
Abstract
A substantial number of epidemiological studies have demonstrated an association between atmospheric conditions and human all-cause as well as cause-specific mortality. However, most research has been performed in industrialised countries, whereas little is known about the atmosphere–mortality relationship in developing countries. Especially with regard to modifications from non-atmospheric conditions and intra-population differences, there is a substantial research deficit. Within the scope of this study, we aimed to investigate the effects of heat in a multi-stratified manner, distinguishing by the cause of death, age, gender, location and socio-economic status. We examined 22,840 death counts using semi-parametric Poisson regression models, adjusting for a multitude of potential confounders. Although Bangladesh is dominated by an increase of mortality with decreasing (equivalent) temperatures over a wide range of values, the findings demonstrated the existence of partly strong heat effects at the upper end of the temperature distribution. Moreover, the study demonstrated that the strength of these heat effects varied considerably over the investigated subgroups. The adverse effects of heat were particularly pronounced for males and the elderly above 65 years. Moreover, we found increased adverse effects of heat for urban areas and for areas with a high socio-economic status. The increase in, and acceleration of, urbanisation in Bangladesh, as well as the rapid aging of the population and the increase in non-communicable diseases, suggest that the relevance of heat-related mortality might increase further. Considering rising global temperatures, the adverse effects of heat might be further aggravated.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
To date, a multitude of studies has assessed the influence of seasonal and meteorological conditions on human mortality. In general, results show a peak in mortality rates during the cold season and an increase with decreasing temperatures over a wide range of values (Basu and Samet 2002; Curriero et al. 2002; Rau 2006; Baccini et al. 2008; Basu 2009; Bhaskaran et al. 2009; Nastos and Matzarakis 2012). Although the lowest levels of mortality are usually observed during summer, extreme events (i.e. heat waves) can lead to serious increases in mortality rates, as observed during the European summer heat waves of 2003 or the Chicago heat wave of 1995 (Schär and Jendritzky 2004; Kaiser et al. 2007; Robine et al. 2007). Moreover, analyses of the association between temperature and mortality have revealed U-, V-, or J-shaped patterns, with an increase in mortality below and above a certain threshold (Basu and Samet 2002; Curriero et al. 2002; Baccini et al. 2008; Basu 2009). Typically, tropical countries with commonly low socioeconomic status have been associated with increased mortality during the hot and humid season (McGregor et al. 1961; Jaffar et al. 1997; Rau 2006). However, more recent studies in low-latitude regions have demonstrated high rates of mortality during the cold season and shown a temperature–mortality relationship with marked cold and heat effects, similar to patterns observed in industrialised countries (Becker and Weng 1998; McMichael et al. 2008; Hashizume et al. 2009; Burkart et al. 2011a, 2011b).
The magnitude and direction of meteorological effects have been shown to depend on existing non-atmospheric circumstances (O’Neill et al. 2005; Hashizume et al. 2007; Medina-Ramón and Schwartz 2007). Population density, age structure, degree of urbanisation, and costs of living have been identified as determinants (Smoyer et al. 2000; Basu and Samet 2002; Rau 2006). Moreover, differences in temperature–mortality regimes have been recognised between different population groups (e.g. ethnic groups) or groups with different social or socio-economic backgrounds (Klinenberg 2002; Rau 2006; Kaiser et al. 2007). The vulnerability and resilience of individuals as well as populations seems to be determined by social and socio-economic conditions and, similarly, heat seems to have social impacts (McGregor et al. 2007). Hence, the effect of atmospheric parameters is likely to change with changes in social and population structures.
To date, research evidence on the atmospheric environment–mortality relationship in developing countries is incomplete. Two recent studies investigated the seasonal and thermal effects on mortality in Bangladesh (Burkart et al. 2011a, 2011b). Although the relevance of cold effects was demonstrated, heat-related mortality became apparent in terms of a secondary summer mortality maximum and an increase in mortality above a specific threshold temperature. This threshold temperature amounted to approximately 29 °C for ambient temperature and ranged between 31 °C and 34 °C for the universal thermal climate index (UTCI), a thermo-physiological index reflecting some sort of apparent temperature.
The projected consequences of climate change have promoted research on the nature of meteorological and particularly thermal effects (Basu and Samet 2002; Basu 2009; Gosling et al. 2011, 2012). Considering the high prevailing temperatures and the generally low socio-economic status in tropical developing countries, we suggest that these regions might be most vulnerable to a rise in temperature, promoted by global warming. Furthermore, many developing countries have underlying strong social and population dynamics, such as the rapid aging of the population, an increase in urbanisation, or a change in disease and mortality patterns (i.e. an increase in non-communicable diseases) (Murray and Lopez 1997; Reddy and Yusuf 1998; United Nations 2004, 2008). These dynamics might be most relevant in shaping future meteorological effect on human health. This study aims to continue our preceding research and seeks to investigate sub-population differences in heat-related mortality. A special focus was given to modifications arising from age, gender, location, and socioeconomic status (SES).
