
Abstract
Background
Laparoscopy-assisted distal gastrectomy (LADG) for gastric cancer has been widely applied; however, its oncologic efficacy has yet been well established. The study aimed to compare the long-term oncologic outcomes of LADG versus open distal gastrectomy (ODG) on gastric cancer.
Methods
The clinicopathologic data of gastric cancer patients who underwent distal gastrectomy with curative intent from October 2004 through September 2014 were included and analyzed in a retrospective cohort. The last follow-up was September 2016.
Results
769 eligible patients (LADG 414 vs. ODG 355) were included in the study. No significant difference was observed between the groups in 5-year DFS (LADG 61.2% vs. ODG 59.1%; p = 0.384) and OS rates (LADG 65.8% vs. ODG 66.3%; p = 0.750). During surgery, though LADG group had longer operating time, the blood loss was less than ODG group. LADG group had faster postoperative recovery course including shorter time to oral intake, ambulation, and discharge time. Postoperative complication rate within 30 days showed no significant difference between the groups (LADG 15.7% vs. ODG 13.0%; p = 0.281). Age over 65 years old, blood loss > 200 ml, postoperative complication, and advanced T and N stage were identified as independent risk factors for DFS and OS.
Conclusions
LADG could yield similar oncologic outcomes compared with ODG in treating distal gastric cancer. However, the findings need to be further confirmed through ongoing prospective randomized controlled trials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Gastric cancer, as the world’s third leading cause for cancer-related deaths, brought more than 300,000 deaths in China annually [1, 2]. Even with the rapid development of multiple treatment modalities [3,4,5], for localized resectable distal gastric cancer, radical distal gastrectomy with sufficient lymphadenectomy still remains the primary treatment.
Laparoscopy-assisted distal gastrectomy (LADG), as a minimally invasive alternative to traditional open distal gastrectomy (ODG), has been applied worldwide in recent years. Reports concerning the safety, feasibility, and oncologic outcomes for LADG have shown that it could yield comparable efficacy with ODG, especially in treatment of early gastric cancer [6, 7]. For locally advanced distal gastric cancer, multicenter prospective trials comparing the oncologic outcomes for LADG with ODG, including CLASS-01 (China), KLASS-02 (Korea), and JLSSG 0901 (Japan) trials are still ongoing. To mention that, the interim report of CLASS-01 has already demonstrated the safety and feasibility of LADG, the long-term oncologic results are still awaited [8]. Before publication of the final results of these randomized controlled trials (RCTs), the efficacy of LADG for distal gastric cancer was primarily supported by retrospective studies [9,10,11]. However, the evidence level of these studies was limited, mainly due to the retrospective design and lack of advanced-stage diseases.
As one of the leading laparoscopic gastrointestinal surgical centers in China, Nanfang Hospital started the first case of laparoscopic distal gastrectomy for distal gastric cancer in 2004. Accordingly, a prospective collected gastric cancer database including clinicopathologic, surgical, and follow-up information was established and adopted as the official database for Chinese Laparoscopic Gastrointestinal Surgery Study (CLASS) group [12]. Through our 10 years’ experience (2004–2014) of performing LADG for distal gastric cancer, we aimed to investigate the long-term oncologic outcomes of LADG with ODG for distal gastric cancer and to further identify the potential risk factors for survival through the study.
Materials and methods
Patient
Between October 2004 and September 2014, 1427 gastric cancer patients who received gastrectomy in our center were identified from the above-mentioned database [12]. Among them, 422 patients who underwent total gastrectomy, 118 who underwent proximal gastrectomy, and one patient who underwent segmental resection were not included in the study. One hundred and seventeen patients with stage IV disease were also excluded. Finally, 769 eligible patients underwent distal gastrectomy (LADG: 414 vs. ODG: 355) with curative intent were subsequently analyzed (Fig. 1).

Flow chart showing study cohort. GC gastric cancer, TG total gastrectomy, PG proximal gastrectomy, SG segmental gastrectomy, LADG laparoscopy-assisted distal gastrectomy, ODG open distal gastrectomy
The study complied with the principles set forth in the Declaration of Helsinki. The data collection protocol was approved by the Ethics Committee of Nanfang Hospital, Southern Medical University. For all patients, full explanations of the advantages, disadvantages, risks, along with possible outcomes and expenses were provided before operations to all the patients. Surgical procedures were determined based on the patients’ own choices. Written informed consent was obtained from all the patients in the study.
