
Abstract
Purpose
Controlling cancer-related pain is an important component in the palliative care of cancer patients. The objective of this review was to assess the effectiveness of acupuncture for treating cancer pain.
Methods
Fourteen databases were searched from their inception through April 2011. Randomised clinical trials (RCTs) were included if acupuncture was used as the sole treatment or as a part of a combination therapy for cancer pain. Studies were included if they were controlled with a placebo or controlled against a drug-therapy or no-treatment group. The Cochrane criteria were used to assess the risk of bias.
Results
A total of 15 RCTs met our inclusion criteria. All of the included RCTs were associated with a high risk of bias. The majority of acupuncture treatments or combination therapies with analgesics exhibited favourable effects compared with conventional treatments in individual studies. However, a meta-analysis suggested that acupuncture did not generate a better effect than drug therapy (n = 886; risk ratio (RR), 1.12; 95% CI 0.98 to 1.28; P = 0.09). The comparison between acupuncture plus drug therapy and drug therapy alone demonstrated a significant difference in favour of the combination therapy (n = 437; RR, 1.36; 95% CI 1.13 to 1.64; P = 0.003). The results of this systematic review provide no strong evidence for the effectiveness of acupuncture in the management of cancer pain.
Conclusion
The total number of RCTs included in the analysis and their methodological quality were too low to draw firm conclusions. Future rigorous RCTs will be necessary to assess the clinical efficacy of acupuncture in this area.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cancer-related pain represents a major challenge for both clinicians and patients. This pain can be associated directly with the cancer or with certain treatments administered to the patient. The prevalence of United States cancer patients receiving pain control is estimated to be 25% for newly diagnosed patients, 33% for patients undergoing active treatment, and greater than 75% for patients with advanced disease [1, 2]. Pain prevalence is also high in specific cancer types, such as pancreatic (44%) and head and neck cancers (40%) [3]. The European Pain in Cancer survey included 11 European countries and indicated that the overall pain prevalence of patients with cancer in the community was 72%. The rate in the UK of 77% was slightly higher [4]. A total of 480 Taiwanese patients receiving outpatient treatment at 15 different outpatient clinics were included in this study. Pain was reported by 257 patients (54%). Severe pain was reported by 35% and moderate pain by 35.4% of the patients [5]. The Korean Society for Hospice and Palliative Care survey was a multi-centre study that included general or university hospitals, and it showed that 52.1% of cancer patients suffer from pain and that 62.6% are not satisfied with the current pain control [6]. Pain prevalence is high in developing countries due to late diagnosis and major impediments to opioid access [7, 8]. Up to 80% of people with cancer experience pain at some time during their illness, and in most cases, they require opioid analgesics [9]. The patients' perceived barriers to managing cancer pain may be culturally influenced. The prevalence of perceived barriers to managing cancer pain was significantly higher in Asian patients compared with Western patients (especially for concerns about disease progression, tolerance, and fatalism) [10].
Although conventional medicine has well-established guidelines to systemically control cancer-related pain [11], over half of all cancer patients still suffer significant pain, which affects their quality of life [12]. Pharmacologic treatment is not always sufficient [13, 14], and serious adverse effects may limit the use of the analgesics [15, 16]. The United States and Europe have developed guidelines on complementary and alternative medicine (CAM), but they are not comprehensive. The New American College of Chest Physicians’ (ACCP) cancer-care guidelines include CAM therapies [17].
These limitations have led to the use of CAM. The use of CAM for chronic cancer pain has become common and widespread [15]. Most patients use CAM as an adjunct therapy along with the conventional treatments [18, 19]. Among the CAM treatments, acupuncture is the most widely used intervention, and it is used to treat a variety of symptoms and conditions associated with cancer and the adverse effects related to the cancer treatments [20]. The effects of acupuncture might decrease the requirement for drugs and may thereby decrease the adverse effects. Acupuncture may also help patients who are sensitive to normal doses of analgesics and patients with uncontrolled pain despite high drug doses [21].
Two systematic reviews of acupuncture for cancer pain exist [22, 23]. One included just three randomised clinical trials (RCTs) and four uncontrolled observational studies (UOSs) [22] and is now outdated. The other review, which was published in 2010, included only seven RCTs [23]. This review failed to include all of the RCTs that are currently available.
The aim of this article was to update, complete, and critically evaluate the evidence from RCTs regarding acupuncture as a treatment for pain experienced by cancer patients.
