
Abstract
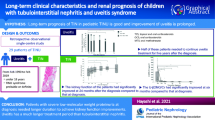
Tubulointerstitial nephritis and uveitis (TINU) syndrome is considered to have a good prognosis even without any immunosuppressive therapy, although there is no histological evidence to support this. The objective of this study was to evaluate, retrospectively, serial renal biopsy findings in three girls with TINU syndrome who were treated with prednisolone. At presentation, all patients had significantly elevated urinary β2-microglobulin levels (7583–19,313 μg/l) and high serum creatinine levels (0.93–1.3 mg/dl). The elevated β2-MG and creatinine levels persisted for 1 month, and renal biopsies were performed to establish a definitive diagnosis. The initial biopsy specimens of all patients revealed marked interstitial enlargement consisting of infiltration of lymphocytes; there was also notable tubulitis and infiltration of eosinophils. All patients received prednisolone therapy following the diagnosis. A second renal biopsy was performed 9 months after the first biopsy for two of three patients, and 2 years later for the third patient. The biopsy specimens taken at 9 months still showed histological changes of acute inflammation; in contrast, that taken at 2 years showed a lower degree of acute inflammation, but scar formation was observed in some regions. Based on these results, we conclude that selected TINU syndrome patients require some immunosuppressive therapy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Tubulointerstitial nephritis and uveitis (TINU) syndrome is characterized by the association of acute tubulointerstitial nephritis with uveitis. It was first described by Dobrin et al. in 1975 [1], and more than 200 cases have since been reported [2] in the pediatric and ophthalmologic literature. The prognosis of the renal symptoms observed in the TINU syndrome is currently regarded as good without systemic steroid therapy [3–5], although only a few reports have described the sequential renal histological changes that occur in TINU syndrome [6, 7], and the natural history and clinical course of the syndrome are still unclear. Moreover, there has been recent reports of the development of end-stage renal failure in patients with TINU syndrome not treated with systemic steroid therapy [8–10].
We recently treated three patients with TINU syndrome with systemic steroid therapy and performed two renal biopsies in each patient. The objective of the study was to evaluate, retrospectively, serial renal biopsy findings in three girls with TINU syndrome who were treated with prednisolone and to confirm the necessity for immunosuppressive therapy in selected TINU syndrome patients.
Patients and methods
Patients
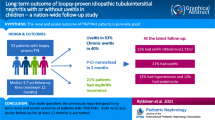
This was a retrospective review of patients with TINU syndrome diagnosed at our institution from 1998 to 2005. Five patients with TINU syndrome were treated during this period. Patients who had serial renal biopsies and were treated with oral steroid therapy were included in this study; three girls, all aged 14–15 years, fulfilled these criteria.
All patients showed low-grade proteinuria and glucosuria on screening tests with dip-and-read reagent strips, including school urinary screening. Blood tests, intensive urine tests, such as urinary β2-microglobulin (β2-MG) and electrolytes, and screening for ocular disease were then performed. The diagnosis of uveitis was made with a slit-lamp examination. If a patient showed any symptoms suggesting acute tubulointerstitial nephritis (ATIN) and was diagnosed with uveitis, the patient was diagnosed as having TINU syndrome clinically, and follow-up was started. Urinary β2-MG and serum creatinine levels were checked once or twice a month. Ocular symptoms were also followed with slit-lamp examinations once or twice a month. Renal biopsies were performed in all patients to make a definitive diagnosis after 1 month of follow-up if they still showed any symptoms suggesting ATIN and/or renal impairment, such as high urinary β2-MG and/or high serum creatinine levels. The second renal biopsies were performed either 9 months (patients 1 and 2) or 2 years (patient 3) after the first biopsy. All patients provided their written informed consent for each renal biopsy. None of the patients complained of rash, arthralgia, or morning finger stiffness, and none of the patients had an abnormal anti-nuclear antibody titer.
