
Abstract
Purpose
This study aims to develop a psychometrically rigorous instrument to measure the unmet needs of adult cancer survivors who are 1 to 5 years post-cancer diagnosis. “Unmet needs” distinguishes between problems which survivors experience and problems which they desire help in managing.
Methods
The survey was developed from a comprehensive literature review, qualitative analysis of the six most important unmet needs of 71 cancer survivors, review of the domains and items by survivors and experts, cognitive interviews and a pilot test of 100 survivors. A stratified random sample of 550 cancer survivors, selected from a population-based Cancer Registry, completed a mailed survey to establish reliability and validity.
Results
The final 89-item Survivors Unmet Needs Survey (SUNS) has high acceptability, item test–retest reliability and internal consistency (Chronbach’s alpha 0.990), face, content and construct validity. Five subscales measure Emotional Health needs (33 items, 19.4% of variance), Access and Continuity of Care (22 items, 15.1%), Relationships (15 items, 12.1%), Financial Concerns (11 items, 10.3%) and Information needs (eight items, 8.1% of the variance).
Conclusions
This instrument has strong psychometric properties and is useful for determining the prevalence and predictors of cancer survivors’ unmet needs across types of cancer, length of survivorship and socio-demographic characteristics. Use of the SUNS will enable more effective targeting of programmes and services and guide policy and health planning decisions.
Relevance
This study is an important step toward evidence-based planning and management of problems which the growing survivor population requires assistance in managing.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Despite relatively stable incidence rates, the prevalence of cancer is increasing due to advances in treatment, longer survival and ageing of the baby boom generation [1–3]. IARC estimates 25 million people worldwide live with cancer [4]. In North America, 2% to 5% of the population live with a cancer diagnosis [5, 6] and researchers predict that the number of survivors will double by 2030 [6]. It is important that health care planners and policymakers understand the needs of this population.
Many survivors experience physical, psychosocial, functional and cognitive problems related to the disease and/or treatment [7–9]. Survivors may experience metastatic disease, recurrence and increased risk of new primary cancers [7, 10]. Fatigue and reduced participation in daily living and leisure activities are common [8]. Return to work, employability, insurance eligibility and coverage, household management and financial security have also been identified as concerns [11–14]. Almost two thirds of cancer survivors are over the age of 65 and may also be coping with other comorbid conditions and functional limitations [15, 16].
Most of the existing cancer-related quality of life instruments ask about problems experienced, but not whether help is required to manage those problems. Two recent publications note significant differences between what health professionals identify as patient problems requiring intervention and what patients indicate they need professional assistance to manage [18, 19]. A needs-based research approach can identify problems survivors experience, whether they desire professional assistance with their problems and if so, the extent of the assistance required [20, 27]. Osse et al. [18] found only two of 15 palliative cancer care questionnaires that were formatted in such a way that the need for help could be assessed. Likewise, Pearce et al. [17] found only two out of nine cancer survivor quality of life instruments that measured the need for assistance. The Cancer Survivors’ Unmet Needs (CaSUN) [21] and the Supportive Care Needs Survey (SCNS) Survivor Module [22] use a needs-based approach and were validated with survivors recruited from hospital oncology clinics. The CaSUN included disease-free survivors of breast, gynaecological, prostate and colorectal cancers and the SCNS early stage breast cancers. The sampling frame (hospital oncology clinics) and survivor characteristics used in developing the SCNS and CaSUN provide validity for similar settings and types of cancers, but not for survivors with recurrent disease, those followed in the community or with other types of cancer which make up 35% to 40% of prevalent cases [5, 23].
These findings highlight the critical need for a psychometrically rigorous instrument that can identify significant issues shared by a broad range of cancer survivors, allow for the examination of needs disparities across geographic areas, policy jurisdictions, socio-demographic characteristics and types of cancer. Such an instrument will enable more effective targeting of programmes and services and be useful in examining the effectiveness of interventions. The term “unmet needs” is used to distinguish between problems which survivors experience and problems they wish help in managing [20, 27–30] and is defined as “a requirement for some desirable, necessary or useful action to be taken or some resource to be provided, in order to attain optimal well-being” [20, pp.227].