Surgical indications and procedures
Preoperative diagnosis was performed by endoscopic biopsy and histological examination. Clinical stage was confirmed by endoscopic ultrasound, enhanced abdominal computed tomography, and positron emission computed tomography if necessary. The 7th edition of AJCC Cancer Staging was applied to determine the stages of the disease [13].
Surgery was attempted for tumors staged T1‒4, with lymph nodes involvement limited to the perigastric tier, and without distant metastasis according to preoperative assessment. After the learning curve of laparoscopic distal gastrectomy with D2 lymphadenectomy was overcome, the indication of LADG was identical with ODG [14]. Open and laparoscopic distal gastrectomies were following the identical oncologic treatment principles. All the surgeries (both open and laparoscopic distal gastrectomies) were performed by the same group of surgeons in our institution. During surgery, D1 or D1+ lymphadenectomy was conducted for early gastric cancer, D2 lymphadenectomy was conducted for advanced gastric cancer. The principles for gastrectomy, lymphadenectomy, and extent of omentectomy were determined according to the gastric cancer treatment guidelines in Japan [15, 16]. The procedure of LADG has been described previously [17]. Reconstruction was performed according to the surgeon’s preference and experience, either Billroth-I gastroduodenostomy, Billroth-II gastrojejunostomy, or Roux-en-Y gastrojejunostomy was adopted during surgery.
Adjuvant chemotherapy and follow-up
The indication for adjuvant chemotherapy was strictly evaluated based on the tumor’s pathologic results and patients’ decision. Despite the changes in first-line chemotherapy regimens for gastric cancer during the past decade, 5-FU-based regimens including XELOX, FOLFOX, and mFOLFOX were applied in T3–4 or any N+ patients. The adjuvant treatment period was 6 months.
All patients were followed up until death or last follow-up in September 2016. The follow-up scheme was 3-month interval during the first 2 years after surgery, and 6-month in the next 3 years, and annually afterward.
Statistical analysis
Data are presented as mean ± standard deviation for continuous variable (for those with non-normal distribution, median and range are shown) and as number (%) for categorical variables. The Student’s t test and Mann–Whitney U test were used to compare continuous variables, and the χ2 test and Fisher’s exact test were used to compare categorical variables, as appropriate. Survival probability was estimated with the Kaplan–Meier method and compared by log-rank test. Risk factors for survival were evaluated by uni- and multivariate analyses using Cox regression models. Variables with statistical significance (p < 0.05) in univariate analysis as well as the critical factor in present analysis, surgical procedure (i.e., LADG or ODG) were entered into the multivariable model and were analyzed by using an “Enter” method. p < 0.05 (two-tailed) was considered statistically significant. The statistical software SPSS version 17.0 for Windows (SPSS, Inc., Chicago, IL, USA) was used for all statistical analyses.
Results
Clinicopathologic characteristics
The clinical and pathologic characteristics of patients are shown in Table 1. There were 276 men in the LADG group and 229 men in the ODG group (p = 0.529). Mean age in the LADG and ODG groups was 56 and 54 years (p = 0.061), with a mean body mass index of 21.88 and 21.68 kg/m2 (p = 0.328). Mean tumor size was 3.27 cm in LADG group and 3.45 cm in ODG group (p = 0.108), respectively, with a median of one metastatic lymph node in both two groups (p = 0.884). There were no significant differences between LADG and ODG groups in terms of previous abdominal surgery, comorbidity, or tumor location. The number of patients in each disease stage was as follows (LADG vs. ODG): stage I, 132 (31.9%) versus 93 (26.2%); stage II, 101 (24.4%) versus 100 (28.2%); stage III, 181 (43.7%) versus 162 (45.6%). TNM stage between LADG and ODG groups did not differ significantly (p = 0.191).