Histological examination
Biopsy specimens were treated by the standard paraformaldehyde fixation protocol for histological staining, and some specimens were used for CD4 and CD8 immunostaining. Tissue injury was assessed by hematoxylin–eosin staining, periodic acid–Schiff staining, periodic acid–methenamine silver staining, and Masson’s trichrome staining. Paraformaldehyde-fixed samples for CD4 and CD8 staining were dipped in 0.01 M citrate buffer pH 7.0 and pH 6.0, respectively, and autoclaved for 20 min at 121°C. An enzyme immunohistochemical peroxidase staining assay was then performed using monoclonal antibodies to detect CD4 and CD8 (Nichirei, Tokyo, Japan).
Grading of histological changes
Tubulointerstitial damage was assessed according to the tubulointerstitial score (TI score) described by Foster et al. [11]. The usefulness of this score was confirmed by Suzuki et al. [7]. Briefly, the percentage involvement of interstitial mononuclear infiltrate (factor 1, acute score), percentage lesion with interstitial edema (factor 2, acute score), tubular damage (factor 3, acute score), and interstitial fibrosis and tubular atrophy (factor 4, chronicity score) were scored. Absence was assigned a score of 0, <50% lesion involvement was assigned a score of 1, and >50% involvement was assigned a score of 2; thus, the total score ranged from 0 to 8.
Therapy
All patients were treated with oral prednisolone, although the protocol differed for each patient, as shown in Fig. 1. The steroid therapy was started at a dose of 40 mg/day (30 mg/m2) of prednisolone for patient 1 and 60 mg/day (60 mg/m2 or the maximum dose of our protocol) for patients 2 and 3 for 4 weeks. After the initial 4 weeks of therapy, the dose of prednisolone was tapered by 10 mg/week (patients 1 and 3) and 5 mg/week (patient 2). The dose of prednisolone, the duration of therapy, and the method of administration (every day or alternate days) were decided upon according to the urinary β2-MG titers and/or the results of the second renal biopsy.

Summary of the clinical courses of the three cases. Solid line β2-microglobulin (β2-MG) value, dotted line maximum normal value of β2-MG (250 μg/l), black bars, dose of oral prednisolone, arrow (↑) timing of renal biopsy (RB) or end of therapy, RB renal biopsy, qd quaque die (daily), qod quaque (every other day)
Results
Clinical manifestations
The patients’ profiles and their initial TINU syndrome symptoms are summarized in Table 1. Urinary β2-MG and serum creatinine levels at the time of the first examination were 15,400 μg/l and 1.3 mg/dl (115 μmol/l) in patient 1, 7583 μg/l and 0.93 mg/dl (82 μmol/l) in patient 2, and 19,313 μg/l and 1.1 mg/dl (97 μmol/l) in patient 3. The blood pressure of patients 1, 2, and 3 was 126/70 mmHg, 110/62 mmHg and 106/56 mmHg, respectively. The changes in these values are presented below. The high β2-MG levels and glucosuria suggested ATIN, and the high serum creatinine levels suggested renal impairment. Immunoglobulin (Ig)G levels were elevated in patients 1 and 2, as previously described in several reports [12].
Urinary β2-MG and serum creatinine levels
The urinary β2-MG and serum creatinine levels decreased in all three patients within 1 month of being started on oral steroid therapy: to 749 μg/l and 0.9 mg/dl (80 μmol/l) in patient 1; 147 μg/l and 0.82 mg/dl (72 μmol/l) in patient 2; 118 μg/l and 0.7 mg/dl (62 μmol/l) in patient 3. The blood pressure of patients 1, 2, and 3 also decreased to 114/66 mmHg, 106/58 mmHg and 102/54 mmHg, respectively. Elevated urinary β2-MG levels after the initiation of steroid therapy were observed in two patients (patients 1 and 3; Fig. 1). The starting dose of prednisolone was lower in patient 1 (30 mg/m2) than in the other two patients, and the dose of prednisolone was tapered faster in patient 3 (10 mg/week) than in patient 2. On the other hand, patient 2, in whom the initial prednisolone dose (60 mg/m2) was higher and the dose tapered more slowly (5 mg/week), did not have such elevated urinary β2-MG levels. The total cumulative prednisolone dose was 5.0 g for patient 1, 5.8 g for patient 2, and 9.0 g for patient 3.
