
Abstract
This study was designed to characterize proteinuria in children with kidney disease. Random urine samples from 250 pediatric patients were examined by quantitative measures of total protein (pr), albumin (Alb), and creatinine (cr). Patient diagnoses were subjectively categorized as “Glomerular” (GD) or “Tubulo-interstitial” disease (TD) in origin. Proteinuria was quantitated by the random urine protein-to-creatinine (Upr/cr) ratio, and glomerular proteinuria was assessed as the albumin-to-creatinine ratio (Ualb/cr) and percentage albuminuria (%Alb=Alb/pr*100). The non-albumin fraction (1−Alb/pr) includes low-molecular-weight proteins and micro- and macroglobulins. Of the 250 patients, 112 (45%) had GD and 138 (55%) had TD. Both proteinuria and albuminuria correlated with a decline in glomerular filtration rate (GFR) (r=−0.4; p<0.0001). Those with GD averaged significantly greater %Alb than those with TD at all levels of proteinuria (p<0.0001). With loss in GFR, %Alb increased significantly in patients with TD (18±13 to 47±30%; p<0.001) and GD (56±26 to 74±15%; p<0.01), respectively. The %Alb at all levels of GFR averaged <50% in those with TD and >50% in those with GD. In conclusion, random Ualb/cr, Upr/cr, and %Alb provide a simple and inexpensive assessment of proteinuria and may profile renal disease activity and response to therapy in pediatric patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Proteinuria is an important indicator of kidney disease activity and progression [1]. However, timed urine collections are fraught with error in small children, and accuracy requires invasive bladder catheterization or restrictive immobilization. Quantitation of proteinuria by random assays in adults and children has afforded an accurate method to assess degree of renal disease activity [2–4]. Albumin excretion defines the glomerular barrier, and small amounts of albuminuria, termed ‘microalbuminuria’, predict cardiovascular and renal disease risks in adults [5]. The majority of low-molecular-weight (LMW) proteins filtered at the glomerulus are reabsorbed in the proximal tubule [1, 6–8]. The measurement of total protein in the urine includes non-albumin components as these may also indicate significant renal pathology [6–9]. Children may be more likely to demonstrate pathologic LMW proteinuria from tubular and interstitial injury due to the nature of congenital renal diseases and their susceptibility to ischemic injury [6–9]. We undertook a rapid method for profiling proteinuria in a large pediatric population to better define proteinuric renal disease and its progression in children.
Methods
Subjects
All patients were referred to the Pediatric Nephrology service at the University of Miami/Holtz Children’s Hospital between January 2002 and December 2005 for evaluation of suspected or known kidney disease. Infants <1 year of age or those patients who were receiving therapy with inhibitors of the renin-angiotensin-aldosterone system (RAAS) or with advanced Stage 5 kidney disease were excluded.
As a routine assessment of proteinuria, random urine specimens were sent for total protein, creatinine, and microalbumin analysis. This was an observational clinical study of minimally invasive examinations approved by the institutional review board of the University of Miami Miller School of Medicine. All subjects were assured anonymity in compliance with the Health Insurance Portability and Accountability Act (HIPAA).
A total of 250 pediatric patients with a mean age of 8.6±6.1 years (range: 1–21 years) were included in the study. There was equal gender distribution and a distinct Hispanic (109) and African ethnic (104) predominance, with only 34 non-Hispanic Caucasian and three Asian patients.
Disease categories
Diagnoses were classified according to probable origin of pathologic proteinuria and were broadly categorized as ‘Tubulo-interstitial’ (TD) or ‘Glomerular’ (GD) disease (Table 1).
“Glomerular” disease included any nephrotic or nephritic syndrome. Those with recent onset nephrotic syndrome who were steroid-sensitive were assumed to have minimal change disease and were sampled at the time of relapse or with clinical remission. Others with steroid-resistant or nephritic-nephrotic syndromes were assayed when clinically stable and/or prior to therapeutic intervention. All of these patients had biopsy-proven diagnoses. Patients referred for isolated microhematuria were included in this category. Adolescents referred for asymptomatic “dipstick” proteinuria were evaluated for orthostatic proteinuria, which included the first morning void fasting and an ambulatory void (preferably the second morning void). They were further assessed by 24-h urine for total protein, creatinine, and microalbumin split between the night time supine and the daytime ambulatory collection in order to document the orthostatic change and to quantitate the total daily excretion. For these patients, the first morning void was taken for inclusion in this analysis.
