
Abstract
Background
Chemotherapy-induced neutropenia (CIN) places patients at risk of life-threatening infections. While reduction of chemotherapy dose or delay of the subsequent treatment cycle and, consequently, reduction of relative dose intensity (RDI) may limit myelotoxicity, these actions can also impact adversely on treatment outcome and should be avoided in adjuvant settings.
Patients and methods
Based on data from 444 breast cancer patients in the INC-EU Prospective Observational European Neutropenia Study, we have evaluated patient-specific and treatment-specific factors that impact on the incidence of grade 4 CIN (absolute neutrophil count <0.5 × 109/L), either during the first or in any cycle of (neo)adjuvant chemotherapy, across a range of regimens and doses.
Results
Using multivariate logistic regression analysis, risk factors for grade 4 CIN were identified as older age, lower weight, higher planned dose intensity of doxorubicin, epirubicin, or docetaxel, higher number of planned cycles, vascular comorbidity, lower baseline white blood cell count, and higher baseline bilirubin. Use of colony-stimulating factor before a neutropenic event occurred, dose delays, and dose reductions were protective against grade 4 CIN.
Conclusions
By identifying risk factors for grade 4 CIN, CSF prophylaxis may be appropriately targeted to prevent low RDI in patients treated with curative intent.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most common form of cancer among women in Europe, with an incidence of 110 per 100,000 and mortality of 25 per 100,000 in 2006 [1]. Disease-free survival (DFS) and overall survival (OS) rates have significantly improved in the last 30 years with the introduction of treatment with adjuvant chemotherapy in addition to surgery [2]. However, the benefits of adjuvant chemotherapy are largely dependent on optimal dose delivery, without dose delays and reductions [3–5]. In a 20-year follow-up study of women treated with cyclophosphamide, methotrexate, and 5-fluorouracil (CMF) for node-positive breast cancer, receiving full-dose chemotherapy (≥85%) impacted positively on DFS and OS [3]. A more recent study of anthracycline-based nontaxane chemotherapy regimens similarly showed benefits in DFS and OS for patients receiving full-dose and on-schedule chemotherapy (≥85%) [5]. The benefit of higher dose intensity for DFS and OS has also been demonstrated for adjuvant 5-fluorouracil, doxorubicin, and cyclophosphamide (FAC) chemotherapy in the treatment of node-positive breast cancer [4].
Chemotherapy frequently results in severe chemotherapy-induced neutropenia (grade 4 CIN; absolute neutrophil count [ANC] <0.5 × 109/L) and febrile neutropenia (FN; ANC <0.5 × 109/L and temperature ≥38°C). Myelosuppression puts patients at risk of life-threatening infection. In Europe, it is common practice in many hospitals to delay or reduce chemotherapy doses in an effort to minimize this risk or in response to the occurrence of a myelosuppressive event or low neutrophil nadir. For example, Chirivella et al. reported that, in their hospital it was standard protocol to delay chemotherapy by 5–7 days even at lower grades of neutropenia, if the neutrophil count was <1.5 × 109/L or if the platelet count was <100 × 109/L [5]. The Neulasta [pegfilgrastim] versus Current Practice (NeuCuP) integrated analysis also demonstrated the occurrence of dose delays in current practice [6]. Consequently, patients receive reduced relative dose intensity (RDI) [7]. We have previously reported that the practice of dose delays and reductions affects a high proportion of breast cancer patients; 34% of patients in the INC-EU Prospective Observational European Neutropenia Study experienced grade 4 CIN, over 20% received a reduced RDI (≤85%), and grade 4 CIN was a significant predictor of low RDI, dose delays, and dose reductions [8].
Colony-stimulating factor (CSF) primary prophylaxis can be used to support chemotherapy delivery by reducing the duration of severe neutropenia [9–12]. Current European Organisation for Research and Treatment of Cancer (EORTC) guidelines recommend primary prophylaxis for patients where reductions in dose intensity have been shown to result in poorer prognosis, even where the overall FN risk is low [10].
The aim of the present analysis was to evaluate factors that predict grade 4 CIN in early stage breast cancer patients treated with curative intent, a patient group for whom delivery of full RDI has been shown to benefit survival [3–5]. By identifying risk factors, protective measures may be targeted towards patients most at risk of developing neutropenia and subsequent chemotherapy dose delays and reductions.