Data and methods
Meteorological data
Meteorological data from 26 stations distributed throughout Bangladesh were provided by the Bangladesh Meteorological Department. The data were composed of 3-hourly values of temperature, humidity, wind speed, and cloud coverage. In order to assess the multitude of meteorological parameters affecting the human heat balance, we calculated the universal thermal climate index (UTCI), using BioKlima Software (Version 2.6) (Jendritzky et al. 2007). The UTCI represents an equivalent temperature that equals the ambient air temperature that results in the same energy gain or loss an average human would experience in a reference environment (with 50 % relative humidity, still air, and a radiant temperature equalling air temperature) (Jendritzky et al. 2007). The input variables are temperature, humidity, wind speed, and mean radiant temperature. The input variable mean radiant temperature (the uniform temperature of a surrounding surface that results in the same radiation energy gain on a human body as the prevailing radiation fluxes) is modelled as a function of temperature and cloud coverage using RayMan (Version 1.2) (Matzarakis et al. 2007). Daily mean values of the UTCI were calculated from 3-hourly values for each station, when the measurements were complete for a given day. Approximately 17 % of the calculated daily data were missing. The missing daily values of temperature or the UTCI were replaced by linear interpolation. In a previous study (Burkart et al. 2011a) we compared the predictive power of different equivalent temperatures, namely Heat Index, Physiological Equivalent Temperatures, and UTCI. All three parameters were highly correlated and based on the Unbiased Risk Estimation Criterion (UBRE); no index showed a predictive advantage. Hence, for this study, we limited ourselves to only one thermo-physiological indicator, and chose the UTCI index as it is well documented and the software is easy to handle. The monthly seasonal distributions of the mean temperature and the UTCI, as well as of the precipitation in Dhaka, are displayed in Fig. 1. Temperatures are particularly high during months with high precipitation, with equivalent temperature surpassing ambient temperature. During the dry season, equivalent temperature approximates ambient temperature.

Monthly average mean values of temperature, universal thermal climate index (UTCI), and monthly precipitation in Dhaka. Inset Annual average temperature and the UTCI as well as the annual amount of precipitation
Given the sample nature of the mortality data, we needed to aggregate over space. To delimit thermal regimes, we conducted a factor analysis using the Kaiser criterion as a cut-off criterion for the number of factors necessary. In the case of the 26 (equivalent) temperature time-series, the Kaiser criterion indicated that one factor represents more than 99 % of the variability. In a second step, we conducted a cluster analysis to investigate whether different large-scale regional climate units can be observed (e.g. North–south differences with higher temperatures in one region and lower in the other region). The cluster analysis did not reveal any macro-scale pattern. Therefore, any existing regional meteorological variations were not considered, and a spatial average daily mean value for the whole country was calculated. Spatial UTCI maps were generated for each day using inverse distance interpolation (R, Version 2.11.0, package ‘gstat’). Subsequently, a mean value was calculated from the map grid values.
Mortality data
The mortality data analysed within this study were collected within the Sample Vital Registration System (SVRS)—a core activity of the Bangladesh Bureau of Statistics (BBS). The SVRS comprises and surveys approximately 200,000 households, with an average size of 4.7 members, throughout Bangladesh. Of the total number of households, 132,646 are located in rural areas, whereas 57,852 households are located in urban areas and 16,024 households are placed in the statistical metropolitan area. The SVRS collects data under a dual recording system. Events are recorded by a local registrar when they occur, and they are also registered retrospectively by officials from the Upazila division of the BBS on a quarterly basis. Subsequently, the data are matched by quality control personnel of the BBS. Partially matched and non-matched events are subject to further verification through field visits. The following information is recorded: name, date of birth, date of death, and gender of the deceased. In addition, a cause of death is attributed; however, the cause is not medically certified (Bangladesh Bureau of Statistics 2008). For the purpose of this study, all accidental and maternity-related deaths were excluded. The sample was stratified into three age groups: children and youths (1–14 years), adults (15–64 years), and elderly persons (65+ years). Deaths of infants younger than 1 year of age were not included as births exhibit seasonal variations that could confound the analysis. In total, 22,840 deaths were analysed. Tables with the number of death counts and the crude death rates per strata are provided in the supplementary material (Supplementary Material S1, Table S1.1 and Table S1.2).
Statistical analysis
Analysis of time structure and temporal effect displacement
In order to describe the time structure of thermal effects, we employed a recently developed distributed lag non-linear model (DLNM). This methodology is based on the definition of a ‘cross-basis’—a bi-dimensional space of functions that describes simultaneously the shape of the relationship along both the space of equivalent temperature and the lag dimension of its occurrence (Gasparrini et al. 2010). The effects are estimated using smooth non-linear functions for both dimensions, the equivalent temperature and the lag effect (Gasparrini et al. 2010). Such an approach provides an insight into the temporal displacement of effects as well as harvesting effects. The crossbasis function was included into a generalised additive model (GAM); the specifics of the GAM and the confounder variables included will be discussed in the following section. The basis for temperature was centred at the median equivalent temperature (26.9 °C UTCI), which represents the reference point for the predicted effects. The DLNM requires setting degrees of freedom for the temperature and lag relationships. As a sensitivity analysis we tested several degrees of freedom but found that the general conclusions about the temporal occurrence of heat effect was unaffected by this.