“Tubulo-interstitial” disease included congenital anomalies of the kidney and urinary tract (CAKUT) such as hypoplasia, dysplasia, vesico-ureteral reflux, or urinary tract obstruction with predominant TD injury. Patients with history of ischemic injury, extreme low birth weight, hereditary tubulopathies such as Bartter’s syndrome, cystinosis, renal tubular acidosis (RTA), or Fanconi’s syndrome were also considered in this category.
Random urine samples: components of proteinuria
All urine product measurements were reported or converted into metric units. The degree of proteinuria was determined by the random urine protein-to-creatinine ratio (Upr/cr; in mg/mg) with normal assessed at <0.2 and the nephrotic range at >2.0. These values reflect the range of proteinuria seen in children [1]. Normal proteinuria in children is ≤100 mg/m2 per day or ≤4 mg/m2 per h [1]. Nephrotic range proteinuria is ≥1000 mg/m2 per day or 40 mg/m2 per h [1]. Albuminuria was determined by the urine albumin-to-creatinine ratio (Ualb/cr) converted to milligram per milligram creatinine (mg Alb/mg cr) for ease of comparison to the Upr/cr. The calculation was as follows: Ualb/cr=Ualb (mg/dl) ÷ Ucr (mg/dl), with normal considered to be ≤0.030 mg Alb/mg cr or <30 mg/g cr. Glomerular proteinuria (GPr) was assessed as the percentage albuminuria (% Alb = Alb/Pr*100).
Random urine samples in children were obtained during waking hours with a preference for the period from the first morning void to 4:00 p.m. [3, 9]. Most patients were providing urine in the outpatient clinic setting and were clinically stable. No patient in the primary cohort had active urinary tract infection, fever, or sepsis. In the setting of relapse of the nephrotic syndrome or hospitalization, sequential urine samples were obtained to follow the evolution of the disease. However, only the initial urine from each patient in the primary cohort of 250 patients was used in the final analyses. Iterative specimens in 12 selected stable patients were used to verify the reproducibility of the measurements using the urine Alb/Pr ratio. Two patients with evolutionary disease served as examples of the clinical application of the method. Their assays were not a component of the primary cohort. Clinical chemistries, including serum creatinine, were available in the medical records in 92% (230/250) of the children.
Assays were performed in the central hospital clinical laboratory on the multichannel analyzer or in the Quest referral laboratories. Total protein was analyzed by a standard modification of the Lowry technique using a dye-binding automated spectrophotometric method. The coefficient of variation is <5%. Creatinine analysis was performed by the alkaline picrate method, which is a modification of the kinetic Jaffé reaction (Dade Paramax;Dade Corp, Miami, Fla.). The coefficient of variation is <2%. Microalbumin was determined by rate nephelometry with the Beckman Coulter array. The coefficient of variation is <4%.
Random urine dipsticks were performed in conjunction with the quantitative assays for total protein and creatinine when possible (221/250; 88%). The urinary dipsticks (Multistix 10 SG; Bayer Reagent Strips) consist of an alkaline color reaction to tetrabromphenol blue in the presence of albumin in the urine. These are the dipsticks used in our clinics and in the hospital for rapid assessment and monitoring purposes and are usually read and recorded by the nurses in attendance; they are entirely subjective. The color change is assessed against the color strip provided on the bottle. Any development of green above ‘trace’ is indicative of the presence of significant albuminuria ranging in concentration from 15 mg/dl to >300 mg/dl. A dipstick read as 1+ or greater was considered to be positive.
An estimation of glomerular filtration rate (GFR) was calculated as the creatinine clearance (Ccr) by the height index formula of Schwartz and expressed as milliliters/minute per 1.73 meters squared (ml/min/1.73 m2) [1, 10]. The stratification of chronic kidney disease (CKD) was according to the recommendations of K/DOQI Stages 1–5 [11]. Patients with a Ccr ≥60 ml/min/1.73 m2 were considered to have an early CKD (Stage<2), while those with a Ccr≤59 ml/min/1.73 m2 had advanced CKD (Stages 3–4). No patient with Stage 5 (GFR <15 ml/min/1.73 m2) was included in the present study (Table 2).
