vailati C, Testoni S, et al. Transoral incisioness fundoplication (TIF 2.0) EsophyX for gastroesophageal reflux disease: long-term results and findings affecting outcome. Surg Endosc. 2012;26:1425–35.
Liu H, Zhang J, Li J, et al. Improvement of clinical parameters in patients with gastroesophageal reflux disease after radiofrequency energy delivery. World J Gastroenterol. 2011;17:4429–33.
Luis H, Devière J. Endoscopic implantation of enteryx for the treatment of gastroesophageal reflux disease: technique, pre-clinical and clinical experience. Gastrointest Endosc Clin N Am. 2003;13:191–200.
Fockens P. Gatekeeper reflux repair system: technique, pre-clinical, and clinical experience. Gastrointest Endosc Clin N Am. 2003;13:179–89.
Acknowledgments
This article was supported by a Grant-in-Aid from the JSGE. The authors thank investigators and supporters for participating in the studies. The authors express special appreciation to Drs. Junya Oguma (Tokai University), Akiyo Kawada, Shiko Kuribayashi, Yasuyuki Shimoyama, Hiroko Hosaka, Masaki Maeda (Gunma University), Yukie Kohata (Osaka City University), Yasuhisa Sakata (Saga University), Mariko Hojo (Juntendo University), Takahisa Yamasaki (Hyogo College of Medicine).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Any financial relationships with enterprises, businesses or academic institutions in the subject matter or materials discussed in the manuscript are listed as follows; [1] those from which the authors, the spouse, partner or immediate relatives of authors, have received individually any income, honoraria or any other types of remuneration; Astellas Pharma Inc., AstraZeneca K. K., Eisai Co., Ltd., Otsuka Pharmaceutical Co.,Ltd., Daiichi Sankyo Company, Limited., Takeda Pharmaceutical Company Limited., Nippon Shinyaku Co., Ltd. and [2] those from which the academic institutions of the authors received support (commercial/academic cooperation); Astellas Pharma Inc., AstraZeneca K. K., Eisai Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Given Imaging Ltd., Daiichi Sankyo Company, Limited, Takeda Pharmaceutical Company Limited., Mitsubishi Tanabe Pharma Corporation, Nihon Pharmaceutical Co., Ltd.
Additional information
The original version of this article appeared in Japanese as “Ishokudo Gyakuryu-shou Shinryo Guidelines 2015” from the Japanese Society of Gastroenterology (JSGE), published by Nankodo, Tokyo, 2015. Please see the article on the standards, methods, and process of developing the guidelines (doi:10.1007/s00535-014-1016-1).
The members of the Guidelines Committee are listed in the "Appendix" in the text.
Appendix
Appendix
Members of the Guidelines Committee who created and evaluated the JSGE ‘‘Evidence-based clinical practice guidelines for gastroesophageal reflux disease’’ are listed below.
Executive Committee
Chair: Yoshikazu Kinoshita (Department of Gastroenterology and Hepatology, Shimane University School of Medicine)
Vice-Chair: Katsuhiko Iwakiri (Department of Gastroenterology, Nippon Medical School Graduate School of Medicine)
Members: Kiyoshi Ashida (Department of Gastroenterology and Hepatology, Rakuwakai Otowa Hospital), Ryuichi Iwakiri (Department of Internal Medicine & Gastrointestinal Endoscopy, Saga Medical School), Tadayuki Oshima (Division of Gastroenterology, Department of Internal Medicine, Hyogo College of Medicine), Shuichi Ohara (Department of Gastroenterology, Tohoku Rosai Hospital), Soji Ozawa (Department of Gastroenterological Surgery, Tokai University School of Medicine), Hideyuki Kashiwagi (Department of Surgery, Fuji City General Hospital), Osamu Kawamura (Department of Endoscopy and Endoscopic Surgery, Gunma University Hospital), Akihito Nagahara (Department of Gastroenterology and Hepatology, Juntendo University Shizuoka Hospital), Yasuki Habu (Department of Gastroenterology, Saiseikai Noe Hospital), Yasuhiro Fujiwara (Department of Gastroenterology, Osaka City University Graduate School of Medicine), Noriaki Manabe (Division of Endoscopy and Ultrasonography, Department of Clinical Pathology and Laboratory Medicine, Kawasaki Medical School)
Evaluation Committee
Chair: Michio Hongo (Kurokawa General Hospital)
Vice-Chair: Kyoichi Adachi (Health Center, Shimane Environment & Health Public Corporation)
Members: Tatsuyuki Kawano (Department of Esophageal and General Surgery, Tokyo Medical and Dental University), Motoyasu Kusano (Department of Endoscopy and Endoscopic Surgery, Gunma University Hospital), Ken Haruma (Department of General Internal Medicine 2, Kawasaki Hospital, Kawasaki Medical School), Kazuhide Higuchi (2nd Department of Internal Medicine, Osaka Medical College), Kazuma Fujimoto (Department of Internal Mediceine and Gastrointestinal Endoscopy, Saga Medical School), Yoshio Hoshihara (Department of Gastroenterology, Nippon Medical School Graduate School of Medicine), Hiroto Miwa (Division of Upper Gastroenterology, Department of Internal Medicine, Hyogo College of Medicine)
The Japanese Society of Gastroenterology
President: Tooru Shimosegawa (Division of Gastroenterology, Tohoku University Graduate School of Medicine)
Rights and permissions
About this article

Cite this article
Iwakiri, K., Kinoshita, Y., Habu, Y. et al. Evidence-based clinical practice guidelines for gastroesophageal reflux disease 2015. J Gastroenterol 51, 751–767 (2016). https://doi.org/10.1007/s00535-016-1227-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-016-1227-8