Criteria for psychometrically rigorous instruments recommend the instrument (1) has acceptable reliability and validity; (2) measures the multi-dimensional nature of cancer-related needs; (3) collects data directly from subjects; (4) is responsive to changes over time; (5) is acceptable to subjects and easy to complete; and (6) is feasible to administer in the setting in which it will be used [24–26].
Reliability is assessed by intra-class correlation coefficient or kappa as a measure of reproducibility for items in the scale over time. Cronbach’s alpha is commonly used as a measure of internal consistency [25, 26]. Face and content validity, assessed by having subject experts and the target audience review the instruments, determines whether the survey makes sense and if it represents the concept of unmet needs. Construct validity, established using factor analysis, provides a quantitative measure of whether the instrument is measuring what is intended [24, 25].
Methods
Aim of the study
To develop a psychometrically rigorous instrument to measure the unmet needs of adult cancer survivors who are 12 to 60 months post-cancer diagnosis.
Development of the survivor unmet needs survey
Literature review
An extensive review of published and unpublished literature on general health, quality of life, unmet needs of cancer patients and cancer survivorship identified existing domains and items for possible inclusion in our instrument.
Cancer survivor input
Cancer survivors who were over age 18 years and at least 1 year post-diagnosis were recruited by the Canadian Cancer Society from six provinces and one territory. They were mailed an open-ended survey which asked them to list their six most important unmet needs in the last month. Seventy-one of 74 survivors (20 males, 51 females) met the eligibility criteria. The majority (74.6%) were between 1 and 5 years post-diagnosis and had finished treatment (69.0%) with 18.3% in follow-up, remission or cancer-free, 7.0% dealing with a recurrence and three (4.2%) receiving treatment. One third (35.2%) had breast cancer, one third (32.4%) reported other cancers (bladder, brain, larynx, leukaemia, melanoma, multiple myeloma, nasopharyngeal, neuroblastoma, ovarian, penile, stomach, testicular, thyroid, tongue, uterus), followed by lymphoma (12.7%), colorectal (8.5%), lung (5.6%) or prostate (5.6%) cancers. Unmet needs were coded independently by two researchers and discrepancies discussed to reach consensus. Domains and needs were merged with those identified in the literature, duplicate items were eliminated and a draft instrument with 200 items in nine domains was created.
Professional input
A panel of behavioural scientists, psychosocial health care providers and Canadian Cancer Society support staff reviewed the draft instrument for relevance and completeness. Wording clarifications were made, redundant and overlapping items were removed resulting in 160 items in six domains.
Feedback from cancer survivors
Telephone interviews using modified cognitive interviewing techniques were conducted with a sub-sample of the survivors who had participated in generating items to examine face and content validity, relevance, ease of understanding and acceptability. Eight more items were eliminated.
Readability/acceptability
The reading level, organisation and presentation of the draft version were assessed by the Plain Language Service, Canadian Public Health Association [31], to attain a grade 4 to 6 reading and comprehension level.
Pilot test
To examine survey acceptability, time to complete and response rates, surveys were mailed to a random sample of 100 eligible survivors selected from the Manitoba Cancer Registry. The completion rate was 54.2% with no follow-up. Feedback suggested that the survey length and content were acceptable. Minor changes to the invitation letter and to two items in the daily living domain and demographic questions were made before full psychometric testing was undertaken.
Survivor unmet needs survey
The draft Survivor Unmet Needs Survey (SUNS) included 152 items measuring unmet needs in six domains: information (15 items), job and financial needs (14 items); daily living needs (four items); medical care (55 items); relationship needs (26 items) and emotional and mental health (38 needs). An open-ended question allowed additional unmet needs. Questions about demographic and contextual factors and survey acceptability were asked.
Response options and scoring system
A five-point Likert-type scale ranging from zero (no unmet need) to four (very high unmet need) was adopted since consumer feedback indicated that this was easiest to understand. By including “no unmet need” as an anchor, the scale is able to distinguish between those items with which survivors did and did not require help and the level of help needed. Respondents were directed to consider their unmet needs within the last month in an effort to increase accuracy, reduce recall bias and measure current unmet needs [26, pp.37].
Demographic and contextual questions measured survivors’ sex, age, highest education, employment status, who they lived with, geographic location and distance from the cancer treatment centre. Cancer type, diagnosis date, recurrence, current status and treatment within the last month were also collected. Five questions assessed survey acceptability: easy to understand, difficulty answering, time to completion, distressing to answer and agreement to be contacted again.