Statistical methods
All data sets were analyzed for Gaussian distribution using the D’Agostino-Pearson omnibus test for normality. Iterative sampling in stable patients to validate the method was also analyzed for kurtosis (to quantify the shape of the distribution) and skewness (to quantify the asymmetry of the distribution) with a normal Gaussian distribution having no skew and zero kurtosis. If the kurtosis is negative more values are centered, whereas if the kurtosis is positive, more values are in the “tails” of the distribution.
Differences between diagnostic categories and clinical characteristics were analyzed by one-way analysis of variance (ANOVA) using Tukey’s multiple comparisons post test. Correlation coefficients were calculated using Spearman rank order correlation. Urinary protein excretions and creatinine clearances, which are not normally distributed, were log-transformed for further analysis. Sensitivity and specificity with positive (PPV) and negative (NPV) predictive values were calculated using contingency tables and Fisher’s exact test. p values of less than 0.05 were considered to be significant. All results are expressed as the mean ± standard deviation (SD). All graphs and statistical analyses were determined using GraphPad Prism ver. 4.00 for Windows (GraphPad Software, San Diego, Calif.; https://doi.org/www.graphpad.com
Results
Validation and reproducibility by multiple sampling
To validate the reproducibility of the method, 12 patients considered to be clinically stable based on more than five iterative samples (mean: 10 samples; range: 5–13) over a period of 1 year provided 12 data sets that were analyzed for Gaussian distribution using the test for kurtosis, skewness, and normality. The %Alb was taken for this analysis since it does not include the urine creatinine, thereby avoiding the potential bias of variable renal function. Each data set was found to be normally distributed with the median well within the 95% confidence intervals. The average skew of the data sets was −0.178. The average kurtosis was −0.63, indicating “centered” values between narrow confidence intervals.
Distribution of proteinuria by age and disease category
There was a distinct difference in the character of proteinuria according to the designated disease categories. As shown in composite Fig. 1, children younger than 7 years of age had predominantly TD, whereas children older than 7 years had progressively more GD. There were 112 patients with GD who had an average age of 13±4 years and a female (n=65) and African ethnic (n=59) predominance. Those children with TD (n=138) had an average age of 5±5 years with a male (56%) and Hispanic (53%) predominance.

Composite of renal disease categories according to age and percentage albuminuria (%Alb). Filled diamond Tubular disease (TD) is significantly more common in children <7 years of age, while glomerular disease (GD) is more common after 7 years (p<0.001), filled star difference from TD category is significant at all levels of proteinuria (p<0.001)
Twelve children referred for asymptomatic dipstick proteinuria had supine and upright urines collected to determine the 24-h total protein and albumin excretion as well as to confirm orthostatic variation. Of these, eight had >1 g/m2/day of total proteinuria and underwent renal biopsy. Subsequent diagnoses were membranous nephropathy (1), mesangial proliferative glomerulitis (1), and focal segmental glomerulosclerosis (FSGS) (6). Of the remaining four in this subgroup, two had microalbuminuria but normal Upr/cr and two had confirmed orthostatic proteinuria (Table 1).
When proteinuria was profiled according to %Alb, the %Alb was greatest in those patients with GD (58%Alb) compared to those with TD (22%Alb) (Table 2, Fig. 1). When the degree of total proteinuria (Upr/cr) for the disease categories was longitudinally distributed into low (Upr/cr <0.2), moderate (Upr/cr>0.2<2.0), and severe (Upr/cr >2.0), the fraction of albuminuria was always significantly greater in patients with GD than in those with TD (F=38; p<0.0001) (Table 2; Fig. 1).
Renal function and proteinuria profiles
When the GD and TD categories were subdivided into those patients with Stages 1–2 CKD (Ccr: >60 ml/min/1.73 m2) and those with Stages 3–4 CKD (Ccr⩾16⩽59 ml/min/1.73 m2), there was a marked increase in %Alb and Ualb/cr in those with the more advanced stage of CKD. The most striking distinction was in the TD category in which the %Alb rose significantly with loss of renal function (18±13%Alb vs. 47±30%Alb; p<0.001). For those in the GD category, there was also a significant increase in %Alb with loss in renal function (56±26%Alb vs. 74±15%Alb; p<0.01) (Table 2; Fig. 2). Of note, those with TD averaged <50%Alb, while those with GD averaged >50%Alb at all levels of GFR.

