
Abstract
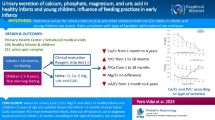
The aims of this study were to determine reference ranges for the urinary calcium (UCa/Cr) and phosphate (UPO4/Cr) creatinine ratios and to study factors influencing these ratios in a representative population of preterm infants managed according to current nutritional guidelines. Spot urine samples were obtained from 186 preterm infants (gestation 24–34 weeks) for measurement of UCa/Cr and UPO4/Cr ratios as part of a routine metabolic bone screening program, once every 2–4 weeks from the 3rd to the 18th week of life. Data were also collected on gender, appropriate or small for gestational age (SGA), nutrition [total parenteral nutrition (TPN), preterm or term formula, and breast milk], plasma Ca, PO4, urea, and electrolytes and on the use of drugs (frusemide, dexamethasone, and theophylline). Data from infants treated with any of these three drugs were analysed separately and not included in establishing the reference ranges for UCa/Cr and UPO4/Cr. The mean gestational age of the study population was 28 weeks (range 24–34 weeks). The 95th percentile for UCa/Cr at 3 weeks of age was 3.8 mmol/mmol and decreased significantly with increasing postnatal age ( P <0.001). The 95th percentile for UPO4/Cr was 26.69 mmol/mmol at 3 weeks of age, but this did not change significantly with increasing postnatal age ( P =0.296). On univariate analysis there was no significant association of UCa/Cr and UPO4/Cr with gender and type of enteral nutrition. The UCa/Cr was lower in infants who were SGA ( P =0.013) and with low plasma Ca ( P =0.008). Infants on TPN had significantly higher UCa/Cr ( P =0.019) and lower UPO4/Cr ratios ( P ≤0.001). Multivariate analysis confirmed the decrease in UCa/Cr ratio with increasing postnatal age, but the SGA effect was eliminated. The use of furosemide ( P <0.001) and theophylline ( P =0.003) was associated with a significant increase in the UCa/Cr ratio. The use of dexamethasone was also associated with an increase in UCa/Cr ratio, but this did not achieve statistical significance ( P =0.339). The use of furosemide, theophylline, and dexamethasone had no effect on UPO4/Cr. We report a reference range for UCa/Cr and UPO4/Cr ratios and factors influencing these ratios in a representative population of preterm infants between 24 and 34 weeks gestation, managed according to current nutritional guidelines.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The urinary excretion of calcium (UCa) and phosphate (UPO4) in healthy children between 1 and 18 years [1, 2, 3, 4, 5] has been well documented, but studies on UCa and UPO4 excretion in preterm infants are limited. Research on UCa and UPO4 in preterm babies has used normal reference ranges for UCa and UPO4 in term infants [6]. However, the normal UCa and UP04 might vary in preterm infants according to postnatal age (PNA). Reference data for UCa and UPO4 in preterm babies would enable a more accurate study of the aetiology of nephrocalcinosis (NC) in this age group and would be useful in studies of Ca and PO4 metabolism and in optimizing Ca and PO4 supplementation. Karlen et al. [7] studied UCa and UPO4 excretion in 51 stable preterm infants (mean gestation 32 weeks) who were fed predominantly on breast milk without PO4 supplementation. However, it is recognised that extremely low birth weight infants fed on breast milk are depleted in PO4 and Ca and are paradoxically hypercalciuric in relation to the degree of PO4 deficiency [8, 9]. It is also likely that these data no longer reflect current nutritional practice.
Increased excretion of UCa and UPO4 has been associated with the development of NC in preterm infants [10, 11, 12]. We and others have reported an incidence of NC of 16%–63% in preterm infants born before 32 weeks gestation or very low birth weight (VLBW) infants [10, 13, 14]. A recent retrospective study of babies born at <37 weeks gestation reported that the incidence of NC was 0.73% (1.7% for VLBW infants) [15]. Factors known to influence UCa excretion in the preterm infant include frusemide [16, 17], theophylline [18, 19], and dexamethasone [20]. Furosemide has also been shown to increase UPO4 excretion in VLBW infants [17].
A close linear correlation has been established between 24-h UCa excretion and random UCa/Cr ratio in children [1, 3] and adults [21], but accurate timed collection of urine in preterm infants is difficult. The present study was conducted to determine reference ranges for UCa/Cr and UPO4/Cr ratios in a population of preterm infants born at 24–34 weeks gestation, who were managed according to current nutritional guidelines, and to study the effect of frusemide, theophylline, and dexamethasone.
