
Abstract
Global environmental change, in particular climate change, will have adverse effects on public health. The increased frequency/intensity of heat waves is expected to increase heat-related mortality and illness. To quantify the climatic risks of heat-related mortality in Lisbon an empirical-statistical model was developed in Part I, based on the climate-mortality relationship of the summer months of 1980–1998. In Part II, scenarios of climate and population change are applied to the model to assess the potential impacts on public health in the 2020s and 2050s, in terms of crude heat-related mortality rates. Two regional climate models (RCMs) were used and different assumptions about seasonality, acclimatisation and the estimation of excess deaths were made in order to represent uncertainty explicitly. An exploratory Bayesian analysis was used to investigate the sensitivity of the result to input assumptions. Annual heat-related death rates are estimated to increase from between 5.4 and 6 (per 100,000) for 1980–1998 to between 5.8 and 15.1 for the 2020s. By the 2050s, the potential increase ranges from 7.3 to 35.6. The burden of deaths is decreased if acclimatisation is factored in. Through a Bayesian analysis it is shown that, for the tested variables, future heat-related mortality is most sensitive to the choice of RCM and least to the method of calculating the excess deaths.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Climate change is likely to have wide-ranging and adverse impacts on human health. An increased frequency or severity of heat waves would cause an increase in mortality and illness (McMichael et al. 2001). There are many studies relating climate and mortality, but few have used this knowledge to assess changes in heat-related mortality under climate change scenarios. Kalkstein and Green (1997) made predictions of heat-wave-related mortality for 44 U.S. cities on the basis of climate scenarios for the years 2020 and 2050 using an air-mass-based synoptic approach. Duncan et al. (1997) also followed the air mass approach, as well as a threshold temperature approach, to estimate heat-related mortality in ten Canadian cities under global warming scenarios. Guest et al. (1999) quantified the relationship between climatic extremes and mortality in the five largest Australian cities during the period 1979–1990 and then applied this relationship to scenarios for climate and demographic change, to predict potential impacts on mortality in the year 2030 (using temporal synoptic indices and non-linear regression methods). Donaldson et al. (2002) estimated the impact of climate change on temperature-related mortality for the UK, from the observed temperature-mortality relationship. While some of these studies show that, by the middle of the century, summer heat-related mortality could increase dramatically (Donaldson et al. 2002; Duncan et al. 1997; Kalkstein and Green 1997), others conclude that the expected changes in mortality would be minor (Guest et al. 1999). An overall problem with these studies is the absence of sensitivity analysis and the lack of an explicit representation of uncertainties.
The aim of this paper is to estimate the potential impact of climate change on heat-related mortality in the city of Lisbon. In Part I, an empirical-statistical model for heat stress was constructed for the summer months of the period 1980–1998 for the district of Lisbon. The model is based on the regression of an aggregate dose-response relationship between maximum temperature and excess heat-related deaths, i.e. the difference between observed and expected deaths. The model was validated using correlation and residual analysis (Dessai 2002). Part II of this work, which is described in this paper, applies the model developed in Part I to scenarios of future population and climate change to assess the potential impacts on public health. The sensitivity of future heat-related mortality to input assumptions is quantified by an exploratory Bayesian analysis.
Materials and methods
The construction and validation of the heat stress empirical-statistical model is described in Part I of this work (Dessai 2002) so here I will focus on the scenario-building exercise and its application.
Population scenarios
Population scenarios for Lisbon were constructed in line with the Intergovernmental Panel on Climate Change Special Report on Emission Scenarios (SRES; Nakićenović and Swart 2000). National projections were not used because they did not go far enough into the future. The OECD (developed countries) population growth rates from each SRES storyline (A1, A2, B1 and B2) was applied to the 1990 Lisbon population to produce 10-year spaced population figures until 2100. The median population from these calculations was used for simplicity.
Climate scenarios
The choice of climate change scenarios is important because it can determine the outcome of an analysis of the impacts of a climate change (Smith and Hulme 1998), such as this one. Regional climate prediction is still characterised by a considerable amount of uncertainty. Therefore, I use scenarios, rather than predictions, of climate change to identify the sensitivity, or vulnerability, of systems to climate change (Smith and Pitts 1997). A scenario provides a description of how the future may develop on the basis of a coherent and internally consistent set of assumptions about key social, economic and technological relationships and driving forces (e.g. rate of technology change, demography, prices, etc.).