Regression analysis
The association between atmospheric parameters and mortality was modelled using Poisson GAMs. Penalised regression splines were used to allow for nonlinear confounding effects. Smoothing parameters were chosen to minimise the UBRE score for the models, and estimation of the degrees of freedom is part of the model fitting. A Bayesian approach to variance estimation was employed to estimate the confidence intervals (Wood 2006). The R (Version 2.11.0) package ‘mgcv’ was used for model fitting. In order to remove long-term fluctuations in mortality, the models were adjusted for trend by including a counter variable for each day of the time series and fitting a penalised spline. Additionally, a categorical dummy variable for seasonal adjustment was incorporated to remove the mid- to long-term seasonal cycles in the series, as we aimed to investigate short-term influences. Moreover, this dummy variable allowed for reflection of seasonal differences in air pollution levels with high levels during winter (stable atmospheric conditions), and decreasing levels in the pre-monsoon and monsoon seasons (unstable atmospheric conditions) as long-term air pollution measurements are not available for Bangladesh. In Bangladesh, the year can be divided into three main seasons: winter season (October–February), summer/pre-monsoon season (March–May), and monsoon/rainy season (June–September). In addition, the models were adjusted for day of the week.
Finally, the models were fitted, incorporating UTCI. As described by the distributed lag non-linear models, heat effects generally occur on the 1st and 2nd day. Therefore, averages of same-day UTCI and the UTCI of the previous day (lag 0–1) were incorporated in all models that did not specifically analyse children and youths. As heat effects seemed to be more delayed for children and youths, we integrated the averages of same-day UTCI and the UTCI of the previous 4 days (lag 0–4) into models assessing heat effects in this age group.
As a major research objective of this study was to investigate thermal effects and heat effects in different subpopulations, we stratified the data by cause of death, age, gender, location, and SES. Subsequently, we fitted models including the different subcategories and integrated an interaction term between equivalent temperature and the categories. To group the data by SES, we referred to the socioeconomic data of the administrative departments of the zilas (the 64 districts of Bangladesh). The variables considered were the child mortality rate, the child/woman ratio, the literacy rate, the fertility rate, the sources of drinking and non-drinking water, infant mortality, the insolvency rate and use of solid fuels. A factor analysis using Varimax rotation and Bartlett scores (R, Version 2.11.1) rendered four factors that broadly reflect, “solvency”, ”education”, ”mortality” and “source of water” (the number of factors was based on the Kaiser criterion). For categorising a zila as having a high or low SES, three of the four factors had to either exceed or fall below the 50th percentile. Of the 64 zilas, 23 were categorised as having a low SES, and 25 were categorised as having a high SES. The remaining 16 zilas were used as reference.
In addition to the non-parametric regression analysis representing the UTCI–mortality relationship as a spline, we also fitted GAM models with segmented relationships in order to quantify the observed heat effects. For this, we assumed a piecewise linear relationship between mortality and equivalent temperature. The initial values for the breakpoints were specified over a range of possible integer values, as indicated by the equivalent temperature–mortality plots; subsequently, breakpoints were determined by minimising the UBRE score. For all models, threshold equivalent temperatures lying between 34 °C and 35 °C UTCI were found.
Results
Time structure of thermal effects
Figure 2 shows the three-dimensional plots of the risk of all-cause mortality along equivalent temperature, and the lags for all age groups as well as for children and youths (1–14 years). For all ages, the plot demonstrates a strong effect of high equivalent temperatures occurring immediately on the 1st day. For children and youths these effects of higher equivalent temperatures seemed to be more delayed. Figure 2 also includes lag-specific effects at an equivalent temperature of 35.5 °C UTCI (99th percentile of UTCI), which well exemplify the temporal displacement of effects at higher temperatures. For all-cause mortality including all age groups, maximum risk was observed on the 1st day and then quickly decreased. For children, an increase in mortality was observed between the 2nd and 5th day. However, after the 5th day, the relative risk of mortality notably decreased, which suggests a harvesting effect (deaths of frail individuals are brought forward by a short period of time) rather than excess mortality. DLNM outputs for cause-specific and age-specific mortality are included in a supplementary file (Supplementary Material S2). Generally, they confirm the short-term character of heat effects occurring mostly on the 1st day. Based on these observations, we used a lag period of 2 days for all further analysis, except for children, for whom we used a lag period of 5 days (Fig. 2).