Patients and methods
The study population was drawn from preterm babies born at The Queen Mother’s Hospital, Glasgow, a tertiary neonatal unit. Urine and blood samples were obtained from 186 consecutive preterm infants (gestation 24–34 weeks) as part of a routine metabolic bone screening program performed every 2–4 weeks from the 3rd to 18th week of life. All infants were stable at the time of urine collection (60% required ventilation during the first 1–3 weeks of life and 25% were oxygen dependent at 36 weeks of post-conceptional age). All but 5 infants were Caucasians. Urine samples were collected either by clean catch or adhesive bag (Hollister U-Bag) between 0100 and 0800 hours and blood samples (for plasma urea and electrolytes, Ca, PO4, and alkaline phosphatase) between 0700 and 0900 hours. In total, 296 paired urine and plasma samples were analysed. Data were collected on gender, whether the birth weight was appropriate (AGA) or small (SGA) for gestational age, nutritional details [total parental nutrition (TPN), preterm or term formula, and breast milk], and on the use of drugs (frusemide, dexamethasone, and theophylline). Data from infants treated with frusemide, dexamethasone, or theophylline (88 paired urine and plasma samples) were analysed separately and not used for establishing the reference ranges for UCa/Cr and UPO4/Cr ratios.
Nutrition and supplementation
The unit practice was to use a maximum of 150 ml/kg per day TPN, 170 ml/kg per day preterm formula (Ostoprem), or 200 ml/kg per day expressed breast milk (EBM)/term formula; 100 ml of TPN provided 1 mmol of Ca and PO4 and 1.7 g of protein. TPN infusion commenced at 60 ml/kg per day, increased to a maximum of 150 ml/kg per day over 4 days, and continued at this rate until the baby tolerated oral feeding. The TPN PO4 content was increased according to plasma PO4 and tubular PO4 reabsorption (TRP), and TPN protein content increased to 2.32 g/100 ml from day 8 onwards. No protein fortifier was added to EBM. All infants on enteral feeding received routine supplementation of vitamin D 800 IU (Mother’s and Children’s Vitamin Drops) and PO4 1 mmol/kg per day (potassium acid phosphate). TPN-fed infants received vitamin D as ergocalciferol (Vitlipid N Infant, Fresenius Kabi, UK) at 160 units/kg per day up to a maximum of 400 units/day. One 32-week and 3 33-week gestation babies did not receive routine PO4 supplementation. Oral supplementation of vitamin D and PO4 was initiated when 50% of the enteral feed was tolerated and PO4 supplementation was adjusted to maintain plasma PO4>1.8 mmol/l and TRP<85%. The sodium intake was adjusted according to the plasma and urinary sodium levels.
Sample analysis
Plasma Ca, PO4, urea, electrolytes, and alkaline phosphatase were analysed by dry slide technique using an Ortho Vitros 950 analyser. Urinary Ca, PO4, and creatinine were also analysed by dry slide technique using an Ortho Vitros 250 analyser. Urine was acidified to pH <3 prior to analysis of PO4 and Ca. The analyzer range for urine Ca is 0.12–4.49 mmol/l and for urine PO4 0.13–6.46 mmol/l. It should be noted that the absolute value of UCa/Cr or UPO4/Cr will depend on the creatinine concentration of the urine specimen. As the urine in preterm infants is often extremely dilute, laboratory practice was to re-analyse urine creatinine specimens with a value less than 1.0 mmol/l, using plasma methodology that has a much lower limit of detection (around 12 μmol/l). UCa/Cr and UPO4/Cr ratios are reported as the molar ratios. TRP (ratio of the PO4 clearance to the creatinine clearance) was calculated and expressed as a percentage.
Statistical analysis
The data were transformed by Box-Cox regression as they were positively skewed. Transformation used the parameter lambda=0.3 for the UCa/Cr ratio and lambda=0.5 for the UPO4/Cr ratio. We performed multivariate linear regression with the clustering option since more than one measurement was taken from the same individual at different times. The 5th and 95th percentiles for the UCa/Cr and UPO4/Cr ratios were calculated using the square root of the error mean square of the regression as an estimate of the standard deviation for the distribution. Univariate and multivariate analysis was performed to determine the factors influencing UCa/Cr and UPO4/Cr ratios.
Results
The mean gestational age was 28 weeks with lower and upper quartiles of 27 and 30 weeks, respectively. Plasma urea, creatinine, bicarbonate, PO4, Ca, and alkaline phosphatase values are shown in Table 1. Since there was no significant difference on univariate analysis in UCa/Cr and UPO4/Cr with gestation and gender, all data were grouped for further analysis (Table 2).