Sampling frame
The sampling frame was the Manitoba Cancer Registry, operated by CancerCare Manitoba, which records all cases of cancer in that province. Vital status is checked against the provincial death register. Eligible persons were those over 19 years of age, alive, with a histologically confirmed cancer diagnosis in the preceding 12 to 60 months. In situ, neurological and non-melanoma skin cancers were excluded as well as survivors who had previously indicated they do not want to participate in research.
Sample
A cross-sectional stratified sample of 1,600 cancer survivors (n = 400 per stratum) was randomly selected from the Manitoba Cancer Registry. Stratification was based on time from diagnosis (12 to 24, 25 to 36, 37 to 48, and 49 to 60 months).
Ethical approval
The study received ethical clearance from the Universities of Waterloo and Manitoba with the restriction that only Cancer Registry staff could access personal identifiers.
Data collection
The Cancer Registry sent the initial SUNS with all surveys returned to the research team, identified only by study ID. Non-respondents received a reminder letter 4 weeks later and a second reminder with a replacement survey 2 weeks after that. Test–retest surveys were sent to respondents immediately upon return of the SUNS and those returned within 20 days were included in the analysis.
Item reduction
The 152 items were initially developed to ensure all potential unmet needs were covered but a shorter survey reduces completion burden for the survivor group and enhances usefulness. Thirty-nine items were eliminated if the time 1 to time 2 95% confidence interval of the intra-class correlation coefficient did not include 0.70. Five more items were eliminated because 85% or more of the respondents reported they had no unmet need, which suggested unacceptable face and content validity. Mean substitution of item scores was used for items which were missed by fewer than 10% of respondents. Based on these criteria, 108 items were retained for factor analysis.
Results
Response rates
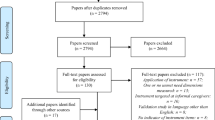
Of the 1,600 survivors who were mailed surveys, 29.5% (n = 472) were ineligible due to the wrong address, death and previous requests not to be contacted. Of the remaining 1,128 eligible survivors, the completion rate was 48.8% (n = 550). There were no statistically significant differences in response rates by strata (53.0% of those 12 to 24 months post diagnosis; 46.0% of those 25 to 36 months; 51.0% of those 37 to 48 months and 44.8% for those 49 to 60 months post-diagnosis \( \left( {\chi_{\left( {3{\rm{df}}} \right)}^2 = 4.7.0,\;p = 0.19} \right) \).
Respondent characteristics
There were no statistically significant differences between survivor respondents and the provincial population of survivors for sex, age or type of cancer with the exception of a lower proportion of respondents diagnosed at age 80 years and over \( \left( {\chi_{\left( {5{\rm{df}}} \right)}^2 = 35.2,\;p \leqslant 0.0001} \right) \) (Table 1). Slightly more than half (54.2%) had up to a high school education, 53.5% were retired and 31.9% were in paid employment. Current cancer status and treatment data were not available from the registry but self-report indicate the majority were either receiving follow-up care or had finished follow-up (Table 1). Less than 5% were dealing with a recurrence or in palliative care. Interestingly, nearly 10% wrote in that they “no longer had cancer”. Thirty-nine survivors (7.4%) said they were in active treatment, including long-term hormone and antibody therapies. A separate question found 42.5% of survivors had received treatment in the last month, with the majority being physician visits. Only 6% of all respondents received chemotherapy, radiation, surgery or bone marrow transplant but we do not know if this was for the initial tumour, recurrence or metastasis.
Psychometric properties of survey
Completion time and survey acceptability
The median, modal and mean time to complete the 152-item SUNS was just under 20 min and 26 min, respectively. Over 85% of survivors agreed or strongly agreed that the survey was clear, easy to understand, not distressing and 82.9% agreed to be contacted again, another indicator of survey acceptability.
Internal consistency
Cronbach’s alpha was 0.990 with the subscales ranging from 0.983 for Emotional Health subscale, 0.973 for Relationships, 0.967 for Access and Continuity of Care, 0.936 for Financial Concerns and 0.932 for the Information subscale. These results support strong internal consistency for both the overall scale and each subscale.
