
Abstract
The relationship between air temperature and human mortality is described as non-linear, with mortality tending to rise in response to increasingly hot or cold ambient temperatures from a given minimum mortality or optimal comfort temperature, which varies from some areas to others according to their climatic and socio-demographic characteristics. Changes in these characteristics within any specific region could modify this relationship. This study sought to examine the time trend in the maximum temperature of minimum organic-cause mortality in Castile-La Mancha, from 1975 to 2003. The analysis was performed by using daily series of maximum temperatures and organic-cause mortality rates grouped into three decades (1975–1984, 1985–1994, 1995–2003) to compare confidence intervals (p < 0.05) obtained by estimating the 10-yearly mortality rates corresponding to the maximum temperatures of minimum mortality calculated for each decade. Temporal variations in the effects of cold and heat on mortality were ascertained by means of ARIMA models (Box-Jenkins) and cross-correlation functions (CCF) at seven lags. We observed a significant decrease in comfort temperature (from 34.2°C to 27.8°C) between the first two decades in the Province of Toledo, along with a growing number of significant lags in the summer CFF (1, 3 and 5, respectively). The fall in comfort temperature is attributable to the increase in the effects of heat on mortality, due, in all likelihood, to the percentage increase in the elderly population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Many studies have reported the influence of air temperature on human mortality. This relationship is generally described as being non-linear and V-shaped, due to the fact that mortality rises in response to increasingly hot or cold ambient temperatures from a given comfort or minimum mortality temperature (Kunst et al. 1993; Saez et al. 1995; Alberdi et al. 1998a; Kan et al. 2003; El-Zein et al. 2004). Comfort temperatures may vary according to the climatic characteristics of the designated study area, generally falling as latitude increases or climates become colder, as a consequence of the process of populations adapting to their habitat (Douglas et al. 1991; Keatinge et al. 2000; Curriero et al. 2002). In this respect, towns with lower annual mean temperatures have been observed to register higher heat-related mortality and, conversely, the greater the influence of the summer season, the higher the cold-related mortality (The Eurowinter Group 1997). The surrounding area may also undergo changes that are sufficiently rapid to affect the relationship between temperature, other environmental factors and mortality to a certain extent. In this connection, the influence of environmental variables on morbidity and mortality has been observed to wane as economic development advances, something that in Japan has come to be called “deperiodification” of diseases (Sakamoto-Momiyama 1978). More recent studies have described the way in which the influence of high temperature on mortality has altered with time in some areas, pointing towards a gradually diminishing heat–mortality association (Davis et al. 2003a; Carson et al. 2006; Michelozzi et al. 2006).
It would nevertheless be interesting to ascertain the trend in this non-linear temperature–mortality relationship in terms of comfort or minimum mortality temperature, since this might well serve as a reference in subsequent studies on the relationship between hot and cold temperatures and health indicators (such as morbidity, mortality, hospital admissions, etc.).
Given that there have been no previous studies addressing the influence of temperatures on health indicators in Castile-La Mancha, the information to be obtained will undoubtedly prove novel and useful in drawing up appropriate health plans, and implementing suitable preventive measures and interventions targeting lifestyles or behaviors shown to be risk factors.
The trend, confirmed by experts at the recent Paris meeting of the Intergovernmental Panel on Climate Change (IPCC), towards an overall significant increase in temperatures, coupled with local forecasts issued for Spain as regards not only a rise in mean temperatures, but also the frequency of days with extreme temperatures, particularly in summer (De Castro et al. 2005), render advance evaluation of the potential public health consequences of this process advisable.
Furthermore, most of the studies undertaken to date relate to towns or small geographic areas. Hence, it would also be interesting for methodologies to be applied which enable this type of analysis to target more extensive geographic areas with low population densities, in which it would otherwise be difficult to find statistically significant results, e.g. the Castile-La Mancha Region in central Spain.