Methods
Data sources
The following databases were searched from their inception through April 2011: Medline, AMED, EMBASE, CINAHL, PsycInfo, The Cochrane Library 2011 (Issue 4), six Korean Medical Databases (Korean Studies Information, DBPIA, the Korean Institute of Science and Technology Information, the Research Information Centre for Health Database, KoreaMed, and the Korean National Assembly Library), the Chinese Medical Database of the China Academic Journal (CNKI), and China Doctor/Master’s Dissertations. The following search terms were used in Korean, Chinese, and English: (acupuncture OR electro-acupuncture OR auricular acupuncture OR scalp acupuncture OR needle OR acupuncture point OR meridian OR acupoint OR acupuncture treatment OR acupuncture therapy) AND (cancer OR tumour OR neoplasm OR pain). In addition, a manual search was conducted using our own files and journals (Focus on Alternative and Complementary Therapies [FACT] and Research in Complementary Medicine [Forschende Komplementarmedizin] up to April 2011). Hard copies of all the articles were obtained and read completely.
Study selection
RCTs were included if acupuncture was used as the sole intervention or as an adjunct to another standard treatment for any cancer pain and if the control group received the same concomitant treatments as the acupuncture group. Non-randomised trials were excluded. Trials with designs that did not allow the effectiveness of acupuncture to be evaluated (e.g. by using a treatment of unproven efficacy in the control group or by comparing two different forms of acupuncture), adopted comparison treatments/groups that were expected to have similar effects to acupuncture (moxibustion, transcutaneous electrical nerve stimulation, point injection, laser irradiation, cupping, tuina, etc.) or used herbal medicines were excluded. Trials that studied cancer pain mixed with other types of pain and trials that were conducted on patients during or a few days after operation on their malignant tumours were also excluded. Trials were also excluded if the outcome measures were not relevant to cancer pain. Trials published in the form of dissertations and abstracts were included. No language restrictions were imposed.
Data extraction, quality, and validity assessment
All of the articles were read by two independent reviewers (TYC and MSL) who extracted data from the articles according to the predefined criteria. The risk of bias was assessed using the following criteria from the Cochrane classification: sequence generation, allocation concealment, patient blinding, assessor blinding, incomplete outcome data (reporting dropout and withdrawal), and selective outcome reporting [24]. This review used ‘L, U, and H’ as keys for the judgments; the answer ‘Low’ indicated a low risk of bias (L), ‘Unclear’ indicated that the risk of bias was uncertain (U), and ‘High’ indicated a high risk of bias (H). Disagreements were resolved by discussion between all the authors (TYC, MSL, and EE).
Data synthesis
All clinical endpoints were considered, but the primary outcome measure was the response rate for relieving pain in patients with cancer. We did not evaluate the outcomes related to immunological or other surrogate endpoints. The differences between the intervention and control groups were assessed. Risk ratio (RR) and 95% confidence intervals (CI) were assessed for the effect size of each included study. All of the statistical analyses were performed using the Cochrane Collaboration’s software program, Review Manager (RevMan), Version 5.0 for Windows (Copenhagen, The Nordic Cochrane Centre). For studies with insufficient information, we contacted the primary authors to acquire and verify data when possible. The chi-square test for heterogeneity and the I 2 test were used to evaluate the heterogeneity of the included studies. Unless excessive statistical heterogeneity was present, we pooled the data for a meta-analysis using a random-effects model.
Results
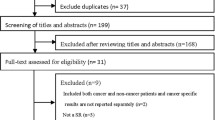
Our search strategy generated 494 hits, and 15 articles met our inclusion criteria (Fig. 1). The reasons that certain RCTs were excluded are listed in Electronic supplementary material 1. The key data from all the included RCTs are listed in Table 1 [25–39]. All of the trials described the selected points and other information related to treatment in sufficient detail, and these data are presented in Table 2.

Flow chart for the publication selection process. RCT: randomised clinical trial; CCT: controlled clinical trial; UOS: uncontrolled observational study; SR: systematic review
Study description
Participants
In total, 1,157 participants were involved in 15 studies in our review. Fourteen studies were conducted in China (1,070 participants), and one study was conducted in France (87 participants). Twelve trials were published in Chinese, and the other three were published in English.
Acupuncture interventions
The acupuncture style, details of needling, number of sessions and duration all varied among the included studies. Most of the studies used manual acupuncture based on Traditional Chinese Medicine theory [40]. Three studies used wrist–ankle acupuncture [25, 26, 38]. One study used ear acupuncture [33], and one study used ear acupuncture and electro-acupuncture (EA) [32]. One study used manual acupuncture and fire needle [28], and another study used EA alone [35]. Participants received semi-standardised acupuncture treatment, e.g. the use of a predetermined set of points combined with a set of points used flexibly [28, 29, 32–37, 39]. Six studies used Ashi points for all of the participants [25–27, 30, 31, 38]. The number of acupuncture sessions administered ranged from 1 to 60. De qi, a needling sensation perceived as numbness, soreness or distension that is usually generated by manipulating acupuncture needles to obtain an intended therapeutic effect, was reported in 11 studies [27, 29–32, 34–39]; the other four studies did not mention this effect [25, 26, 28, 33]. The practitioners’ backgrounds were not reported in any of the included studies.
