
Abstract
Background
End-stage renal disease (ESRD) in children is associated with impaired neurocognitive function and development. However, data on factors associated with neurocognitive dysfunctions in children with kidney transplants are limited.
Methods
We conducted a cross-sectional analysis comparing cognitive functions (using the Woodcock-Johnson International Edition, WJIE) in 35 kidney transplant and 35 healthy control children. Data on laboratory measurements, comorbidities, and social characteristics were collected.
Results
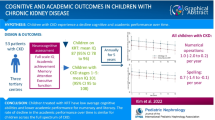
Transplant children had significantly worse scores on the intelligence quotient (IQ) test compared with controls [Full Scale IQ score 85 (26) vs 107 (10), p <0.001]. Lower maternal education level was significantly associated with lower WJIE cognitive test scores; however, no association was found between laboratory values and WJIE scores. Among children with kidney transplants, those with medical comorbid conditions had significantly lower Verbal Ability and Full Scale IQ scores. Earlier age of dialysis onset and a longer total time on dialysis (>9 months) were associated with lower test scores. Age-standardized duration of hospitalization was inversely correlated with IQ (r = −0.46, p <0.01) and was an independent significant predictor (Beta = −0.38, p = 0.02) of IQ scores in transplanted children.
Conclusions
Child kidney transplant recipients have neurocognitive function impairments that are associated with markers of socioeconomic status (SES) and factors related to disease severity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Children with end-stage renal disease (ESRD) are at increased risk for atypical neurocognitive development [1–3] accompanied by documented impairments of the central nervous system [4]. Recent studies have suggested that pediatric patients with chronic kidney disease (CKD) have lower intellectual functioning, deficits in executive functions, and problematic academic progress compared with normal controls or their sibling controls [5, 6]. However, studies from the 2000s indicate that neuropsychological outcomes for children with CKD are more favorable [mean intelligent quotient (IQ) within 1–2 standard deviations (SD) of the norm] than was detected in earlier reports [6–8].
In children with CKD, poor neurocognitive functions have been associated with anemia, hypertension, cardiovascular disease, malnutrition, seizures, earlier age of CKD onset, longer disease duration, and kidney disease staging [5, 6]. In addition, age at diagnosis and longer dialysis duration, as well as lower mother/caregiver's educational level, may play a role in neurocognitive performance of kidney transplant recipient children [1]. However, there are other risk factors that may contribute to poor cognitive function (e.g., perinatal problems, underlying disease, long anesthesia). ESRD in childhood may also impact adult neurocognitive function. Groothoff et al. reported that adults with ESRD who also had >4 years of cumulative dialysis in childhood had a 3.4-times higher chance of having IQ scores 1 SD below the mean of the corresponding general population [9].
The few studies that have examined the impact of kidney transplantation on cognitive functions in children have reported conflicting results regarding IQ differences between child transplant recipients and dialysis patients [1, 10, 11]. An early study by Fennell et al. showed that children with ESRD who received kidney transplants showed significant improvement in Full Scale and Performance IQ test scores 1 month after transplant compared with healthy matched control children [12]. Icard et al. also reported approximately a 12-point increase in intellectual functioning before and after transplantation; however, according to their study results, transplantation does not appear to normalize developmental or intellectual status in children with ESRD [10].
We designed a cross-sectional study to compare the intellectual function of Hungarian children with kidney transplants to age- and gender-matched healthy controls by using standard and validated questionnaires. We also assessed the predictors of IQ in the transplanted children. Based on our previous findings, we hypothesized that cognitive functions are lower in transplant children than their healthy counterparts and that earlier dialysis onset and longer dialysis duration are associated with lower intellectual abilities.
Methods
Patients and data collection
We collected data on all Hungarian children with a kidney transplant between 6 and 18 years of age (n = 40) who were regularly followed at the kidney transplant outpatient clinics of the First Department of Pediatrics and the Department of Transplantation and Surgery at the Semmelweis University, Budapest, between September 2007 and December 2008. Exclusion criteria were current acute rejection (within the last 4 weeks), hospitalization, and transplantation in the previous 3 months. The baseline assessment was conducted between September 2007 and December 2008 [as a part of the Psychosocial Problems and Cognition in Kidney Transplant Children (PPCKTC) Study]. In addition, the children’s parents were invited to participate personally. Parents of three (7 %) of the 40 eligible 40 children refused to participate, and an additional two (5 %) children were excluded (one transplanted within the previous 3 months and one who experienced acute rejection within 4 weeks prior to the study period). The control group was selected (1:1) by matching children from one elementary school and one high school in Budapest, Hungary, based on gender and age (maximum 1 month difference). Children with any chronic illness were ineligible for the control group. The final cohort consisted of 35 kidney transplant children and their parents and 35 healthy children and their parents.
