
Abstract
Objectives: From August 1st to 20th, 2003, the mean maximum temperature in France exceeded the seasonal norm by 11–12°C on nine consecutive days. A major increase in mortality was then observed, which main epidemiological features are described herein. Methods: The number of deaths observed from August to November 2003 in France was compared to those expected on the basis of the mortality rates observed from 2000 to 2002 and the 2003 population estimates. Results: From August 1st to 20th, 2003, 15,000 excess deaths were observed. From 35 years age, the excess mortality was marked and increased with age. It was 15% higher in women than in men of comparable age as of age 45 years. Excess mortality at home and in retirement institutions was greater than that in hospitals. The mortality of widowed, single and divorced subjects was greater than that of married people. Deaths directly related to heat, heatstroke, hyperthermia and dehydration increased massively. Cardiovascular diseases, ill-defined morbid disorders, respiratory diseases and nervous system diseases also markedly contributed to the excess mortality. The geographic variations in mortality showed a clear age-dependent relationship with the number of very hot days. No harvesting effect was observed. Conclusions: Heat waves must be considered as a threat to European populations living in climates that are currently temperate. While the elderly and people living alone are particularly vulnerable to heat waves, no segment of the population may be considered protected from the risks associated with heat waves.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
From August 1st to 5th, 2003, the average maximum temperatures recorded in France increased from a value close to the normal value (25°C) to 37°C, then remained between 36 and 37°C until August 13th, before beginning to fall (28°C on August 16th). Almost all of the population of France, i.e. approximately 60 million people, was exposed to the heat wave: the temperature exceeded 35°C for at least 9 days in 61 of the 96 French departements. A few days after the beginning of the heat wave, information reported by the medical emergency services, fire department and hospital emergency departments showed an abrupt increase in the number of emergency interventions and in the mortality accompanying the heat wave.
The mortality associated with heat has been described and reviewed by several authors (Basu and Samet 2002; Besancenot 2002).
Some authors have described the association between the usual daily fluctuations in temperature and mortality using time series or a spatial approach (Buechley et al. 1972; Dessai 2002; Diaz et al. 2002; Kalkstein and Smoyer 1993; Katsouyanni et al. 1993; Kunst et al. 1993; Matzarakis and Mayer 1991; Oechsli and Buechley 1970; Sartor et al. 1995; Shumway et al. 1988; Smoyer 1998; Smoyer et al. 2000).
Others have focused on individual major heat episodes, in which an exceptional increase in mortality was observed concomitantly with an exceptional heat wave. Those authors described the characteristics of the mortality during or after the heat wave (Applegate et al. 1981; Buechley et al. 1972; Dessai 2002; Ellis and Nelson 1978; Ellis et al. 1980; Henschel et al. 1969; Jones et al. 1982; Katsouyanni et al. 1993; Naughton et al. 2002; Qiu et al. 2002; Rooney et al. 1998; Sartor et al. 1995; Schuman 1972; Whitman et al. 1997). Studies of the 2003 heat waves in Western Europe have been conducted for Portugal (Nogueira et al. 2005), Spain (Simon et al. 2005), Italy (Conti et al. 2005), England and Wales (Johnson et al. 2005), the Netherlands (Garssen et al. 2005) and Switzerland (Grize et al. 2005). The probable increase in the frequency of such events in the twenty-first century has been stressed, as have the time- and place-dependence of the main characteristics of that mortality.
Given that context and using the latter approach, the epidemiological characteristics of the excess mortality associated with the heat wave in France in August 2003 have been reported herein, on the basis of the studies carried out at the French National Institute for Health and Medical Research (Inserm) by the authors and publicly reported to the French health authorities (Hémon and Jougla 2003; Hémon and Jougla 2004).
Material and methods
The observations made from August 1st to November 30th, 2003 in mainland France, were compared to the similar observations for the period 2000–2002, taken as the reference period. The mortality data were derived from the merged data bases of Inserm and INSEE (National Institute of Statistics and Economic Studies), thus ensuring that the data were complete.