Three-dimensional plots of the relative risk of mortality along equivalent temperature and lags, with reference at the median equivalent temperature (26.6 °C UTCI) for all-cause mortality in all ages (top left) and for children and youths (top right); and plots of relative risk of mortality at the 99th percentiles of equivalent temperature distribution (35.5 °C UTCI), with reference at the median equivalent temperature (26.6 °C UTCI) for all ages (bottom left) and children and youths (bottom right). Outputs are adjusted for trend, season, and day of the week. Grey areas Upper and lower 95 % confidence intervals

Association between the daily number of deaths and the average equivalent temperature (UTCI) over a lag period of 2 days (lag 0–1) stratified by cause of death for all-cause mortality (ALL), cardiovascular mortality (CVD), and infectious disease mortality (INF). Curves are adjusted for trend, season, and day of the week. Grey areas Upper and lower 95 % confidence intervals
Thermal effects
All-cause and cause specific thermal effects
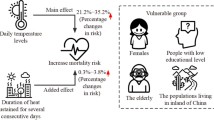
In general, the analysis demonstrated the existence of diverse thermal effects on mortality, which varied with the investigated sub-groups. We observed linear associations between equivalent temperature and mortality, as well as J-, U-, or V-shaped relationships. All-cause mortality decreased with increasing equivalent temperature over a wide range of values (i.e. a cold effect). At the upper end of the equivalent temperature distribution the temperature–mortality relationship changed and mortality started to increase with increasing temperature (i.e. a heat effect). In general, this pattern was observed for all-cause mortality as well as cardiovascular and infectious disease mortality but the effects were most visible for all-cause mortality (Fig. 3). The segmented analysis revealed an increase in all-cause mortality above a threshold of 31.3 % (95%CI: 24.5–44.3) per 1 °C increase in UTCI. For cardiovascular mortality this increase amounted to 20.0 % (95%CI: 10.6–34.7 %) and for infectious mortality to 10.4 % (95%CI: 0.7–25.2 %) (Table 1).
Age-specific thermal effects
Generally, thermal effects were observed in all investigated age groups. Figure 4 shows the UTCI–mortality relationship for children and youths (1–14 years), adults (15–64 years) and the elderly (above 65 years). For children and youths as well as for adults, effects are rather less pronounced and confidence intervals are wide, whilst for the elderly marked cold and heat effects were visible in the equivalent temperature–mortality plots. Similarly, findings from the segmented analysis demonstrate heat effects for all age groups with the highest magnitude observed for the elderly (32.0 %; 95%CI: 29.1–40.7 %). Nevertheless significant heat effects were also found for children (19.4 %; 95%CI: 14.3–30.2 %) and adults (23.1 %; 95%CI: 12.7–40.2 %). However, differences between the age groups were not significant (Table 1).

Association between the daily number of deaths and the average equivalent temperature (UTCI) over a lag period of 5 days (lag 0–5) for children and youths (1–14 yrs.), and a lag period of 2 days (lag 0–1) for adults (15–64 years) and the elderly (65+ years). Curves are adjusted for trend, season, and day of the month. Grey areas Upper and lower 95 % confidence intervals
Thermal effects in different subpopulations
When examining the UTCI–mortality relationship by gender for the elderly above 65 years, it became apparent that men face an increased risk of heat-related mortality compared to women (Fig. 5). A sharp increase in all-cause mortality was observed for men, which was estimated as 45.9 % (95%CI: 39.7–59.0) in the segmented analysis. Contrary to that, heat effects for woman were significantly smaller, with an increase of 24.3 % (95%CI: 16.9–38.8 %) above the threshold temperature. A significant increase of 26.0 % (95%CI: 10.3–44.1 %) in cardiovascular mortality was also observed for males, whereas no effect was observed for females. No significant effects were found for infectious disease mortality for either males or females (Table 2).

Association between the daily number of deaths and the average equivalent temperature (UTCI) over a lag period of 2 days (lag 0–1) for males vs females above the age of 65 years. Curves are adjusted for trend, season, and day of the month. Grey areas Upper and lower 95 % confidence intervals
With regard to all-cause mortality and cardiovascular mortality in the elderly, urban areas showed more pronounced and more severe heat effects as compared to rural areas (Fig. 6). UTCI–mortality plots indicated a steep increase in all-cause mortality in urban areas. The segmented analysis depicted this increase with 46.3 % (95 % CI: 39.2–61.1 %) per 1 °C increase in UTCI, whilst in rural areas the heat effects is significantly smaller and was estimated with 25.5 % (95%CI: 21.7–35.5 %). Regarding cardiovascular mortality, the GAM plots do not indicate any kind of heat-related mortality in rural areas, whilst in urban areas mortality increased above a threshold UTCI. The segmented analysis showed a significant increase in cardiovascular mortality of 22.6 % (95%CI: 8.7–41.7 %) in urban areas and a negative slope for rural areas. Contrary to the increased risk of heat related all-cause and cardiovascular mortality in urban areas, a significant increase in infectious disease mortality was observed for rural areas, whilst no effect was found for urban areas (Table 2).