Surgical characteristic, postoperative recovery courses, and complications
The surgical and postoperative outcomes are presented in Table 2. The median operating time of LADG group was longer than ODG group (202 vs. 170 min; p < 0.001). However, the median estimated blood loss in LADG group was less than ODG group (100 vs. 200 ml; p < 0.001). Also, less patients needing blood transfusion during operation was observed in LADG group, compared with ODG group (3.1 vs. 9.0%; p < 0.001). There was no significant difference between the two groups in terms of length of proximal resection margin. No positive resection margin was observed in all patients. Two groups showed different distributions in reconstruction (p < 0.001), with more Billroth-I observed in LADG group (66.4%) and more Billroth-II in ODG group (60.8%). Lymphadenectomy and the number of lymph nodes retrieved were similar between the groups. Among patients in LADG group, 13 (3.1%) experienced conversion to open surgery due to bulky tumor (eight patients), technical difficulties (two patients), severe adhesion (one patient), uncontrolled bleeding (one patient), and intolerance to pneumoperitoneum (one patient). In term of recovery course, time to first flatus, first liquid intake, first soft diet and ambulation, and postoperative hospital stay were significantly shorter in LADG group than ODG group (all p < 0.001).
Postoperative morbidity and mortality are listed in Table 3. A total of 81 postoperative complications occurred in 65 (15.7%) patients in LADG group and 56 complications in 46 (13.0%) patients in ODG group. There was no significant difference in total number of patients occurring complications between the groups (p = 0.281). Among all the complications (anastomotic leakage, wound problem, intraabdominal bleeding, intraabdominal abscess, ileus, intraabdominal lymphorrhagia, gastroparesis, pancreatic fistula, cholecystitis, pulmonary, cardio-cerebrovascular and renal complication, and others), no significant difference was observed between the groups. According to the Clavien–Dindo classification of surgical complications [18], the severity of complications was similar between the two groups (p = 0.950). One patient in ODG group died due to severe pancreatitis.
Long-term oncologic outcomes
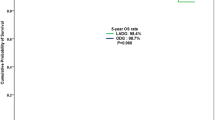
The patients were followed up for a median of 45 months (range 1–146 months). The 5-year DFS rate was 61.2% (95% confidence interval [CI] 55.2‒67.1%) in LADG group and 59.1% (95% CI 53.6‒64.6%) in ODG group, with no significant difference between the groups (hazard ratio [HR] 1.11; 95% CI 0.88–1.41; p = 0.384) (Fig. 2A). Both LADG and ODG groups yielded a similar 5-year OS rate [65.8% (95% CI 59.9‒71.7%) vs. 66.3% (95% CI 61.0‒71.6%); HR 1.04, (95% CI 0.81‒1.35); p = 0.750] (Fig. 2B). When stratified by tumor stage, patients yielded similar 5-year DFS and OS rates between the two groups in each stage (Fig. 2C, D).

Comparison of cumulative survival rates for LADG and ODG groups in terms of A 5-year disease-free survival, B 5-year overall survival, and C 5-year disease-free survival according to tumor stages and D 5-year overall survival according to tumor stages
Risk factors for survival
Uni- and multivariate analyses of risk factors for survival are presented in Table 4. Univariate analyses revealed that age over 65 years, bearing more than one comorbidity, tumor located at the lower third, tumor size > 4.0 cm, estimated blood loss over 200 ml, intraoperative blood transfusion, postoperative complication, and advanced tumor T and N stage were risk factors for either DFS or OS. Furthermore, multivariate analyses indicated that age over 65 years, estimated blood loss > 200 ml, postoperative complication, and advanced tumor T and N stage were independent risk factors for DFS and OS. Notably, LADG was not identified as a risk factor for both OS and DFS, compared with ODG.
Discussion
Since its introduction for early gastric cancer by Kitano et al. [19], LADG has gradually gained popularity in the management of distal gastric cancer in East Asia [20,21,22]. After the first report of LADG for distal gastric cancer in China in 2000 [23], our center also started LADG for early distal gastric cancer in 2004. From 2004 to 2014, with the accumulation of laparoscopic surgical experience and improvement in surgical techniques, the indications of LADG have gradually been extended from early-staged disease to resectable locally advanced diseases. To date, some of the prospective results about LADG for early gastric cancer including short- and long-term outcomes have demonstrated its comparable efficacy with ODG [6, 7, 24]; however, RCTs relating LADG versus ODG for advanced gastric cancer are still lacking, especially from the long-term aspects [25]. There were also a few retrospective reports on the laparoscopic distal gastrectomy with lymphadenectomy in treating gastric cancer, and these reports came to similar conclusion of our study [26, 27]. Since the final results of the large-scale RCTs comparing LADG and ODG for locally advanced gastric cancer are still being awaited, herein, we retrospectively analyzed our center’s 10-year data of LADG for gastric cancer with emphasis on the long-term oncologic outcomes.