Demographic data and details of medical history were collected at enrollment, and information on the transplant recipient’s use of immunosuppressive drugs was obtained. Estimated glomerular filtration rate (eGFR) was calculated using the Schwartz formula: eGFR (ml/min/1.73 m2) = k (height)/serum creatinine where k = 0.45 in term infants to 1 year of age and 0.55 in children to 13 years of age [13]. Two patients had a previous transplantation. We collected data on age at the time of first dialysis and cumulative time spent in the hospital over the course of their life. As an older child has a higher chance of having a longer lifetime hospitalization, we calculated the age-standardized duration of hospitalization as follows: cumulative lifetime length of hospitalization/age of the child. This variable was called the age-standardized duration of hospitalization. Bloodwork, laboratory data, information about social characteristics, and cognitive measurements were all obtained on the same day.
Laboratory data and comorbidity
Laboratory data were extracted from medical records and the electronic laboratory database of the hospital. The following laboratory parameters were tabulated: blood hemoglobin, serum creatinine, and serum albumin. We also collected information on the transplanted children’s comorbid conditions, such as diabetes, hypertension, osteoporosis, seizures, and other diseases, from their charts.
Immunosuppressive therapy
Standard maintenance immunosuppressive therapy generally consisted of prednisolone/methylprednisolone [either cyclosporine A microemulsion formulation (Neoral) (CsA) or tacrolimus combined with mycophenolate-mofetil (MMF)] or azathioprine, or sirolimus, or everolimus.
Social characteristics
Data on psychosocial parameters were obtained, and maternal education level was used as a marker of socioeconomic status (SES). A learning problem was an indicator, and parents were asked to report if their child had an official report of different types of learning problems (disorder/disability or other difficulties related with learning achievement), which was independent of performance for other markers of achievement. All official reports had been released by the Hungarian Official Board of Learning Disorders and Disabilities, the official government department.
Woodcock-Johnson Cognitive Ability Test – International Edition (WJIE)
The adapted and validated Standard Battery of the Hungarian version of Woodcock-Johnson Tests of Cognitive Abilities Revised (WJIE) was used in this study [14], which measures cognitive abilities in individuals between 2 and 90 years of age and provides a comprehensive system for measuring general intellectual ability, specific cognitive abilities, language skills, and academic achievement [15]. The battery consists of seven tests (verbal comprehension, visual/auditory learning, spatial relations, sound blending, concept formation, visual matching, and numbers reversed), each one selected to serve as an indicator of at least one of the broad Cattell-Horn-Carroll (CHC) cognitive abilities. CHC theory is the most comprehensive, consensual, and empirically supported psychometric theory of the structure of cognitive and academic human abilities and is an amalgamation of two similar theories: Gf-Gc (fluid and crystallized intelligence) and the three-stratum theory [first stratum represents narrow abilities, second broad abilities, and third general abilities (g factor)] [16]. The WJIE General Intellectual Ability scale or Full Scale Intellectual Abilities test can be reported as one overall score or broken down by its three parts: verbal ability, thinking ability, and cognitive efficiency [15]. All WJIE scores are standardized to a mean of 100 points and an SD of15; so accordingly, it can be compared with scores obtained on other IQ tests.
Learning and intellectual disabilities
Learning disability (LD) was defined by applying the ability–achievement discrepancy approach, as follows: an academic standard score at least 1 SD (15 points, i.e., 70–85 IQ points) lower than a standard score according to the accepted routine clinical practice [17]. For intellectual disability (ID), we used the definition and criteria provided in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV): profound mental retardation (MR) = IQ <35; severe MR = IQ 36 - 49; mild MR = IQ 50 - 69 points [18].
Statistical analysis
Statistical analyses were carried out using the IBM SPSS 20.0 software. Data were summarized using proportions, means (± (SD) or median [interquartile range, (IQR)], as appropriate. Continuous variables were compared using independent samples t test, Mann–Whitney U test, or one-way analysis of variance (ANOVA). Correlation analysis was performed using Pearson or Spearman correlation analysis, as appropriate. To explore potential differences between short/long duration of dialysis and intelligence, we divided the transplant group into two subgroups according to median dialysis duration. Linear regression analysis was used to determine the independent association between the presence of cognitive deficits (dependent variable) and the following variables: age of dialysis onset, age-standardized duration of hospitalization, and maternal education in transplant recipient children. We also performed linear regression analyses for Full Scale IQ (dependent variable) and the following predictors—being transplanted (vs. healthy) and maternal education—to assess the independent association between IQ and being transplanted. Multivariate models were constructed based on theoretical considerations. In all analyses, two-sided tests were used, and p values <0.05 were considered significant.