There are several types of climate change scenarios, e.g. incremental, analogue (both temporal and spatial) and model-based scenarios. All the climate-mortality studies mentioned in the Introduction were based on outputs from general circulation models (GCMs) which, according to Mearns et al. (2001b), are the most advanced tools currently available for simulating the response of the global climate system to changing atmospheric composition. The spatial resolution of GCMs is generally low, a few hundred kilometers, which means that only two grid boxes represent the whole of Portugal. Even though heat waves may affect entire regions, some epidemiological studies can be criticised for using weather stations miles away from the area in which most deaths occur (Kilbourne 1997). The results of the typical resolution of a GCM, 250 × 250 km, would therefore be too coarse. In light of this, and owing to the recent development of regional climate modelling, I used results from high-resolution regional climate models (RCMs) that yield greater spatial detail (around 50 km; grid box 38.92N, 9.32W was used) about climate, but which are still constrained at their boundaries by the coarse-scale output from GCMs.
Results from two RCMs were used for this study: PROMES, from the Universidad Complutense de Madrid (Castro et al. 1993; Gallardo et al. 2001) and HadRM2, from the Hadley Centre (Jones et al. 1997; Noguer et al. 1998). RCMs are driven by boundary conditions extracted from GCM experiments, in this case the HadCM2 model (Johns et al. 1997) for both RCMs. We used results from two experiments performed with both RCMs: a control experiment (driven by results from the HadCM2 control or unforced experiment; 1 × CO2) and a future greenhouse-gas-forced experiment (2 × CO2). Output variables included minimum, maximum and average temperature. PROMES simulates two 10-year periods, one for 1 × CO2 (1981–1990), and another for 2 × CO2 (2040–2049). The HadRM2 control experiment simulates a 30-year period (2007–2036) nominally representing "current" climate conditions (pre-industrial atmospheric concentration levels of greenhouse gases) while the HadRM2 greenhouse-gas-forced experiment simulates a 20-year period (2080–2099) (Doherty et al. 2000). RCM evaluation (i.e. comparison between the RCM control run and climate observations) is not described here, but has been performed for the whole of Portugal elsewhere (cf. Miranda et al. 2002). It is important to note that HadRM2 showed better agreement with observations than PROMES.
A typical baseline climate for impact assessment covers 30 years of weather data (e.g. 1961–1990). In order to cover the period for which the model was constructed and validated (1980–1998) I chose the period 1969–1998 as our baseline climate for the purpose of scenario building. Future daily weather scenarios for maximum temperature were constructed by adding each year of the baseline climate (1969–1998) daily temperatures and 1 year of daily temperature anomalies (2 × CO2–1 × CO2) based on the RCMs outputs. This representative 365-day period of temperature anomalies was constructed by linearly interpolating the calculated average monthly anomaly of the 10- and 20-year period (depending on the RCM) in order to avoid step changes between months. This aggregation and disaggregation of data were necessary because the daily outputs from the RCMs were not deemed as reliable as the monthly outputs. Daily weather scenarios were thus produced for a 30-year period centred on the 2040s for PROMES and 2080s for HadRM2. We assumed that temperature change grows linearly throughout the century so, for PROMES, anomalies for the 2020s are half the 2040s values and anomalies for the 2080s are double. The same was done for HadRM2 on the basis of 2080s values. Though there were no more time slices available from the RCMs used in this study, the GCM that provided the boundary conditions for the RCMs did show a fairly linear warming for the Iberian Peninsula (cf. Miranda et al. 2002). By combining 30 years of observed climate data with changes in monthly means it is assumed that climate variability remains unchanged in the future. To my knowledge, daily weather scenarios from RCMs have never been applied to climate-mortality studies.
Assumptions about unknowns
A number of assumptions had to be made regarding numerous unknown factors because, in the future:
-
1.
Temperatures above 29 °C (the critical threshold above which heat-related deaths become discernible) have a higher frequency than in the period 1980–1998, and often occur outside summer.
-
2.
Temperatures will go well beyond previously experienced conditions where the dose-response relationship established in Part I is no longer proven valid.
-
3.
People will acclimatize/adapt to future climates.
To deal with these problems of epistemic uncertainty (i.e. incomplete knowledge of processes that influence events) a set of assumptions were made to provide, in my opinion, a wider picture of the possible impacts. With respect to point 1, the model constructed in Part I is only valid for summer months but, taking into account the possiblility that heat waves could extend their period outside summer in the future, I assumed the relationship holds outside summer (considered a high estimate and called hereafter year-round). I also only selected future summer daily temperatures to calculate future mortality. This was considered a low estimate and designated summer (June, July, August; JJA) hereafter. Year-round and summer (JJA) are part of the seasonality assumption.