Controls
Two studies used non-penetrating sham acupuncture controls on the identical acupuncture points that were used for the real acupuncture group [32, 33]. In 12 studies, acupuncture was compared with conventional medication, and in one study, acupuncture was compared with radiotherapy or chemotherapy.
Risk of bias
All of the included RCTs were associated with a high risk of bias (Table 2). Of the 15 included RCTs, nine RCTs did not describe the issues related to the randomisation process [27–29, 34–39]. Two RCTs used a random-numbers table [30, 31], and two other studies used a random sequence generated by a computer [32, 33]. Two other RCTs used a visiting sequence for sequence generation [25, 26]. Allocation concealment was appropriately employed in only one study [33]. Only two RCTs properly reported the information on dropouts or withdrawals [31, 33]. Assessor blinding and adverse events were described in two studies [32, 33].
Description of individual studies
Liver cancer
Three RCTs [25–27] focused on liver cancer. Compared with conventional analgesic treatment, single wrist–ankle acupuncture or combination therapy generated more favourable results with respect to total response rates. Hu et al. [25] conducted an RCT to evaluate the effectiveness of wrist–ankle acupuncture for the treatment of moderate and severe liver cancer pain. Ninety-four patients were divided randomly into five groups. Forty patients with moderate pain were divided into two groups (wrist–ankle acupuncture and codeine). Fifty-four patients with severe cancer pain were divided into three groups: wrist–ankle acupuncture, acupuncture combined with controlled-release morphine sulphate (MS Contin) and MS Contin. The pain-relief levels, side effects and the patients’ plasma β-endorphin levels and substance P levels were observed. These studies confirm the analgesic efficacy of wrist–ankle acupuncture therapy in cancer pain caused by hepatocarcinoma, especially in the treatment of moderate pain.
Hu et al. [26] assessed the effectiveness of wrist–ankle acupuncture in treating liver cancer pain. Eighty-six cases of liver cancer pain were divided into two groups, a treatment group (n = 36) treated with simple wrist–ankle acupuncture and a control group (n = 50) treated with simple medicine according to the 32-step analgesic principle. The therapeutic effects and side effects were compared. Wrist–ankle acupuncture was reported to have a therapeutic effect on liver cancer pain with no side effects and a longer analgesic period.
Sun et al. [27] tested the effects of acupuncture on advanced liver cancer pain using two randomised groups. One hundred forty patients were allocated to acupuncture (needle-retaining method of triple acupuncture, n = 80) on Ashi points or drug therapy (morphine hydrochloride, n = 40). The acupuncture group’s response rate showed greater improvement than the control group.
Stomach cancer
Mi et al. [27, 28] conducted an RCT to test the effectiveness of acupuncture plus fire needle for the treatment of cancer pain in comparison with the WHO three-step analgesic ladder drug therapy (WTSLDT). The results show that acupuncture together with the WTSLDT for treating stomach cancer pain (which is renowned for its efficacy) is worthy of clinical application. Adverse drug reactions occurred less frequently for the acupuncture group than the control group.
Dang et al. [29] compared the effects of acupuncture on cancer pain with the WTSLDT. The results from 48 cases of stomach cancer pain indicated that acupuncture, including the filiform needle group and the point-injection group, exhibited better therapeutic effects in the treatment of stomach cancer pain when the patient’s attention was focussed on the regional site of the disease.
Late-stage cancer
Chen et al. [30] evaluated whether acupuncture for the treatment of cancer pain was more effective than the three-step administration. Sixty-six cases of late cancer with pain were first divided into three different levels of pain (mild, moderate and severe), and patients with same degree of pain were randomly allocated into either an acupuncture (treated by acupuncture at three to five of the most severe tender points) or a medication group (treated with oral administration according to the WTSLDT, i.e. the patients with mild pain received aspirin while those with moderate pain received codeine and those with severe pain received morphine). The analgesic effect of the acupuncture treatment was more beneficial than the three-step administration protocol and caused no adverse effects or additional requirement of analgesics.
Qiao et al. [31] reported a significant difference in cancer pain between a treatment group (acupuncture group plus chemotherapy + WTSLDT, n = 33) and a control group (chemotherapy + WTSLDT, n = 30). In this study, the treatments were assessed using the clinical efficacy numerical scale for rating pain relief.