Association between the daily number of deaths and the average equivalent temperature (UTCI) over a lag period of 2 days (lag 0–1) for the elderly above the age of 65 years in rural vs urban areas. Curves are adjusted for trend, season, and day of the month. Grey areas represent the upper and lower 95 % confidence intervals
When contrasting zilas with low and high SES, increased heat effects in the elderly above 65 years were evident for high SES areas regarding all-cause mortality and cardiovascular mortality (Fig. 7). The increase in all-cause mortality was estimated with 41.6 % (96%CI: 34.4–55.0 %) in the segmented analysis for areas with high SES. In contrast, areas with low SES showed a heat-related increase of 24.1 % (95% CI: 16.4–37.6 %). While areas with low SES exhibited no heat effect for cardiovascular mortality, areas with high SES areas showed a significant increase in cardiovascular mortality of 44.9 % (95%CI: 1.4–37.0 %). No effects of heat on infectious disease were found, for either areas with low or high SES (Table 2).

Association between the daily number of deaths and the average equivalent temperature (UTCI) over a lag period of 2 days (lag 0–1) in areas with low vs high SES. Curves are adjusted for trend, season, and day of the month. Grey areas Upper and lower 95 % confidence intervals
Discussion
This study emphasizes the relevance of thermal effects on human all-cause and cause-specific mortality. We found a strongly pronounced relationship between equivalent temperature and mortality. Moreover, the findings of this work clearly demonstrate that atmospheric effects vary with the cause of death, as well as with intra-population differences.
In general, mortality showed a J-shaped UTCI-mortality curve, with increasing mortality below and above a threshold, ranging between 34 and 35 °C UTCI. Generally, this pattern was mostly visible for all-cause, but cardiovascular and infectious disease mortality also showed cold and heat effects. Considerable differences regarding the magnitude of these effects were found for different subgroups, and heat effects showed especially pronounced intra-population modifications. Generally, heat effects were strongly pronounced for the elderly, for males, and for those living in urban and high SES areas.
Age proved to be a determining factor in shaping meteorological effects. Generally the strongest association between equivalent temperature and mortality was found for the elderly above the age of 65 years; however, adults and children also showed an increase in mortality with decreasing as well as increasing equivalent temperatures. As shown by the DLNMs, heat effects seemed to be more delayed for children and youths, occurring after several days. Several other studies have investigated thermal effects in children with inconsistent findings. Gouveia et al. (2003) found marked heat effects in children and youths under the age of 15 years in São Paulo, Brazil, whereas Bell et al. (2008) found no heat effect for children under the age of 16 years in São Paulo and Mexico City using a case-crossover design. Likewise, no heat effects were found by O’Neill et al. (2005) in children under the age of 15 in Mexico City and no heat effects could be observed in a rural area of Matlab in Bangladesh (Hashizume et al. 2009). Detecting heat effects in children is rather difficult as usually the number of cases is limited for these age groups. The restriction of heat effects to a relatively short range of temperature values further complicates the analysis. Moreover, heat effects in younger individuals seem to have a different time structure than observed for other ages, which suggests a different cause-and-effect relationship. Further stratification by cause of death would be desirable at this point to better understand how thermal conditions affect the physical health of children, but the limited number of death counts does not allow doing so. Another important point regarding heat effects in children is “harvesting”. Outputs of the DLNM indicate a forward shift in the occurrence of deaths of children and youths rather than an excess in mortality.
For adults between 15 and 64 years of age, a relatively weak relationship between equivalent temperature was displayed by the GAM plots. Nevertheless, the segmented analysis revealed significant heat effects that correspond approximately with the effects observed for children. Heat effects for adults were also found in São Paulo (Brazil) and Mexico City (Mexico) but the observed effects were generally weaker than found for this study (Gouveia et al. 2003; O’Neill et al. 2005; Bell et al. 2008). GAM plots as well as the segmented analysis depict a growing relevance of heat effect for the elderly. The observed heat effects of a 32.0 % (95%CI: 29.1–40.7) mortality increase per 1 °C increase in equivalent temperature exceeded the effects reported in studies conducted in São Paulo and Mexico City (Gouveia et al. 2003; Bell et al. 2008). Nevertheless, Hashizume et al. (2009) found an increase in mortality of 108 % (95%CI: 32.3–227.1 %) per 1 °C temperature increase for the elderly in Matlab, a rural area of Bangladesh. The findings of our study underline the high heat-related vulnerability of the elderly living in Bangladesh.
The stratified analysis further revealed that males faced a higher risk of heat-related all-cause and cardiovascular mortality than females. This finding was particularly true for elderly males. Few studies to date have investigated gender differences in the temperature–mortality relationship in developing countries. To our knowledge, only one study, conducted by Bell et al. (2008), has assessed heat effects by gender (in São Paulo, Santiago de Chile and Mexico City). However, that study found no significant differences. In studies conducted in industrialised countries, there were either no differences by gender (O’Neill et al. 2003; Stafoggia et al. 2008), or a greater risk was observed for females (Fouillet et al. 2006; Ishigami et al. 2008). The high risk of heat-related mortality in males in Bangladesh might be due to increased exposure to heat. In general, men are more involved in outside activities and are often occupied in heavy labor, whereas woman are traditionally oriented to the home and engaged in housework. In addition, cardiovascular and other non-communicable diseases are more prevalent causes of death in males (see Supplementary Material S1, Table S1.2), causing them to be more susceptible to adverse heat effects.