As for the second point, I took two approaches. In the first approach, I allowed the extension of the dose-response curves into "unobserved" temperatures (i.e. temperatures outside the demonstrated range of the model for the period 1980–1998) assuming the association holds its characteristics for temperatures higher than those observed in Part I of this study (the highest observed temperature for the 1980–1998 period was 41.5 °C). This was considered a high estimate; however, a limit was set to avoid unrealistic results. We only considered valid future periods that contemplated less than 0.5 day/year of "unobserved" temperatures, i.e. in 30 years of future data there can only be 15 days over 41.5 °C or else this period is disregarded as far as this study is concerned. This is roughly saying that the heat model holds for an extra 2 °C outside its proven-valid range. In the second approach, which takes into account point 3 at the same time, I assumed that people will acclimatize/adapt to a warmer climate with time. In their study, Kalkstein and Green (1997) accounted for acclimatisation by using analogue cities, i.e. cities whose present climate approximates the estimated climate of a target city as expressed by the GCM (e.g. in the future New York's population will have St Louis's dose-response curve). However, heat waves are location- and/or population-specific, so I propose a new approach. This approach is centred on the possibility that people may acclimatize over long periods. It is known that initial physiological acclimatisation to hot environments can occur over a few days but complete acclimatisation may take several years (McMichael et al. 1996; Kovats 1999). "How many years?" is still an unanswered question owing to the lack of long-term studies on climate and human health. In this paper it was assumed that complete acclimatisation to an extra 1 °C (compared to the 1990s) is reached after three decades, making the dose-response relationship work from 30 to 42 °C in the 2020s, 31 to 43 °C in the 2050s, and 32 to 44 °C in the 2080s (as compared to 29 to 41 °C in the 1980–1998 period). This was called the acclimatisation assumption.
Using the model developed in Part I together with the results from two RCMs assumptions about seasonality (summer months or year-round) and acclimatisation (full or no), future heat-related mortality was estimated for the 2020s and the 2050s (the 2080s are also shown, but are not considered in this study). I used two different methods to calculate excess deaths (i.e. deaths beyond those expected for that period in that population) in order to represent uncertainty in the model constructed in Part I. The first approach, called the summer months mean, uses a fixed mean of daily mortality for each summer month, for the period 1980–1998. The second approach uses a 30-day running mean between mid-May and mid-September, but only the summer values are used.
Bayesian analysis
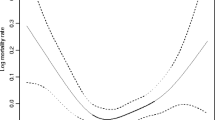
I used an exploratory Bayesian analysis to investigate the impact of input assumptions – about seasonality, acclimatisation, RCMs and the method of calculating excess deaths – on the resulting heat-related mortality. I only intend this to be illustrative, because I did not perform Monte Carlo sampling (cf. New and Hulme 2000; Jones and Page 2001). The Bayesian paradigm is a formal and rigorous language to communicate uncertainty (Moss and Schneider 2000). It involves the definition of prior probabilities for parameters of the model in question and the definition of posterior probabilities (or frequency) distribution of outcomes. In this paper, I represented the uncertainty of several parameters by taking two approaches to certain unknowns, e.g. two RCMs were used, two assumptions about acclimatisation (full or no) and seasonality (year-round or summer only), etc. As expected, the combination of different assumptions (e.g. full or no) for each parameter (e.g. acclimatisation) yields different mortality rates (as shown in Table 4). In order to represent uncertainties in terms of probability for the Bayesian analysis I converted the deterministic results (shown in Table 4) into probabilities. I used the values of mortality rate for each assumption as the tails of an arbitrary prior probability distribution function (PDF), either triangular or bimodal with a frequency of 1, as shown in Table 1. The middle values of the PDF (with a frequency of 0, 2 or 3) were estimated by interpolating between the mortality rates of the assumption being considered. For example, in simulation A, for HadRM2 and the summer-mean approach, three numbers were interpolated between the year-round and the summer mortality rates to construct the PDF. The same was done for acclimatisation where the values were estimated by interpolating between full and no acclimatisation mortality rates (Fig. 1). After interpolating the values, I multiplied the frequency distributions (shown in the table) together to find out how many times that number would be represented in the histogram that would be produced. For example, the middle value between year-round and summer (x 13, frequency of 3), and one of the extremes of the acclimatisation distribution (x 51, frequency of 1) would result in that number being repeated three times (3 × 1; this can be seen as simple matrixes calculations). In simulation A, this would be done twice for each of the methods of calculating excess deaths because of its bimodal distribution. This was done for each (prior) probability distribution in order to produce a histogram of the posterior probability. We ran four simulations, always changing the variables that were being compared. The sensitivity of the result to input PDFs was measured by the spread between the cumulative probability curves of the variables being compared, i.e. the bigger the spread, the higher the impact of that parameter on the resulting probabilities of heat-related mortality.