This study sought to ascertain the time trend in the maximum temperature of minimum organic-cause mortality in Castile-La Mancha, in the period 1975 to 2003.
Materials and methods
Trends in maximum comfort temperature were analyzed in the five provinces into which Castile-La Mancha is divided, i.e., Albacete, Ciudad Real, Cuenca, Guadalajara and Toledo (Fig. 1).

Provinces of Castile-La Mancha in central Spain
Data were drawn from the Castile-La Mancha Mortality Registry, which comes under the purview of the Regional Health Authority and records all deaths that occurred in Castile-La Mancha from 1975 to 2003 (last year available). Provincial data on daily organic-cause mortality (all except external causes) were coded as per the International Classification of Diseases (ICD 8: 1975–1979, ICD 9: 1980–1998 and ICD 10: 1999–2003), using codes 001–799 for ICD-8 and ICD-9, and A00-R99 for ICD-10. External causes were not included because they display a weak relationship with temperature. The number of deaths were converted into rates per 100,000 population, using annual population data as of 1 January. Provincial population data, furnished by the National Statistics Institute (Instituto Nacional de Estadística), were taken from annual intercensus interpolations calculated on the basis of official 10-yearly censuses (1970, 1981, 1991 and 2001).
Daily temperature records were supplied by the National Meteorology Institute (Instituto Nacional de Meteorología). Those corresponding to provincial capitals (Table 1) were chosen from 42 preselected meteorological stations on the basis of an earlier study, in which daily maximum, mean and minimum temperature data were subjected to a process that, consecutively, consisted of filling in gaps, detecting discontinuities, homogenization, and principal components factor analysis (Miron et al. 2006). This method of factor analysis is a widely-used tool in climatology (Stone 1989; White et al. 1991), which ensures the representativeness of the stations selected and so enables the territory to be divided into areas in which population exposure to air temperature can be assumed to be similar. In the case of Castile-La Mancha, all the daily temperature series (maximum, mean and minimum) proved to belong to a single cluster (Miron et al. 2006), thereby making it possible for the region to be divided into what were considered suitable administrative units, which in our case meant provinces. An earlier study which covered the whole of Spain and used similar methodology, albeit exclusively with daily minimum temperature series, likewise included Castile-La Mancha within a single cluster (Prieto et al. 2004). Moreover, it should be pointed out that the National Preventive Action Plan (Plan Nacional de Actuaciones Preventivas) approved by the Spanish Ministry of Health and Consumer Affairs (Ministerio de Sanidad y Consumo 2007) and designed to combat the effects of excess temperature on health, uses a single representative station for each province, covering areas of up to 21,766 sq km (Badajoz).
Even though the regression coefficient linking maximum temperatures to organic-cause mortality in Castile-La Mancha was slightly lower than that obtained with mean temperatures (and higher than that yielded by minimum temperatures), we nevertheless chose to analyze on the basis of the series of daily maximum temperatures because these were the temperatures that were really generated, and so enabled us to pursue a line of research that was fundamentally related to the effects of heat on the local population. At the same time, such a method made it possible for the results to be compared against those obtained in neighboring regions, such as Madrid, in which studies conducted on heat waves had used series of daily maximum temperatures. Indeed, there can be no doubt that, should the case ever arise, expressing preventive measures in terms of maximum temperatures will make them more readily comprehensible to the population implicated.
To study the time trend in minimum mortality temperatures, the study period was divided into three decades, namely, 1975–1984, 1985–1994 and 1995–2003 (comprising 9 years), thereby establishing a 10-yearly comparison. In this way, we had three groups of data on daily maximum temperatures and daily organic-cause mortality rates for each of the five provinces of Castile-La Mancha (two groups of 10 years and one, the last, of 9 years).
