
Abstract
Background
Endoscopic submucosal dissection (ESD) for various colorectal neoplasms is more technically difficult than gastric ESD. We evaluated treatment outcomes and the learning curve for colorectal ESD of laterally spreading tumors (LSTs) based on the experience of a single endoscopist.
Methods
We included 93 colorectal ESD procedures for colorectal LST that were performed between March 2009 and June 2012 by a single experienced endoscopist who previously performed hundreds of cases of gastric ESD. The cases were grouped chronologically into three periods by multi-dimensional analyses. For procedure time, the learning curve was analyzed using the moving average method, and for complication, the learning curve was analyzed using cumulative sum (cusum) method.
Results
The median procedure time for 93 colorectal ESD was 45 min, and the rates of en bloc resection and R0 resection were 89.25 and 83.87 %. When results were compared among three periods in order to determine the learning curve, the procedure time and en bloc resection rates were not significantly different. However, the procedure proficiency (about 0.16 cm2/min) was significantly faster during the second period, after about 25 cases of colorectal ESD. In the third period (about 50 cases), the number and rate of en bloc resection (over 90 %) reached the same as that of en bloc R0 resection. When comparing outcomes based on LST subtype, the procedure proficiency of LST-granular type (LST-G) was significantly faster than that of LST-non granular type (LST-NG) (LST-NG, 0.072 cm2/min; LST-G, 0.157 cm2/min; p = 0.01).
Conclusion
Endoscopists fully experienced in gastric ESD need a relatively short learning period for colorectal ESD in terms of procedure time and complication. However, approximately 50 cases might be needed to acquire an adequate skill of colorectal ESD for LST in an experienced gastric ESD endoscopist. Colorectal ESD for LST-NG seems to have higher technical difficulty and a longer learning curve than LST-G.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Most colorectal adenomas smaller than 20 mm can be resected en bloc with a conventional endoscopic mucosal resection (EMR) technique. However, when the lesion is larger than 20 mm, en bloc resection becomes difficult. Larger tumors are more difficult to be resected en bloc.
Endoscopic submucosal dissection (ESD) is used to treat premalignant and early gastrointestinal cancers. ESD enables en bloc resection of large colorectal neoplasms, which are difficult to remove by EMR, allowing more accurate histological evaluation of resected specimens and reducing the risk of recurrence [1–3]. However, this procedure requires a high level of endoscopic skill to overcome the high risk of complication and long procedure time. Moreover, colorectal ESD is a more technically difficult procedure than gastric ESD, due to the thinner wall and higher perforation. Therefore, the learning curve is an important aspect of quality assurance and the rate of proficiency acquisition should be quantified. Few studies have described the learning curve for colorectal ESD. Most previous studies used only simple chronological grouping. No published reports detail a multi-dimensional assessment of the learning curve, including procedure time and complication rates.
The aims of this study were to evaluate the clinical outcomes of ESD and to describe the learning curve for ESD of the colon, based on the analysis of a single endoscopist’s experience, using multi-dimensional assessment.
Patients and methods
Patients
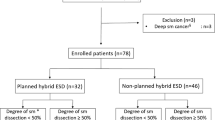
We analyzed 93 consecutive colorectal ESD procedures (47 males, median age 63 years) performed by a single experienced endoscopist at Gangnam Severance Hospital in Seoul, Korea, between March 2009 and June 2012. The single experienced endoscopist (Youn) had performed approximately 2000 colonoscopies, 500 colonic mucosal resections and 300 upper gastrointestinal ESDs before beginning colorectal ESD in 2009. We retrospectively reviewed clinical outcomes for 93 consecutive patients. This retrospective review was approved by the Institutional Review Board of Severance Hospital. All of the patients provided written informed consent for the colorectal ESD procedure.
Lesions
Lateral spreading tumors (LSTs) are formally defined as lesions larger than 10 mm, and this study was restricted to LST lesions, which are difficult to remove en bloc using conventional EMR. The general indications for colorectal ESD in this study were LSTs larger than 20 mm and lesions with fibrosis due to multiple previous endoscopic biopsies or incomplete resection. ESD was not used in cases where lesions were highly suspected to have deep submucosal cancer invasion due to deeply depressed surfaces or folds converging toward the tumor. The LST lesions were divided into two subtypes based on the endoscopic finding: LST-granular type (LST-G) and LST-non granular type (LST-NG), according to the classification by Kudo [4, 5].