In this study, there were no significant differences in 5-year DFS and OS between LADG and ODG groups. While stratified by stages, the survival rates for stage I, II, and III were also similar between the groups, which might help support that LADG could yield comparable oncologic outcomes with ODG for distal gastric cancer. Since different from other studies, in our analyzed cohorts, the majority of patients were with advanced-staged diseases, it is inappropriate to directly compare our 5-year survival rates with others’. For example, the 5-year OS in our study was 65.8% in LADG group; however, in a Japanese study, where more clinical stage I patients (243 out of 278) were included, the 5-year OS was 85.6% [28]. However, when analyzing by stages, our survival data of stage I, II, and III diseases in LADG and ODG were similar with other reports [7, 9, 10, 29].
In our study, we found that postoperative complication and advanced tumor T and N stage were independent risk factors for both DFS and OS, which have also been demonstrated in other studies [30,31,32]. Also, age over 65 years was identified as risk factor for survival in our study, which was similar with results from two recent Korean studies [33, 34]. By explanation, a poorer prognosis in elderly patients might be partly attributed to the weaker host-defense mechanisms [35, 36]. In addition, we found that intraoperative blood loss over 200 ml was also a risk factor for survival. In Mizuno et al.’s [37] and Ishino et al.’s [38] studies, they found that excessive intraoperative blood loss was associated with poorer prognosis. Although the mechanisms of negative effect of excessive blood loss on long-term outcomes are not fully understood, but evidence showed that excessive blood loss may, by itself, impair immunity against cancer cells and nutritional status via loss of plasma constituents [39], which might be associated with poor survival. Notably in our study, the surgical procedure of LADG versus ODG was not a risk factor for DFS or OS, which might indicate that LADG was an oncologically efficient treatment alternative to ODG in distal gastric cancer.
Regarding postoperative complication, a total rate of postoperative complication after LADG reported by other authors range between 11.0 and 19.9% [6, 8, 22, 34, 40]. In our study, the postoperative complication rate was 15.7% in LADG group and 13.0% in ODG group. Complication rate and severity were both similar between the groups, hence, LADG could be equally safe and feasible with ODG. In our cohort, no matter in LADG group or ODG group, the most common complication was pulmonary infection after surgery. This phenomenon was identical with CLASS-01’s interim report [8]. The reason might be that after upper abdominal surgeries, reduced diaphragmatic activity and microatelectasis would cause decreased pulmonary function, which eventually resulted in pulmonary infection [41, 42].
For surgical findings and recovery course, our study demonstrated similar minimally invasive benefits including less blood loss, shorter times of recovery (ambulation, first flatus, oral intake, and hospital stay) as with other studies [8, 20, 24, 43, 44]. For reconstruction after gastrectomy, in LADG group, Billroth-I reconstruction was preferred by surgeons while more Billroth-II reconstruction was adopted by open surgeons. This was mainly due to the different distributions of T stage tumors between the groups. Usually, in our center, Billroth-I reconstruction was preferred in T1 stage tumors before 2012 as long as sufficient resection margin could be ascertained. However, since 2012, after observation of three cases of recurrent tumor at the anastomosis after Billroth-I reconstruction, the difficulty of performing second surgery reminded us of modifying our reconstruction preference after distal gastrectomy. Ever since then, Billroth-II or Roux-en-Y reconstruction was adopted in either LADG of ODG.