Materials and methods
Study design and patient selection
The study design and patient selection have previously been described in detail [8]. Briefly, the INC-EU Prospective Observational European Neutropenia Study involved 749 patients with histologically confirmed breast cancer, non-Hodgkin lymphoma, or Hodgkin lymphoma enrolled at 66 centers in Belgium, France, Germany, Spain, and the UK between January 2004 and May 2005. Ethical approval was obtained from all participating centers, and all patients provided informed consent. The present analysis covers a subset of 444 breast cancer patients. Patients eligible for inclusion required adjuvant or neoadjuvant chemotherapy for grade I–III breast cancer, with at least four cycles of a myelosuppressive chemotherapy regimen sequence planned. Permitted chemotherapy regimens included anthracycline-containing regimens including doxorubicin and cyclophosphamide (AC), epirubicin and cyclophosphamide (EC), FAC, 5-fluorouracil, epirubicin, and cyclophosphamide (FEC), and epirubicin, cyclophosphamide, methotrexate, and 5-fluorouracil (E-CMF); taxane-containing or sequential regimens including docetaxel, doxorubicin, and cyclophosphamide (TAC); and CMF.
Statistical methods
From an initial set of covariates considered to be potential predictors of grade 4 CIN (ANC <0.5 × 109/L), based on biomedical/clinical reasoning and given earlier published reports, candidate model covariates were preselected on the basis of statistical criteria (presence of an association with p ≤ 0.25 in standard univariate analysis) and clinical relevance. Subsequently, multivariate logistic regression models of grade 4 CIN occurrence in any cycle and in cycle 1 were developed. Main effects were identified through manual exploration of all plausible combinations of candidate covariates. Generalized estimation equations-based robust standard error estimates were used to allow for clustering by study center. For candidate predictors with more than 5% missing values, missing categories were introduced in order to avoid loss of observations. Sensitivity analyses were performed to address concerns that this approach can lead to biased estimation results [13, 14].
Model fit was assessed using the Hosmer–Lemeshow goodness of fit test and plots of mean observed versus mean predicted event probabilities, by deciles of the linear predictor. Predictive ability of the models was characterized by sensitivity and specificity, positive predictive value and negative predictive value (PPV and NPV, respectively), the area under the receiver operating characteristic (ROC) curve, and the total proportion of correct predictions. The ability of the models to predict lower grades of CIN ≥3 (ANC <1.0 × 109/L) or ≥2 (ANC <1.5 × 109/L) was also tentatively determined. Tenfold cross-validation was performed in the absence of an independent validation dataset. Finally, clinical utility of the “any cycle” model was assessed by applying the model to hypothetical case scenarios.
The initial set of potential predictors of grade 4 CIN in any cycle included patient factors, baseline laboratory measures and comorbidities, frequency of hematology laboratory tests, planned treatment characteristics, and actual treatment characteristics before a grade 4 CIN occurred. For the model of grade 4 CIN occurrence in cycle 1 of chemotherapy, an appropriate subset of these covariates was considered.
Results
Patient and treatment characteristics
Patient and baseline disease characteristics are shown in Table 1. The majority of patients (70%) received anthracycline-based treatments; the remaining patients received anthracycline-containing and taxane-containing sequential regimens (20%), TAC (4%), other taxane-containing regimens (2%), or CMF (4%). Patients receiving nonsequential chemotherapy regimens were planned for four cycles (25%) or six cycles (72%) in the vast majority of cases. Patients receiving sequential regimens were typically planned for six cycles (10%) or eight cycles (89%). Cycles were 3 weeks long in most cases. Primary CSF prophylaxis was provided to 9% of patients overall (5% for anthracycline-based regimens, 14% for anthracycline-containing and taxane-containing regimens, 71% for TAC, and 11% for CMF), and secondary CSF prophylaxis or treatment was provided to a further 24% of patients.