Results
Demographics and baseline characteristics of the sample
Table 1 shows the main characteristics of the 35 child kidney transplant recipients and 35 matched controls (Co). The cause of ESRD was autosomal recessive polycystic kidney disease (ARPKD) in eight (23 %) patients; kidney/urinary tract abnormalities in seven (20 %); chronic glomerulonephritis in four (11 %); congenital/hereditary kidney disease in three (9 %); chronic pyelonephritis/interstitial nephritis in two (6 %), and unknown in 11 (31 %); 60 % of transplant children had no known comorbidity. For the 14 patients with comorbidities, the prevalence of each comorbidity was hypertension (n = 6, 43 %); diabetes (n = 2, 14 %); osteoporosis (n = 1, 7 %); seizures (n = 1, 7 %). Fourteen percent of the patients had more than one transplant ,and 6 % (n = 2) received a kidney from a living donor. Every patient underwent kidney transplant at least 3 months prior to study initiation. Median length of ESRD duration was 40 (IQR: 57) months; median age at the beginning of dialysis treatment was 9 years; and a median of 10 years at first transplantation. Median duration of dialysis therapy was 9 months (IQR: 14), and duration between transplant and cognitive assessment was 28 months (IQR: 40). Four patients (12 %) had a blood hemoglobin level ≤115 g/L. At the time of enrolment, 40 % of patients were taking prednisolone or methylprednisolone, and none of them were on CsA therapy. The percentage of patients taking MMF was 69 % compared with 77 % taking tacrolimus and 3 % azathioprine. Expectedly, cumulative lifetime spent in the hospital was significantly different between groups, but the prevalence of learning problems was similar (Table 1).
Prevalence of cognitive deficits in transplant and control group
Transplant recipients reported significantly worse scores on all clusters of the WJIE compared with controls (Table 1). All subtest scores of both groups are shown in Table S1. Normal intellectual achievements (measured in IQ points) were shown in 100 % of control children and 60 % of transplant children, while another 17 % of transplant children were classified as having a learning disability (below average) and 23 % were considered intellectually disabled (mental retardation groups) (Table 2).
Correlates of intellectual achievements in transplant group
Sociodemographic parameters
We analyzed the correlation between children’s cognitive function and age, gender, and maternal education. Chronological age had no correlation with intellectual achievements except thinking ability (r = 0.36, p <0.05). In addition, there was no association between children’s cognitive function and gender of cause of ESRD. All parts of the WJIE cognitive test showed a direct linear relationship between higher maternal education level and higher patient test scores (Table 3). Notably, in the assessment of Full Scale Intellectual Ability, children with a mother who had an elementary school education or less had an average performance IQ score of 48 (±27), while their peers who had a mother with a higher education had an average IQ score of 105 (±16).
Laboratory data and comorbidity
None of the laboratory data (blood hemoglobin, serum creatinine, serum albumin) had significant correlations with intellectual performance scores. However, we found significant differences in between transplant children with and without comorbid conditions. Transplant children with comorbid conditions (such as diabetes, hypertension, osteoporosis, seizures, and other diseases) achieved significantly lower points in Verbal Ability (85 ± 30 vs. 105 ± 17, p = 0.01), Cognitive Efficiency (70 ± 23 vs 89 ± 24, p = 0.02), and Full Scale IQ scores (74 ± 28 vs. 92 ± 23, p = 0.03), but no differences were noted in Thinking Ability (79 ± 32 vs. 93 ± 23, p = 0.13).
Estimated GFR, dialysis, and hospitalization
Table 4 shows correlations of intellectual achievements with medical parameters in transplanted children. Estimated GFR did not correlate with any intellectual function tests; however, age of dialysis onset was positively correlated with all composite scores of intellectual achievements (Table 4). Children with longer age-standardized duration of hospitalization had significantly lower IQs than those who spent less time in hospital (r = −0.46, p <0.01). This correlation remained the same after taking into account patients’ age (older patients have higher chance to be hospitalized) in the age-standardized analyses (Table 4). Median time on dialysis for transplant children was 9 months. When we compared transplanted patients according to total time on dialysis (less or more than 9 months), children with a shorter dialysis duration showed higher test scores in all intellectual performance evaluations: Verbal Ability [109 (26) vs. 90 (49), p = 0.07)] Thinking Ability [99 (22) vs. 86 (46), p = 0.02)] Cognitive Efficiency [93 (22) vs. 79 (45), p = 0.01], and Full Scale Intellectual Abilities [99 (17) vs. 81 (53), p = 0.01].