ESD procedure
We used a pediatric-type colonoscope with a built-in water jet system (PCF-Q260JI; Olympus Optical Co.) and an attachment. A dual knife (KD-630 L; Olympus Medical System Co.) was used as the main electrosurgical knife, and a hook knife (KD-620 QR; Olympus) was used in combination during difficult situations. 10 % glycerol and 5 % fructose in a normal saline solution mixed with hyaluronic acid were used as submucosal fluid cushions to lift the lesions sufficiently. Lesion margins of LST were delineated before ESD using indigo carmine spray. After submucosal injection, the mucosal layer around the lesion (3–5 mm outside lesion edge) was incised with the knife and the submucosal layer was dissected. An additional submucosal injection was repeated as needed. A carbon dioxide (CO2) insufflation system was used instead of air insufflations. In all periods, we used a high-frequency generator unit (VIO300D; Erbe Elektromedizin, Germany). ESD was performed under conscious sedation using intravenous midazolam and/or propofol with continued monitoring of electrocardiography and oxygen saturation.
Definitions
Resection
Resections were evaluated according to the presence of tumor cells at the margin of the resected specimen and were defined as follows: R0 resection, all margins were negative for tumor; and R1 resection, tumor extended to the lateral margin or basal margin. If ESD could not be completed en bloc in one piece, it was classified as an R1 resection.
Procedure time and proficiency
The procedure time was defined as the beginning of the local injection to the end of procedure, and the procedure proficiency was calculated by dividing the procedure time by the area of the resected specimen (cm2/min). We regarded the area of the resected specimen to be an oval shape, and the area was calculated as follows: 3.14 × 0.25 × long axis × minor axis.
Period
To confirm the learning curve for colorectal ESD, time periods were sorted by procedure time and complication. We used a moving average method to sort the periods by procedure time and found that 25th case and 58th case were cutoff points (Fig. 1). A five-case moving average was used: 1st–24th moving average is increasing than overall average, 58th–93rd moving average is decreasing than overall average, and 25th–57th moving average is unstable. Based on trend of moving average, we determined the optimal cutoff point. We used the cumulative sum (cusum) method to sort the periods by complication and found that the 28th case and 56th case were cutoff points (Fig. 2). Cusum is a technique for analysis of dichotomous outcome, to chart the changes in the failure rate of the complication. Cusum was defined as ∑(X i − X 0), where X i is individual attempt and X 0 was the reference or target value for the procedure, with X i = 1 for failure (complication) and X i = 0 for success (no complication). The X 0 for conversion rate was set at 0.1, reflecting a target conversion rate of 10 %. Positive slope means failure, and negative slope means success. On the other hand, 28th–55th cusum’s slope is gradually decreasing, and 1st–27th and 56th–93rd cusum’s slope show fluctuation. In particular, 1st–27th has a strong tendency to increase and 56th–93rd has a strong tendency to decrease.

Time taken to perform colorectal endoscopic submucosal dissection as a function of the number of cases. The moving average method was used to determine changes in procedure times

Complications of colorectal endoscopic submucosal dissection as a function of the number of cases. The cusum method was used to determine changes in complication rates
Based on the above three periods, which were assorted by procedure time and complication rates, respectively, we analyzed the main outcome parameters.
Main outcome parameters
We retrospectively evaluated data including LST type, histology, en bloc resection rate, en bloc R0 resection rate, pathologic diameter, resected specimen diameter, procedure time, procedure proficiency, complication rate and hospital stay period. The main complications were bleeding and perforation, which included during and after ESD. Bleeding was defined as massive bleeding requiring a colonoscopy due to hematochezia. Perforation was defined as overt perforation and microperforation, which was a partial defect of the muscular layer.
Statistical analysis
Categorical variables were compared by Chi-squared or Fisher’s exact tests. Continuous variables are presented as mean (±SD) or median (interquartile range or range) and were compared using an independent two sample t test or the Mann–Whitney U test. p values <0.05 were considered statistically significant. All statistical analyses were performed using the statistical software SAS (version 9.2, Institute, Cary, NC, USA).