Miscellaneous
Peng et al. [32] conducted a study of cancer pain in which 22 patients were stratified into three levels of pain (light, moderate and severe pain) and were assigned to an acupuncture group or a placebo group according to a random number table, which resulted in 11 patients in each group. For the acupuncture group, a combination of electro-acupuncture and auricular needling was employed, and the selection of symptom-complexes (bian zheng) points was implemented based on the painful point and primary lesion points. For the placebo group, non-penetrating sham needling shallow puncture without electrostimulation, noninvasive ear needle and other placebo measures were employed. This study did not report a definite conclusion for the effectiveness of acupuncture for improving pain, quality of life and overall mental status.
Alimi et al. [33] assessed the efficacy of auricular acupuncture in the treatment of cancer pain. Ninety patients were randomly divided into three groups; one group received two courses of auricular acupuncture at points where an electrodermal signal had been detected, and two placebo groups received auricular acupuncture either at points with no electrodermal signal (not acupuncture points) or with auricular seeds fixed at the placebo points. Patients were required to be in pain and must have attained a Visual Analogue Scale (VAS) of 30 mm or more after having received analgesic treatment that was individualised for intensity and type of pain for at least 1 month of therapy. The treatment efficacy was based on the absolute decrease in VAS pain intensity measured 2 months after randomisation. The observed reduction in the pain intensity measured using the VAS represents a clear benefit from auricular acupuncture for cancer patients who are in pain despite stable analgesic treatment.
Zhang et al. [34] performed an RCT comparing acupuncture with drug therapy. Ninety cancer patients with varying degrees of pain received acupuncture analgesia, Chinese herbal medicine or oral medication according to the WTSLDT. The results showed that the analgesic effect in the acupuncture group and the Chinese herbs group was better compared with the Western-medicine group; this difference was highly significant. This study concluded that the analgesic effects of acupuncture and Chinese herbs on cancer pain were highly valued as clinical treatments.
Bian et al. [35] conducted an RCT to evaluate the effectiveness of acupuncture for the treatment of cancer pain. One hundred three patients were randomly divided into three groups: an electro-acupuncture group, a WTSLDT group and an electro-acupuncture plus WTSLDT group. The acupuncture plus WTSLDT group exhibited the most favourable effect on the response rate. A large amount of analgesics was required to reduce the side effects.
Dan [36] compared the effect of a single acupuncture treatment to the WTSLDT and acupuncture with WTSLDT. Acupuncture was more effective than WTSLDT for treating pain, and acupuncture plus WTSLDT demonstrated an even higher clinical efficacy for the treatment of cancer pain.
Chen et al. [37] reported that acupuncture demonstrated a statistically higher response rate compared with drug therapy. Sixty-two patients were included in an RCT to evaluate the effectiveness of acupuncture in comparison with WTSLDT for the treatment of cancer pain. Acupuncture plus WTSLDT was demonstrated to enhance the analgesic efficacy, reduce side effects, avoid the risk of opioid overdose and significantly improve the patients’ quality of life.
In a study by Shen et al. [38], 65 patients were randomly divided into a wrist–ankle acupuncture plus WTSLDT group and a WTSLDT-only group. The acupuncture group showed the most favourable improvements according to the patients’ responses. The authors concluded that acupuncture can be used for the routine treatment of patients with cancer pain and can improve the quality of life of cancer patients.
Finally, Xia et al. [39] compared the efficacy of acupuncture with either radiotherapy or chemotherapy. Seventy-six cases were randomly divided into two groups; 38 patients received acupuncture treatment, and 38 patients received radiotherapy or chemotherapy treatment. Two types of points were selected: specific points and points selected by pattern differentiation of the symptom complexes (bian zheng). The acupuncture group exhibited greater improvement than the control group.
Meta-analysis
Acupuncture versus drug therapy
Eight RCTs tested the effects of acupuncture compared with conventional drug therapies [25–27, 29, 30, 35–37]. The meta-analysis failed to show superior effects of acupuncture on pain relief (n = 886; RR, 1.12; 95% CI 0.98 to 1.28; P = 0.09), although there was a high level of heterogeneity (χ 2 = 24.21, P = 0.02, I 2 = 67%; Fig. 2). A subanalysis was performed to explore whether the heterogeneity could be partially explained by the type of cancer. The subgroup analysis indicated that no better improvements were observed after acupuncture treatment for any of the included types of cancer patients.