Results
The application of socio-economic scenarios is becoming increasingly important in climate impact assessment (Carter et al. 2001). With respect to population scenarios, Lisbon was shown to grow in all scenarios, reaching a maximum of 3.6 million (in SRES A2) and a minimum of 2.2 million (in SRES B2) by 2100 (Fig. 2). The middle-range scenarios all converged around 2.6 million. The median value was used in this modelling exercise for simplicity.

Lisbon population scenarios for each Special Report on Emission Scenarios (SRES) storyline (A1, A2, B1, B2) and the median value, 1990–2100
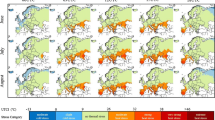
The climate scenario development exercise focuses on RCMs and the construction of daily weather scenarios. In order to produce these, each year of the 1969–1998 baseline climate was added to a daily temperature anomaly, which was linearly extracted from monthly mean anomalies (Fig. 3). Analysis of both RCMs, which were constrained at their boundaries by results from the same GCM (HadCM2; with a 1%/year increasing CO2 compound concentration and no sulfate aerosols), showed that PROMES predicts a slightly warmer climate than HadRM2 (Table 2). PROMES and HadRM2 represent slightly different future time-scales, but since the amount of overlap between the future 30-year periods is almost total, I only consider the years set out in Table 2, for simplification.

Daily maximum temperature change in HadRM2 and PROMES for the 2040s based on the linear interpolation between mean monthly maximum temperature anomalies (2 × CO2–1 × CO2)
There is a consistent increase in the number of extra days above the critical temperature (29 °C) in both RCMs when compared to the baseline climate (Table 3). Acclimatisation reduced the number of days above the critical temperature when either RCM was used, and in HadRM2 the 2050s even have fewer extra days than the 2020s with no acclimatisation. A substantial number of days with "unobserved" temperatures (above 0.5 day/year) is only reached by the 2080s (discarded values, crossed-out in the table). For the 2020s and the 2050s (and the 2080s in HadRM2 with full acclimatisation) year-round and summer simulations have the same number of days over 41.5 °C, which implies that "unobserved" temperatures only occur in summer, whereas in most of the 2080s these numbers are not identical, showing that some maximum temperatures over 41.5 °C are already occurring outside the summer period.
In Part I, the empirical-statistical model showed that annual heat-related mortality for the period 1980–1998 was between 5.4 and 6 (per 100,000 population) if respectively a 30-day running mean and a summer months mean approach is used to calculate excess deaths. Throughout this paper all death rates are crude parameters, i.e. they are not age-adjusted. The application of future population and climate change scenarios to the model showed a consistent increase in death rates under all assumptions (Table 4). At the very least, heat-related death rates are expected to increase to between 5.8 and 7.8 by the 2020s (compared to 5.4 in 1980–1998), in the most conservative approach, for each RCM used. At most, in the 2020s death rates could rise to between 11.6 and 15.1 for each RCM if there is no acclimatisation and if deaths occur all year round, on the basis of the summer-means approach (compared to 6 in 1980–1998). This modelling exercise shows a wide range of results for heat-related death rates for the 2020s, from a slight 7% increase to a more than doubling. Similar results are shown for the 2050s, where changes in the death rate, compared to the 1980–1998 period, range from a 35% increase to an almost sixfold increase. Most of the 2080s results are discarded because they refer to periods in which substantial "unobserved" temperatures occur. We have merely displayed the numbers to show how the model behaves unrealistically when the dose-response relationship is extended considerably outside its proven valid range. Clearly, depending on the model assumptions, a wide range of results is obtained, indicating significant uncertainties within the analytical framework.