In this type of non-linear, V-shaped temperature-mortality relationship, the best statistical fit is afforded by a quadratic function. In each decade, therefore, a second-order polynomial regression analysis was performed, with daily maximum temperatures as the independent variable and daily mortality rates as the dependent variable. By finding the minimum point of the function (of the adjusted curve), the maximum temperature of minimum mortality for each decade was obtained. In each analysis, estimated mortality rates were obtained, together with their respective confidence intervals (p < 0.05), for each maximum temperature. The comfort temperature obtained for the first decade (T1) was then transferred to the second. Corresponding to it here was an estimation of the organic-cause mortality rate, together with its confidence interval, reflecting the influence of the new socio-demographic structure of the population. In this second decade, the comfort temperature (T2) was calculated, and its estimated mortality rate (with another confidence interval) was then compared against that obtained for T1 under the same socio-economic and socio-demographic structural conditions. If the two confidence intervals failed to overlap, this meant that T1 and T2 would be significantly different. Analysis of the third decade yielded a new maximum temperature of minimum mortality (T3) with an estimated organic-cause mortality rate, a second rate corresponding to T1, and a third to T2, under the same new structural and social conditions. Comparison of the respective confidence intervals determined whether the comfort temperature in this third decade had varied to a statistically significant degree vis-à-vis the first and second decades.
To ascertain whether such variation was due to greater or less intensity in the association between cold or hot temperatures and organic-cause mortality over time, the ARIMA model estimated for the daily maximum temperature series was applied to these and to the series of daily mortality rates. With the residuals obtained from both series, cross-correlation functions (CCF) at 7 lags (Box-Jenkins method) were calculated for warm (June, July, August and September) and cold (November, December, January, February and March) months, and for each of the study decades.
All analyses were performed using the SPSS 11.5 and Statgraphics 5.1 statistical packages.
Results
The maximum temperatures of minimum mortality calculated on the basis of organic-cause mortality rates and their trend can be seen in Table 2. The comfort temperature was observed to fall from the first to the second, and stabilize from the second to the third, decades. In general, there was a downward trend in the comfort temperature over the 29 years studied, except for the Province of Albacete where the overall trend was slightly upward.
Table 3 shows that in the Provinces of Guadalajara and Toledo confidence intervals CI1(T1) and CI2(T2) did not overlap, whereas CI2(T2) and CI3(T3) did. In other words, the mortality rate associated with the maximum temperature of minimum mortality in each decade rose significantly between the first and second but not between the second and third decades. In Ciudad Real, the same occurred between the first two decades, but there was also an increase in rates from the second to the third decades. In Albacete and Cuenca, no significant differences were in evidence. Nevertheless, to ascertain whether the trend in maximum temperature of minimum mortality registered for the overall period was significant, the confidence intervals of organic-cause mortality rates must be compared within each decade. Hence, in the Province of Toledo, no overlap is in evidence for CI2(T1) and CI2(T2), or for CI3(T1) with respect to CI3(T2) and CI3(T3), meaning that the maximum temperature of minimum organic-cause mortality can be said to have fallen significantly (p < 0.05) between both the first and second and the first and third decades. Despite the fact that, in absolute terms, the Provinces of Guadalajara and Cuenca registered the steepest falls in maximum comfort temperature between the periods 1975–1984 and 1985–1994 (9.5°C in the former and 8.5°C in the latter provinces), this failed to prove statistically significant in terms of the confidence intervals of the respective mortality rates. These were practically at the limit of statistical significance for p < 0.05.
Figure 2(a–c) indicates the trend in the relationship between maximum temperatures and organic-cause mortality rates in the Province of Toledo, where statistical significance was reached. A similar trend is observable in the scatter-plot diagrams for Cuenca, Guadalajara and Ciudad Real. As can be seen, not only did the minimum mortality temperature fall but, in addition, the right-hand part of the characteristic V-shape, which depicts the “hot” component of the relationship, continued to rise from decade to decade, and particularly from the first to the second.