Results
General outcomes of colorectal ESD procedures
Ninety-three consecutive patients with 93 lesions were enrolled in this study. Table 1 shows the clinicopathological features and treatment outcomes of colorectal ESD. The median patient age was 65 years (range 38–87 years). The patient population comprised 47 men (50.54 %) and 46 women (49.46 %). Lesions were located in the rectum in 31 patients (33.33 %), and the sigmoid colon in 22 (23.66 %) and the other in 40 (43.01 %) were more proximal. Twenty-two LST-NG (23.66 %) and 71 LST-G (76.34 %) were removed by ESD. The median pathologic diameter was 27 mm (20–35), and the median resected specimen diameter was 30 mm (25–40). The median procedure time was 45 min (30–80), and procedure proficiency was 0.13 cm2/min (0.07–0.263). The median hospital admission stay was 3 days (2–5). The rate of en bloc resection was 89.25 % (83/93). The rate of en bloc R0 resection was 83.87 % (78/93). Overt perforation and microperforation occurred in two (2.15 %) and four lesions (4.3 %). All perforations were recognized during the procedure and were successfully treated by endoscopic clipping and antibiotics. There were no bleeding complications.
Learning curve analysis
To determine the learning curve in colon ESD skill over time, the cases were grouped into three periods by the moving average method and the cusum method. Based on procedure time by the moving average method, we divided 93 colorectal ESD procedures into the first period (1–24), second period (25–57) and third period (58–93) (Table 2). The rates of en bloc resection were 83.33 % (20/24), 87.88 % (29/33) and 94.44 % (34/36), respectively. The rates of en bloc R0 resection were 75 % (18/24), 78.79 % (26/33) and 94.44 % (34/36), respectively. The rates of en bloc resection and en bloc R0 resection tended to increase during the third period, though this was not statistically significant. Procedure time during the periods was 58, 42 and 44.5 min, respectively. The rate of en bloc resection, rate of en bloc R0 resection and procedure time showed no significant differences between the three periods. However, pathologic diameter and resected specimen diameter increased significantly after the second period (p = 0.015 and p = 0.032). The proficiencies in the first, second and third periods were 0.07, 0.159 and 0.202 (cm2/min), respectively. Proficiency in the second period was significantly faster than that of the first period (p < 0.001). However, there were no statistically significant differences between the periods with regard to other factors.
Based on complications according to the cusum method, we divided 93 colorectal ESD procedures into first period (1–27), second period (28–55), and third period (56–93) (Table 3). The rates of en bloc resection were 85.19 % (23/27), 85.71 % (24/28) and 94.74 % (36/38), respectively. The rates of en bloc R0 resection were 74.07 % (20/27), 82.14% (23/28) and 92.11 % (35/38), respectively. Similarly, the rates of en bloc resection and en bloc R0 resection were higher during the third period, though this was not statistically significant. Procedure times were 44, 46 and 44.5 min, respectively. Similarly, pathologic diameter, resected specimen diameter and procedure proficiencies increased significantly after the second period (p = 0.011, p = 0.014 and p < 0.001). There were no statistically significant differences between the periods with regard to other factors.
We also analyzed the procedure data through the LST type (Table 4). LST-NG often had smaller tumors and a smaller resected specimen diameter than LST-G (p = 0.004 and p = 0.024). Though the procedure time did not differ between LST-NG and LST-G, the median procedure proficiency did (LST-NG, 0.072 cm2/min; LST-G, 0.157 cm2/min; p = 0.01). Other factors including the en bloc resection rate and the en bloc R0 resection rate were similar between the groups.
Discussion
Laterally spreading tumor (LST) is a convenient name for larger (10 mm) sessile or flat lesions extending laterally along the colon wall, corresponding to the macroscopic type Is and IIa lesions in the Paris classification [6]. In one of the most well-known classification systems, Kudo et al. [4, 5] reported that the LST-non granular type (LST-NG) and LST-granular type (LST-G) are two major subtypes. LST is a flat or depressed neoplasm that is a risk factor for the development of advanced colon cancer [7, 8]. Endoscopic mucosal resection (EMR) was the standard endoscopic treatment for removing such lesions. With EMR, en bloc resection is restricted to lesions less than 20 mm. Therefore, endoscopic piecemeal EMR is often applied for lesions larger than 20 mm, which may lead to incomplete removal, difficult histological assessment and an increased risk of local recurrence [9–11].