An exploratory Bayesian analysis was conducted to explore the sensitivity of the effect of the prior probabilities described in Table 1, and exemplified in Fig. 1, on the resulting mortality rates. We ran four simulations (A, B, C, D) with arbitrary prior probabilities (Fig. 4). The sometimes non-normal shape of the probability curves is due to the lack of discrete numbers, because I only interpolated three additional values between the existing ones from Table 4. A Monte Carlo simulation, which would have randomly sampled the parameter space according to the pre-defined PDF would have produced more bell-shaped curves. By measuring the maximum distance between two cumulative probability curves in each graph, I conclude that future heat-related mortality is mostly sensitive to, in order of magnitude the RCMs acclimatisation/adaptation, seasonality, and lastly the method of estimating excess deaths.

Posterior probability and cumulative probability of death rates for different parameters (in the 2020s), when variables are sampled according to the prior distribution described in Table 1: A comparing regional climate models, B comparing methods to estimate excess deaths, C comparing acclimatisation versus no acclimatisation, and D comparing seasonality
Discussion
The population scenarios developed in this study were probably the simplest possible. Using the SRES storylines as a basis was intended to imply something about vulnerability and link it to the climate scenarios driven by the SRES emission scenarios. However, the median of the modelled values was used because, at the time, RCMs had not been run with all the SRES emission scenarios. This has the disadvantage of not exploring the uncertainties associated with population growth. Nonetheless, it is clear that heat-related mortality would be larger than (in the case of SRES A2), smaller than (in the case of SRES B1) or similar to (in the case of SRES A1 and B2) the results presented if all the population scenarios were used. With the continuous development of regional climate modelling, I expect to fulfil this objective in the future (cf. Hulme et al. 2002 who have presented results from a RCM linked to four SRES emission scenarios). Also under development are methodologies that characterise not only population but also socio-economic conditions in different scenarios (Moss 2003), which is important for assessing the impact on health. This study focused on all-age mortality, but it is a well-known fact that heat waves disproportionately affect the elderly, the young, people with pre-existing illnesses and low-income groups (Kilbourne 1997). Therefore, it is important to note that the majority of the heat-related deaths reported in this paper will occur in these vulnerable groups.
One of the novelties of this assessment of the impact of climate change was the use of RCMs in a health context. To my knowledge this had not yet been done except in other sectors such as agriculture (Mearns et al. 2001a), water resources (Kim et al. 2002) etc. I have not shown a comparison with GCMs because all GCMs are consistent in showing a temperature increase for Portugal, though the magnitudes are different (cf. Miranda et al. 2002). The greater regional detail of RCMs is a considerable advance on GCMs as its grid box matches the study area (district of Lisbon) almost perfectly. However, I would like to emphasise that greater precision does not necessarily imply greater accuracy. Further research into the representation of uncertainty in RCM experiments is necessary (cf. STARDEX 2002; PRUDENCE 2002). Furthermore, another complication arises from the fact that outdoor temperatures do not necessarily reflect the variable conditions within dwellings and other buildings where most deaths occur (Kilbourne 1997).
Constructing daily weather scenarios is by no means uncontroversial. In simply adding baseline climate to the mean monthly anomaly from the RCMs it was assumed there was no change in the shape of the frequency distribution of temperature, i.e. variability would remain constant; the distribution only shifted laterally. With increased variability the number of "unobserved" temperatures could have grown much larger, so the results could be underestimated. It is important to emphasise that the daily weather scenarios are different from observational data (though they are based on these) in that they are purely nominal. They are being used here to illustrate the potential impacts of climate change and should not be seen as representing "real" future daily weather, but plausible futures, i.e. scenarios. In order to derive more time slices (other than the original output of the RCMs) I assumed that temperature would change linearly throughout the century. This is a simplification of the real climate system, as ideally one ought to pattern-scale the output using a simple climate model (cf. Hulme et al. 2002). However, this shortcut is less problematic than the fact that by using only two RCMs I have sampled only a small part of the possible distribution of outcomes (at least with respect to climate). Many upstream uncertainties were not sampled, such as different GCMs different techniques to produce climate scenarios (e.g. weather generators, statistical downscaling, etc.), different greenhouse gas emission scenarios (e.g, SRES) and the unpredictability of the climate system. It is expected that more of these uncertainties will be included in future work, thus moving towards a more comprehensive risk-type framework that explicitly represents uncertainty in the assessment.