Our results have several limitations. First, its retrospective design has the weakness of being observational or non-experimental in nature. Second, the imbalance of T and N stage between the groups might influence the long-term outcomes though the TNM stage distribution was similar. Third, during a decade’s period, the changes of treatment concepts, surgical preferences might also create bias in the analyses. Despite these limitations, our study evaluating our 10 years’ experience of LADG in views of long-term oncologic outcomes, would represent the development of Chinese laparoscopic gastric cancer surgery during the past decade, since our center is one of the first centers in China to perform LADG for distal gastric cancer. In conclusion, the findings of this study might suggest comparable safety and oncologic efficacy of LADG in treating distal gastrectomy in experienced centers. However, the long-term multicenter prospective randomized controlled trials would still be awaited.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A (2015) Global cancer statistics, 2012. CA Cancer J Clin 65(2):87–108
Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J (2016) Cancer statistics in China, 2015. CA Cancer J Clin 66(2):115–132
Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T, Aprile G, Kulikov E, Hill J, Lehle M, Ruschoff J, Kang YK, To GATI (2010) Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet 376(9742):687–697
Ng J, Lee P (2017) The role of radiotherapy in localized esophageal and gastric cancer. Hematol Oncol Clin 31(3):453–468
Al-Batran SE, Lorenzen S (2017) Management of locally advanced gastroesophageal cancer: still a multidisciplinary global challenge? Hematol Oncol Clin 31(3):441–452
Kim W, Kim HH, Han SU, Kim MC, Hyung WJ, Ryu SW, Cho GS, Kim CY, Yang HK, Park DJ, Song KY, Lee SI, Ryu SY, Lee JH, Lee HJ, Korean Laparo-endoscopic Gastrointestinal Surgery Study G (2016) Decreased morbidity of laparoscopic distal gastrectomy compared with open distal gastrectomy for stage i gastric cancer: short-term outcomes from a Multicenter Randomized Controlled Trial (KLASS-01). Ann Surg 263(1):28–35
Kim HH, Han SU, Kim MC, Kim W, Lee HJ, Ryu SW, Cho GS, Kim CY, Yang HK, Park DJ, Song KY, Lee SI, Ryu SY, Lee JH, Hyung WJ, Group KL-eGSS (2016) Long-term outcomes of laparoscopic distal gastrectomy compared with open distal gastrectomy for clinical stage I gastric adenocarcinoma (KLASS-01): a multi-center prospective randomized controlled trial. J Clin Oncol 34(15_suppl):4060–4060
Hu Y, Huang C, Sun Y, Su X, Cao H, Hu J, Xue Y, Suo J, Tao K, He X, Wei H, Ying M, Hu W, Du X, Chen P, Liu H, Zheng C, Liu F, Yu J, Li Z, Zhao G, Chen X, Wang K, Li P, Xing J, Li G (2016) Morbidity and mortality of laparoscopic versus open D2 distal gastrectomy for advanced gastric cancer: a Randomized Controlled Trial. J Clin Oncol 34(12):1350–1357
Honda M, Hiki N, Kinoshita T, Yabusaki H, Abe T, Nunobe S, Terada M, Matsuki A, Sunagawa H, Aizawa M, Healy MA, Iwasaki M, Furukawa TA (2016) Long-term outcomes of laparoscopic versus open surgery for clinical stage I gastric cancer: The LOC-1 Study. Ann Surg 264(2):214–222
Kim HH, Han SU, Kim MC, Hyung WJ, Kim W, Lee HJ, Ryu SW, Cho GS, Song KY, Ryu SY (2014) Long-term results of laparoscopic gastrectomy for gastric cancer: a large-scale case-control and case-matched Korean multicenter study. J Clin Oncol 32(7):627–633
Hu Y, Ying M, Huang C, Wei H, Jiang Z, Peng X, Hu J, Du X, Wang B, Lin F, Xu J, Dong G, Mou T, Li G, Chinese Laparoscopic Gastrointestinal Surgery Study G (2014) Oncologic outcomes of laparoscopy-assisted gastrectomy for advanced gastric cancer: a large-scale multicenter retrospective cohort study from China. Surg Endosc 28(7):2048–2056
Hu YF, Yu J, Zhang C, Wang YN, Cheng X, Huang F, Li GX (2010) Development and implementation of a clinical data mining system for gastric cancer surgery. Chin J Gastrointest Surg 13(7):510–515