Scatter-plot diagrams of daily maximum temperatures (°C) and organic-cause mortality rates (deaths/100,000 inhabitants per day) in the Province of Toledo. Trend shown by decade: a 1975–1984, b 1985–1994, and c 1995–2003
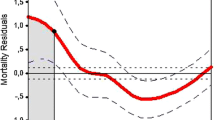
In Fig. 3, the three decades studied are compared by means of the corresponding CCF between the residuals of organic-cause mortality rates and the residuals of daily maximum temperatures during the hot months. There was an increase from only one significant lag (2) (significant increase in mortality at two days of the hot event) in the period 1975–1984, to three significant lags (2, 3 and 4) in 1985–1994, and five in the last decade (1, 2, 3, 4 and 7). It should be pointed out, however, that if the winter months (November to March) are considered, no noteworthy trend between these same decades will be seen.

Ten-yearly trends in CCF at 7 lags (a, b and c), between the residuals of organic-cause mortality rates and the residuals of the series of daily maximum temperatures for the months of June, July, August and September. Province of Toledo
Discussion
The series of maximum temperatures shows that the Region of Castile-La Mancha registered a downward trend in minimum mortality or comfort temperature from 1975–1984 to 1985–1994, with this then stabilizing between the latter decade and 1995–2003. All the provinces display a similar behavior pattern, except Albacete, where this temperature can be said to have remained stable or described a slight upward trend during these years. The decrease in comfort temperature proved statistically significant in the Province of Toledo and was at the limit of statistical significance in the Provinces of Cuenca and Guadalajara. Moreover, if absolute organic-cause mortality data were to be used instead of rates, the downward trend in the maximum temperature of minimum mortality would also prove statistically significant in the Provinces of Ciudad Real and Guadalajara.
This indicates that, in the above provinces, there has been an increase in the effects of heat on the population with respect to the decade 1975–1984, as can also be seen from Fig. 3, which shows growth over time in the coefficients of the corresponding CCF during the summer, with the number of significant lags in Toledo going from 1 to 3 and from 3 to 5. That is to say, in the first decade a significant increase in organic-cause mortality was observed solely on the day immediately after a maximum temperature had been recorded, which then increased to 3 days and, subsequently, to 5 days in later decades. The decline in the comfort temperature is thus due to a greater effect of heat on mortality rather than to the diminishing influence of low temperatures, since the 10-yearly CCF calculated on the basis of the latter display no such growth. This could be particularly dangerous in the light of the above-mentioned forecasts made by the IPCC and local studies (De Castro et al. 2005).
In contrast, other studies, such as those undertaken in US towns (Davis et al. 2003b) and in London (Carson et al. 2006), have reported a reduction in the intensity of the relationship between temperature and mortality, though the methodology used in these studies does not allow for conclusive comparison with the results obtained for Castile-La Mancha. Furthermore, it should be borne in mind that, rather than quantifying the intrinsic 10-yearly variation in the temperature-mortality association, the aim of our study was simply to ascertain the trend in real comfort temperature for the practical purposes of planning subsequent studies and health information.
Paradoxically, the growing relationship observed between hot temperatures and mortality coincided precisely with a notable increase in the socio-economic development of the Castile-La Mancha Region, reinforced by Spain’s entry into the European Economic Community in 1986. This also contradicts the arguments put forward in other studies with respect to the direct relationship between the level of economic development (better infrastructures, health care services, access to air-conditioning, etc.) and the decrease in heat-related mortality (Pappas et al. 1993; Keatinge et al. 2000; Braga et al. 2001; O’Neill et al. 2003; El-Zein and Tewtel-Salem 2005). Accordingly, there must be specific regional factors that counteract the effect of such development and dictate a different course.
The continuous percentage growth in the elderly population could account for the increase in heat-related mortality between decades and, in turn, for the ensuing reduction in the minimum mortality temperature.