A prior descriptive analysis of the daily mortality-rate process over the reference period has shown that, when the seasonal effect and linear annual trend were controlled, the residuals were distributed as a first-order autoregressive process with extra-Poisson variability. Two methods were then used to estimate the expected number of deaths and the expected variance of daily death counts in 2003. Method A combined modelling of the time course of monthly mortality rates, by age and gender, from 2000 to 2002, extrapolated to 2003, with estimations of the populations by year, age and gender, from 2000 to 2003. The model adopted was a log-linear Poisson model incorporating a linear annual trend and a specific term for each month of the year. Method B consisted in estimating the mean mortality rates by age, gender and month, from 2000 to 2002, and applying them to the 2003 population estimates. In both cases, an over-dispersion parameter was estimated and applied to parameter variance estimation. Ten-year age groups were considered.
For France as a whole, method A was adopted, since the daily numbers of deaths observed from March to June 2003 were, on average, closer to the estimated values calculated using method A, did not differ significantly from them, and differed significantly from the estimated values calculated using method B. At the finer geographical scale of the 22 “regions” and 96 “departements” that constitute mainland France, method B proved superior to method A on the basis of the same criteria.
Given the observed (O) and the expected (E) numbers of deaths, mortality was quantified using excess mortality (O−E), rounded up to the nearest integer, and mortality ratios (O/E).
On the basis of the fluctuations in the daily numbers of deaths that were observed during the reference period (days of August in 2000, 2001 and 2002), “95% fluctuation intervals” were defined as intervals in which there was a 95% probability of observing the daily numbers of deaths in the future if they had the same expected value, variance and auto-correlation as the deaths which were observed during the reference period. “Fluctuation intervals” are therefore prediction intervals.
The 95% fluctuation intervals of the observed mortality around the expected mortality for the period 2000–2002 were estimated by day, 10-day period and month, taking into account the autoregressive structure of the daily mortality-rate process and the extra-Poisson variability observed over the reference period.
The analysis of the causes of death was conducted on the causes of death reported by the physicians making out the death certificates as the “initial” cause. The latter is defined as the cause initiating the morbid process resulting in death. The causes of death were classified using the International Classification of Diseases (ICD10) and an additional category for deaths reported to be directly related to the heat wave by the physician, i.e.: dehydration, hyperthermia and heatstroke.
Usually, coding the medical causes of death involves a long validation process. Validation is still ongoing for 2002. In the 2003 heat wave context, validation was accelerated for August 2003. It was thus possible to compare the number of deaths by cause occurring in France in the first 20 days of August 2003 with the means of the same death counts for August 2000 and 2001, considered to be the expected number of deaths by cause. The statistical significance of the difference between the observed and expected number of deaths due to a given cause was determined under the hypothesis that the numbers of deaths used in the comparisons were independently Poisson distributed.
The daily maximum and minimum temperature statistics used are those derived from the Météo-France network of 192 meteorological stations representative of the cities of France. For each of the 96 departements of France, a “number of very hot days” was determined. The number was defined as the number of days on which the minimum and maximum temperatures reported by the departement’s meteorological stations simultaneously exceeded the corresponding 30-year averages by 5 and 9°C, respectively, between August 1st and 20th, 2003. The temperature cut-off points (5 and 9°C) were chosen so as to minimize the deviance of the relationship between the mortality ratios and the number of very hot days using a Poisson regression. The 96 France departements were divided into four groups with nearly equal numbers of expected deaths and an increasing number of very hot days: 0–1; 2–3; 4–7; 8–13 days.
Results
Time course of the heat wave and excess mortality
For the period from March to June 2003, approximately 95% of the observed mortality ratios were shown to lie within the 95% fluctuation intervals. This was also true for the daily time course of the mortality in July (Fig. 1).

Number of excess deaths observed during the French heat wave from July to September 2003 and average daily maximum (T max) and minimum (T min) temperatures recorded during the period. The X axis shows the 92 days from July 1st to September 30th 2003. The histogram shows the numerical values of the daily excess mortality for August 4, 8, 12 and 16. The dotted horizontal lines show the limits of the 95% fluctuation intervals of the daily number of deaths
In August, the mortality first deviated significantly from its usual range of fluctuation on the 4th. The daily excess then increased regularly and massively, reaching 1,193 deaths on August 8th and 2,200 deaths on August 12th (Fig. 1). Excess mortality then fell to 1,943 deaths on August 13th and 988 on August 14th. Mortality had returned to normal as of August 19th. The fall-off in excess mortality reflected the fall in temperature, stabilizing around August 20th. The cumulative excess mortality from August 1st to 20th was 14,729 deaths, equivalent to an excess mortality of 55%.