Forest plot of acupuncture for the treatment of cancer pain compared with drug therapy. AT: acupuncture
Acupuncture plus drug therapy versus drug therapy alone
Seven RCTs compared the effects of acupuncture plus conventional drug therapies on cancer pain with conventional drug therapy alone [25, 28, 31, 35–38]. All of the trials reported favourable effects of acupuncture on pain reduction. The meta-analysis showed superior effects of acupuncture combined with conventional drug therapy for pain reduction compared with conventional drug therapy alone (n = 437; RR, 1.36; 95% CI 1.13 to 1.64; P = 0.003) with high heterogeneity (χ 2 = 19.92, P = 0.003, I 2 = 70%; Fig. 3).

Forest plot of acupuncture plus drug therapy compared with drug therapy alone
Acupuncture versus sham acupuncture
Two RCTs assessed the effects of acupuncture on cancer pain compared with sham acupuncture [32, 33]. One RCT showed significantly favourable effects of acupuncture, while the other trial did not. The meta-analysis did not show significant effects of acupuncture on cancer pain reduction (n = 79; SMD, −0.41; 95% CI −1.39 to 0.49; P = 0.37; heterogeneity: χ 2 = 3.35, P = 0.07, I 2 = 70%; Fig. 4).

Forest plot of acupuncture compared with sham acupuncture
Adverse effects
Seven RCTs assessed adverse effects, while the others did not. None of the seven RCTs reported adverse events [25, 26, 28, 29, 31, 32, 39].
Discussion
The aim of this systematic review was to critically evaluate the effectiveness of acupuncture for the treatment of cancer pain. Several RCTs suggest that acupuncture can alleviate pain in patients with cancer. The majority of the individual studies suggested comparable effects of acupuncture and conventional drug therapy on cancer pain. However, whether the studies reporting no differences between acupuncture and conventional drug therapies reflect an equivalence of effects is unclear. The scarcity of trials, their low methodological quality, the small sample sizes and the results of the overall meta-analysis did not provide strong evidence in favour of acupuncture.
Our review aimed to update and complete the evidence by adding recent RCTs that examined the use of acupuncture for treating cancer pain [22, 23]. We identified eight new RCTs and updated the evidence [25, 26, 28, 30–32, 37, 38]. The results of our review are similar to the other two reviews [22, 23]. One previous review showed that acupuncture may be beneficial for controlling cancer pain [22, 23], while the other review reported insufficient evidence of an ability of acupuncture to alleviate cancer pain [22]. Both previous reviews also expressed concern regarding the poor methodological quality of the included primary studies.
Among all of the included studies, only four RCTs [30–33] adopted an adequate random sequence generation method, and only one RCT possessed a low risk of bias for allocation concealment; therefore, a serious selection bias should be considered when interpreting the results of these studies. Only small numbers of trials that included information on blinding the participants [33] and assessors [32, 33] were reported in this review; these factors can contribute to a performance and detection bias. Furthermore, only two studies reported dropout or withdrawals [31, 33]. We could not locate any online protocols registered before the start of the trials; therefore, all of the included studies exhibited an unclear risk of bias in the selective outcome reporting domain. As suggested by previous systematic reviews, these methodological flaws suggest that caution should be taken when interpreting the results of these studies and limit the original value of acupuncture [41, 42]. Future acupuncture trials should address these methodological quality issues so that a valid appraisal of the effectiveness or efficacy of acupuncture treatment for the treatment of cancer pain can be conducted.
The number of acupuncture treatment sessions varied according to the response of the patient. The extent to which acupuncture demonstrates therapeutic effects according to the duration and frequency of acupuncture is unclear. The optimum dose of acupuncture is unknown. The duration of the interventions was short in most studies. Arguably, longer treatment periods are required for acupuncture to have any chance of showing clinical effects. Therefore, future trails should incorporate sufficiently large samples and extended treatment and follow-up periods.
Several RCTs failed to mention adverse effects, which seems to conflict with research ethics and guidelines on reporting clinical trials. Acupuncture is not entirely free of adverse effects [43]. Non-reporting of adverse outcomes in clinical trials will generate an inaccurate profile concerning the safety of this treatment.
All of the included RCTs reported subjective symptom relief from the patients’ baseline cancer pain status. Pain studies rely heavily on subjective patient reports because of the lack of objective measurement tools. Presently, there is no universally accepted tool to assess cancer pain in the palliative care setting [44, 45]. Until a validated objective measurement for pain is developed, attempts to use psychometrically validated subjective outcomes, such as a self-administered diary or a health-related quality of life (QoL) questionnaire, a scientific and systematic approach to cancer pain assessment is necessary. This approach must involve extensive literature review, expert opinions and consensus, rigorous translation procedures and comprehensive validation [46]. The standard of cancer pain assessment could be enhanced using this methodology.