In this regard, the percentage of population over the age of 65 years increased notably in Castile-La Mancha across the 29 years analyzed. For instance, it went from 11.41% in 1975 to 18.02% in 2003 in the Province of Albacete, and from 12.42% to 19.06% in the Province of Toledo (Fig. 4), leading to a rise in organic-cause mortality rates (slight and non-significant in Albacete), as explained above. The relationship between ambient temperature and mortality has been described as being more intense in the elderly population (Díaz et al. 2002a; Conti et al. 2005), due principally to the increase in circulatory-and respiratory-cause mortality (Bull 1980; Enquselassie et al. 1993; Pan et al. 1995; Carder et al. 2005). There are studies undertaken in Madrid, an area bordering on Castile-La Mancha and forming part of the same natural region, which show this to be so (Montero Rubio et al. 1997; Díaz et al. 2002b).

Trend from 1975 to 2003 in the percentage of the population over the age of 65 years in the Provinces of Toledo (a) and Albacete (b)
Yet, under the same conditions of demographic evolution, the interdecennial mortality-maximum temperature pattern observed for the Province of Albacete was not the same as that observed for the remaining provinces in the region. Curiously, this is the province having the greatest population concentration in an urban centre, i.e., Albacete, with 155,142 inhabitants in 2003, close on 50% of the provincial total and double that of the second largest town in the region, Talavera de la Reina (79,916 inhabitants), in the Province of Toledo. Nevertheless, further in-depth study is required into all the differential determinants that might possibly exist between these provinces.
The slight upward trend in maximum temperatures throughout the region from 1975 to 2003 was not significant, was not in evidence when ARIMA modelling of the daily data series was performed, and must, in the event, have been controlled for by the relevant differentiation, so that it cannot be regarded as a factor to be borne in mind.
In any case, and for practical purposes, the results obtained are important data for drawing up heat prevention plans put in place as a result of the heat wave that struck Europe during the summer of 2003 (Conti et al. 2005; Díaz et al. 2006; Le Tertre et al. 2006), since they point to a significant dynamism in the relationship between air temperature and mortality and, at the same time, indicate that this dynamism may not move in the same direction in different towns or regions.
Insofar as study limitations are concerned, it should be said that the failure to use standardized mortality rates prevents conclusions being drawn about trends in the comfort temperature to the exclusion of structural changes in the population, though this was not the aim of this study. Similarly, there were no air pollution data for such a large study area, nor any possibility of having these, since measuring stations are only located in important urban centres and these cannot represent the exposure of the regional population. In the adjacent Madrid Region, the influence of this factor on mortality has been documented (Alberdi Odriozola et al. 1998b). However, owing to the low density and dispersion of the population in Castile-La Mancha, a region having no urban or industrial centres, given towns can be presumed to exert very limited influence, without any ensuing repercussions on overall provincial mortality of a magnitude sufficient to cause any significant change in the relationship between temperature and mortality.
Conclusions
The decline in the maximum temperature of minimum mortality across the study period, as a consequence of a growing effect of heat on organic-cause mortality, may be attributable to the percentage growth in the most susceptible, i.e., the oldest, population segment. The differential pattern detected in the Province of Albacete calls for specific analysis.
The growing level of socio-economic development in Castile-La Mancha over the three decades, with a notable improvement in infrastructures of all types, served to prevent an even steeper rise in mortality, bearing in mind the percentage of the population above the age of 65 years, with the trend in the maximum comfort temperature having stabilized between the second and third decades, which could indicate a shift in the trend of the relationship.
In essence, this indicates that it would be advisable for established heat-prevention plans to be regularly reviewed, since the effects of heat on the population tend to vary at least every 10 years. Changing situations in the population structure, such as aging or intense migratory movements, can render preventive measures obsolescent. This underscores the specific nature of the dynamic relationship between temperature and mortality with respect to the geographic area studied, so that neither results nor conclusions can be extrapolated, not even between countries or regions having a similar level of socio-economic development. This goes to confirm the need to plan preventive measures subject to prior study and characterization of this relationship in appropriate territorial units, such as provinces in the case of Castile-La Mancha.