Incidence of CIN
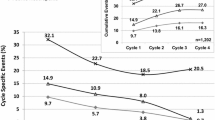
Overall, grade 4 CIN occurred in around a third of patients (152 out of 442; 34%) at some stage during their treatment (Table 2) and was most frequent in patients receiving TAC chemotherapy (seven out of 17; 44%). Over two thirds of all grade 4 CIN events (107 out of 152; 70%) occurred during the first cycle of treatment, and almost one in four breast cancer patients (107 out of 442; 24%) experienced first cycle grade 4 CIN. Lower grades of CIN were also frequent. Across all cycles, maximum CIN grades of 3, 2, and 1 were seen in 132 (30%), 72 (16%), and 67 (15%) of 442 patients, respectively. Only 19 patients (4%) experienced no CIN.
Chemotherapy dose limitations
Patients were more likely to receive a reduced RDI (≤85%) if they experienced grade 4 CIN whether in the first cycle of chemotherapy or at any other point during treatment (Table 3). In patients without grade 4 CIN, the risk of RDI ≤85% was 17% (95% confidence interval [95% CI], 13–22%), whereas in patients with grade 4 CIN in any cycle, the risk of RDI ≤85% was 28% (95% CI, 21–36%). The occurrence of grade 4 CIN in any cycle of chemotherapy was also significantly associated with dose delays (≥4 days; odds ratio [OR], 1.57; 95% CI, 1.02–2.40) and dose reductions (≥10% of planned dose; OR, 1.86; 95% CI, 1.16–2.97).
Predictors of CIN
Significant risk factors associated with the occurrence of grade 4 CIN in any cycle of chemotherapy were identified using logistic regression analysis (Table 4). These were older age, lower weight, higher planned dose intensity of doxorubicin, epirubicin, or docetaxel, higher number of planned cycles, vascular comorbidity, lower baseline WBC count, and higher baseline bilirubin. A higher number of hematology laboratory tests per cycle and availability of a cycle 1 nadir hematology laboratory test were also shown to be significant in the model, but this may be related to patient management and not a direct correlation between these tests and CIN. The model also identified factors that protected against grade 4 CIN; these were CSF use, dose reductions, and dose delays, all before an event occurred.
We investigated whether weight may have been identified as a predictor of grade 4 CIN because body surface area (BSA)-based chemotherapy dosing leads to higher chemotherapy dose per kilogram of body weight in lighter patients. Consistent with this hypothesis, substantial and highly significant negative correlations between BSA and dose per kilogram body weight were found for a wide range of antimalignant substances. For example, the correlation between BSA and absolute doxorubicin dose per kilogram body weight in the first cycle of chemotherapy was −0.76 for TAC (N = 88; p < 0.001) and −0.81 for AC chemotherapy (N = 17; p < 0.001; Fig. 1).

Scatter plot of absolute doxorubicin dose per kilogram body weight in the first cycle of chemotherapy and BSA at baseline. AC Adriamycin (doxorubicin) 60 mg/m2 and cyclophosphamide 600 mg/m2, TAC Taxotere (docetaxel) 75 mg/m2, doxorubicin 50 mg/m2, and cyclophosphamide 500 mg/m2
The model correctly classified 320 of 434 patients (73%). The area under the ROC curve was 0.82 (95% CI, 0.78–0.86) and test characteristics (using the cut-off with the best ability to discriminate between occurrence and nonoccurrence of grade 4 CIN) were sensitivity 73%, specificity 74%, PPV 59%, and NPV 84%. Under tenfold cross-validation conditions, the area under the ROC curve was 0.78 (95% CI, 0.63–0.93), demonstrating that predictive ability was only modestly decreased.
Risk factors for the occurrence of grade 4 CIN in the first cycle of chemotherapy were also modeled by logistic regression. Factors associated with a significant risk of or protection against grade 4 CIN were broadly consistent with the “any cycle” model with the exception of high baseline bilirubin, low baseline white blood cell (WBC) count, and age, which showed consistent direction of effects, but only reached statistical significance in the “any cycle” model. The area under the ROC curve for the “cycle 1” model was 0.73 (95% CI, 0.68–0.78). The PPV was 38% and the NPV was 86%.