Percentage (%) albuminuria according to renal disease categories with early Stage 2 chronic kidney disease (CKD) [creatinine clearance (Ccr): >60 ml/min/1.73 m2) and advanced Stages 3–4 glomerular filtration rate (GFR) (15<Ccr≤59 ml/min/1.73 m2). Filled star Significantly different from Stage 2 CKD in the same category, filled diamond significantly different from advanced Stage >3 CKD in the alternate category
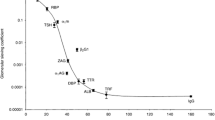
Progression of renal disease correlated significantly with increasing total proteinuria (Upr/cr) and albuminuria (Ualb/cr). These are not prospective analyses but cross-sectional data for the primary cohort. The regression equations and significance were similar for both variables (r=−0.4; p<0.0001). These regression analyses are shown in the composite Fig. 3.

Regression analyses of decline in GFR relative to proteinuria (Upr/cr) and albuminuria (Ualb/cr). Data are log-transformed to adjust for normality
Clinical application of urine profiling
As examples of the clinical application of sequential assays of the urine profile in individual patients, two patients are described below and their urine profiles depicted in Fig. 4.

Clinical longitudinal urine profiling in a patient with TD due to vesico-ureteral reflux during two episodes of pyelonephritis (upper panel) and in a GD patient with systemic lupus erythematosus (SLE) during treatment for exacerbation of lupus nephritis with intravenous solumedrol, mycophenolate mofetil (Cellcept), rituximab, and angiotensin receptor blocker (ARB) (lower panel)
Patient 1 is a 3-year-old girl with TD due to neurogenic bladder and reflux nephropathy. She was diagnosed during the first year of life following an episode of urosepsis. The proteinuria profile depicted in Fig. 4, upper panel was obtained before, during, and after two episodes of recurrent pyelonephritis.
Patient 2 is a 12-year-old girl with systemic lupus erythematosus (SLE) who was profiled during treatment for an exacerbation of her lupus nephritis (WHO IV). She had previously been treated unsuccessfully with cyclophosphamide therapy and, therefore, was given a course of pulse solumedrol followed by rituximab and maintenance therapy with mycophenylate mofetil (Cellcept) and an angiotensin receptor blocker (ARB). Figure 4, lower panel demonstrates the patient’s proteinuria profile in response to the therapeutic interventions applied for this lupus exacerbation.
Urinary dipstick, Upr/cr, and Ualb/cr: sensitivity and specificity; PPV and NPV
Table 3 provides the statistical comparisons between urinary dipsticks and quantitative random urines with the relative application of predictive values of each test for the detection of significant proteinuria and albuminuria in this cohort of patients.
There were 240 urine samples that were quantitatively assessed by Upr/cr and Ualb/cr. The sensitivity of the Upr/cr for detection of albuminuria was 84%, with a specificity of 81%, whereas the sensitivity of the Ualb/cr for detection of proteinuria was only 60%, with a specificity of 93%. Although 81 (34% of these urine samples had a normal quantitative Upr/cr of <0.2, 32 (13%) of these demonstrated albuminuria (Ualb/cr) above the threshold of 30 mg/g creatinine.
There were 221 urine samples that were assessed by both quantitative Upr/cr and the urinary dipstick. Of these, 54 had a normal Upr/cr of <0.2, and 167 (76%) had a pathologic Upr/cr of >0.2. This gave a sensitivity of 42% for the urinary dipstick, with a specificity of 98%.
Discussion
This paper describes important unique aspects of proteinuria in a large pediatric patient population through the application of simple and inexpensive techniques. We show that a distinction can be made between tubular and glomerular components of proteinuria by “profiling” random urine samples for total protein and albumin referenced to creatinine. Normal components of proteinuria have previously been estimated to be 30% albumin, which is the ‘glomerular’ component and 30–60% Tamm-Horsfall protein, which is the tubular secretory glycoprotein, with the remainder being LMW proteins that escape proximal tubular reabsorption [1, 6–9, 12, 13].