As demonstrated in a previous study, all-cause and cardiovascular mortality in urban areas is subject to noticeable heat effects (Burkart et al. 2011a), as confirmed in this study. However, this study also demonstrated a heat-related increase in infectious disease mortality in rural areas whereas no such association could be observed for urban areas or any other strata. In addition, this study assessed the differences between areas with a low and high SES and found that heat effects were considerably stronger in high SES areas, especially for the elderly. The strong relationship between heat and mortality in urban as well as high SES areas indicates the relevance of socio-economic and socio-cultural conditions. An urban lifestyle, usually associated with a lack of physical activity, sedentary behaviour and an unhealthy diet are believed to contribute to a higher prevalence of non-communicable diseases in urban populations (Proctor et al. 1996; Shetty 2002; Kelishadi et al. 2008; Khan et al. 2009). Of equal importance is the finding that an improvement in SES is likely to be accompanied by socio-cultural changes and changes in disease patterns (a decrease of communicable diseases and an increase in non-communicable diseases) (Murray and Lopez 1997; World Health Organisation 2010). Although it is unclear for urban areas whether heat effects originate from higher temperatures (due to urban heat islands) or from a higher susceptibility to heat as a consequence of a modified health or age pattern, our analysis by SES demonstrates the relevance of socio-economic and socio-cultural factors for heat-related excess mortality.
Strengths and limitations
The obvious strength of this study is based in the multi-stratified analysis of meteorological effects. We showed that different strata feature different characteristics that are crucial for thermal effects. To date, few studies have assessed meteorological effects in tropical developing countries, and even fewer studies have conducted analyses in different strata. However, understanding these non-atmospheric effect modifications is crucial for targeting intervention measures properly and efficiently. The use of DLNMs helped to better understand the time structure of thermal effects in Bangladesh. They confirmed a lag period of 2 days for most investigated categories, which is commonly used in heat effect assessment. However, they also revealed that heat effects in children and youths are more delayed and equally as important indicated the relevance of harvesting effects for this age group. Nonetheless, confidence intervals for the DLNM outputs are relatively wide, which needs to be attributed partly to the complexity of the DLNM requiring an extensive data basis. Additionally, the wide confidence intervals reflect uncertainties in daily effect estimations (different from estimations for multi-day averages). Due to the sample nature of the data set used in this analysis and the small number of death counts, the applicability of DLNMs is limited.
Fitting GAMs with interaction terms had the great advantage that all counts could be included into one model and data sets did not need to be divided, thus strengthening the statistical power. Nonetheless, when fitting these interaction models with segmented relationships in order to quantify heat effects, one common breakpoint for all strata included was determined. However, it is quite likely that different subcategories exhibit different thresholds marking a change in the equivalent temperature–mortality relationship. The estimated breakpoints were generally placed between 34 and 35 °C UTCI—a rather high value that corresponds approximately with the 95th percentile. This might lead to an overestimation of heat effect in several subgroups.
There are several further constraints related to the data set that we need to acknowledge. As mentioned above, the SVRS collects vital events from a sample population, instead of the total population. The limited number of counts weakens the statistical power of our analysis and makes stratification more problematic. Similarly, the spatial aggregation and the determination of spatial meteorological averages—which were necessary to increase the statistical power—left meso- and micro-climatic differences unconsidered. Misclassification of exposure might be another limitation as exposure is dependent on the particular micro-environment an individual inhabits. In general, the nature of this eco-epidemiological study includes the danger of the so-called ecological fallacy. Due to the aggregation of data that defines ecological studies, inferences about individual members or a subgroup must be made carefully as these do not necessarily reflect the characteristics of a wider group (Wakefield and Salway 2001). Another limitation, associated with the data quality, refers to the attribution of the causes of deaths. Causes of death were not medically certified and did not follow the International Classification of Disease. Moreover, we could not adjust our analysis for the effects of air pollutants due to the absence of long-term time series of air pollution measurements.
Conclusion
This study demonstrated the relevance of atmospheric effects on human mortality. Although an increase in mortality with decreasing temperature, i.e. a cold effect, occurred over a wide range of values, partly strong heat effects above a threshold temperature were observed for various causes of deaths, age groups and subpopulations. In general, heat effects were observed for all-cause mortality, cardiovascular and infectious disease mortality. Moreover, all age groups exhibited heat-related mortality with strong effects observed for the elderly above the age of 65 years. The effect in children and youths was more delayed than for other ages and, most importantly, a decline in mortality after several days was observed, suggesting a harvesting effect. Males generally seemed to be at higher risk for heat-related all-cause as well as cardiovascular mortality. Likewise, an increased risk for heat-related all-cause and cardiovascular mortality was found in urban areas as compared to rural areas. In contrast, heat-related infectious disease mortality was observed in rural areas whereas no such effect could be observed for urban areas. Furthermore, areas with high SES showed increased heat effect for all-cause and cardiovascular mortality in comparison to areas with low SES. Because of the ongoing dynamics in Bangladesh—particularly the rapid aging of the population, the increase in non-communicable disease prevalence, and the growing urban population—heat effects are likely to be magnified in the future. The projected rise in temperature due to global warming is likely to further aggravate these adverse effects of heat.