When the “any cycle” model was tentatively used to predict CIN grades of 3 or higher, the area under the ROC curve was 0.71 (95% CI, 0.66–0.76), and PPV and NPV were 77% and 51%, respectively. Prediction for the first cycle yielded an area under the ROC curve of 0.71 (95% CI, 0.66–0.75). PPV was 62% and NPV was 64%. For CIN grades of 2 or higher, ROC results were similar, but the shift of predictive ability towards higher PPV and lower NPV was stronger, given that 83% of patients experienced this endpoint.
Patient scenarios
Table 5 shows the predicted risk of grade 4 CIN during any cycle of chemotherapy for a selection of hypothetical patients presenting various risk factors. Hypothetical subjects of either 70 kg (the median weight of the breast cancer study population) or 55 kg received chemotherapy with either FEC followed by docetaxel (FEC-T) or TAC. This table of predicted risk is based on the assumption that no CSF support was given. Lower weight increased the risk of grade 4 CIN at any age and for both types of chemotherapy regimen, and the highest risk was in subjects with multiple risk factors.
Discussion
In this sample of breast cancer patients receiving chemotherapy treatment, multivariate analyses were used to identify risk factors for grade 4 CIN. Patient characteristics contributing to increased risk were higher age and lower weight, vascular comorbidity and levels of some baseline laboratory measures, specifically low baseline WBC count and high baseline bilirubin. Treatment factors that increased risk of grade 4 CIN were high planned chemotherapy dose intensity, a higher number of planned chemotherapy cycles, and a higher number of hematology laboratory tests measured per cycle. CSF use, dose reductions, or dose delays, all before a neutropenic event occurred, protected against grade 4 CIN.
The relationship between increased risk of myelotoxicity and older age is well established and is incorporated in both European and American clinical practice guidelines [10–12]. Lower weight may increase the risk of grade 4 CIN as a result of drug dosing by BSA; as lighter patients are exposed to more chemotherapy per kilogram of body weight, this may result in higher toxicity. In our sample, this assumption was supported by significant correlations observed between dose per kilogram of each chemotherapy agent and BSA.
In our model, a strong predictor for grade 4 CIN was high baseline bilirubin, which is indicative of impaired liver function [15]. Baseline bilirubin level may be a particularly important predictive factor in patients receiving chemotherapy with doxorubicin, epirubicin, or docetaxel, as these agents are detoxified by the liver rather than excreted by the kidneys [16]. Baseline laboratory measures of pretreatment ANC and WBC count have been shown to predict neutropenic events in breast cancer patients receiving FEC chemotherapy [17], consistent with the present finding that low baseline WBC was a risk factor for grade 4 CIN. From our dataset, we could not confirm an independent role of lymphocyte count, which has been reported by some authors [17–19].
High planned chemotherapy dose intensity of doxorubicin, epirubicin, or docetaxel was a risk factor for grade 4 CIN. Using planned chemotherapy dose intensity as a measure of the myelosuppressive potential of a regimen allows comparison between different regimens and between ranges of planned drug doses within the same regimen (for example, in this study, epirubicin doses in FEC regimens ranged from 50 to 120 mg/m2 BSA). As the model was derived from data that reflect the “real-life” clinical situation of dose variation, it can potentially be used in clinical practice to predict grade 4 CIN in breast cancer patients across a variety of regimens and doses. It should be noted, however, that correlations with the use of other antimalignant agents may have masked the contribution of those agents to the neutropenic potential of the chemotherapy regimens studied. Validation against an independent dataset is pending.
The average number of hematology laboratory tests per cycle at each study site (averaged across patients) and the presence of a nadir hematology laboratory test in cycle 1 were significant predictive factors for grade 4 CIN. The most probable explanation for this is that grade 4 CIN is more likely to be detected at sites which tend to perform more hematology laboratory tests. This observation raises the possibility that neutropenic events may be underreported.
Consistent with current literature, CSF prophylaxis was strongly protective against grade 4 CIN [10, 12, 20]. Dose reductions and dose delays before an event occurred were also identified as protective factors against grade 4 CIN; although they may be an appropriate course of action to limit neutropenia in patients receiving palliative treatment, in an adjuvant setting, reductions in chemotherapy dose intensity have been shown to impact negatively on treatment outcome [2–5]. Current EORTC and American Society of Clinical Oncology guidelines recommend CSF use to support dose dense or dose intense regimens that have survival benefits where reductions in intensity or density are known to be associated with a poor prognosis or where a regimen ± risk factors is associated with a >20% risk of FN [10, 12].