Urinary Ca/Cr
The percentile distribution of UCa/Cr is shown in Fig. 1, which shows a significant decrease with increasing PNA ( P <0.001).

Urinary calcium/creatinine ( UCa/Cr) ratio percentile for 24- to 34-week preterm infants from 3 to 18 weeks of age. Conversion factor: 1 mmol/mmol=0.355 mg/mg
Univariate analysis
UCa/Cr was significantly lower in SGA babies and in babies with lower plasma Ca and higher in babies on TPN and with higher TRP. No significant association was found with gestation, gender, the type of enteral feed, plasma bicarbonate, PO4, or alkaline phosphatase (Table 2).
Multivariate analysis
UCa/Cr was significantly lower in babies on EBM and in those with a low plasma PO4, but the effect of SGA was eliminated. In addition, UCa/Cr was significantly higher in babies with higher plasma Ca and bicarbonate, and babies on TPN (Table 3).
Urinary PO4/Cr
The percentile distribution of urinary UPO4/Cr is shown in Fig. 2. By univariate analysis babies on TPN had significantly lower UPO4/Cr ratio and those with lower plasma PO4 and higher plasma Ca had lower and higher UPO4/Cr ratios respectively; however this was not significant. In addition, there was no significant association between the UPO4/Cr ratio and gestation, PNA, gender, SGA, type of enteral feed, plasma bicarbonate, and alkaline phosphatase (Table 2).

Urinary phosphate/creatinine ( UPO 4 /Cr) ratio percentile for 24- to 34-week preterm infants from 3 to 18 weeks of age. Conversion factor: 1 mmol/mmol=2.74 mg/mg
Multivariate analysis
Babies on TPN ( P <0.001) and with lower gestational age (24–29 weeks) had a significantly lower UPO4/Cr ratio ( P =0.03). Babies with a higher plasma Ca had a significantly higher UPO4/Cr ( P =0.04) and there was a trend towards a lower UPO4/Cr in babies with lower plasma PO4 ( P =0.06).
There was no change in the percentile reference ranges for UCa/Cr and UPO4/Cr ratios when the data were re-analysed after excluding values from week 13–18 (Figs. 3 and 4).

UCa/Cr ratio percentile for 24- to 34-week preterm infants from 3 to 12 weeks of age (excluding values from weeks 13–18)

UPO4/Cr ratio percentile for 24- to 34-week preterm infants from 3 to 12 weeks of age (excluding values from week 13–18)
Drugs and urinary Ca and PO4
Frusemide and theophylline (both loading and maintenance doses) significantly increased UCa/Cr. Babies who received postnatal dexamethasone also had higher UCa/Cr, but this was not significant (Table 4). There was no association between UPO4/Cr and the use of frusemide, theophylline, or dexamethasone (Table 4).
Discussion
We report reference ranges for UCa/Cr and UPO4/Cr ratios for a population of preterm infants (24–34 weeks gestation) who received PO4 supplementation and found a significant negative correlation between UCa/Cr and PNA. This age-related decrease in UCa/Cr is similar to that seen in term infants within the 1st year of life [22] as well as in older children [5, 23]. Our data differ from other studies [1, 2], including those of Karlen et al. [7] who found little or no correlation of UCa with PNA. However, this latter study was carried out in infants who did not receive PO4 supplementation and as a result were likely to be hypercalciuric [8, 9].
We believe the decrease in UCa/Cr ratio with advancing PNA results from improved bone deposition of Ca [24, 25, 26]. The negative correlation could also be due to a decrease in urinary sodium excretion [27, 28], since Ca reabsorption in the proximal tubule (50%–55%) and loop of Henle (20%–30%) parallels sodium reabsorption [29]. The influence of PNA on urinary creatinine excretion is somewhat controversial. Al-dahhan et al. [30] and Coulthard et al. [31] found no relationship between urinary creatinine and PNA. However, others have reported that urinary creatinine excretion is positively correlated with PNA [28].