The majority of the RCT studies regarding the use of acupuncture for treating cancer pain are inconclusive. However, the effectiveness of acupuncture should be explored further with more rigorous studies because acupuncture continues to be widely used for this condition [18, 21] and in experimental studies [47, 48], which suggests that acupuncture may be an effective intervention for controlling cancer pain. Acupuncture may be effective in treating cancer-related pain for several reasons; for example, acupuncture may diminish pain induced by the direct infiltration of cancer or the compression of nerves as the tumour grows and in traction pain due to the rapid enlargement of the tumour or pain resulting from long-term confinement to bed [49]. The complete understanding of the mechanism of acupuncture remains unclear, but several mechanisms have been suggested to explain the analgesic effect of acupuncture in animal models. Acupuncture may alleviate pain by suppressing the expression of interleukin-1beta [50], one of the tumour-derived factors that sensitises primary afferent neurons to elicit cancer-related pain [51], and the expression of preprodynorphin [52] at the spinal cord level. The regulation of substance P and an increase in β-endorphin could also be responsible for the analgesic effect of acupuncture [53].
To determine whether acupuncture can effectively treat cancer pain, the selection of an appropriate control group is essential. The treatment of patients with acupuncture continues, but whether this treatment is beneficial remains unknown. Generally, complementary and alternative therapies have been assumed to be safe and pose minimal risk to patients. This assumption is not always correct. Acupuncture, however, is a relatively safe procedure when practiced by well-trained clinicians and acupuncturists who have detailed knowledge of human anatomy.
The results of this meta-analysis apply to traditional Chinese acupuncture (TCA) only. In TCA, a diagnosis is made in terms of a disturbance in the body’s ‘balance’, which is then corrected with needles. Western medical acupuncture (WMA) may appear to be similar to traditional Chinese acupuncture. However, there are considerable differences between the two approaches. In WMA, a medical diagnosis is made in the conventional manner, and needles are used to influence the physiology of the body according to the conventional view. WMA regards acupuncture as a conventional treatment along with drugs, surgery or any other treatment required for the patient [54, 55]. When WMA is administered in cancer patients with pain, conventional methods of medical history and examination are used with clinical investigations, if necessary, to establish a conventional diagnosis; however, judgement must be used to know when it is appropriate and when it is not appropriate to use acupuncture.
Our review has several limitations. Although considerable effort was made to retrieve all of the RCTs on the subject, we cannot be absolutely certain that we succeeded. Moreover, selective publishing and reporting are other major causes for bias and must be considered. It is conceivable that several negative RCTs remain unpublished, which would distort the overall picture [41, 42]. For the present review, no restrictions were placed on the review publication language, and a large number of different databases were searched. Therefore, we are confident that our search strategy located all of the relevant data on the subject. However, because all of the included research was conducted in China, a degree of uncertainty regarding the veracity of the findings remains. Further limitations include the paucity of published studies and often suboptimal quality of the primary data.
Future rigorous RCTs should be designed and conducted to evaluate whether acupuncture is an effective intervention for cancer pain. The studies need to incorporate accepted standards for trial design and reporting. Specifically, these studies should be based on proper power calculations for sample size, use validated outcome measures, control for nonspecific effects and adhere to modern human research ethics.
In conclusion, the results of this systematic review provide no strong evidence supporting the effectiveness of acupuncture in the management of cancer pain. However, the total number of RCTs included in the analysis and their methodological quality were both too low to draw firm conclusions. Further investigations seem warranted but must overcome the methodological shortcomings of the existing evidence.