Excess mortality by age and gender
Overall, no mortality ratio significantly greater than unity was observed for subjects aged less than 35 years (Table 1). From the age of 35 years, the mortality ratios were significantly greater than 1 and increased regularly with age, rising from 1.19 for subjects aged 35–44 years to 2.00 for subjects aged 95 years and over. The number of excess deaths increased very rapidly with age: 11,731 of the 14,729 excess deaths occurred in subjects aged 75 years and over and 2,930 in subjects aged 35–74 years.
Among male subjects, significant excess mortality was observed for infants aged less than 1 year (+29%) and adults aged 35–44 years (+27%), while, for female subjects in those age groups, mortality was normal. From age 55 years, the mortality ratios by age group were significantly higher for women, by about 15%. The total excess mortality for women (+9,378 deaths) was 75% higher than that for men (+5,351 deaths).
Excess mortality by place of death
Major excess mortalities were observed for deaths at home (+5,130 deaths), in retirement homes (+2,574 deaths) and in public hospitals (+5,996 deaths). The relative increase in mortality at home (+74%) and in retirement homes (+91%) was, however, markedly greater than that observed in public hospitals (+45%) and private clinics (+22%). This was observed both globally and by age group (Table 2).
Excess mortality by matrimonial status
The mortality ratios by age group over the period from August 1st to 20th (Table 2) were much higher for single people than for married people, while divorced and widowed subjects showed intermediate values.
Medical causes of death
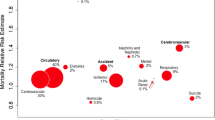
Certain medical causes of death had a major impact on the overall increase in mortality (Table 3):
-
The causes directly related to the heat wave (heatstroke, hyperthermia and dehydration) responsible for 3,306 deaths, i.e. a 20-fold overall increase in the number of deaths, and an even greater increase in certain age-group categories,
-
Circulatory system diseases (+3,004 deaths), ill-defined morbid conditions (+1,741 deaths), respiratory system diseases (+1,365 deaths) and nervous system diseases (+1,001 deaths).
Other medical causes of death, although contributing less markedly to the overall excess mortality, increased in frequency by 70–90% during the same period: mental disorders (+748 deaths), infectious diseases (+483 deaths), genitourinary system diseases (+381 deaths) and endocrine and nutritional diseases (+620 deaths).
Almost all the other medical causes of death increased, but to a lesser extent.
In subjects aged less than 45 years, only the causes of death directly related to the heat wave and death due to ill-defined morbid conditions and musculoskeletal diseases increased. These increases were observed for men only. For subjects aged 45–74 years and those aged 75 years or more, the cause-of-death profiles were similar and also similar to that for the total population.
Geographic variability of the excess mortality
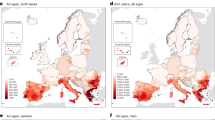
In all the 22 regions of France a significant increase in mortality was observed from August 1st to 20th, 2003. However, the geographic heterogeneity of the mortality was marked (Fig. 2). The highest excess mortality was observed in the Paris region (+142%), the most heavily populated and urbanized area: +149% for the city of Paris and +174% for the nearest suburb (immediately surrounding Paris). The region contiguous with the Paris area in the south-west had the second highest mortality ratio (+104%), although it has no major cities and is relatively little urbanized. In contrast, lower excess mortalities were observed in the Mediterranean, Atlantic and Channel coastal regions (Fig. 2, left map). While the increases were statistically significant, they were smaller, of the order of 20%.