References
Baccini M, Biggeri A, Accetta G, Kosatsky T, Katsouyanni K, Analitis A, Anderson H, Bisanti L, D’Ippoliti D, Danova J, Forsberg B, Medina S, Paldy A, Rabczenko D, Schindler C, Michelozzi P (2008) Heat effects on mortality in 15 European cities. Epidemiology 19(5):711–719
Bangladesh Bureau of Statistics (2008) Report on the Sample Vital Registration System 2007. Dhaka
Basu R (2009) High ambient temperature and mortality: a review of epidemiologic studies from 2001 to 2008. Environ Health 8(1):40
Basu R, Samet JM (2002) Relation between elevated ambient temperature and mortality: a review of the epidemiologic evidence. Epidemiol Rev 24(2):190–202
Becker S, Weng S (1998) Seasonal patterns of deaths in Matlab, Bangladesh. Int J Epidemiol 27(5):814–823
Bell ML, O’Neill MS, Ranjit N, Borja-Aburto VH, Cifuentes LA, Gouveia NC (2008) Vulnerability to heat-related mortality in Latin America: a case-crossover study in São Paulo, Brazil, Santiago, Chile and Mexico City, Mexico. Int J Epidemiol 37(4):796–804
Bhaskaran K, Hajat S, Haines A, Herrett E, Wilkinson P, Smeeth L (2009) Effects of ambient temperature on the incidence of myocardial infarction. Heart 95(21):1760–1769
Burkart K, Breitner S, Schneider A, Khan M, Krämer A, Endlicher W (2011a) The effect of atmospheric thermal conditions and urban thermal pollution on all-cause and cardiovascular mortality in Bangladesh. Environ Pollut 159(8–9):2035–2043
Burkart K, Khan M, Krämer A, Breitner S, Schneider A, Endlicher W (2011b) Seasonal variations of all-cause and cause-specific mortality by age, gender, and socio-economic condition in urban and rural areas of Bangladesh. Int J Equity Health 10:32
Curriero FC, Heiner KS, Samet JM, Zeger SL, Strug L, Patz JA (2002) Temperature and mortality in 11 cities of the Eastern United States. Am J Epidemiol 155(1):80–87
Fouillet A, Rey G, Laurent F, Pavillon G, Bellec S, Guihenneuc-Jouyaux C, Clavel J, Jougla E, Hémon D (2006) Excess mortality related to the August 2003 heat wave in France. Int Arch Occup Environ Health 80(1):16–24
Gasparrini A, Armstrong B, Kenward MG (2010) Distributed lag non-linear models. Stat Med 29(21):2224–2234
Gosling SN, Warren R, Arnell NW, Good P, Caesar J, Bernie D, Lowe JA, van der Linden P, O’Hanley JR, Smith SM (2011) A review of recent developments in climate change science. Part II: the global-scale impacts of climate change. Prog Phys Geogr 35(4):443–464
Gosling S, McGregor G, Lowe J (2012) The benefits of quantifying climate model uncertainty in climate change impacts assessment: an example with heat-related mortality change estimates. Clim Chang 112:217–231
Gouveia N, Hajat S, Armstrong B (2003) Socioeconomic differentials in the temperature–mortality relationship in São Paulo, Brazil. Int J Epidemiol 32(3):390–397
Hashizume M, Armstrong B, Hajat S, Wagatsuma Y, Faruque ASG, Hayashi T, Sack DA (2007) Association between climate variability and hospital visits for non-cholera diarrhoea in Bangladesh: effects and vulnerable groups. Int J Epidemiol 36(5):1030–1037
Hashizume M, Wagatsuma Y, Hayashi T, Saha SK, Streatfield K, Yunus M (2009) The effect of temperature on mortality in rural Bangladesh—a population-based time-series study. Int J Epidemiol 38(6):1689–1697
Ishigami A, Hajat S, Kovats RS, Bisanti L, Rognoni M, Russo A, Paldy A (2008) An ecological time-series study of heat-related mortality in three European cities. Environ Health 7(1):5
Jaffar S, Leach A, Greenwood A, Jepson A, Muller O, Ota M, Bojang K, Obaro S, Greenwood B (1997) Changes in the pattern of infant and childhood mortality in Upper River Division, The Gambia, from 1989 to 1993. Tropical Med Int Health 2(1):28–37
Jendritzky G, Havenith G, Weihs P, Batchvarova E, DeDear R (2007) The Universal Thermal Climate Index UTCI. NCUB London, London
Kaiser R, Le Tertre A, Schwartz J, Gotway C, Daley W, Rubin C (2007) The effect of the 1995 heat wave in Chicago on all-cause and cause-specific mortality. Am J Public Health 97(1):158–162
Kelishadi R, Alikhani S, Delavari A, Alaedini F, Safaie A, Hojatzadeh E (2008) Obesity and associated lifestyle behaviours in Iran: findings from the First National Non-communicable Disease Risk Factor Surveillance Survey. Public Health Nutr 11(3):246–251