Forecasts issued by experts with respect to the increasing intensity of temperature extremes as a consequence of climate change, in the south of Europe in particular, reinforce the need for additional studies to be conducted in Castile-La Mancha, which will enable the relationship between ambient temperature and health indicators, especially in heat wave conditions, to be more precisely characterized.
References
Alberdi JC, Diaz J, Montero JC, Miron I (1998a) Daily mortality in Madrid community 1986–1992: relationship with meteorological variables. Eur J Epidemiol 14(6):571–578
Alberdi Odriozola JC, Diaz J, Montero Rubio JC, Miron IJ, Pajares Ortiz MS, Ribera RP (1998b) Air pollution and mortality in Madrid, Spain: a time-series analysis. Int Arch Occup Environ Health 71(8):543–549
Braga AL, Zanobetti A, Schwartz J (2001) The time course of weather-related deaths. Epidemiology 12(6):662–667
Bull GM (1980) The weather and deaths from pneumonia. Lancet Jun 28; 1(8183):1405–1408
Carder M, McNamee R, Beverland I, Elton R, Cohen GR, Boyd J et al (2005) The lagged effect of cold temperature and wind chill on cardiorespiratory mortality in Scotland. Occup Environ Med 62(10):702–710
Carson C, Hajat S, Armstrong B, Wilkinson P (2006) Declining vulnerability to temperature-related mortality in London over the 20th century. Am J Epidemiol 164(1):77–84
Conti S, Meli P, Minelli G, Solimini R, Toccaceli V, Vichi M et al (2005) Epidemiologic study of mortality during the Summer 2003 heat wave in Italy. Environ Res 98(3):390–399
Curriero FC, Heiner KS, Samet JM, Zeger SL, Strug L, Patz JA (2002) Temperature and mortality in 11 cities of the eastern United States. Am J Epidemiol 155(1):80–87
Davis RE, Knappenberger PC, Michaels PJ, Novicoff WM (2003a) Changing heat-related mortality in the United States. Environ Health Perspect 111(14):1712–1718
Davis RE, Knappenberger PC, Novicoff WM, Michaels PJ (2003b) Decadal changes in summer mortality in U.S. cities. Int J Biometeorol 47(3):166–175
De Castro M, Martín-Vide J, Alonso S (2005) El Clima de España: Pasado, Presente y Escenarios de Clima para el Siglo XXI. In: Moreno JM (eds). Evaluación Preliminar General de los Impactos en España por Efecto del Cambio Climático Misterio de Medio Ambiente, Madrid; Universidad de Castilla-La Mancha. Available in: http://www.mma.es/oecc and http://ecce.uclm.es
Diaz J, Garcia R, Velazquez de CF, Hernandez E, Lopez C, Otero A (2002a) Effects of extremely hot days on people older than 65 years in Seville (Spain) from 1986 to 1997. Int J Biometeorol 46(3):145–149
Diaz J, Jordan A, Garcia R, Lopez C, Alberdi JC, Hernandez E et al (2002b) Heat waves in Madrid 1986–1997: effects on the health of the elderly. Int Arch Occup Environ Health 75(3):163–170
Diaz J, Garcia-Herrera R, Trigo RM, Linares C, Valente MA, De Miguel JM et al (2006) The impact of the summer 2003 heat wave in Iberia: how should we measure it?. Int J Biometeorol 50(3):159–166
Douglas AS, Al-Sayer H, Rawles JM, Allan TM (1991) Seasonality of disease in Kuwait. Lancet 337(8754):1393–1397
El-Zein A, Tewtel-Salem M (2005) On the association between high temperature and mortality in warm climates. Sci Total Environ 343(1-3):273–275
El-Zein A, Tewtel-Salem M, Nehme G (2004) A time-series analysis of mortality and air temperature in Greater Beirut. Sci Total Environ 330(1–3):71–80
Enquselassie F, Dobson AJ, Alexander HM, Steele PL (1993) Seasons, temperature and coronary disease. Int J Epidemiol 22(4):632–636