Multivariate analysis
In our multivariate linear regression model (adjusted R 2 0.50), examining predictors of Full Scale IQ scores in transplant recipients, age-standardized duration of hospitalization (B = −63.47, Beta = −0.38, T = −2.39, p = 0.02), and maternal education (B = 8.92, Beta = 0.35, T = 2.25, p = 0.03) were significant predictors. Age of dialysis onset (B = 0.13, Beta = 0.11, T = 1.23, p = 0.23) showed no predictive role. We also assessed the independent association between IQ and being transplanted. Multivariate linear regression (adjusted R 2 0.38), examining predictors of Full Scale IQ (WJIE) scores in the entire population, being healthy (vs. transplanted) (Beta = 0.44, p <0.001), and having a higher level of maternal education (Beta = 0.41, p <0.001) were significant and independently associated with higher IQ scores.
Discussion
In this cross-sectional study, we found two important new findings: (1) kidney transplantation is an independent predictor of lower IQ score; (2) age-standardized duration of hospitalization may have a predictive role in general intellectual function in children. In addition, our study confirmed that age of dialysis onset, cumulative time on dialysis, and maternal education seem to be important factors of neurocognitive outcomes in children.
A relevant rate of transplant recipients had different learning problems. A few prior studies have shown that children with CKD or ESRD have a higher risk for grade retention and an increased risk for impairments on measures of academic skills and criteria for low school achievement [1, 2]. However, another study showed that children with ESRD compared with their sibling-matched controls showed no differences in the prevalence of learning difficulties (except in relation to motor skills) despite ESRD children having significantly lower IQ scores [8]. Compared with normal controls, clinically significant differences were detected in school functioning in CKD patients in the recently published landmark Chronic Kidney Disease in Children (CKiD) study [19], which reported that school quality of life diminished with age based on parental assessments [20]. Learning problems based on different neurodevelopmental disorders, therefore, probably have roots in the preceding periods of development.
Similar to results of studies on general intellectual functions of CKD patients in recent decades, in our study, transplant recipients, in comparison with normal controls, reported significantly lower intellectual achievements in all IQ test scales at the time of school age [2, 11], showing best performances in verbal abilities, while their most problematic area was cognitive efficiency, which was evaluated by sampling two different factors of automatic cognitive processing: processing speed and short-term memory. Most transplant patients belonged to the normal IQ range, but 40 % showed impaired intellectual functioning. These findings coincide with international reports of IQ measures in children with CKD [11, 19].
In our transplant group, maternal education was a very strong predictor of general intellectual skills. The association of maternal education with children’s IQ in the general population is well known [21]. However, maternal education may play an even more important role for intellectual development in children with chronic illnesses such as ESRD. Previous studies have shown that maternal education is strongly correlated with factors related to ESRD history and management, such as age of dialysis onset and period of dialysis time [1, 22]. In our study, cumulative dialysis duration and maternal education were the significant medical and social factors associated with IQ scores. Although, dialysis factors showed no direct predictive role for cognitive function in the Brouhard et al. study [1], maternal influences that can impact cumulative dialysis duration may still play a role. Based on these findings, we assume that parents’ education level and the role of parental advocacy could probably influence long-term outcomes of neurocognitive functions in the mentioned population, because for children with chronic conditions, parents with better circumstances (higher level of education and higher income) might articulate stronger effects on their own child’s successful health care [23]. However, this question is multifactorial and probably needs to be addressed in further studies.
We found a lack of association between laboratory data such as eGFR, blood hemoglobin, serum creatinine, and albumin with intellectual skills. These results are in contrast with the findings of Duquette et al., who found associations between renal function and intellectual function in CKD children [2]. Conversely, other studies of long-term neurocognitive outcomes in ESRD children found questionable associations between kidney function and intellectual skills [3]. There are a couple of potential explanations for the discrepant results seen in our study and that of Duquette et al. First, our cohort consisted of kidney transplant recipients, while Duquette et al. examined CKD patients. Since all studies (including ours) used cross-sectional baseline laboratory data and no time-dependent analysis was done, there has been no way to evaluate the association between progressive kidney function decline with change in intellectual functioning. Furthermore, since we are uncertain how kidney function abnormalities were treated in Duquette’s study cohort, it is unknown what effect these factors may have had on examined associations.