In this series of pediatric patients we have shown that components of proteinuria vary according to disease category and loss of renal function. Glomerular and tubular or interstitial injury appear to determine the degree and character of the proteinuria which can serve as important markers of kidney disease progression [1, 6–9, 14]. Pathologic macroglobulinuria with increased filtration of the IgM immunoglobulin signals large defects in the glomerular pore barrier [15]. Protein electrophoresis can provide a visual array of the various proteins, such as β-2-microglobulin and retinal binding protein, which are excreted as menacing chemokines, slough, or overflow. These are expensive to assay and require immediate alkalinization for preservation and accuracy [16]. We believe that simple urine protein profiling interpreted in the context of the clinical setting can serve as a useful tool for diagnosis and management. As an example, a young patient with vesico-ureteral reflux who had baseline urine protein profiling developed a febrile urinary tract infection. With sequential Upr/cr and Ualb/cr we were able to detect a rise in proteinuria and albuminuria, respectively, that returned to normal after response to antibiotic therapy. This provided impetus for early surgical intervention and closer surveillance for scar formation. The utility of these simple quantitative assays for individual patient assessment has been very enlightening in our Pediatric Nephrology practice and seems to have potential for further development in the clinical arena.
Pediatric patients with proteinuria vary widely in their origins of disease. Many have CAKUT or inherited genetic tubulopathies [1, 2, 6, 14, 17]. Most of these children are diagnosed within the first years of life and have a prevalence of tubular proteinuria as shown by our population. In our young cohort the magnitude of the total proteinuria as well as albuminuria correlated with loss of GFR, confirming previous published observations [1, 5, 6, 13, 14]. At similar levels of proteinuria, those patients with GD always had a significantly greater percentage of albuminuria, usually averaging more than 50% of total protein. An important observation was that a significant increase in the fraction of albuminuria heralded the loss of renal function in patients with TD. It is still unclear whether proteinuria or albuminuria are merely surrogate markers of renal disease progression. This is confounded by the fact that proteinuria may actually perpetuate renal interstitial injury [6]. Nevertheless, medical interventions that alter proteinuria do impact on renal survival [18]. It is imperative that pediatricians recognize the importance of characterizing proteinuria in their diverse population with a caveat towards better and earlier interventions.
Although the quantitative assay for albuminuria has the greatest specificity for detecting pathologic proteinuria, it lacks the sensitivity required in patients with predominant TD as in this pediatric population. Our data are similar to a much larger cohort of Australians in which urines were assayed for both proteinuria and albuminuria in over 10,000 participants in a lifestyle study [19]. As the magnitude of proteinuria increased from normal to >0.8 mg/mg creatinine, the fraction of albuminuria increased from 21 to 73%. Albuminuria performed well as a screening test in this older population but still missed significant proteinuria in 8% of their cohort. This re-enforces the usefulness of assaying for both total protein and albumin.
In large clinical trials, the best biologic endpoints are those that can be accurately quantitated and are relatively non-invasive, inexpensive, and easily performed in the out patient setting [20]. The current method of profiling urines for components of proteinuria offers an advantage in that the assays are performed on a single random urine that requires no special handling or preservation. The sample can be refrigerated for a week or frozen at 0°C without any loss of reproducibility. This makes the use of protein profiling of random urines a compelling instrument in the design of large pediatric clinical trials requiring accurate detection and assessment of kidney disease activity.
There are several categories of emerging pediatric populations that deserve special attention for increased risk and more astute urine profiling. The surviving low birth weight, premature infant is more susceptible to oligonephropathy and/or ischemic nephropathy that may progress with age [21]. The obesity epidemic and the emergence of the metabolic syndrome in younger populations requires urine profiling for early detection of microalbuminuria as a potential independent risk factor for cardiovascular disease [22]. Focal glomerulosclerosis in high-risk ethnic populations is increasing and may be strangely silent in its early stages [23, 24]. Patients with sickle cell disease are also prone to complex renal lesions which might be better followed by specific profiling of their proteinuria [25]. In the work-up of isolated microhematuria, glomerular pathology is distinquished by micro-albuminuria [26].