Colorectal ESD was developed for en bloc resection of large colorectal tumors. Colon ESD has increased in popularity as a treatment approach for endoscopic resection in Korea and Japan due to its high cure rate and tolerable complication rate [12]. However, colorectal ESD is still technically difficult and time-consuming and can be accompanied by significant complications [1–3, 12]. Therefore, it is important to identify the learning curve for acquiring proficiency in colorectal ESD. Some studies analyzed learning curves for ESD in the treatment of early gastric cancers [13–16]. However, the learning curve for colorectal ESD was evaluated in several studies. Hotta et al. demonstrated that approximately 40 procedures are enough for achieving the procedure time and perforation rate. However, approximately 80 procedures should be carried out to acquire ESD skills adequate for consistency for LST [17]. Sakamoto et al. [18] found that colon ESD can be performed safely and independently after experience with ≥30 cases. Most previous studies used a simple chronological grouping analysis method. To the best of our knowledge, the present study is the first report evaluating the learning curve for ESD of colorectal tumors by multi-dimensional assessment, including procedure time and complication rates.
This study clearly demonstrated that colorectal ESD was performed safely and efficiently by an endoscopist experienced in gastric ESD. Previous studies showed that when colorectal ESD was attempted in referral centers, the result showed a high en bloc resection rate and low recurrence rates [2, 19–21]. Perforation rates varied in these studies, ranging from 1.4 to 10 % [2, 19–21]. Based on previous studies [2, 20–23], Hotta et al. [17] set target levels for en bloc resection rates, en bloc R0 resection rates and perforation rates at 90, 80 and 5 %, respectively. In our study, we showed the target en bloc, R0 resection rate and perforation rate approximately.
There were no significant differences in procedure time, en bloc resection rate, en bloc R0 resection rate and complication rate among the three periods. Pathologic diameter, resected specimen diameter and procedure proficiency differed significantly. The tumor size and resected specimen became larger, and the procedure speed became faster after the second period. We used procedure proficiency (area of resected specimen per procedure time; cm2/min) to evaluate the learning curve. This measurement eliminated confounding differences in colon LST size. Using this measurement, only the procedure proficiency significantly improved after about 25 cases. This result may be due to the endoscopist, who is fully experienced in gastric ESD; in addition, Korean endoscopists have many chances to perform ESD on the stomach due to the high incidence of gastric cancer in Korea. In the third period, the number and rate of en bloc resection reached the same as that of en bloc R0 resection and is greater than the other two periods. Considering these results, about 50 procedures may be needful to acquire adequate colorectal ESD skills.
The outcomes in terms of procedure time, en bloc resection, en bloc R0 resection and complications of ESD for LST-NG were similar to that of LST-G, and ESD is an effective treatment for LST-NG. However, the technical difficulty was higher for LST-NG because the procedure proficiency was slower. LST-NG lesions are small, light and thin and do not move away from the muscle layer, making resection and dissection of the mucosal flap more difficult. Second, LST-NG lesions have a thin submucosal layer which can be easily affected by fibrosis due to a previous biopsy [9, 24].
There are several limitations to our study. It was retrospective, single operator and a single-center analysis with small samples. Further investigations with a large number of colon ESD procedures will be necessary to confirm our results.
Based on our analysis of the learning curve, endoscopists who are fully experienced in gastric ESD need a short learning period for colorectal ESD in terms of procedure time, en bloc resection, en bloc R0 resection and complication rates. Procedure proficiency can significantly improve after about 25 cases of colorectal ESD, which estimates the number of cases that might be needed to acquire technical skills for colorectal ESD for LST. For reaching en bloc resection and en bloc R0 resection enough, about 50 procedures might be needed to acquire technical skills for colorectal ESD for LST. ESD is an effective treatment modality for LST-NG. However, the degree of technical difficulty is higher for LST-NG than for LST-G. ESD for LST-NG should be possibly performed by endoscopists with significant experience in colorectal ESD.