We used the type of nutrition as a proxy for Ca and PO4 intake, and found no relationship between the type of milk ingested and UCa/Cr on univariate analysis. However, babies on breast milk had a significantly lower UCa/Cr ratio on multivariate analysis. These findings are similar to other reports in which no relationship was found between UCa/Cr and Ca intake [2, 22, 24, 32]. The likely explanation for this lack of correlation is that UCa in preterm infants originates mainly from bone turnover with a relatively small percentage (12%–27%) coming from oral intake [24]. Preterm infants fed unsupplemented breast milk tend to be hypercalciuric due to PO4 deficiency [8, 9, 33] and our finding of a low UCa/Cr in infants given PO4-supplemented EBM suggest improved bone deposition of Ca [9]. However, Schell-Feith et al. [6] found that a high Ca intake was associated with higher Ca excretion and an increased risk of NC. These authors also noted that the PO4 intake was higher in the NC group, but found no difference in UPO4 excretion, duration and volume of parenteral or enteral (breast or formula) nutrition between NC and non-NC infants. We found that infants with NC received smaller amount of Ca and PO4 between 2 and 6 weeks of life compared with non-NC babies, and there was no difference in urinary excretion of Ca between the two groups. NC babies also received TPN for significantly longer [13]. Our finding of an increase in UCa/Cr in infants on TPN is in agreement with those of Vileisis [34] and Hoppe et al. [35]. Explanations for this finding include a relative PO4 depletion [34], a higher sodium intake [35], and a lower protein intake [26] resulting in hypercalciuria due to decreased utilisation of Ca for bone growth. Decreased bone mineralisation may result in metabolic bone disease of prematurity, abnormal growth, and fractures [36]. We did not measure direct bone mineral content in this study but the indirect measure of bone mineral content was within acceptable limits for preterm infants (Table 1). All our infants with a plasma alkaline phosphatase >500 U/l had a plasma PO4>1.6 mmol/l, with the exception of 1 whose plasma PO4 was 1.13 mmol/l. A recent study by Backstrom et al. [37] showed that a combination of plasma alkaline phosphatase activity above 900 IU/l and plasma PO4 below 1.8 mmol/l yields a sensitivity of 100% and a specificity of 70% for detection of low bone mineral density in preterm infants.
Infants in this study with higher plasma Ca had a higher UCa/Cr ratio as expected, but we found no correlation between UCa/Cr and gestational age at birth, AGA/SGA, or gender. Hillman et al. [24] reported a similar lack of correlation between UCa and gestational age or birth weight, and a number of studies found no correlation between UCa and gender in children [1, 2, 3, 4, 5, 23], but there are no available comparative data in preterm infants. We did not analyse our data according to race, as our population was predominantly Caucasian. It has been shown however that UCa/Cr is lower in African-American [38] and Asian children [39] than Caucasian children due to differences in diet. However, any racial differences in UCa/Cr in preterm infants are unlikely as all infants receive similar nutrition according to their clinical state/need.
We found the UPO4/Cr ratio remained stable from the 3rd week to the 18th week of PNA. These findings are similar to those of Mihatsch et al. [40] who reported that in infants sufficiently substituted with PO4, although the plasma PO4 decreased with increasing PNA, the urinary PO4 excretion remained stable due to a progressive decrease in renal phosphate threshold. Karlen et al. [7] found that UPO4 was high during the 1st postnatal week, decreased during the 2nd, remained low up to the 5th, increased from the 6th, and remained stable until at least 3 months of PNA. However, it is difficult to compare these data with our own as the study group of Karlen et al. [7] was not supplemented with PO4, was more mature, and the data were given as a mean value and not as a percentile. In addition, a number of reports have documented low UPO4 in PO4-deficient infants [9, 34].
In the present study, the infants on TPN and of low gestational age (24–29 weeks) had lower UPO4/Cr. This may be the result of a lower PO4 intake and/or an increased mineral demand for growth [41]. We found no gender differences in UPO4/Cr and no differences between infants who were AGA compared with those SGA. UPO4/Cr did not vary with different milk intake, and we feel this resulted from our PO4 supplementation policy.
Infants who received frusemide [16, 17] and theophylline [18, 19] had significantly higher UCa/Cr as previously reported. Infants on dexamethasone also had higher UCa/Cr, but this did not achieve statistical significance, in contrast to the data of Kamitsuka et al. [20], perhaps because of the relatively small numbers in this study. Frusemide, theophylline, and dexamethasone had no effect on the UPO4/Cr ratio, but there are no comparative published data available.
In conclusion, we report reference ranges for UCa/Cr and UPO4/Cr ratio in a population of preterm infants between 24 and 34 weeks′ gestation. The UCa/Cr ratio is inversely related to PNA, whereas the UPO4/Cr ratio remained stable between the 3rd to 18th weeks of PNA. Gender and SGA had no effect on either ratio. Infants on TPN had higher UCa/Cr and lower UPO4/Cr ratios. Frusemide and theophylline increased UCa/Cr but not the UPO4/Cr ratio.