Kan HD, Jia J, Chen BH (2003) Temperature and daily mortality in Shanghai: a time-series study. Biomed Environ Sci 16(2):133–139
Keatinge WR, Donaldson GC, Cordioli E, Martinelli M, Kunst AE, Mackenbach JP et al (2000) Heat related mortality in warm and cold regions of Europe: observational study. BMJ 321(7262):670–673
Kunst AE, Looman CW, Mackenbach JP (1993) Outdoor air temperature and mortality in The Netherlands: a time-series analysis. Am J Epidemiol 137(3):331–341
Le Tertre TA, Lefranc A, Eilstein D, Declercq C, Medina S, Blanchard M et al (2006) Impact of the 2003 heatwave on all-cause mortality in 9 French cities. Epidemiology 17(1):75–79
Michelozzi P, De SM, Accetta G, de’Donato F, Kirchmayer U, D’Ovidio M et al (2006) Temperature and summer mortality: geographical and temporal variations in four Italian cities. J Epidemiol Community Health 60(5):417–423
Ministerio de Sanidad y Consumo (2007) Plan Nacional de Actuaciones Preventivas de los efectos del exceso de temperaturas sobre la salud http://www.msc.es/ciudadanos/saludAmbLaboral/planAltasTemp/2007/home.htm
Miron IJ, Montero JC, Criado-Alvarez JJ, Gutierrez AG, Paredes BD, Mayoral AS et al (2006) [Treatment and temperature series study for use in public health. The case of Castilla-La Mancha, Spain]. Rev Esp Salud Publica 80(2):113–124
Montero Rubio JC, Miron IJ, Diaz J, Alberdi Odriozola JC (1997) [The effect of atmospheric variables on mortality due to respiratory and cardiovascular diseases in those over 65 in the Community of Madrid]. Gac Sanit 11(4):164–170
O’Neill MS, Zanobetti A, Schwartz J (2003) Modifiers of the temperature and mortality association in seven US cities. Am J Epidemiol 157(12):1074–1082
Pan WH, Li LA, Tsai MJ (1995) Temperature extremes and mortality from coronary heart disease and cerebral infarction in elderly Chinese. Lancet 345(8946):353–355
Pappas G, Queen S, Hadden W, Fisher G (1993) The increasing disparity in mortality between socioeconomic groups in the United States, 1960 and 1986. N Engl J Med 329(2):103–109
Prieto L, García Herrera R, Díaz J, Hernández E, Del Teso T (2004) Minimum extreme temperatures over Peninsular Spain. Global Planetary Change 44:59–71
Saez M, Sunyer J, Castellsague J, Murillo C, Anto JM (1995) Relationship between weather temperature and mortality: a time series analysis approach in Barcelona. Int J Epidemiol 24(3):576–582
Sakamoto-Momiyama M (1978) Changes in the seasonality of human mortality: a medico-geographical study. Soc Sci Med 12(1D):29–42
Stone RC (1989) Weather types at Brisbane, Queensland: an example of the use of principal components and cluster analysis. Int J Climatol 9:3–32
The Eurowinter Group (1997) Cold Exposure and winter from ischaemic heart disease, cerebrovascular disease, respiratory disease, and all causes in warm and cold regions of Europe. Lancet 349:1341–1346
White D, Richman M, Tarnal B (1991) Climate regionalization and rotation of principal component analysis. Int J Climatol 11:1–25
Acknowledegment
This study was funded by a grant from the Castile-La Mancha Preventive Medicine & Public Health Society, Castile-La Mancha Regional Health Authority (Dossier PI 22/2003).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Miron, I.J., Criado-Alvarez, J.J., Diaz, J. et al. Time trends in minimum mortality temperatures in Castile-La Mancha (Central Spain): 1975–2003. Int J Biometeorol 52, 291–299 (2008). https://doi.org/10.1007/s00484-007-0123-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-007-0123-6