Khan MMH, Krämer A, Grübner O (2009) Comparison of health-related outcomes between urban slums, urban affluent and rural areas in and around Dhaka megacity, Bangladesh. Die Erde 140(1):69–87
Klinenberg E (2002) Heat wave: a social autopsy of disaster in Chicago. University Of Chicago Press, Chicago
Matzarakis A, Rutz F, Mayer H (2007) Modelling radiation fluxes in simple and complex environments—application of the RayMan model. Int J Biometeorol 51:323–334
McGregor IA, Billewicz WZ, Thomson AM (1961) Growth and mortality in children in an African village. Br Med J 2(5268):1661–1666
McGregor G, Pelling M, Wolf T, Gosling S (2007) The social impacts of heat waves. Science Report SC20061/SR6. Environment Agency, Bristol. ISBN 978-1-84432-811-6
McMichael AJ, Wilkinson P, Kovats RS, Pattenden S, Hajat S, Armstrong B, Vajanapoom N, Niciu EM, Mahomed H, Kingkeow C, Kosnik M, O’Neill MS, Romieu I, Ramirez-Aguilar M, Barreto ML, Gouveia N, Nikiforov B (2008) International study of temperature, heat and urban mortality: the "ISOTHURM" project. Int J Epidemiol 37(5):1121–1131
Medina-Ramón M, Schwartz J (2007) Temperature, temperature extremes, and mortality: a study of acclimatisation and effect modification in 50 US cities. Occup Environ Med 64:827–833
Murray CJL, Lopez AD (1997) Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 349(9064):1498–1504
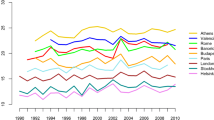
Nastos P, Matzarakis A (2012) The effect of air temperature and human thermal indices on mortality in Athens, Greece. Theor Appl Climatol 108(3–4):591–599
O’Neill M, Hajat S, Zanobetti A, Ramirez-Aguilar M, Schwartz J (2005) Impact of control for air pollution and respiratory epidemics on the estimated associations of temperature and daily mortality. Int J Biometeorol 50(2):121–129
O’Neill MS, Zanobetti A, Schwartz J (2003) Modifiers of the temperature and mortality association in seven US cities. Am J Epidemiol 157(12):1074–1082
O’Neill MS, Hajat S, Zanobetti A, Ramirez-Aguilar M, Schwartz J (2005) Impact of control for air pollution and respiratory epidemics on the estimated associations of temperature and daily mortality. Int J Biometeorol 50(2):121–129
Proctor MH, Moore LL, Singer MR, Hood MY, Nguyen US, Ellison RC (1996) Risk profiles for non-communicable diseases in rural and urban schoolchildren in the Republic of Cameroon. Ethn Dis 6(3–4):235–243
Rau R (2006) Seasonality in human mortality. A demographic approach. Springer, Berlin
Reddy KS, Yusuf S (1998) Emerging epidemic of cardiovascular disease in developing countries. Circulation 97(6):596–601
Robine J-M, Cheung SL, Le Roy S, Van Oyenm H, Herrmann FR (2007) Report on excess mortality in Europe during summer 2003. 2003 Heat Wave Project. EU Community Action Programme for Public Health, Grant Agreement 2005114
Schär C, Jendritzky G (2004) Climate change: Hot news from summer 2003. Nature 432(7017):559–560
Shetty PS (2002) Nutrition Transition in India. Public Health Nutr 5(1A):175–182
Smoyer K, Rainham D, Hewko J (2000) Heat-stress-related mortality in five cities in southern Ontario: 1980–1996. Int J Biometeorol 44(4):190–197
Stafoggia M, Forastiere F, Agostini D, Caranci N, de’Donato F, Demaria M, Michelozzi P, Miglio R, Rognoni M, Russo A, Perucci CA (2008) Factors affecting in-hospital heat-related mortality: a multi-city case-crossover analysis. J Epidemiol Community Health 62(3):209–215
United Nations (2004) World population to 2300. United Nations, New York
United Nations (2008) World Urbanization Prospects: The 2007 Revision. United Nations, New York
Wakefield J, Salway R (2001) A statistical framework for ecological and statistical studies. J R Stat Soc 164(1):119–137
Wood S (2006) Generalized additive models: an introduction with R. Chapman & Hall/CRC, London
World Health Organisation (2010) Noncommunicable disease risk factors and socioeconomic inequalities—what are the links? A multicountry analysis of noncommunicable disease surveillance data. Western Pacific Region. WHO, Geneva
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Burkart, K., Breitner, S., Schneider, A. et al. An analysis of heat effects in different subpopulations of Bangladesh. Int J Biometeorol 58, 227–237 (2014). https://doi.org/10.1007/s00484-013-0668-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-013-0668-5