Face validity
Iterative consultation and input from survivors, health professionals and front line staff confirmed the SUNS domains and items represented issues and concerns with which cancer survivors would like help, providing evidence of good face validity.
Content validity
Content validity was also confirmed by the input from cancer survivors and the expert panel. Only 11 of the 152 items were missed by more than 10% of respondents, which provides further support for content validity. Missed items related to reproductive, sexual and spousal issues, child care, respite care, access to clinical trial information and the internet. Respondents used the full range of response options which supports our decision to use a five-point response scale.
Construct validity
Factor analysis was used and the number of factors to be retained was first determined by the eigenvalue greater than one rule. The analysis initially extracted 14 factors with eigenvalues greater than one. On the basis of the scree plot, a second principal components factor analysis using varimax rotation forcing five factors was conducted. Only those items with a factor loading of greater than 0.50 and no double loading were retained (Table 2). This resulted in a final version of the Survivor Unmet Needs Survey with 89 items across five subscales which accounted for an acceptable 64.4% of the total variance.
The first subscale Emotional Health, which measures survivors’ needs for help in dealing with their intrinsic feelings, consists of 33 items and accounted for 19.4% of the variance. For example, survivors want help “dealing with not feeling able to set future goals or make long term plans”, “coping with feeling like a different person”, “dealing with feelings of isolation”, “dealing with worry about the emotional well-being of my family”, “knowing how to relax” and “trying to stay positive”. Twenty-two items measured Access and Continuity of Care which accounted for 15.1% of the variance. Examples of unmet needs include “getting the health care team to attend promptly to my physical needs”, “getting test results quickly”, “understanding the information I was given”, “making sure my family doctor could get information from specialists” and “having access to cancer services close to my home”.
Fifteen items (12.1% of the variance) reflected Relationships which included “dealing with people who expect me to be back to normal”, “dealing with strains in my relationships”, finding someone to talk to who understands and has been through a similar experience”, “talking to my family and friends about how they were feeling” and “dealing with reduced support from others when treatment has ended”. The fourth subscale dealt with Financial Concerns (11 items, 10.3% of the variance) such as “worry about earning money”, “paying non-medical costs related to my cancer”, “finding what type of financial assistance is available and how to obtain it” as well as needing help “doing yard work” and “around the house”. The final Information subscale (eight items, 8.1% of the variance) included needs related to finding information, “knowing which sources of information to trust” and worrying about cancer recurrence and spread. The latter items loaded more highly in the Information domain than Emotional Health which supports the role information plays in helping survivors dealing with their disease. Separate items measuring feelings of worry and stress loaded highly in the Emotional Health domain.
We calculated Spearman correlation coefficients to examine relationships among the subscales (Table 3). We found correlations of 0.75 to 0.85 between Emotional Health, Relationships and Access and Continuity of Care and between the Relationships and Access subscales. Information was highly correlated with Access, Emotional Health and Relationships.
Highest unmet needs
Figure 1 shows respondents’ top ten unmet needs with the highest needs related to dealing with fears about the cancer spreading, not feeling sure the cancer had gone, fatigue, stress and having a bad memory or lack of focus. This corresponds with the literature which consistently identifies these as major problems experienced by survivors. The SUNS indicates a proportion of survivors are not getting the help they would like to deal with these problems.

Ten highest unmet needs identified by survivors. Single asterisk means “Finding what financial assistance is available and how to obtain it.” Double asterisks indicates that CAM means complementary and alternative medicine
Discussion
Understanding the impact of cancer beyond the first year is important as survival rates improve and follow-up moves from oncology clinics to community health services. Survivors face a number of physical, cognitive, functional and psychosocial problems, as well as work related and financial concerns [7], but most existing scales do not clearly identify those issues with which survivors want help [17]. An instrument that allows survivors to indicate which issues are not being resolved and the level of help required will aid health care planning and resource allocation.