References
Ghazali S, Barratt TM (1974) Urinary excretion of calcium and magnesium in children. Arch Dis Child 49:97–101
Sargent JD, Stukel TA, Kresel J, Klein RZ (1993) Normal values for random urinary calcium to creatinine ratios in infancy. J Pediatr 123:393–397
Reusz SS, Dobos M, Byrd D, Sallay P, Miltenyi M, Tulassay T (1995) Urinary calcium and oxalate excretion in children. Pediatr Nephrol 9:39–44
Matos V, Malle GV, Boulat OO, Markert M, Bachmann C, Guignard JP (1997) Urinary phosphate/creatinine, calcium/creatinine, and magnesium/creatinine ratios in a healthy pediatric population. J Pediatr 131:252–257
Vachvanichsanong P, Lebl L, Moore ES (2000) Urinary calcium excretion in healthy Thai children. Pediatr Nephrol 14:847–850
Schell-Feith EA, Kist-van Holthe JE, Conneman N, Zwieten PH van, Holscher HC, Zonderland HM, Brand R, Heijden BJ van der (2000) Etiology of nephrocalcinosis in preterm neonates: association of nutritional intake and urinary parameters. Kidney Int 58:2102–2110
Karlen J, Aperia A, Zetterstrom R (1985) Renal excretion of calcium and phosphate in preterm and term infants. J Pediatr 106:814–819
Rowe J, Rowe D, Horak E, Spackman T, Saltzman R, Robinson S, Philipps A, Raye J (1984) Hypophosphatemia and hypercalciuria in small premature infants fed human milk: evidence for inadequate dietary phosphorus. J Pediatr 104:112–117
Lyon AJ, McIntosh N (1984) Calcium and phosphorus balance in extremely low birth weight infants in the first 6 weeks of life. Arch Dis Child 59:1145–1150
Short A, Cooke RWI (1991) The incidence of renal calcification in preterm infants. Arch Dis Child 66:412–417
Short A, Shaw NJ, Weindling AM (1990) Nephrocalcinosis and phosphate supplementation in a preterm infant. Acta Paediatr Scand 79:968–969
Saarela T, Vaarala A, Lanning P, Koivisto M (1999) Incidence, ultrasonic patterns and resolution of nephrocalcinosis in very low birth weight infants. Acta Paediatr 88:655–660
Narendra A, White MP, Rolton HA, Alloub ZI, Wilkinson G, McColl JH, Beattie J (2001) Nephrocalcinosis in preterm babies. Arch Dis Child 85:207–213
Jacinto JS, Modanlou HD, Crade M, Strauss AA, Bosu SK (1988) Renal calcification in very low birth weight infants. Pediatrics 81:31–35
Hoppe B, Duran I, Martin A, Kribs A, Benz-Bohm G, Michalk DV, Roth B (2002) Nephrocalcinosis in preterm infants: a single center experience. Pediatr Nephrol 17:264–268
Atkinson SA, Shah JK, McGee C, Steele BT (1988) Mineral excretion in premature infants receiving various diuretic therapies. J Pediatr 113:540–545
Vileisis RA (1990) Furosemide effect on mineral status of parenterally nourished premature neonates with chronic lung disease. Pediatrics 85:316–322
Zanardo V, Dani C, Trevisanuto D, Meneghetti S, Guglielmi A, Zacchello G, Cantarutti F (1995) Methylxanthines increase renal calcium excretion in preterm infants. Biol Neonate 68:169–174
Mazkereth R, Laufer J, Jordan S, Pomerance JJ, Boichis H, Reichman B (1997) Effects of theophylline on renal functions in premature infants. Am J Perinatol 14:45–49
Kamitsuka MD, Williams MA, Nyberg DA, Fox KA, Lee DL, Hickok D (1995) Renal calcification: a complication of dexamethasone therapy in preterm infants with bronchopulmonary dysplasia. J Perinatol 15:359–363
Nordin BEC (1959) Assessment of calcium excretion from the urinary calcium/creatinine ratio. Lancet I:368–371
Knapp EL (1947) Factors influencing the urinary excretion of calcium. 1. In normal persons. J Clin Invest 26:182–202
Esbjorner E, Jones IL (1995) Urinary calcium excretion in Swedish children. Acta Paediatr 84:156–159
Hillman LS, Johnson LS, Lee DZ, Vieira NE, Yergey AL (1993) Measurement of true absorption, endogenous fecal excretion, urinary excretion, and retention of calcium in term infants by using a dual-tracer, stable-isotope method. J Pediatr 123:445–456