A recent model identified risk factors for FN or grade 4 CIN across multiple chemotherapy cycles in early stage breast cancer patients in the US that were broadly similar to those identified in our analysis [21]. The planned intensity of different chemotherapy regimens impacted on the risk of neutropenia in both models; in the US model, TAC regimens were associated with the highest neutropenia risk, consistent with the identification of planned dose intensity of doxorubicin, epirubicin, or docetaxel as predictors in the present model. Baseline bilirubin was a risk factor for neutropenic events in both models, as was baseline WBC. Lower glomerular filtration rate, predictive of neutropenic events in the US model, was a replacement for age. CSF use was protective against neutropenia in both analyses.
Risk and protective factors we identified for grade 4 CIN in any cycle of chemotherapy were also identified in a model for the first cycle of chemotherapy. Effect sizes were comparable, although some covariates were no longer statistically significant, presumably due to the lower number of events in the first cycle analysis. The only substantial reduction in effect size was seen in baseline bilirubin. It is possible that, after one cycle of chemotherapy, liver function was not sufficiently impaired to affect chemotherapy drug metabolism, but with repeated exposure to chemotherapy agents, this impairment could have become more pronounced.
Our model showed good predictive ability, correctly classifying 73% of grade 4 CIN patients and with an NPV of 84%. Some predictive ability was maintained when the endpoint was modified to include lower CIN grades. The role of individual, intrinsic chemosensitivity, which we cannot adequately predict to date, may make it difficult to achieve better test characteristics in neutropenia risk models [17]. The model performed well in tenfold cross-validation but remains to be validated further against an independent dataset.
To evaluate its potential clinical utility, the model was applied to scenarios of hypothetical patients treated with FEC-T, representative of a taxane–anthracycline sequential therapy, which has been demonstrated to be efficacious in the treatment of breast cancer [22], and TAC, representative of a more myelotoxic regimen [10]. Older and lower weight patients were shown to have a higher predicted risk of grade 4 CIN, independent of other risk factors. The highest risk of neutropenia was in patients with multiple risk factors.
The identification of risk factors for grade 4 CIN has important clinical implications. Current guidelines recommend CSF use not only when the overall risk of FN is >20%, but also to allow maintenance of chemotherapy dose. Few patients in this dataset experienced FN; however, grade 4 CIN was frequent and was associated with chemotherapy dose delays, reductions, and low RDI. A higher proportion of patients who had grade 4 CIN received low RDI, compared to patients without grade 4 CIN. The issue of impaired RDI achievement in routine practice deserves greater attention. When the 20-year outcome results from the Bonadonna study [3] are applied in different breast cancer populations, the findings are similar; namely, a lower than planned dose intensity is associated with inferior long-term DFS and OS [23].
In conclusion, we have identified several risk factors for grade 4 CIN in breast cancer patients receiving adjuvant chemotherapy in the European practice. Our model provides a broad list of risk factors applicable across a range of chemotherapy regimens. Such risk factors may be considered by clinicians identifying patients vulnerable to dose reductions and delays, which may ultimately compromise chemotherapy delivery, to enable appropriate targeting of supportive care.