Geographic distributions of mortality ratios O/E (left map) and the number of “very hot days” (right map) by Departement in France—August 1st to 20th, 2003. O observed number of deaths, E expected number of deaths, O/E mortality ratio. The mortality ratios have been grouped into five classes containing approximately equal expected numbers of deaths. The 96 French departements have been grouped into four classes on the basis of the number of “very hot days”. Number of “very hot days”: number of days on which the minimum and maximum temperatures simultaneously exceeded the corresponding 30-year averages by 5 and 9°C, respectively, between August 1st and 20th, 2003
The mortality ratios observed over the period from August 1st to 20th in the 96 French departements increased with the number of very hot days in each departement (Table 2). The increase was statistically significant for subjects aged less than 55 years, significant and very marked for subjects aged 55–74 years, significant and still more pronounced for subjects aged 75 years and older.
The geographic distribution of the number of “very hot days” (Fig. 2, right map) was similar to that of mortality ratios (Fig. 2, left map).
With regard to infants aged less than 1 year, no excess mortality was observed for girls, either in the Paris region or in the rest of France. For boys, the excess mortality in the Paris region (+55%) was significantly greater than that in the remainder of France (+12%).
Post-heat wave time course of overall mortality
The daily mortality observed from August 19th to September 30th, 2003, for the overall population did not deviate from its usual fluctuation intervals (Fig. 1). Such was also the case for the daily mortality observed from October 1st to November 30th, 2003, for the overall population.
The return of mortality to normal was also observed on the 10-day period scale as of the third 10-day period in August, and, on the one-month scale, as of the month of September. Normalization affected both the overall population of France and the various sub-populations that exhibited various degrees of excess mortality over the first two 10-day periods in August. Mortality returned to normal as of August 19th and remained so until November 30th, 2003:
-
For all age groups,
-
For both men and women,
-
For all place-of-death categories (at home, hospital, institutions and retirement homes),
-
For all matrimonial status categories (single, divorced, widowed and married),
-
For each of the 22 French regions and each of the 4 groups of departements defined by the number of very hot days experienced between August 1st and 20th, 2003.
Discussion
In the first fortnight of August 2003, the entire population of the 60 million inhabitants of France was exposed to a heat wave of unprecedented amplitude. The first significant excess mortality was observed 3 days after the maximum temperatures rose above the seasonal normal value. Over the nine consecutive days that maximum temperatures remained 11–12°C higher than the seasonal average, the daily excess mortality increased constantly. Mortality returned to normal for the overall population of France on August 19th, 4 days after the maximum temperatures had returned to values close to the seasonal averages. Almost 15,000 excess deaths occurred between August 1st and 20th, 2003, i.e. 55% more than the expected mortality.
On a larger scale, from June to August 2003, the whole of Western Europe was struck by a series of heat waves. Excess mortality was observed in Portugal (+1,316 deaths) (Nogueira et al 2005), Spain (+6,595–8,648 deaths) (Simon et al. 2005), Italy (in 21 cities: +3,134 deaths) (Conti et al. 2005), England and Wales (+2,139 deaths) (Johnson et al. 2005), the Netherlands (+1,400–2,200 deaths) (Garssen et al. 2005) and Switzerland (+975 deaths) (Grize et al. 2005). Therefore, the overall excess death count of the 2003 heat wave is higher if all Western European countries are considered from June to August. A large fraction of the excess deaths appears to have occurred in France between August 1st and 20th, with a marked increase in mortality applied to a large population (60 million people).
Numerous other episodes of major excess mortality associated with heat waves have been reported in North America (Applegate et al. 1981; Buechley et al. 1972; Ellis and Nelson 1978; Henschel et al. 1969; Jones et al. 1982; Naughton et al. 2002; Schuman 1972; Whitman et al. 1997), Europe (Dessai 2002; Ellis et al. 1980; Katsouyanni et al. 1993; Rooney et al. 1998; Sartor et al. 1995) and Japan (Qiu et al. 2002). As was the case in those reported heat waves, the excess mortality observed in France in August 2003 increased with age.(Applegate et al. 1981; Bark 1998; Oechsli and Buechley 1970; Schuman 1972; Whitman et al. 1997). It is, however, noteworthy that even though the majority of the excess mortality affected subjects aged 75 years and over (+11,731 deaths), very marked excesses were nonetheless observed in all age groups from 35 to 74 years (+2,930 deaths). Moderate but significant excess mortality also occurred among male infants aged less than 1 year (+25 deaths). If the elderly are a particularly vulnerable population, the belief that they only are at risk of heat-related death would thus be erroneous.