Our results suggest much progress toward the development of a psychometrically robust instrument that will enable the accurate assessment of issues and problems with which all survivors want help. First, we selected a needs-based approach and an easy to understand response scale which identifies both the unmet needs and the magnitude of the unmet needs. Second, input from survivors, health professionals and researchers ensured survey acceptability, face and content validity. Third, we systematically applied strict pre-defined criteria in reducing the number of items. Our final instrument, with five subscales, accounted for 64.4% of the total variance. This compares favourably to the explained variance obtained by the other needs-based survivor instruments. The CaSUN (54% of total variance) [21] and SCNS Survivors Module (62.3% of total variance) [22] used factor loadings less than 0.50 for item retention (≥ 0.30 and ≥ 0.40, respectively). More critically, if the SUNS is used to examine individual unmet needs, there is the reassurance obtained by acceptable item test–retest reliability. Only surveys returned within 20 days were included in the test–retest analysis. The high Cronbach’s alpha coefficients for the SUNS overall and the subscales indicate strong internal consistency. Based on the extensive survivor input and feedback on the items and respondents’ use of the full response scale, the high coefficients are unlikely to be due to item redundancy or response bias.
The content of the items in the SUNS Emotional Health subscale and the Relationships subscale echo the importance of issues previously identified in the literature [8]. The first focused on intrinsic, emotional reactions to cancer, whereas the second domain captured feelings and behaviours for connecting with others. Economic and work-related issues are captured by the Financial Concerns subscale.
Examination of the item factor scores and subscale correlations suggests that interventions directed to specific domains of unmet needs will also help survivors deal with other areas of unmet needs. For example, helping survivors deal with the emotional impact of cancer may also help them address concerns about inter-personal relationships. Likewise attention to health care access and providing trustworthy information about disease progression and probabilities of recurrence could reduce survivors’ fears of recurrence. Cancer patients have a high need for information [20, 37] and our results suggest survivors are not getting adequate information about treatment success, cancer recurrence or spread.
External validity was strengthened by selecting a random sample of all survivors from a population-based Cancer Registry. Survivors were invited directly, reducing non-random error which can occur when health care professionals pre-screen potential participants for eligibility.
Limitations
Development of a new instrument is a long and complicated process, and there are some limitations in this research. One relates to the response rate of 48.8% which, although lower than desired, was similar to other studies recruiting from cancer registries which have achieved only slightly more than 50% response rate [32, 33]. Comparison of demographic characteristics and cancer type indicated our sample is representative of the population of survivors with the exception of the very elderly. We do not know if stage, disease or treatment status is similar since those data were not available from the cancer registry. These may affect unmet needs and further research is encouraged.
Several factors potentially contributed to the low response. Qualitative feedback from staff suggest that some non-respondents felt the survey did not apply to them because they believed they no longer had cancer; they were not undergoing treatment or they had no needs in the last month. The latter was supported by written comments such as “[I] do not have needs now” or “had no unmet needs in the last month”. Seasonal effects may have contributed as well since recruitment extended into the summer. Sutherland et al. who recruited patients with familial breast cancer reported similar seasonal effects on response rates [34].
Postal return between time 1 and time 2 was slow and consequently we extended the retest time frame to 20 days from the recommended 2- to 14-day period [24]. While the shorter time frame is preferred from a psychometric perspective, it is difficult to achieve when there is a reliance on postal services, particularly in rural areas. However, as noted above, the high Chronbach’s alpha coefficients suggest this time frame did not negatively affect reliability. Among existing survivor quality of life and needs assessment instruments, only the QOL-CS [35] and the CaSUN [21] examined item test–retest reliability based on “approximately two week period” and “twenty-one day timeframe”, respectively. The SCNS-Survivors Module [22] and the USCA-PCI [36], which examined domain test–retest reliability, used 14- and 28-day retest timeframes, respectively. The value of domain-based reliability could be questioned given the probability of within-item variance while still allowing time 1 to time 2 similarity in overall domain or subscale scores.
When planning the study, consideration was given to examining unmet needs scores against other measures such as depression or anxiety. From a theoretical prospective, a weak relationship may exist between unmet needs and depression and anxiety. However, the addition of extra questionnaires was felt to impose an unreasonable burden on survivors given the length of the initial survey. The research team is considering examining the predictive validity of the instrument against future events such as hospital visits and healthcare provider contact.
Conclusion
This study is an important step toward evidence-based planning and management of problems which the growing survivor population require assistance. SUNS captures five dimensions of the survivorship experience of which two (Access and Continuity of Care and Financial Concerns) are unique to survivorship. Additional validation studies with other survivor populations are encouraged to confirm the items and domains and increase the probability that the SUNS will provide accurate information about cancer survivors’ unmet needs.