Uveitis
All three patients were diagnosed as having bilateral anterior uveitis and were followed by an ophthalmologist. Their symptoms resolved with topical corticosteroid therapy. During oral steroid therapy, none of the patients complained of ocular symptoms, and reducing the prednisolone dose did not induce recurrence of uveitis within the 2-year follow-up period.
Histological changes
The initial biopsy specimens of all patients showed marked interstitial enlargement consisting of an infiltration of lymphocytes; there was also notable tubulitis and infiltration of eosinophils. Neutrophils were rare, and the glomeruli were within the normal range. Immunofluorescent staining showed no evidence of immune complex deposition, and electron microscopy also showed no electron-dense deposits. The TI scores of patients 1, 2 and 3 were 7, 6 and 7, respectively. The chronicity scores of all patients were 1, and, in patient 2, the factor 2 score was 1. The second biopsy specimens of patients 1 and 2 (shown in Fig. 2a and b), taken 9 months after the first biopsy, continued to show histological changes of acute tubulointerstitial nephritis with mononuclear cell infiltration (CD4 dominant; data not shown) and edematous regions. Interstitial fibrosis and tubular atrophy were also observed. Foci of granulomatous inflammation and collapsed glomeruli with peri-capsular fibrosis, which would ultimately form scars, were also noted in patient 1. The specimen of patient 3, which was taken 2 years after the first biopsy (Fig. 2c), showed a lower degree of infiltration of inflammatory cells in interstitial regions and almost normal tubules, but scar formation was observed in some regions. With respect to infiltrating lymphocytes, there were more CD4-positive cells than CD8-positive cells (Fig. 3), as has previously been reported [6].

Findings of the second renal biopsy. All tissue samples were treated with Masson’s trichrome stain. Magnification: ×100. a, b Biopsy findings of patients 1 and 2, respectively, 9 months after the first biopsy, showing tubular atrophy ( ) and interstitial fibrosis (
) and interstitial fibrosis ( ) indicating chronicity, but also infiltrating lymphocytes and edematous regions (
) indicating chronicity, but also infiltrating lymphocytes and edematous regions ( ) indicating acuteness. The collapsed glomeruli (
) indicating acuteness. The collapsed glomeruli ( ) and the granulomatous region (
) and the granulomatous region ( ) present will ultimately form scars. c Biopsy findings of patient 3, 2 years after the first biopsy, showing almost complete amelioration, although some scar formation is visible (
) present will ultimately form scars. c Biopsy findings of patient 3, 2 years after the first biopsy, showing almost complete amelioration, although some scar formation is visible ( )
)

CD4 and CD8 expression on interstitial lymphocytes of the first renal biopsy of patient 1. Magnification: ×100. CD4 expression is more prominent than CD8 expression. Similar results were observed in the other two patients
Discussion
The prognosis of TINU syndrome is currently considered to be good without systemic steroid therapy [3–5]. However, two of the patients in this study still had histological evidence of acute tubulointerstitial inflammation 9 months after the initiation of therapy, and the third patient improved with scar formation after systemic steroid therapy. It would therefore appear that some patients with TINU syndrome develop chronic renal damage.
Systemic steroid therapy was considered to be effective in our patients because their serum creatinine values recovered smoothly following the initiation of therapy, as has been previously reported [13]. Despite the patients showing a reduction in serum creatinine levels, examination of renal biopsy specimens obtained 9 months after therapy initiation revealed active lesions of tubulointerstitial nephritis, and the specimen obtained at 2 years showed healing with scar formation. Many of the studies published on the clinical course of TINU syndrome report that the prognosis for patients’ renal function is favorable without systemic steroid therapy [3–5]. However, there have been a number of reports of TINU patients who developed end-stage renal failure [8–10]. Given the results of our patients, it is important to recognize that some patients with TINU syndrome heal with scar formation and, thus, their reserve renal functional capacity is decreased.