References
Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P (2007) Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol 18(3):581–592
Bonadonna G, Moliterni A, Zambetti M, Daidone MG, Pilotti S, Gianni L, Valagussa P (2005) 30 years' follow up of randomised studies of adjuvant CMF in operable breast cancer: cohort study. Br Med J 330(7485):217
Bonadonna G, Valagussa P, Moliterni A, Zambetti M, Brambilla C (1995) Adjuvant cyclophosphamide, methotrexate, and fluorouracil in node-positive breast cancer: the results of 20 years of follow-up. N Engl J Med 332(14):901–906
Budman DR, Berry DA, Cirrincione CT, Henderson IC, Wood WC, Weiss RB, Ferree CR, Muss HB, Green MR, Norton L, Frei E 3rd (1998) Dose and dose intensity as determinants of outcome in the adjuvant treatment of breast cancer. The Cancer and Leukemia Group B. J Natl Cancer Inst 90(16):1205–1211
Chirivella I, Bermejo B, Insa A, Perez-Fidalgo A, Magro A, Rosello S, Garcia-Garre E, Martin P, Bosch A, Lluch A (2009) Optimal delivery of anthracycline-based chemotherapy in the adjuvant setting improves outcome of breast cancer patients. Breast Cancer Res Treat 114(3):479–484
von Minckwitz G, Schwenkglenks M, Skacel T, Lyman G, Lopez-Pousa A, Bacon P, Easton V, Aapro M (2009) Febrile neutropenia and related complications in breast cancer patients receiving pegfilgrastim primary prophylaxis versus current practice neutropenia management: results from an integrated analysis. Eur J Cancer 45(4):608–617
Leonard RC, Miles D, Thomas R, Nussey F (2003) Impact of neutropenia on delivering planned adjuvant chemotherapy: UK audit of primary breast cancer patients. Br J Cancer 89(11):2062–2068
Pettengell R, Schwenkglenks M, Leonard R, Bosly A, Paridaens R, Constenla M, Szucs TD, Jackisch C (2008) Neutropenia occurrence and predictors of reduced chemotherapy delivery: results from the INC-EU prospective observational European neutropenia study. Support Care Cancer 16(11):1299–1309
Kuderer NM, Dale DC, Crawford J, Lyman GH (2007) Impact of primary prophylaxis with granulocyte colony-stimulating factor on febrile neutropenia and mortality in adult cancer patients receiving chemotherapy: a systematic review. J Clin Oncol 25(21):3158–3167
Aapro MS, Cameron DA, Pettengell R, Bohlius J, Crawford J, Ellis M, Kearney N, Lyman GH, Tjan-Heijnen VC, Walewski J, Weber DC, Zielinski C (2006) EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphomas and solid tumours. Eur J Cancer 42(15):2433–2453
National Comprehensive Cancer Network Inc. (2008) NCCN clinical practice guidelines in oncology—breast cancer V.2.2008. Available at http://www.nccn.org/professionals/physician_gls/PDF/breast.pdf. Accessed on 5 December 2008
Smith TJ, Khatcheressian J, Lyman GH, Ozer H, Armitage JO, Balducci L, Bennett CL, Cantor SB, Crawford J, Cross SJ, Demetri G, Desch CE, Pizzo PA, Schiffer CA, Schwartzberg L, Somerfield MR, Somlo G, Wade JC, Wade JL, Winn RJ, Wozniak AJ, Wolff AC (2006) 2006 update of recommendations for the use of white blood cell growth factors: an evidence-based clinical practice guideline. J Clin Oncol 24(19):3187–3205
Greenland S, Finkle WD (1995) A critical look at methods for handling missing covariates in epidemiologic regression analyses. Am J Epidemiol 142(12):1255–1264
Vach W, Blettner M (1991) Biased estimation of the odds ratio in case–control studies due to the use of ad hoc methods of correcting for missing values for confounding variables. Am J Epidemiol 134(8):895–907
Field KM, Dow C, Michael M (2008) Part I: liver function in oncology: biochemistry and beyond. Lancet Oncol 9(11):1092–1101
Hladnik M, Wills AR, Augustin KM (2007) Systemic chemotherapy: special considerations. In: The Washington manual of oncology, 2nd ed. Lippincott Williams and Wilkins, pp 30–32
Jenkins P, Freeman S (2009) Pretreatment haematological laboratory values predict for excessive myelosuppression in patients receiving adjuvant FEC chemotherapy for breast cancer. Ann Oncol 20:34–40