Both women (Michelozzi et al. 2005; Rooney et al. 1998) and men (Whitman et al. 1997) have been reported to have higher mortality ratios than the opposite gender. In this study, the overall excess mortality for women was 75% higher than that for men. However, most of this difference may be explained by the greater longevity of women. When equal ages are considered, from age 55 years, there is only a female excess mortality of about 15%. While the difference needs to be elucidated, it would be imprudent to consider that only women are exposed to the risk of death in heat waves.
While the relative increase in mortality observed in hospitals and clinics was less than that for subjects at home or in retirement homes, the absolute excess mortality in the public hospitals was nonetheless major. Thus, all the medical emergency services and emergency care management systems were subject to exceptionally intense demand. The particularly high mortality ratios observed among people living at home and the substantially higher mortality ratios observed for single and divorced subjects compared to married subjects point to the key role of isolation in vulnerability to heat waves (Kilbourne et al. 1982; Naughton et al. (2002); Semenza et al. 1996). People living alone at home are to be considered a sub-population exposed to a particularly high risk.
The deaths occurring during the heat waves described in the literature were related to a wide variety of diseases (Applegate et al. 1981; Ellis and Nelson 1978; Henschel et al. 1969; Michelozzi et al. 2005; Rooney et al. 1998; Schuman 1972; Semenza et al. 1996). Among the variety of medical causes of the excess deaths in France in August 2003, some reflect the very morbid process which resulted in death. This is the case for the deaths due to heatstroke, hyperthermia and dehydration, but also, probably, for a fraction, at least, of the deaths for other diseases, particularly circulatory and respiratory diseases (Applegate et al. 1981; Ellis and Nelson 1978; Henschel et al. 1969; Huynen et al. 2001; Michelozzi et al. 2005; Rooney et al. 1998; Schuman 1972). Certain medical causes of death may also reflect special vulnerability to a heat wave associated with a chronic disease. This was particularly the case for deaths related to mental disorders, nervous system diseases (Bark 1998; Michelozzi et al. 2005; Naughton et al. 2002; Semenza et al. 1996) and endocrine diseases (Michelozzi et al. 2005; Schuman 1972) but also, probably, for other causes.
The excess mortality was substantially greater in the departements that had the greatest number of very hot days and more markedly in the older age groups. However, the relationship is far from perfect: the meteorological indicator of heat-wave exposure used herein is, in fact, only a parameter enabling classification of the 96 French departements on an ordinal scale of heat-wave exposure. An analysis of heat heterogeneity on a finer geographic scale is required. In addition, several heat-wave characteristics appear to have a strong impact on mortality: an abrupt major increase in temperature, whose impact is immediate or very short term (Kalkstein and Smoyer 1993); a succession of very hot days (Gover 1938; Smoyer et al. 2000); and the time during the summer at which the heat wave occurs (Diaz et al. 2002). The exact form of the impact is still far from being elucidated. Heat waves may be described using multiple meteorological indicators such as minimum, maximum or apparent temperature and relative humidity (Ellis et al. 1980; Kunst et al. 1993; Oechsli and Buechley 1970). The latter remained particularly low during the August 2003 heat wave and the daily meteorological data for that indicator were therefore not taken into account herein.
The excess mortality observed showed great geographic heterogeneity ranging from +20% in the least-affected coastal regions to +142% in the Paris area region. The particularly marked excess mortality in the city of Paris and the immediately suburbs is probably related to the higher risks of death in large metropolitan areas reported by certain authors (Buechley et al. 1972; Katsouyanni et al. 1993). This observation is to be considered in the context of the heat island concept (Buechley et al. 1972; Clarke 1972; Livada et al. 2002; Schuman 1972; Smoyer 1998) and the question of whether there is a synergy between prolonged high temperatures and socioeconomic characteristics (Henschel et al. 1969; Jones et al. 1982; Klinenberg 1999; Michelozzi et al. 2005; Rooney et al. 1998; Smoyer et al. 2000). Some studies also suggest a possible contribution of atmospheric pollution to the increase in the number of deaths during heat waves (Kalkstein and Smoyer 1993; Katsouyanni et al. 1993; Matzarakis and Mayer 1991; Sartor et al. 1995; Shumway et al. 1988). In August 2003, ozone and particulate matter concentrations were particularly high in France: the ozone concentration alert threshold (240 μg/m3) was exceeded for at least one recording station for 12 consecutive days from August 2nd to 13th, 2003. Moreover, exceptionally high values were observed in areas where the ozone concentration is generally low (InVS 2004).