Elevated urinary β2-MG levels were observed after a small initial amount of steroid therapy or rapid tapering of the steroid dose in patients 1 and 3. Patient 2, however, whose initial therapy consisted of a large dose (60 mg/m2) of prednisolone for 4 weeks, followed by slow tapering of the prednisolone dose, did not show such an elevation. Vohra et al. [8] and Kobayashi et al. [14] reported that TINU patients tend to have a prolonged clinical course. The biopsy findings at 9 months still showed acute inflammation and thus confirm their reports. In our opinion, selected TINU syndrome patients may need treatment with some anti-inflammatory drugs and long-term therapy.
Our three patients formed, or one can assume that they formed, scar lesions, even after treatment with prednisolone. Although systemic steroid therapy appears to be effective, it is not known whether steroid therapy is a sufficient treatment for TINU syndrome. Thus, immunosuppressive agents other than prednisolone may be necessary. Mycophenolate mofetil has recently been reported to be a useful agent for the uveitis of TINU syndrome [15]. The establishment of evidence-based therapies is needed in the future.
Not all patients need systemic steroid (or other immunosuppressant) therapy, as many reports have concluded. We have also cared for a girl with TINU syndrome whose renal symptoms improved within a few weeks of follow-up without any therapy (data not presented). Suzuki et al. [7] used the TI score described by Foster et al. [11] to quantify the renal biopsy findings of their TINU patients and concluded that TINU patients with high TI scores should be treated with immunosuppressive therapy. All three patients in our study had high TI scores (6 or 7). It would therefore appear that the TI score is an important indicator of the need for systemic therapy.
Another factor that may indicate the need for some immunosuppressive therapy is renal function at the first visit and the duration of renal dysfunction. Our three patients showed elevated serum creatinine and urinary β2-MG levels at their first visit to our hospital, and this elevation continued for more than 1 month before oral prednisolone therapy was started. Many of the patients reported by Takemura et al. [5] recovered within 1 month without systemic therapy. In addition, Hamdan et al. [10] reported that delayed diagnosis and initiation of treatment make the outcome of patients with TINU less favorable. We suggest that renal biopsy should be performed for TINU patients who show renal dysfunction for more than 1 month, and the treatment strategy should be determined according to the histological findings.
The pathophysiology of TINU syndrome is assumed to differ from that of other types of ATIN. In our three patients with TINU syndrome, interstitial infiltrating mononuclear cells prominently expressed CD4, as has been reported elsewhere [6, 16]. In contrast, in ATIN of other etiologies, the infiltrating cells usually predominantly express CD8 [17, 18]. Clinically, TINU syndrome has a prolonged course compared with other types of ATIN [8, 14]. In addition, it has recently been reported that a patient with TINU syndrome produced autoantibodies against tubular and uveal cells [19]. Taken together, these results suggest that the pathogenesis of TINU syndrome differs from that of other types of ATIN and, therefore, patients with TINU syndrome should not be treated in the same manner as patients with other types of ATIN.
Conclusion
Our study of three patients with TINU syndrome showed the presence of acute tubulointerstitial inflammation 9 months after the initiation of systemic steroid therapy and the development of chronic renal damage. We believe that TINU patients who still show renal dysfunction after a 1 month follow-up should have a renal biopsy. If the TI score of the biopsy findings is high, the patient requires immunosuppressive therapy. Patients need to be closely observed for more than 2 years. Prospective randomized control studies are needed to identify the best therapy for TINU syndrome.