In our cohort of Hungarian transplant children, more time spent on dialysis and earlier onset of ESRD (or age of dialysis initiation) were associated with lower IQ scores, which is consistent with findings in previous studies [1, 3, 11]. One of the new findings of our study was the association between cumulative time spent in the hospital and IQ scores. A longer hospitalization record was strongly associated with lower IQ. In our multivariate model of 35 transplant children, age-standardized duration of hospitalization was the independent and significant predictor of general intellectual functions. According to results of Gulleroglu et al., CKD children missed school much more frequently than their siblings, and time missed from school interfered with their academic achievements [22]. Moreover, it is known from earlier psychological literature in the general population that hospitalizations have powerful influences on delayed development of children [24]. This finding of the effect of hospitalization duration on neurocognitive function in transplant children may be important and relevant to clinical practice, as it may be a modifiable factor. However, it is unknown whether intervention aimed at shorter hospitalization has any impact for further neurocognitive development. Future well-designed studies are needed to answer this clinically relevant question.
There are a number of limitations of our study, which need to be discussed. First, our sample size is limited, which may lead to type II errors. However, the 35 transplant recipients in represent the majority of the Hungarian child transplant population. Second, intellectual function was assessed based only on IQ using the new Hungarian version of the Woodcock; however, other methods such as relevant executive functions (memory, attention, visual–spatial abilities), and language could have been used [11]. At the time this study was conducted, the new validated Hungarian version of the Wechsler test was not yet available. Third, we did not collect standardized scores, such as Charlson Comorbidity Index, to assess patient comorbidity. Fourth, we did not have data about patients’ academic scores. Finally, we could not analyze the association of intellectual function with perinatal events [25], effect of immunosuppressive therapy [26], and perioperative events, such as type of anesthesia during transplantation [27]. Also, we had no information regarding central nervous system imaging and the prematurity status of these patients.
Conclusions
Here we show the results of a cross-sectional study of kidney transplanted children and their healthy age- and gender-matched counterparts. We found that age of dialysis onset, cumulative time on dialysis, maternal education, and a new potentially modifiable factor—age-standardized duration of hospitalization—were predictors of neurocognitive outcomes in children. Further well-designed, larger, multicenter studies are needed to examine whether shortened hospitalization duration may improve intellectual and executive skill development in kidney transplant recipient children.
References
Brouhard BH, Donaldson LA, Lawry KW, McGowan KRB, Drotar D, Davis I, Rose S, Cohn RA, Tejani A (2000) Cognitive functioning in children on dialysis and post-transplantation. Pediatr Transplant 4:261–267
Duquette PJ, Hooper SR, Wetherington CE, Icard PF, Gipson DS (2007) Brief report: intellectual and academic functioning in pediatric chronic kidney disease. J Pediatr Psychol 32:1011–1017
Johnson RJ, Warady B (2013) Long-term neurocognitive outcomes of patients with end-stage renal disease during infancy. Pediatr Nephrol 28:1283–1291
Gipson DS, Duquette PJ, Icard PF, Hooper SR (2007) The central nervous system in childhood chronic kidney disease. Pediatr Nephrol 22:1703–1710
Gipson DS, Hooper SR, Duquette PJ, Wetherington CE, Stellwagen KK, Jenkins TL, Ferris ME (2006) Memory and executive functions in pediatric chronic kidney disease. Child Neuropsychol 12:391–405
Slickers J, Duquette PJ, Hooper SR, Gipson DS (2007) Clinical predictors of neurocognitive deficits in children with chronic kidney disease. Pediatr Nephrol 22:565–572
Madden SJ, Ledermann SE, Guerrero-Blanco M, Bruce M, Trompeter RS (2003) Cognitive and psychosocial outcome of infants dialysed in infancy. Child Care Health Dev 29:55–61
Bawden HN, Acott P, Carter J, Lirenman D, MacDonald GW, McAllister M, McDonnell MC, Shea S, Crocker J (2004) Neuropsychological functioning in end-stage renal disease. Arch Dis Child 89:644–647