Urinary dipsticks, as used in pediatric practice, remain poor diagnostic tools for assessing proteinuria [4, 27]. This report confirms and emphasizes previous observations showing that while the most commonly used dipstick (Multistix 10 SG) is highly specific for the presence of albuminuria, it lacks sensitivity and has a low negative predictive value. Although more sensitive dipsticks have been developed and been shown to be reliable in screening large populations, they are still not readily available for office practice [28, 29]. Therefore, we emphasize that commercially available dipsticks miss over half of young patients with TD and warrant quantitative assays for a thorough assessment.
The circadian rhythm of proteinuria described by Ginsberg et al. [3] some years ago showed that the lowest ebb of daily proteinuria followed the first morning void and that the random Upr/cr obtained during the ambulatory period from late morning to early afternoon correlated best to the total 24-h urine protein. In pediatrics, we must consider the issue of orthostatic proteinuria, which is reported to occur in up to 10% of the population with a peak in adolescence [30, 31]. In the current population there were only 12 patients with asymptomatic proteinuria, eight of whom were found to have significant pathology after biopsy. Although the condition is thought to be benign, there is a lack of confirming evidence, and sporadic reports question the validity of such a benign prognosis [32]. Our data support this approach, and we recommend urine profiling and quantitation of daily proteinuria in adolescents with asymptomatic proteinuria.
In conclusion, quantitative measures of both proteinuria and albuminuria are important in the context of children with known or suspected kidney disease to guide diagnosis, prognosis and patient management.
References
Hogg RJ, Portman RJ, Milliner D, Lemley K, Eddy A, Ingelfinger J (2000) Evaluation and management of proteinuria and nephrotic syndrome in children: recommendations from a pediatric nephrology panel established at the National Kidney Foundation Conference on Proteinuria, Albuminuria, Risk, Assessment, Detection, and Elimination (PARADE). Pediatrics 105:1242–1249
Barratt TM, McLaine PM, Soothhill JF (1970) Albumin excretion as a measure of glomerular dysfunction in children. Arch Dis Child 45:496–501
Ginsberg JM, Chang BS, Matarese RA, Garella S (1983) Use of single voided urine specimens to estimate quantitative proteiuria. N Engl J Med 309:1543–1546
Abitbol C, Strauss J, Zilleruelo G, Freundlich M (1990) Quantitation of proteinuria with urinary protein/creatinine ratios and random testing with dipsticks in nephrotic children. J Pediatr 116:243–247
Eknoyan G, Hostetter T, Bakris GL, Hebert G, Levey A, Parving HH, Parving H-H, Steffes MW, Toto R (2003) Proteinuria and other markers of chronic kidney disease: a position statement of the National Kidney Foundation (NKF) and the National Institute of the Diabetes and Digestive and Kidney Diseases (NIDDK). Am J Kidney Dis 42(4):617–622
Eddy A (2004) Proteinuria and interstitial injury (editorial comments). Nephrol Dial Transpl 19:277–281
Christensen EI, Gburek J (2004) Protein reabsorption in renal proximal tubule-function and dysfunction in kidney pathophysiology. Pediatr Nephrol 19:714–721
Ojala R, Ala-Houhala M, Harmoinen A, Luukaala T, Uotila J, Tammela O (2006) Tubular proteinuria in preterm and fullterm infants. Pediatr Nephrol 21:68–73
Christensen EI, Gburek J (2004) Protein reabsorption in renal proximal tubule-function and dysfunction in kidney pathophysiology. Pediatr Nephrol 19:714–721
Schwartz GJ, Haycock GB, Edelmann CM (1976) A simple estimate of glomerular filtration in children derived from body length and plasma creatinine. J Pediatr 58:259–263
National Kidney Foundation (2002) K/DOQI clinical practice guidelines: evaluation, classification, stratification. Am J Kidney Dis 39:S1–S00
Thornley C, Dawnay A, Cattell WR (1985) Human Tamm-Horsfall glycoprotein: urinary and plasma levels in normal subjects and patients with renal disease determined by a fully validated radioimmunoassay. Clin Sci (Lond) 68:529–535