Washington K (2010) 7th edition of the AJCC cancer staging manual: stomach. Ann Surg Oncol 17(12):3077–3079
Hu YF, Yu J, Wang YN, Zhang C, Cheng X, Li GX (2010) Learning curve of laparoscopic D2 gastrectomy for gastric cancer. J South Med Univ 30(5):1095–1098
Nakajima T (2002) Gastric cancer treatment guidelines in Japan. Gastric Cancer 5(1):1–5
Japanese Gastric Cancer A (1998) Japanese classification of gastric carcinoma—2nd English edition. Gastric Cancer 1(1):10–24
Li GX, Zhang C, Yu J, Wang YN, Hu YF (2010) A new order of D2 lymphadenectomy in laparoscopic gastrectomy for cancer: live anatomy-based dissection. Minim Invasive Ther Allied Technol 19(6):355–363
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Kitano S, Iso Y, Moriyama M, Sugimachi K (1994) Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc 4(2):146–148
Huscher CG, Mingoli A, Sgarzini G, Sansonetti A, Di Paola M, Recher A, Ponzano C (2005) Laparoscopic versus open subtotal gastrectomy for distal gastric cancer: five-year results of a randomized prospective trial. Ann Surg 241(2):232–237
Katai H, Sasako M, Fukuda H, Nakamura K, Hiki N, Saka M, Yamaue H, Yoshikawa T, Kojima K, Group JGCSS (2010) Safety and feasibility of laparoscopy-assisted distal gastrectomy with suprapancreatic nodal dissection for clinical stage I gastric cancer: a multicenter phase II trial (JCOG 0703). Gastric Cancer 13(4):238–244
Kim HH, Hyung WJ, Cho GS, Kim MC, Han SU, Kim W, Ryu SW, Lee HJ, Song KY (2010) Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: an interim report–a phase III multicenter, prospective, randomized trial (KLASS Trial). Ann Surg 251(3):417–420
Lan H, Zhu N, Lan Y, Jin K, Teng L (2015) Laparoscopic gastrectomy for gastric cancer in China: an overview. Hepatogastroenterology 62(137):234–239
Kim YW, Baik YH, Yun YH, Nam BH, Kim DH, Choi IJ, Bae JM (2008) Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg 248(5):721–727
Li G, Hu Y, Liu H (2015) Current status of randomized controlled trials for laparoscopic gastric surgery for gastric cancer in China. Asian J Endosc Surg 8(3):263–267
Hao YX, Yu PW, Qian F, Zhao YL, Shi Y, Tang B, Zeng DZ, Zhang C (2016) Comparison of laparoscopy-assisted and open radical gastrectomy for advanced gastric cancer: a retrospective study in a single minimally invasive surgery center. Medicine (Baltimore) 95(25):e3936
Zhao XF, Jeong O, Jung MR, Ryu SY, Park YK (2013) A propensity score-matched case-control comparative study of laparoscopic and open extended (D2) lymph node dissection for distal gastric carcinoma. Surg Endosc 27(8):2792–280028
Sugita H, Kojima K, Inokuchi M, Kato K (2015) Long-term outcomes of laparoscopic gastrectomy for gastric cancer. J Surg Res 193(1):190–195
Zhang Y, Qi F, Jiang Y, Zhai H, Ji Y (2015) Long-term follow-up after laparoscopic versus open distal gastrectomy for advanced gastric cancer. Int J Clin Exp Med 8(8):13564–13570
Li QG, Li P, Tang D, Chen J, Wang DR (2013) Impact of postoperative complications on long-term survival after radical resection for gastric cancer. World J Gastroenterol 19(25):4060–4065
Tokunaga M, Tanizawa Y, Bando E, Kawamura T, Terashima M (2013) Poor survival rate in patients with postoperative intra-abdominal infectious complications following curative gastrectomy for gastric cancer. Ann Surg Oncol 20(5):1575–1583
Marrelli D, Morgagni P, de Manzoni G, Coniglio A, Marchet A, Saragoni L, Tiberio G, Roviello F, Italian Research Group for Gastric C (2012) Prognostic value of the 7th AJCC/UICC TNM classification of noncardia gastric cancer: analysis of a large series from specialized Western centers. Ann Surg 255(3):486–491
Pak KH, Hyung WJ, Son T, Obama K, Woo Y, Kim HI, An JY, Kim JW, Cheong JH, Choi SH, Noh SH (2012) Long-term oncologic outcomes of 714 consecutive laparoscopic gastrectomies for gastric cancer: results from the 7-year experience of a single institute. Surg Endosc 26(1):130–136