Abrams SA, Schanler RJ, Yergey AL, Vieira NE, Bronner F (1994) Compartmental analysis of calcium metabolism in very-low-birth-weight infants. Pediatr Res 36:424–428
Hillman LS, Salmons SS, Erickson MM, Hansen JW, Hillman RE, Chesney R (1994) Calciurea and aminoaciduria in very low birth weight infants fed a high-mineral premature formula with varying levels of protein. J Pediatr 125:288–294
Sulyok E, Varga F, Gyory E, Jobst K, Csaba IF (1980) On the mechanism of renal sodium handling in new born infants. Biol Neonate 37:75–79
Gillini F, Maggio L, Romagnoli C, Marrocco G, Tortorolo G (2000) Progression of renal function in preterm neonates with gestational age ≤32 weeks. Pediatr Nephrol 15:119–124
Adelman RD, Solhaug MJ (2000) Calcium. In: Behrman RE, Kliegman RM, Jenson HB (eds) Nelson text book of pediatrics. Saunders, Philadelphia, pp 200–201
Al-dahhan J, Stimmler L, Chantler C, Haycock GB (1988) Urinary creatinine excretion in the newborn. Arch Dis Child 63:398–402
Coulthard MG, Hey EN, Al-dahhan J, Haycock GB (2000) Evaluating urinary flow and solute excretion from urinary creatinine in the first week of life. Arch Dis Child 82:F257–F258
Siegel SR, Hadeed A (1987) Renal handling of calcium in the early new born period. Kidney Int 31:1181–1185
Hoppe B, Hesse A, Neuhaus T, Fanconi S, Blau N, Roth B, Leumann E (1997) Influence of nutrition on urinary oxalate and calcium in preterm and term infants. Pediatr Nephrol 11:687–690
Vileisis RA (1987) Effect of phosphorous intake in total parenteral nutrition infusates in premature neonates. J Pediatr 110:586–590
Hoppe B, Hesse A, Neuhaus T, Fanconi S, Forster I, Blau N, Leumann E (1993) Urinary saturation and nephrocalcinosis in preterm infants: effect of parentaral nutrition. Arch Dis Child 69:299–303
NJ Bishop (1999) Metabolic bone disease. In: Rennie JM, Roberton NRC (eds) Text book of neonatology, 3rd edn. Churchill Livingstone, Edinburgh, pp 1002–1008
Backstrom MC, Kouri T, Kuusela AL, Sievanen H, Koivisto AM, Ikonen RS, Maki M (2000) Bone isoenzyme of serum alkaline phosphatase and serum inorganic phosphate in metabolic bone disease of prematurity. Acta Paediatr 89:867–873
So NP, Osorio AV, Simon SD, Alon US (2001) Normal urinary calcium/creatinine ratios in African-American and Caucasian children. Pediatr Nephrol 16:133–139
Wong GWK, Lam CWK, Kwok MY, Mak TWL (1998) Urinary calcium excretion in Chinese adolescents. J Paediatr Child Health 34:226–228
Mihatsch WA, Muche R, Pohlandt F (1996) The renal phosphate threshold decreases with increasing post menstrual age in very low birth infants. Pediatr Res 40:300–303
McCrory WW, Forman CW, McNamara H, Barnett HL (1952) Renal excretion of inorganic phosphate in newborn infants. J Clin Invest 31:357–366
Acknowledgement
We are grateful to Dr. B. Holland, Consultant Neonatalogist, The Queen Mother’s Hospital, Glasgow for allowing us to collect the clinical and biochemical data of the infants.
Author information
Authors and Affiliations
Corresponding author
Additional information
Editorial comment: this paper describing urinary excretion of calcium and phosphate in preterm infants elicited completely different reactions from the three referees selected to review the manuscript. It is important to establish reference ranges for urinary excretion of these minerals. Nevertheless, it is also important to understand the effect of dietary intake of both calcium and phosphate in defining normative data. It is essential that readers of this article also read the accompanying commentary by Professor Frank Pohlandt.
Rights and permissions
About this article
Cite this article
Aladangady, N., Coen, P.G., White, M.P. et al. Urinary excretion of calcium and phosphate in preterm infants. Pediatr Nephrol 19, 1225–1231 (2004). https://doi.org/10.1007/s00467-004-1574-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-004-1574-1