The above factors could explain some of the differences between the geographic distributions of mortality ratios and the number of “very hot days”. Both a finer geographic analysis of temperatures and further investigation of the vulnerability factors related to socioeconomic characteristics are required.
Few observations relating to the existence of a harvesting effect following earlier heat waves are available. They show that a harvesting effect was limited (Braga et al. 2002; Dessai 2002; Hajat et al. 2005; Kalkstein and Smoyer 1993; Sartor et al. 1995) or even non-existent (Huynen et al. 2001; Rooney et al. 1998). In the present study, no harvesting effect was observed; the excess mortality of the August 2003 heat wave was not followed by a less-than-expected number of deaths until the end of 2003. Moreover, the excess mortality in the first 20 days of August 2003 was not followed, from August 21st to November 30th, 2003, by persistent excess mortality.
According to the IPCC’s (2001) climate change models, average temperatures should increase by 1.4–5.8°C between 1990 and 2100. In 2100, the annual probability of a summer heat wave similar to that which struck western Europe in August 2003 could be greater than 50% (Schär et al. 2004). Given that context, the setting up of systems to prevent the risks related to heat waves, combining long-term preventive measures with alert systems based on short term weather forecasts, needs to be seriously considered even in countries which have, so far, been relatively spared by heat waves. Several preventive and alert systems have been set up in response to heat waves associated with marked excess mortality (http://www.ci.mil.wi.us) (Kalkstein 2000; Naughton et al. 2002; Semenza et al. 1996). In France, the Institut de Veille Sanitaire (InVS), in cooperation with Météo-France set up such a system in June 2004 (InVS 2005).
The epidemiological knowledge that could orient such preventive actions and alert systems is currently far from complete, given that the climate configuration of population exposure to heat waves and the population sensitivities thereto appear to be population- and time-dependent (Basu and Samet 2002; Besancenot 2002). Research on modelling heat-mortality relationships and on the individual and collective vulnerability factors that modulate those relationships is therefore required.
The findings reported herein show that while there are populations that are particularly vulnerable to heat waves, such as the elderly and people living alone, no segment of the population may be considered protected from the risks associated with heat waves.
References
Applegate WB, Runyan JW Jr, Brasfield L et al (1981) Analysis of the 1980 heat wave in Memphis. J Am Geriatr Soc 29(8):337–342
Bark N (1998) Deaths of psychiatric patients during heat waves. Psychiatr Serv 49(8):1088–1090
Basu R, Samet JM (2002) Relation between elevated ambient temperature and mortality: a review of the epidemiologic evidence. Epidemiol Rev 24(2):190–202
Besancenot J (2002) Vagues de chaleur et mortalité dans les grandes agglomérations urbaines. Environ Risques Santé 4(1):229–240
Braga AL, Zanobetti A, Schwartz J (2002) The effect of weather on respiratory and cardiovascular deaths in 12 U.S. cities. Environ Health Perspect 110(9):859–863
Buechley RW, Van Bruggen J, Truppi LE (1972) Heat island equals death island? Environ Res 5(1):85–92
Clarke JF (1972) Some effects of the urban structure on heat mortality. Environ Res 5(1):93–104
Conti S, Meli P, Minelli G et al (2005) Epidemiologic study of mortality during the Summer 2003 heat wave in Italy. Environ Res 98(3):390–399
Dessai S (2002) Heat stress and mortality in Lisbon part I. Model construction and validation. Int J Biometeorol 47(1):6–12