Schwab SJ, Dunn FL, Feinglos MN (1992) Screening for microalbuminuria. A comparison of single sample methods of collection and techniques of albumin analysis. Diabetes Care 15:1581–1584
Ardissino G, Avolio L, Dacco V, Testa S, Marra G, Vigano S, Loi S, Caione P, De Castro R, De Pascale S, Marras E, Riccipetitoni G, Selvaggio G, Pedotti P, Claris-Appiani A, Ciofani A, Dello Strologo L, Lama G, Montini G, Verrina E; ItalKid Project (2004) Long-term outcome of vesicoureteral reflux associated chronic renal failure in children. Data from the ItalKid Project. J Urol 172:305–310
Bakoush O, Torrffvit O, Rippe B, Tencer J (2001) High proteinuria selectivity index based upon IgM is a strong predictor of poor renal survival in glomerular diseases. Nephrol Dial Transpl 16:1357–1363
Donaldson MD, Chambers RE, Woolridge MW, Whicher JT (1989) Stability of alpha 1-microglobulin, beta 2-microglobulin and retinol binding protein in urine. Clin Chim Acta 179:73–77
Kuwayama F, Miyazaki Y, Ichikawa I (2002) Embryogenesis of the congenital anomalies of the kidney and urinary tract. Nephrol Dial Transplant 17[Suppl 9]:45–47
Wühl E, Mehls O, Schaefer F; ESCAPE Trial Group (2004) Antihypertensive and antiproteinuric efficacy of ramipril in children with chronic renal failure. Kidney Int 66:768–776
Atkins RC, Briganti EM, Zimmet PZ, Chadban SJ (2003) Association between albuminuria and proteinuria in the general population: the AusDiab Study. Nephrol Dial Transpl 18:2170–2174
Hewitt SM, Dear J, Star RA (2004) Discovery of biomarkers for renal diseases. A review. J Am Soc Nephrol 15:1677–1689
Abitbol CL, Bauer CR, Montane B, Chandar J, Duara S, Zilleruelo G (2003) Long-term follow-up of extremely low birth weight infants with neonatal renal failure. Pediatr Nephrol 18:887–893
Csernus K, Lanyi E, Erhardt E, Molnar D (2005) Effect of childhood obesity and obesity-related cardiovascular risk factors on glomerular and tubular protein excretion. Eur J Pediatr 164:44–49
Chesney R (2004) The changing face of childhood nephrotic syndrome. A review. Kidney Int 66:1294–1300
Srivastava T, Simon SD, Alon US (1999) High incidence of focal segmental glomerulosclerosis in nephrotic syndrome of childhood. Pediatr Nephrol 13:13–18
Dharnidharka VR, Dabbagh S, Atiyeh B, Simpson P, Sarnaik S (1998) Prevalence of microalbuminuria in children with sickle cell disease. Pediatr Nephrol 12:475–478
Assadi FK (2005) Value of urinary excretion of microalbumin in predicting glomerular lesions in children with isolated microscopic hematuria. Pediatr Nephrol 20:1131–1135
Ralston SH, Caine N, Richards I, O’Reilly D, Sturrock RD, Capell HA (1988) Screening for proteinuria in a rheumatology clinic: comparison of dipstick testing, 24 hour urine quantitative protein, and protein/creatinine ratio in random urine samples. Ann Rheum Dis 47:759–763
Kaneko K, Someya T, Nishizaki N, Shimojima T, Ohtaki R, Kaneko KI (2005) Simplified quantification of urinary protein excretion using a novel dipstick in children. Pediatr Nephrol 20:834–836
Wallace JF, Pugia MJ, Lott JA, Luke KE, Shihabi ZK, Sheehan M, Bucksa JM (2001) Multisite evaluation of a new dipstick for albumin, protein, and creatinine. J Clin Lab Anal 15:231–235
Houser MT, Jahn MF, Kobayashi A, Walburn J (1986) Assessment of urinary protein excretion in the adolescent: Effect of body position and exercise. J Pediatr 109:556–561
Vehashkari VM, Robson AM (1992) Proteinuria. In: Edelmann CM (ed) Pediatric kidney disease. Little-Brown, Boston, pp 531–551
Berns JS, McDonald B, Gaudio KM, Siegel NJ (1986) Progression of orthostatic proteinuria to focal and segmental glomerulosclerosis. Clin Pediatr 25(3):165–166
Acknowledgement
This study was supported in part by a grant from Florida’s Department of Health, Children’s Medical Services.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abitbol, C.L., Chandar, J., Onder, A.M. et al. Profiling proteinuria in pediatric patients. Pediatr Nephrol 21, 995–1002 (2006). https://doi.org/10.1007/s00467-006-0103-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-006-0103-9