Modelling future heat-related deaths is not straightforward. It would be easy to use one method to calculate excess deaths, to use just one RCM, to assume no acclimatisation and only to consider summer deaths in the future. Such a single output of heat-related mortality could provide an illusion of certainty, but it would reveal nothing about uncertainty, a crucial factor in assessing the impact of climate on health that is so often neglected. In order to quantify some of this uncertainty, I decided to explore a number of assumptions and scenarios, which resulted in the wide range of results described in Table 4. The method of calculating excess deaths has already been discussed in Part I, but Table 4 makes it clear that the 30-day running mean is more conservative than the summer-months-mean approach to estimating heat-related deaths. An exception occurs when a substantial number of "unobserved" temperatures occur, as in the "no acclimatisation" scenario in the 2080s in both models and in the 2050s for PROMES. This is the result of expanding our dose-response relationship to temperatures way outside its proven valid range. Hence, the decision to ignore 2080s results.
In terms of seasonality, year-round heat-related mortality is on average 25% higher than the mortality of the summer months alone in both the 2020s and 2050s. The year-round heat-related mortality is likely to be an extreme case, but it should not be dismissed as an implausible scenario. Acclimatisation clearly reduces heat-related deaths under all scenarios. For the summer months mean approach, acclimatisation reduces deaths on average by 15% and 40% for the 2020s and 2050s respectively, while for the 30-day running mean approach acclimatisation reduces deaths by 32% and 54%. Populations in urban areas like Lisbon will probably adapt to future warmer climates in order to minimise heat-related deaths. A scenario of "no acclimatisation" is therefore an extreme case. However, the assumption that people will acclimatise to 1 °C per 30 years is simply illustrative. In order to shed ligh on this aspect of the assessment, there needs to be ground-breaking research on the past acclimatisation of populations to heat stress, which to my knowledge has never been performed anywhere because of the lack of long-term health and meteorological data.
We have to learn to quantify uncertainty and perform sensitivity analyses in the assessment of the impact of climate upon health (cf. Moss and Schneider 2000). Though my approach is far from comprehensive, Bayesian analysis is a good starting point from which to investigate the sensitivity of results to uncertainties in complex systems, such as the climate and human biology. Our simulations were purely exploratory, but they were intended to demonstrate the method's usefulness. The input variable that proved most sensitive in this exercise were the RCMs used. Sufficient to say that had other upstream uncertainties been included – such as the GCMs that constrained the RCMs boundaries, the emissions scenarios that were used for the GCM, etc. – the uncertainty range would probably be much bigger. The analysis also showed that the method of calculating excess deaths is the parameter that least changes the probability of heat-related mortality. This demonstrates that the uncertainties surrounding model development (Part I) are small and make relatively little difference to the end results when compared to the uncertainties introduced by the application of scenarios and assumptions (as in Part II).
Decision makers and public health officials are expected to take these results as plausible futures (remember that these are scenarios, not predictions) and use a bottom-up approach to the problem, i.e. how do I reach the acclimatisation scenarios described in this study? This inverts the problem, to question how we (as a society) can acheive an acclimatisation/adaptation of 1 °C per three decades in order to keep heat-related deaths at an acceptable level. I will not dwell here on an extensive list, but some known examples include the establishment of a heat wave early-warning system (which Lisbon has; cf. Nogueira et al. 1999), usage of air conditioners, improved ventilation of dwellings, appropriate communication to high-risk groups via the media, etc.
To the decision-maker of today these results might seem too distant in the future to warrant any action, and indeed, as pointed out by Sarewitz and Pielke (2000), the efforts to predict phenomena with complex, diffuse, and regional impacts such as global climate change have rarely contributed to the resolution of policy debates. Nonetheless, I believe this study illuminated, as explicitly as possible, the complexities involved in estimating the impacts of climate change on public health, and that an increased risk of heat-related mortality exists in the case of Lisbon even if the most conservative assumptions are made. Though cold-related mortality was not addressed in this study, it is possible that a climate change induced decrease in cold-related mortality could offset the increase in heat-related mortality; this hypothesis requires further investigation.
In summary, assuming a number of population and climate change scenarios, it has been shown that heat-related mortality will have increased consistently by the 2020s and the 2050s. If acclimatisation is taken into account this burden is decreased. A Bayesian analysis showed that heat-related mortality is mostly affected by the choice of RCM and least by the method of calculating excess deaths. The interaction between climate and human health needs further investigation, especially with respect to acclimatisation and adaptation to thermal stress. Knowledge gaps remain a problem in assessing the impact of climate on health, leading to endemic uncertainty that needs to be carefully quantified when one interprets the policy implications. Nevertheless, as in most areas of public policy formation, uncertainty remains a constant companion.