Park DJ, Han SU, Hyung WJ, Kim MC, Kim W, Ryu SY, Ryu SW, Song KY, Lee HJ, Cho GS, Kim HH, Korean Laparoscopic Gastrointestinal Surgery Study G (2012) Long-term outcomes after laparoscopy-assisted gastrectomy for advanced gastric cancer: a large-scale multicenter retrospective study. Surg Endosc 26(6):1548–1553
Park HA, Park SH, Cho SI, Jang YJ, Kim JH, Park SS, Mok YJ, Kim CS (2013) Impact of age and comorbidity on the short-term surgical outcome after laparoscopy-assisted distal gastrectomy for adenocarcinoma. Am Surg 79(1):40–48
Kim EJ, Seo KW, Yoon KY (2012) Laparoscopy-assisted distal gastrectomy for early gastric cancer in the elderly. J Gastric Cancer 12(4):232–236
Mizuno A, Kanda M, Kobayashi D, Tanaka C, Iwata N, Yamada S, Fujii T, Nakayama G, Sugimoto H, Koike M, Fujiwara M, Kodera Y (2016) Adverse effects of intraoperative blood loss on long-term outcomes after curative gastrectomy of patients with stage II/III gastric cancer. Dig Surg 33(2):121–128
Ishino Y, Saigusa S, Ohi M, Yasuda H, Tanaka K, Toiyama Y, Mohri Y, Kusunoki M (2014) Preoperative C-reactive protein and operative blood loss predict poor prognosis in patients with gastric cancer after laparoscopy-assisted gastrectomy. Asian J Endosc Surg 7(4):287–294
Morner ME, Gunnarsson U, Jestin P, Svanfeldt M (2012) The importance of blood loss during colon cancer surgery for long-term survival: an epidemiological study based on a population based register. Ann Surg 255(6):1126–1128
Yoo HM, Lee HH, Shim JH, Jeon HM, Park CH, Kim JG, Song KY (2011) Long-term outcomes and survival after laparoscopy-assisted distal gastrectomy for gastric cancer: three-year survival analysis of a single-center experience in Korea. J Surg Oncol 104(5):511–515
Inokuchi M, Kojima K, Kato K, Sugita H, Sugihara K (2014) Risk factors for post-operative pulmonary complications after gastrectomy for gastric cancer. Surg Infect (Larchmt) 15(3):314–321
Kanat F, Golcuk A, Teke T, Golcuk M (2007) Risk factors for postoperative pulmonary complications in upper abdominal surgery. ANZ J Surg 77(3):135–141
Kitano S, Shiraishi N, Fujii K, Yasuda K, Inomata M, Adachi Y (2002) A randomized controlled trial comparing open vs laparoscopy-assisted distal gastrectomy for the treatment of early gastric cancer: an interim report. Surgery 131(1 Suppl)):S306–S311
Hayashi H, Ochiai T, Shimada H, Gunji Y (2005) Prospective randomized study of open versus laparoscopy-assisted distal gastrectomy with extraperigastric lymph node dissection for early gastric cancer. Surg Endosc 19(9):1172–1176
Acknowledgements
This work was supported by the grants from the State’s Key Project of Research and Development Plan (2017YFC0108300, 2017YFC0108301), National Natural Science Foundation of China (81672446), Guangdong Provincial Science and Technology Key Project (2014A020215014), Research Fund of Public Welfare in the Health Industry, the National Health and Family Planning Commission of China (201402015), the Southern Medical University Clinical Research Start-Up Project (LC2016ZD003), Guangzhou Science and Technology Project (201400000004-5), and the Key Clinical Specialty Discipline Construction Program ([2011]170).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Disclosures
Drs. Hao Wang, Tingyu Mou, Hao Chen, Yanfeng Hu, Tian Lin, Tuanjie Li, Jiang Yu, Hao Liu, and Guoxin Li have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Wang, H., Mou, T., Chen, H. et al. Long-term outcomes of laparoscopy-assisted distal gastrectomy versus open distal gastrectomy for gastric cancer: a 10-year single-institution experience. Surg Endosc 33, 135–144 (2019). https://doi.org/10.1007/s00464-018-6283-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-018-6283-0