References
Canadian Strategy for Cancer Control Governing Council (2006) Canadian Cancer Strategy Discussion Paper. Available via http://www.partnershipagainstcancer.ca/sites/default/files/documents/reports/CSCC_CancerPlan_2006.pdf Accessed December 5 2008
Stein K, Smith T, Kim Y, Mehta CC, Stafford J, Spillers RL, Baker F (2006) The American Cancer Society’s Studies of cancer survivors: the largest, most diverse investigation of long term cancer survivors so far. Cancer Nurs 29(2 Suppl):3–85
Welch HG, Schwartz LM, Woloshin S (2000) Are increasing 5-year survival rates evidence of success against cancer? JAMA 283:2975–2978
International Agency for Research on Cancer. World Cancer Day 2008. Press Release 182. Available via http://www.iarc.fr/ENG/Press_Releases/pr182a.html. Accessed January 14, 2009
Canadian Cancer Society/National Cancer Institute of Canada (2009) Canadian Cancer Statistics 2009. Canada, Toronto
Ries LAG, Melbert D, Krapcho M, Mariotto A, Miller BA, Feuer EJ, Clegg L, Horner MJ, Howlader N, Eisner MP, Reichman M, Edwards BK (eds). SEER Cancer Statistics Review, 1975-2004, National Cancer Institute. Bethesda, MD Available via http://seer.cancer.gov/csr/1975_2004/. Accessed June 12, 2009
Institute of Medicine (2006) The medical and psychological concerns of cancer survivors after treatment. In: Hewitt M, Ganz P (eds) From cancer patient to cancer survivor: Lost in transition. The National Academies Press, Washington, DC, pp 66–186
Stein KD, Syrjala KL, Andrykowski MA (2008) Physical and psychological long-term and late effects of cancer. Cancer 112(suppl):2577–2592
Burkett S, Cleeland CS (2007) Symptom burden in cancer survivorship. J Cancer Survivorship 1:167–175
Travis LB (2006) The epidemiology of second primary cancers. Cancer Epidemiol Biomarkers Prev 15:2020–2026
Yabroff KR, Lawrence WF, Clauser S, Davis WW, Brown ML (2004) Burden of illness in cancer survivors: Findings from a population-based national sample. JNCI 96:1322–1330
Steiner JF, Cavender TA, Main DS, Bradely CJ (2004) Assessing the impact of cancer on work outcomes. Cancer 101:1703–1711
Short PF, Vasey JJ, Markowski M, Zabora JR, Harper Gr, Rybka WB (2005) Risks to quality of life in a large cohort of adult cancer survivors. Penn State Population Research Institute Working Paper 2005-01. Available via www.pop.psu.edu/general/pubs/working_papers/psu-pri/wp0501.pdf Accessed January 14, 2009
Hewitt M, Ganz P (eds) (2006) From cancer patient to cancer survivor—lost in transition: an American Society of Clinical Oncology and Institute of Medicine Symposium. National Academies Press, Washington, DC
Yancik R (1997) Cancer burden in the aged: an epidemiologic and demographic overview. Cancer 80:1273–1283
Rowland JH, Yancik R (2006) Cancer survivorship: the interface of aging, comorbidity and quality care. JNCI 98:504–505
Pearce NJM, Sanson-Fisher R, Campbell HS (2008) Measuring quality of life in cancer survivors: a methodological review of existing scales. Psych-Oncol 17:629–640
Osse BH, Vernooij-Dassen MJFJ, de Vree BPE, Schadé E, Grol RPTM (2000) Assessment of the need for palliative care as perceived by individual cancer patients and their families: a review of instruments for improving patient participation in palliative care. Cancer 88:900–911
Pollock K, Wilson E, Porock D, Cox K (2007) Evaluating the impact of a cancer supportive care project in the community: patient and professional configurations of need. Health & Social Care in the Community 15:520–529. doi:10.1111/j.1365-2524.2007.00711.x
Sanson-Fisher R, Girgis A, Boyes A, Bonevski B, Burton L, Cook P, the Supportive Care Review Group (2000) The unmet supportive care needs of patients with cancer. Cancer 88:226–237
Hodgkinson K, Butow P, Hunt GE, Hunt S, Pendlebury S, Hobbs KM, Los SK, Wain G (2007) The development and evaluation of a measure to assess cancer survivors’ unmet supportive care needs: the CaSUN (Caner Survivors’ Unmet Needs measure). Psycho-Oncol 16:796–804
Thewes B, Butow P, Girgis A, Pendlebury S (2004) Assessment of unmet needs among survivors of breast cancer. J Psychosocial Oncology 22:51–73
National Cancer Institute. Estimated Number of Persons Alive in the U.S. Diagnosed with Cancer on January 1, 2006 by Site (N = 11.4 M). Available via http://cancercontrol.cancer.gov/ocs/prevalence/prevalence.html#allsites Accessed November 12, 2009.