References
Carter TR, LaRovere EL, Jones RN, Leemans R, Mearns LO, Nakicenovic N, Pittock AB, Semenov SM, Skea J (2001) Developing and applying scenarios. In: McCarthy JJ, Canziani OF, Leary NA, Dokken DJ, White KS (eds) Climate change 2001: Impacts, adaptation, and vulnerability. Cambridge University Press, Cambridge, pp 145–190
Castro M, Fernandez C, Gaertner MA (1993) Description of a mesoscale atmospheric numerical model. In: Diaz JI, Lions JL (eds) Mathematics, climate and environment. Recherches en mathematics appliques. Series Mason, pp 227–251
Dessai S (2002) Heat stress and mortality in Lisbon. Part I. Model construction and validation. Int J Biometeorol 47:6–12
Doherty R, Hulme M, Lu X (2000) Interim UKCIP98 daily weather scenarios. http://www.cru.uea.ac.uk/∼mikeh/datasets/uk/maff75869/maff2000_data.htm
Donaldson G, Kovats RS, Keatinge WR, McMichael AJ (2002) Heat- and cold-related mortality and morbidity and climate change. In: Health effects of climate change in the UK. Department of Health, London pp 70–80
Duncan K, Guidotti T, Cheng W, Naidoo K, Gibson G, Kalkstein L, Sheridan S, Waltner-Toews D, MacEachern S, Last J (1997) Health sector. In: Canada Country Study: impacts and adaptation. Environment Canada, pp 520–580
Gallardo C, Arribas A, Prego JA, Gaertner MA, Castro M (2001) Multi-year simulations using a regional-climate model over the Iberian Peninsula: current climate and doubled CO2 scenario. Q J R Meteorol Soc 127:1659–1681
Guest CS, Willson K, Woodward A, Hennessy K, Kalkstein LS, Skinner C, McMichael AJ (1999) Climate and mortality in Australia: retrospective study, 1979–1990 and predicted impacts in five major cities. Clim Res 13:1–15
Hulme M, JenkinsGJ, Lu X, Turnpenny JR, Mitchell TD, Jones RG, Lowe J, Murphy JM, Hassell D, Boorman P, McDonald R, Hill S (2002) Climate change scenarios for the United Kingdom. The UKCIP02 scientific report. Tyndall Centre for Climate Change Research, School of Environmental Sciences, University of East Anglia, Norwich, UK
Johns TC, Carnell RE, Crossley JF, Gregory JM, Mitchell JFB, Senior CA, Tett SFB, Wood RA (1997) The second Hadley Centre coupled ocean–atmosphere GCM: model description, spinup and validation. Clim Dyn 13:103–134
Jones RG, Murphy JM, Noguer M, Keen AB (1997) Simulation of climate change over Europe using a nested regional climate mode II. Comparison of driving and regional model responses to a doubling of carbon dioxide. Q J R Meteorol Soc 123:265–292
Jones RN, Page CM (2001) Assessing the risk of climate change on the water resources of the Macquire catchment. In: Ghassemi F, Whetton P, Little R, Littleboy M (eds) Integrating models for natural resources management across disciplines, issues and scales. Modelling and Simulation Society of Australia and New Zealand, Canberra, pp 673–678
Kalkstein LS, Greene JS (1997) An evaluation of climate/mortality relationships in large U.S. cities and the possible impacts of a climate change. Environ Health Perspect 105:84–93
Kilbourne EM (1997) Heat waves and hot environments. In: Noji EJ (ed) The public health consequences of disasters. Oxford University Press, Oxford, pp 245–269
Kim J, Kim T-K, Arritt RW, Miller NL (2002) Impacts of increased atmospheric CO2 on the hydroclimate of the Western United States. J Clim 15:1926–1942
Kovats RS (1999) Climatic variability: daily temperature extreme. Commentary presented at Workshop 1. Health and climate variability in Masstricht, The Netherlands 24–26 September 1999. http://geog.queensu.ca/h_and_e/healthandenvir/workshop1.htm
McMichael AJ, Haines A, Slooff R, Kovats RS (eds) (1996) Climate change and human health: an assessment by a task group on behalf of the World Health Organization, the World Meteorological Organization and the United Nations Environment Programme, WHO, Geneva
McMichael AJ, Akhtar R, Carcavallo R, Gubler D, Haines A, Kovats RS, Martens P, Patz J, Sasaki A (2001) Human health. In: McCarthy JJ, Canziani OF, Leary NA, Dokken DJ, White KS (eds) Climate change 2001. Impacts, adaptation, and vulnerability. Cambridge University Press, Cambridge, pp 451–485