References
American Pain Society (2008) Principles of analgesic use in the treatment of acute pain and cancer pain. 6th ed. Glenview, IL: American Pain Society
National Comprehensive Cancer Network (2010) Clinical practice guidelines in oncology for adult cancer pain. Fort Washington, PA: National Comprehensive Cancer Network: Available at: www.nccn.org. Accessed November 1, 2010
Burton AW, Fanciullo GJ, Beasley RD, Fisch MJ (2007) Chronic pain in the cancer survivor: a new frontier. Pain Med 8:189–198
Breivik H, Cherny N, Collett B, Fd C, Filbet M, Foubert AJ, Cohen R, Dow L (2009) Cancer-related pain: a Pan-European survey of prevalence, treatment, and patient attitudes. Ann Oncol 20:1420–1433
Hsieh RK (2005) Pain control in Taiwanese patients with cancer: a multicenter, patient-oriented survey. J Formos Med Assoc 104:913–919
Korean Society for Hospice and Palliative Care (2001) Cancer pain relief guideline. Seoul: Korean Society for Hospice and Palliative Care, Korean Cancer Study Group
Soyannwo O (2009) Cancer pain–progress and ongoing issues in Africa. Pain Res Manag 14:349
Koshy RC, Rhodes D, Devi S, Grossman SA (1998) Cancer pain management in developing countries: a mosaic of complex issues resulting in inadequate analgesia. Support Care Cancer 6:430–437
Quugley C (2008) Opioids in people with cancer-related pain. Clin Evid: 2408
Chen CH, Tang ST, Chen CH (2011) Meta-analysis of cultural differences in Western and Asian patient-perceived barriers to managing cancer pain. Palliat Med [Epub ahead of print]
Stjernsward J, Colleau SM, Ventafridda V (1996) The World Health Organization Cancer Pain and Palliative Care Program. Past, present, and future. J Pain Symptom Manage 12:65–72
van den Beuken-van Everdingen MH, de Rijke JM, Kessels AG, Schouten HC, van KM, Patijn J (2007) Prevalence of pain in patients with cancer: a systematic review of the past 40 years. Ann Oncol 18: 1437–1449
Harris J-D (2008) Management of expected and unexpected opioid-related side effects. Clin J Pain 24:S8–S13
Schug SA, Zech D, Grond S (1992) Adverse effects of systemic opioid analgesics. Drug saf 7:200–213
Cassileth B, Trevisan C, Gubili J (2007) Complementary therapies for cancer pain. Curr Pain Headache Rep 11:265–269
Cleary J (2007) The pharmacologic management of cancer pain. J Palliat Med 10:1369–1394
American College of Chest Physicians (2007) New ACCP cancer care guidelines include CAM. J Altern Complement Med 13:1049
Richardson MA, Sanders T, Palmer JL, Greisinger A, Singletary SE (2000) Complementary/alternative medicine use in a comprehensive cancer center and the implications for oncology. J Clin Oncol 18:2505–2514
Goudas LC, Bloch R, Gialeli-Goudas M, Lau J, Carr DB (2005) The epidemiology of cancer pain. Cancer Invest 23:182–190
Ernst E, Lee MS (2010) Acupuncture for palliative and supportive cancer care: a systematic review of systematic reviews. J Pain Symptom Manage 40:e3–e5
Filshie J, Thompson JW (2009) The Oxford textbook of palliative medicine. Oxford University Press
Lee H, Schmidt K, Ernst E (2005) Acupuncture for the relief of cancer-related pain: a systematic review. Eur J Pain 9:437–444
Peng H, Peng HD, Xu L, Lao LX (2010) Efficacy of acupuncture in treatment of cancer pain: a systematic review. J Chin Integr Med 8:501–509
Higgins JPT, Green S, eds. (2008) Chapter 8: Assessing risk of bias in included studies. In: Higgins J, Altman DG (eds) Cochrane handbook for systematic reviews of intervention. Wiley-Blackwell, West Sussex, England, pp. 187–241.
Hu X, Gu W, Zhou QH (2005) Analgesic efficacy and mechanism of wrist-ankle acupuncture on pain caused by liver cancer. Chin J Integr Med 15:131–133
Hu X, Ling CQ, Zhou QH (2004) Clinical observation on wrist–ankle acupuncture for treatment of pain of middle-late liver cancer. Chin Acupunct Moxibustion 24:149–151
Sun YL, Yu LR (2000) Observation on therapeutic effect of needle-retaining method of triple acupuncture in 80 cases of pain due to liver cancer. Chin Acupunct Moxibustion 21:211–212
Mi JP, Deng TW, Zhou DJ (2010) Clinical observation on fire acupuncture and three step analgesic ladder treatment for stomach cancer. Liaoning J Tradit Chin Med 37:2018–2019
Dang W, Yang JB (1998) Clinical study on acupuncture treatment of stomach carcinoma pain. J Tradit Chin Med 18:31–38