Blay JY, Chauvin F, Le Cesne A, Anglaret B, Bouhour D, Lasset C, Freyer G, Philip T, Biron P (1996) Early lymphopenia after cytotoxic chemotherapy as a risk factor for febrile neutropenia. J Clin Oncol 14(2):636–643
Borg C, Ray-Coquard I, Philip I, Clapisson G, Bendriss-Vermare N, Menetrier-Caux C, Sebban C, Biron P, Blay JY (2004) CD4 lymphopenia as a risk factor for febrile neutropenia and early death after cytotoxic chemotherapy in adult patients with cancer. Cancer 101(11):2675–2680
Komrokji RS, Lyman GH (2004) The colony-stimulating factors: use to prevent and treat neutropenia and its complications. Exp Hematol 4(12):1897–1910
Culakova E, Wolff DA, Poniewierksi MS, Crawford J, Dale DC, Lyman GH (2008) Factors related to neutropenic events in early stage breast cancer patients. J Clin Oncol 26(Suppl):Abstract 634
Roche H, Fumoleau P, Spielmann M, Canon JL, Delozier T, Serin D, Symann M, Kerbrat P, Soulie P, Eichler F, Viens P, Monnier A, Vindevoghel A, Campone M, Goudier MJ, Bonneterre J, Ferrero JM, Martin AL, Geneve J, Asselain B (2006) Sequential adjuvant epirubicin-based and docetaxel chemotherapy for node-positive breast cancer patients: the FNCLCC PACS 01 Trial. J Clin Oncol 24(36):5664–5671
Kahlert S, Rosenfeld J, Mair K, Sorokina Y, Engel J, and Friese K (2008) Adjuvant chemotherapy for breast cancer prognostic impact of relative dose–intensity. 31st Annual San Antonio Breast Cancer Symposium (SABCS), Abstract 4109
Acknowledgements
The authors would like to thank the following physicians for providing patient data: J.C.A. Adansa; J.J.C. Hernandez; S. Al-Ismail; C. André; G.-A. Banat; A. Barnes; A.L. Barriuso; J.L. Bello; A. Biswas; A. Bols; A. Brownell; W. Brugger; R.O. Casasnovas; M. Clemens; R. Coleman; P. Colombat; N. Davidson; R. Depenbusch; H.G. Derigs; A. Engert; J.C. Espinosa; S. Ferrer; O. Fitoussi; B. Gaede; L. Garderet; B. Hancock; M. Hänel; A. Hasenburg; A. Hong; U. Karck; G. Köhler; A.W. Hutcheon; C. Lerchenmüller; R. Lipp; J.R.M. Lorenzo; K. McAdam; F. Majois; J.L. Mansi; M.G. Martinez; J. Mebis; N. Mounier; A.A. Munoz; A. O’Callaghan; M. Quigley; S. Rösel; C. Rudin; R. Schlag; G. Schlimok; M. Sandherr; P. Solal-Celigny; T. Steck; H. Tesch; D. Turner; X. Vallantin; J. Van Erps; E. Van Den Neste; A. Van Hoof; J.B. Vermorken; K. Verpoort; A. Wardley; M. Warm; E. Weidmann; J. Wimperis; W. Zeller. The authors wish to thank Prof. Gary Lyman, Duke University and the Duke Comprehensive Cancer Center, Durham, North Carolina and members of the Awareness of Neutropenia in Chemotherapy (ANC) Study Group for the useful discussions comparing risk models. The authors wish to thank Amgen (Europe) GmbH, Zug, Switzerland for supporting this work with an educational grant. The authors wish to thank medcept ltd., Switzerland, who provided medical writing support to the INC-EU with funding from Amgen (Europe) GmbH.
Conflicts of interest
This study was supported by an educational grant from Amgen (Europe) GmbH. M.S. receives research funding from Amgen and acts as a consultant in receipt of honoraria from Amgen. R.P. is a consultant in receipt of honoraria from Chugai, Bayer, Roche, and Amgen. C.J. is a consultant in receipt of honoraria from Amgen and Astra Zeneca. R.Pa. is a consultant in receipt of honoraria from Astra Zeneca, Novartis, Pfizer, Sanofis, and Schering-Plough and receives research funding from Amgen, Novartis, and Pfizer. M.C. has no conflicts of interest to declare. A.B. receives research funding from Amgen. T.S. has no conflicts of interest to declare. R.L. has modest share ownership interest in GlaxoSmithKline, is a consultant in receipt of honoraria from Amgen, Astra Zeneca, Novartis, Pfizer, Roche, and Zeneus, and was in receipt of research funding from Amgen.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schwenkglenks, M., Pettengell, R., Jackisch, C. et al. Risk factors for chemotherapy-induced neutropenia occurrence in breast cancer patients: data from the INC-EU Prospective Observational European Neutropenia Study. Support Care Cancer 19, 483–490 (2011). https://doi.org/10.1007/s00520-010-0840-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-010-0840-y