Groothoff JW, Grootenhuis M, Dommerholt A, Gruppen MP, Offringa M, Heymans HS (2002) Impaired cognition and schooling in adults with end stage renal disease since childhood. Arch Dis Child 87:380–385
Icard P, Hooper SR, Gipson DS, Ferris ME (2010) Cognitive improvement in children with CKD after transplant. Pediatr Transplant 14:887–890
Gerson AC, Butler R, Moxey-Mims M, Wentz A, Shinnar S, Lande MB, Mendley SR, Warady BA, Furth SL, Hooper SR (2006) Neurocognitive outcomes in children with chronic kidney disease: current findings and contemporary endeavors. Ment Retard Dev Disabil Res Rev 12:208–215
Fennell RS 3rd, Rasbury WC, Fennell EB, Morris MK (1984) Effects of kidney transplantation on cognitive preformance in pediatric population. Pediatrics 74:273–278
Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A (1976) A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics 58:259–263
Ruef M, Furman A, Munoz-Sandoval A (2003) Woodcock–Johnson nemzetközi kiadás. Vizsgálatvezetői kézikönyv magyar kiadás. The Woodcock Muñoz Foundation, Nashville
Schrank FA, McGrew KS, Woodcock RW (2001) Technical Manual. Woodcock-Johnson III, Itasca, Illinois, USA
Gregory R (2011) Psychological testing: history, principles, and applications, 6th edn. Allyn & Bacon, Boston
Fletcher JM, Denton C, Francis DJ (2005) Validity of alternative approaches for the identification of learning disabilities: Operationalizing unexpected underachievement. J Learn Disabil 38:545–552
American Psychiatric Association (1994) Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR
Copelovitch L, Warady BA, Furth SL (2011) Insights from the chronic kidney disease in children (CKiD) study. Clin J Am Nephrol 6:2047–2053
Gerson AC, Wentz A, Abraham AG, Mendley SR, Hooper SR, Butler RW, Gipson DS, Lande MB, Shinnar S, Moxey-Mims M, Warady BA, Furth SL (2010) Health-related quality of life of children with mild to moderate chronic kidney disease. Pediatrics 125:e349–e357
Carneiro P, Meghir C, Parey M (2013) Maternal education, home environments, and the development of children and adolescents. J Euro Econ Assoc 11:123–160
Gulleroglu K, Baskin E, Bayrakci US, Aydogan M, Alehan F, Kantar A, Karakayali F, Moray G, Haberal M (2013) Neurocognitive functions in pediatric renal transplant recipients. Transplant Proc 45:3511–3513
Grant R, Brito A (2010) Chronic Illness and School Performance: A Literature Review New York: Children’s Health Fund
van der Horst FC, van der Veer R (2008) Loneliness in Infancy: Harry Harlow, John Bowlby and Issues of Separation. Integr Psych Behav 42325–335
van Handel M, Swaab H, de Vries LS, Jongmans MJ (2007) Long-term cognitive and behavioral consequences of neonatal encephalopathy following perinatal asphyxia: a review. Eur J Pediatr 166:645–654
Martínez-Sanchis S, Bernal MC, Montagud JV, Candela G, Crespo J, Sancho A, Pallardó LM (2011) Effects of immunosuppressive drugs on the cognitive functioning of renal transplant recipients: a pilot study. J Clin Exp Neuropsychol 33:1016–1024
Backeljauw B, Holland SK, Altaye M, Loepke AW (2015) Cognition and brain structure following early childhood surgery with anesthesia. Pediatrics 136:e1–e12
Acknowledgments
The authors thank the patients and staff in the First Department of Pediatrics and the Department of Transplantation and Surgery, Semmelweis University, Budapest, Hungary, for helping this survey.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Funding
This study was supported by grant from Hungarian Kidney Foundation, the Eötvös Loránd University Normative Research Fund (No: 364.833.002), the Foundation for Prevention in Medicine and Hungarian National Scientific Research Foundation (No: OTKA K108688 and No: OTKA 100909), and by the János Bolyai Research Scholarship of the Hungarian Academy of Sciences.
Ethical permission
This study has been approved by the Ethics Committee of Semmelweis University (TUKEB number: 165/2007). Before enrollment, all patients and their parents received detailed written and verbal information regarding the aims and protocol of the study, and parents were required to provide a signed informed consent.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Table S1
Scores of WJIE subtests in transplant and control groups (n = 70) (DOCX 12 kb)
Rights and permissions
About this article

Cite this article
Molnar-Varga, M., Novak, M., Szabo, A.J. et al. Neurocognitive functions of pediatric kidney transplant recipients. Pediatr Nephrol 31, 1531–1538 (2016). https://doi.org/10.1007/s00467-016-3380-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-016-3380-y