DeVellis RF (2003) Scale development: theory and applications. Sage Publications, Thousand Oaks
Streiner DL, Norman GR (2003) Health measurement scales: a practical guide to their development and use. Oxford University Press, Oxford
McDowell I (2006) Measuring health: a guide to rating scales and questionnaires. Oxford University Press, Oxford
Richardson A, Medina J, Brown V, Sitzia J (2007) Patients’ needs assessment in cancer care: a review of assessment tools. Support Care Cancer 15:1125–1144
Foot G (1996) Needs assessment in tertiary and secondary oncology practice: a conceptual and methodological exposition. University of Newcastle, Dissertation
Rainbird KJ, Perkins JJ, Sanson-Fisher RW (2005) The Needs Assessment for Advanced Cancer Patients (NA-ACP): a measure of the perceived needs of patients with advanced, incurable cancer—a study of validity, reliability and acceptability. Psycho-Oncol 14:297–306
Davidson P, Cockburn J, Daly J, Sanson-Fisher R (2004) Patient-centered needs assessment: rationale for a psychometric measure for assessing needs in heart failure. J Cardiovasc Nurs 19:164–171
Canadian Public Health Association. Plain Language Assessment Service. Available via http://www.cpha.ca/en/pls.aspx Accessed February 2007
Sisler JJ, Brown JB, Stewart M (2004) Family physicians’ roles in cancer care. Can Fam Physician 50:889–896
Zebrack BJ, Ganz PA, Bernaards CA, Petersen L, Abraham L (2006) Assessing the impact of cancer: development of a new instrument for long-term survivors. Psycho-Oncol 15:407–421
Sutherland HJ, Lacroix J, Knight J, Andrulis IL, Boyd NF, the Ontario Cancer Genetics Network (2001) The Cooperative Familial Registry for Breast Cancer Studies: design and first year recruitment rates in Ontario. J Clin Epidemiol 54:93–98
Ferrell BR, Hassey Dow K, Grant M (1995) Measurement of the quality of life in cancer survivors. Qual Life Res 4:523–531
Litwin MS, Hays RD, Ganz FA, PA LB, Brook RH (1998) The USCA Prostate Cancer Index: development, reliability and validity of a health-related quality of life measure. Med Care 36:1002–1012
Li J, Girgis A (2006) Supportive care needs: are patients with lung cancer a neglected population? Psycho-Oncol 15:509–516
Acknowledgements
The authors acknowledge Cheryl Clague, CHIM, Project Manager and Humaira Khair, MSc., Programmer Analyst, from the Department of Epidemiology and Cancer Registry, CancerCare Manitoba for their management of the sample selection, survey distribution and comparative analysis. We thank Sandra Corbin MSc, Research Coordinator for her role in coordinating the study and Nancy Pearce, PhD, University of Waterloo for assistance in developing the survey items. The Canadian Cancer Society assisted in recruiting cancer survivors for the qualitative survey of unmet needs.
Conflict of interest
No conflict of interest or financial disclosures are reported by the authors.
Sources of support
This study was funded by the Canadian Cancer Society through a grant to the Centre for Behavioural Research and Program Evaluation at the University of Waterloo.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Campbell, H.S., Sanson-Fisher, R., Turner, D. et al. Psychometric properties of cancer survivors’ unmet needs survey. Support Care Cancer 19, 221–230 (2011). https://doi.org/10.1007/s00520-009-0806-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-009-0806-0