Mearns LO, Easterling W, Hays C, Marx D (2001a) Comparison of agricultural impacts of climate change calculated from high and low resolution climate change scenarios. Part I. The uncertainty due to spatial scale. Clim Change 51:131–172
Mearns LO, Hulme M, Carter TR, Leemans R, Lal M, Whetton P (2001b) Climate scenario development. In: Houghton JT, Ding Y, Griggs DJ, Noguer M, Linde PJ van der, Dai X, Maskell K, Johnson CA (eds) Climate change 2001: the scientific basis. Cambridge University Press, Cambridge, pp 734–768
Miranda P, Coelho FES, Tomé AR, Valente MA (2002) 20th century Portuguese climate and climate scenarios. In: Santos FD, Forbes K, Moita R (eds) Climate change in Portugal: scenarios, impacts and adaptation measures. Gradiva, Lisboa, pp 23–83
Moss R (2003) Developing socioeconomic scenarios for use in vulnerability and adaptation assessments. National Communications Support Programme. Global Environment Facility (in press)
Moss R, Schneider S (2000) Uncertainties. In: Pachauri R, Taniguchi T, Tanaka K (eds) Guidance papers on the cross cutting issues of the third assessment report of the IPCC. IPCC, Geneva, pp 33–51
Nakićenović N, Swart R (eds) (2000) Special report on emission scenarios. Cambridge University Press, Cambridge
New M, Hulme M (2000) Representing uncertainty in climate change scenarios: a Monte-Carlo approach. Integrated Assessment 1:203–214
Nogueira PJ, Nunes B, Dias CM, Falcão JM (1999) Um sistema de vigilância e alerta de ondas de calor com efeitos na mortalidade: o índice Ícaro. Rev Port Saúde Púb 1:67–77
Noguer M, Jones R, Murphy J (1998) Sources of systematic errors in the climatology of a regional climate model over Europe. Clim Dyn 14:691–712
PRUDENCE (2002) Prediction of regional scenarios and uncertainties for defining European climate change risks and effects. http://www.dmi.dk/f+u/klima/prudence/
Sarewitz D, Pielke RA Jr (2000) Prediction in science and policy. In: Sarewitz D, Pielke RA Jr, Byerly R Jr (eds) Prediction: science, decision-making, and the future of nature. Island Press, Washington, DC, pp 11–22
Smith JB, Hulme M (1998) Climate change scenarios. In: Feenstra J, Burton I, Smith JB, Tol RSJ (eds) Handbook on methods of climate change impacts assessment and adaptation strategies. Version 2.0 UNEP/IES, Amsterdam, pp 3-1, 3-37
Smith JB, Pitts GJ (1997) Regional climate change scenarios for vulnerability and adaptation assessments. Clim Change 36:3–21
STARDEX (2002) Statistical and regional dynamic downscaling of extremes for European regions. http://www.cru.uea.ac.uk/projects/stardex/
Acknowledgements
Part of this work was commissioned by the SIAM (Scenarios, Impacts and Adaptation Measures to climate change in Portugal) Project, which was funded by the Fundação Calouste Gulbenkian and the Fundação para a Ciência e a Tecnologia (FCT). The writing-up of this paper was supported by a grant (SFRH/BD/4901/2001) from FCT. Henrique Oliveira Pires and Fátima Espírito Santo of the Instituto de Meteorologia are thanked for supplying the baseline data. The HadRM2 data were supplied by the Climate Impacts LINK Project (DETR Contract EPG 1/1/68) on behalf of the Hadley Centre and U.K. Meteorological Office. Manuel Castro supplied the PROMES data to the SIAM Project. Mike Hulme and Xianfu Lu provided extensive advice on the usage of climate scenarios and Mike Hulme also advised on the drafting of the paper. I am particularly grateful to Elsa Casimiro and Filipe Duarte Santos for their encouragement and support throughout the project.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dessai, S. Heat stress and mortality in Lisbon Part II. An assessment of the potential impacts of climate change. Int J Biometeorol 48, 37–44 (2003). https://doi.org/10.1007/s00484-003-0180-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-003-0180-4