Abbreviations
- ATIN:
-
acute tubulointerstitial nephritis
- β2-MG:
-
β2-microglobulin
- TINU:
-
tubulointerstitial nephritis and uveitis
References
Dobrin RS, Vernier RL, Fish AL (1975) Acute eosinophilic interstitial nephritis and renal failure with bone marrow-lymph node granulomas and anterior uveitis. A new syndrome. Am J Med 59:325–333
Izzedine H (2008) Tubulointerstitial nephritis and uveitis syndrome (TINU): a step forward to understanding an elusive oculorenal syndrome. Nephrol Dial Transplant 23:1095–1097
Vanhaesebrouck P, Carton D, De Bel C, Praet M, Proesmans W (1985) Acute tubulo-interstitial nephritis and uveitis syndrome (TINU syndrome). Nephron 40:418–422
Manjon MT, Sanchez-Burson J, Montero R, Perez-Requena J, Alonso M, Marenco JL (1999) Two cases of acute tubulointerstitial nephritis associated with panuveitis (TINU syndrome). J Rheumatol 26:234–236
Takemura T, Okada M, Hino S, Fukushima K, Yamamoto S, Miyazato H, Maruyama K, Yoshioka K (1999) Course and outcome of tubulointerstitial nephritis and uveitis syndrome. Am J Kidney Dis 34:1016–1021
Tanaka H, Suzuki K, Nakahata T, Tateyama T, Waga S, Ito E (2001) Repeat renal biopsy in a girl with tubulointerstitial nephritis and uveitis syndrome. Pediatr Nephrol 16:885–887
Suzuki K, Tanaka H, Ito E, Waga S (2004) Repeat renal biopsy in children with severe idiopathic tubulointerstitial nephritis. Pediatr Nephrol 19:240–243
Vohra S, Eddy A, Levin AV, Taylor G, Laxer RM (1999) Tubulointerstitial nephritis and uveitis in children and adolescents. Four new cases and a review of the literature. Pediatr Nephrol 13:426–432
Tanaka H, Suzuki K, Nakahata T, Waga S (2003) Long-term outcome of acute tubulointerstitial nephritis: report of a case. Clin Nephrol 59:65–67
Hamdan JM, Obeidat FN (2006) Tubulo-interstitial nephritis and uveitis syndrome in a 6-year-old boy: case report. Ann Trop Paediatr 26:145–148
Foster BJ, Bernard C, Drummond KN, Sharma AK (2000) Effective therapy for severe Henoch-Schonlein purpura nephritis with prednisone and azathioprine: a clinical and histopathologic study. J Pediatr 136:370–375
Mandeville JT, Levinson RD, Holland GN (2001) The tubulointerstitial nephritis and uveitis syndrome. Surv Ophthalmol 46:195–208
Hirano K, Tomino Y, Mikami H, Ota K, Aikawa Y, Shirato I, Koide H (1989) A case of acute tubulointerstitial nephritis and uveitis syndrome with a dramatic response to corticosteroid therapy. Am J Nephrol 9:499–503
Kobayashi Y, Honda M, Yoshikawa N, Ito H (2000) Acute tubulointerstitial nephritis in 21 Japanese children. Clin Nephrol 54:191–197
Hinkle DM, Foster CS (2008) Tubulointerstitial nephritis and uveitis syndrome. Int Ophthalmol Clin 48:9–13
Yano N, Miyazaki M, Endoh M, Kuramoto T, Eguchi K, Yagame M, Nomoto Y, Sakai H (1991) Idiopathic acute interstitial nephritis associated with uveitis. Jpn J Med 30:548–552
Yoshioka K, Takemura T, Kanasaki M, Akano N, Maki S (1991) Acute interstitial nephritis and uveitis syndrome: activated immune cell infiltration in the kidney. Pediatr Nephrol 5:232–234
Kobayashi Y, Honda M, Yoshikawa N, Ito H (1998) Immunohistological study in sixteen children with acute tubulointerstitial nephritis. Clin Nephrol 50:14–20
Abed L, Merouani A, Haddad E, Benoit G, Oligny LL, Sartelet H (2008) Presence of autoantibodies against tubular and uveal cells in a patient with tubulointerstitial nephritis and uveitis (TINU) syndrome. Nephrol Dial Transplant 23:1452–1455
Acknowledgments
The authors are grateful to Dr. Mutsumi Murakami (Nippon Medical School) and Dr. Masami Tsuchiya (Nippon Medical School) for their important suggestions and intensive review and to Ms. Arimi Ishikawa (Department of First Pathology, Nippon Medical School) for assistance in the pathological techniques.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yanagihara, T., Kitamura, H., Aki, K. et al. Serial renal biopsies in three girls with tubulointerstitial nephritis and uveitis syndrome. Pediatr Nephrol 24, 1159–1164 (2009). https://doi.org/10.1007/s00467-009-1142-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-009-1142-9