Chen ZJ, Guo YP, Wu ZC (2008) Observation on the therapeutic effect of acupuncture at pain points on cancer pain. Chin Acupunct Moxibustion 28:251–253
Qiao DP, Liu L, Liang YT (2008) Efficacy of acupuncture combined with drug treatment for cancer pain. J Pract Oncol 22:449–449
Peng H (2009) Systematic evaluation of the effect of acupuncture therapy on cancer pain and pilot clinical trial. Second Military Medical University: Masters degree, Shanghai, P.R. China
Alimi D, Rubino C, Pichard-Leandri E, Fermand-Brule S, Dubreuil-Lemaire ML, Hill C (2003) Analgesic effect of auricular acupuncture for cancer pain: a randomized, blinded, controlled trial. J Clin Oncol 21:4120–4126
Zhang M, Xia T, Wu SH, Zhang ZH, Zhang YJ (2000) Analgesic effect of Chinese herbs and acupuncture on cancer patients. Acupunct research 25:64–66
Bian RH (1999) Observation on analgesic effect of acupuncture on carcinous pain. J Pract Traditi Chin Med 15:28
Dan Y, Yang YB, Tao Y (1998) Clinical research on analgesic effect of acupuncture for pain in cancer. Chin Acupunct Moxibustion 19:17–18
Chen H, Liu Y (2002) Effective observations on treating cancerous pain by acupuncture and moxibustion and three levels analgesia. Chin J Pract Chin Mod Med 2:1125–1126
Shen SE (2000) Clinical investigation on analgesic effect of wrist-ankle needling in the patient of cancer. Chin Acupunct Moxibustion 21:143–144
Xia YQ, Zhang D, Yang CX, Xu HL, Li Y, Ma LT (1986) An approach to the effect on tumors of acupuncture in combination with radiotherapy or chemotherapy. J Tradit Chin Med 6:22–26
Kaptchuk TJ (2002) Acupuncture: theory, efficacy and practice. Ann Intern Med 136:374–383
Pittler MH, Abbot NC, Harkness EF, Ernst E (2000) Location bias in controlled clinical trials of complementary/alternative therapies. J Clin Epidemiol 53:485–489
Ernst E, Pittler MH (1997) Alternative therapy bias. Nature 385:480
Northeim AJ (1996) Adverse effects of acupuncture: a study of the literature for the years 1981–1994. J Altern Complement Med 2:291–297
Caraceni A, Brunelli C, Martini C, Zecca E, De Conno F (2005) Cancer pain assessment in clinical trials. A review of the literature (1999–2002). J Pain Symptom Manage 29:507–519
Carr DB, Goudas LC, Balk EM, Bloch R, Ioannidis JP, Lau J (2004) Evidence report on the treatment of pain in cancer patients. J Natl Cancer Inst Monogr 32:23–31
Kaasa S (2008) Palliative care research: time to intensify international collaboration. Palliat Med 22:301–302
Mao-Ying QL, Cui KM, Liu Q, Dong ZQ, Wang W, Wang J, Sha H, Wu GC, Wang YQ (2006) Stage-dependent analgesia of electro-acupuncture in a mouse model of cutaneous cancer pain. Eur J Pain 10:689–694
Wang JY, Xu L, Zhang RX, Lao L (2011) Traditional Chinese medicine for cancer pain. J Chin Integr Med 9:129–134
Paley CA, Johnson MI, Tashani OA, Bagnall AM (2011) Acupuncture for cancer pain in adults. Cochrane Database Syst Rev 19:CD007753
Zhang RX, Li A, Liu B, Wang L, Ren K, Qiao JT, Berman BM, Lao L (2007) Electroacupuncture attenuates bone cancer pain and inhibits spinal interleukin-1 beta expression in a rat model. Anesth Analg 105:1482–1488, Table of contents
Sabino MA, Mantyh PW (2005) Pathophysiology of bone cancer pain. J Support Oncol 3:15–24
Zhang RX, Li A, Liu B, Wang L, Xin J, Ren K, Qiao JT, Berman BM, Lao L (2008) Electroacupuncture attenuates bone-cancer-induced hyperalgesia and inhibits spinal preprodynorphin expression in a rat model. Eur J Pain 12:870–878
Lee HJ, Lee JH, Lee EO, Lee HJ, Kim KH, Lee KS, Lee CH, Nam DW, Kim SH, Lee HJ, Ahn KS (2009) Substance P and beta endorphin mediate electroacupuncture induced analgesic activity in mouse cancer pain model. Acupunct Electrother Res 34:27–40
White A (2009) Western medical acupuncture: a definition. Acupunct Med 27:33–35
White A, Cummings M, Filshie J (2008) An introduction to western medical acupuncture. Elsevier, UK
Acknowledgments
Tae-Young Choi and Myeong Soo Lee were supported by Korea Institute of Oriental Medicine (K11111 and K11130).
Conflict of interest
None declare.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 24 kb)
Rights and permissions
About this article
Cite this article
Choi, TY., Lee, M.S., Kim, TH. et al. Acupuncture for the treatment of cancer pain: a systematic review of randomised clinical trials. Support Care Cancer 20, 1147–1158 (2012). https://doi.org/10.1007/s00520-012-1432-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-012-1432-9