Diaz J, Jordan A, Garcia R et al (2002) Heat waves in Madrid 1986–1997: effects on the health of the elderly. Int Arch Occup Environ Health 75(3):163–170
Ellis FP, Nelson F (1978) Mortality in the elderly in a heat wave in New York City, August 1975. Environ Res 15(3):504–512
Ellis FP, Prince HP, Lovatt G, Whittington RM (1980) Mortality and morbidity in Birmingham during the 1976 heatwave. Q J Med 49(193):1–8
Garssen J, Harmsen C, De Beer J (2005) The effect of the summer 2003 heat wave on mortality in the Netherlands. Euro Surveill 10(7)
Gover M (1938) Mortality during periods of excessive temperature. Public Health Rep 53:1122–1143
Grize L, Huss A, Thommen O, Schindler C, Braun-Fahrlander C (2005) Heat wave 2003 and mortality in Switzerland. Swiss Med Wkly 135(13–14):200–205
Hajat S, Armstrong BG, Gouveia N, Wilkinson P (2005) Mortality displacement of heat-related deaths: a comparison of Delhi, Sao Paulo, and London. Epidemiology 16(5):613–620
Hémon D, Jougla E (2003) Surmortalité liée à la canicule d’août 2003: Estimation de la surmortalité et principales caractéristiques épidémiologiques. Inserm. http://www.sante.gouv.fr/htm/actu/surmort_canicule/rapport_complet.pdf
Hémon D, Jougla E (2004) Surmortalité liée à la canicule d’août 2003. Suivi de la mortalité 21 Août- 31 Décembre 2003—Causes médicales des décès 1–20 Août 2003. Inserm. http://www.ifr69.vjf.inserm.fr/~webifr/pdf/INSERM_rapport_canicule_octobre2004.pdf
Henschel A, Burton LL, Margolies L, Smith JE (1969) An analysis of the heat deaths in St. Louis during July, 1966. Am J Public Health Nations Health 59(12):2232–2242
Huynen MM, Martens P, Schram D, Weijenberg MP, Kunst AE (2001) The impact of heat waves and cold spells on mortality rates in the Dutch population. Environ Health Perspect 109(5):463–470
InVS (2004) Vague de chaleur de l’été 2003 : relations entre températures, pollution atmosphérique et mortalité dans neuf villes françaises. Rapport d’étude. Département Santé environnement. http://www.invs.sante.fr/publications/2004/psas9_070904/rapport.pdf
InVS (2005) Système d’alerte canicule et santé 2005. Rapport opérationnel. Département des maladies chroniques et traumatismes Département Santé environnement. http://www.invs.sante.fr/publications/2005/sacs_2005/rapport_sacs_2005.pdf
IPCC (2001) Climate change 2001: synthesis report. A contribution of working groups I, II and III to the 3rd assessment report of the intergovernmental panel on climate change. Cambridge University Press, Cambridge
Johnson H, Kovats S, McGregor G et al (2005) The impact of the 2003 heat wave on daily mortality in England and Wales and the use of rapid weekly mortality estimates. Euro Surveill 10(7)
Jones TS, Liang AP, Kilbourne EM et al (1982) Morbidity and mortality associated with the July 1980 heat wave in St Louis and Kansas City, Mo. JAMA 247(24):3327–3331
Kalkstein LS, Smoyer KE (1993) The impact of climate change on human health: some international implications. Experientia 49(11):969–979
Kalkstein LS (2000) Saving lives during extreme weather in summer. BMJ 321(7262):650–651
Katsouyanni K, Pantazopoulou A, Touloumi G et al (1993) Evidence for interaction between air pollution and high temperature in the causation of excess mortality. Arch Environ Health 48(4):235–242
Kilbourne EM, Choi K, Jones TS, Thacker SB (1982) Risk factors for heatstroke. A case-control study. JAMA 247(24):3332–3336
Klinenberg E (1999) Denaturalizing disaster: a social-autopsy of the 1995 Chicago heat wave. Theory Soc 28:239–95
Kunst AE, Looman CW, Mackenbach JP (1993) Outdoor air temperature and mortality in the Netherlands: a time-series analysis. Am J Epidemiol 137(3):331–341
Livada I, Santamouris M, Niachou K, Papanikolaou N, Mihalakalou G (2002) Determination of places in the great Athens area where the heat island effect is observed. Theor Appl Climatol 71:219–230
Matzarakis A, Mayer H (1991) The extreme heat wave in Athens in july 1987 from the point of view of human biometeorology. Atmos Environ 25B:203–211
Michelozzi P, de Donato F, Bisanti L et al (2005) The impact of the summer 2003 heat waves on mortality in four Italian cities. Euro Surveill 10(7)
Naughton MP, Henderson A, Mirabelli MC et al (2002) Heat-related mortality during a 1999 heat wave in Chicago. Am J Prev Med 22(4):221–227
Nogueira PJ, Falcao JM, Contreiras M et al (2005) Mortality in Portugal associated with the heat wave of August 2003: early estimation of effect, using a rapid method. Euro Surveill 10(7)
Oechsli FW, Buechley RW (1970) Excess mortality associated with three Los Angeles September hot spells. Environ Res 3(4):277–284
Qiu D, Tanihata T, Aoyama H et al (2002) Relationship between a high mortality rate and extreme heat during the summer of 1999 in Hokkaido Prefecture, Japan. J Epidemiol 12(3):254–257
Rooney C, McMichael AJ, Kovats RS, Coleman MP (1998) Excess mortality in England and Wales, and in Greater London, during the 1995 heatwave. J Epidemiol Commun Health 52(8):482–486
Sartor F, Snacken R, Demuth C, Walckiers D (1995) Temperature, ambient ozone levels, and mortality during summer 1994, in Belgium. Environ Res 70(2):105–113
Schär C, Vidale PL, Luthi D et al (2004) The role of increasing temperature variability in European summer heatwaves. Nature 427:332–336
Schuman SH (1972) Patterns of urban heat-wave deaths and implications for prevention: data from New York and St. Louis during July, 1966. Environ Res 5(1):59–75
Semenza JC, Rubin CH, Falter KH et al (1996) Heat-related deaths during the July 1995 heat wave in Chicago. N Engl J Med 335(2):84–90
Shumway RH, Azari AS, Pawitan Y (1988) Modeling mortality fluctuations in Los Angeles as functions of pollution and weather effects. Environ Res 45(2):224–241
Simon F, Lopez-Abente G, Ballester E, Martinez F (2005) Mortality in Spain during the heat waves of summer 2003. Euro Surveill 10(7)
Smoyer KE (1998) Putting risk in its place: methodological considerations for investigating extreme event health risk. Soc Sci Med 47(11):1809–1824
Smoyer KE, Rainham DG, Hewko JN (2000) Heat-stress-related mortality in five cities in Southern Ontario: 1980–1996. Int J Biometeorol 44(4):190–197
Whitman S, Good G, Donoghue ER et al (1997) Mortality in Chicago attributed to the July 1995 heat wave. Am J Public Health 87(9):1515–1518
Acknowledgements
We would like to express our gratitude to the institutions that afforded us various forms of assistance in this study: the “Ministère de la Santé, de la Famille et des Personnes Handicapées” which commissioned the present study; Inserm, INSEE and Météo-France, and to the members of those institutions with whom we worked: V. Lasserre, with Inserm-U170-IFR69; C. Jacquart, H. Lefèvre, M. Bovet, F. Péquignot, A. Le Toullec and M. Pauchard, with Inserm-CépiDc-IFR69; G. Desplanques, C. Beaume, F. Clanché, R. Merlen, D. Morineau and L. Doisneau, with INSEE; P. Courtier, B. Rambaldelli, N. Bourdette and J. Manach with Météo-France. We are also very grateful to A. Mullarky for his skilful assistance in the preparation of the English version of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
A. Fouillet and G. Rey have equally contributed to this work.
Rights and permissions
About this article
Cite this article
Fouillet, A., Rey, G., Laurent, F. et al. Excess mortality related to the August 2003 heat wave in France. Int Arch Occup Environ Health 80, 16–24 (2006). https://doi.org/10.1007/s00420-006-0089-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-006-0089-4