References
Uraoka T, Kawahara Y, Kato J, Saito Y, Yamamoto K (2009) Endoscopic submucosal dissection in the colorectum: present status and future prospects. Dig Endosc 21(Suppl 1):S13–S16
Tanaka S, Oka S, Kaneko I, Hirata M, Mouri R, Kanao H, Yoshida S, Chayama K (2007) Endoscopic submucosal dissection for colorectal neoplasia: possibility of standardization. Gastrointest Endosc 66(1):100–107
Saito Y, Sakamoto T, Fukunaga S, Nakajima T, Kiriyama S, Matsuda T (2009) Endoscopic submucosal dissection (ESD) for colorectal tumors. Dig Endosc 21(Suppl 1):S7–S12
Kudo S (1993) Endoscopic mucosal resection of flat and depressed types of early colorectal cancer. Endoscopy 25(7):455–461
Kudo S, Tamura S, Nakajima T, Yamano H, Kusaka H, Watanabe H (1996) Diagnosis of colorectal tumorous lesions by magnifying endoscopy. Gastrointest Endosc 44(1):8–14
(2003) The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest Endosc 58(6 Suppl):S3–S43
Rembacken BJ, Fujii T, Cairns A, Dixon MF, Yoshida S, Chalmers DM, Axon AT (2000) Flat and depressed colonic neoplasms: a prospective study of 1000 colonoscopies in the UK. Lancet 355(9211):1211–1214
Tsuda S, Veress B, Toth E, Fork FT (2002) Flat and depressed colorectal tumours in a southern Swedish population: a prospective chromoendoscopic and histopathological study. Gut 51(4):550–555
Tanaka S, Haruma K, Oka S, Takahashi R, Kunihiro M, Kitadai Y, Yoshihara M, Shimamoto F, Chayama K (2001) Clinicopathologic features and endoscopic treatment of superficially spreading colorectal neoplasms larger than 20 mm. Gastrointest Endosc 54(1):62–66
Saito Y, Fujii T, Kondo H, Mukai H, Yokota T, Kozu T, Saito D (2001) Endoscopic treatment for laterally spreading tumors in the colon. Endoscopy 33(8):682–686
Tamura S, Nakajo K, Yokoyama Y, Ohkawauchi K, Yamada T, Higashidani Y, Miyamoto T, Ueta H, Onishi S (2004) Evaluation of endoscopic mucosal resection for laterally spreading rectal tumors. Endoscopy 36(4):306–312
Saito Y, Kawano H, Takeuchi Y, Ohata K, Oka S, Hotta K, Okamoto K, Homma K, Uraoka T, Hisabe T, Chang DK, Zhou PH (2012) Current status of colorectal endoscopic submucosal dissection in Japan and other Asian countries: progressing towards technical standardization. Dig Endosc 24(Suppl 1):67–72
Kakushima N, Fujishiro M, Kodashima S, Muraki Y, Tateishi A, Omata M (2006) A learning curve for endoscopic submucosal dissection of gastric epithelial neoplasms. Endoscopy 38(10):991–995
Yamamoto S, Uedo N, Ishihara R, Kajimoto N, Ogiyama H, Fukushima Y, Yamamoto S, Takeuchi Y, Higashino K, Iishi H, Tatsuta M (2009) Endoscopic submucosal dissection for early gastric cancer performed by supervised residents: assessment of feasibility and learning curve. Endoscopy 41(11):923–928
Probst A, Pommer B, Golger D, Anthuber M, Arnholdt H, Messmann H (2010) Endoscopic submucosal dissection in gastric neoplasia—experience from a European center. Endoscopy 42(12):1037–1044
Hong KH, Shin SJ, Kim JH (2014) Learning curve for endoscopic submucosal dissection of gastric neoplasms. Eur J Gastroenterol Hepatol 26(9):949–954
Hotta K, Oyama T, Shinohara T, Miyata Y, Takahashi A, Kitamura Y, Tomori A (2010) Learning curve for endoscopic submucosal dissection of large colorectal tumors. Dig Endosc 22(4):302–306
Sakamoto T, Saito Y, Fukunaga S, Nakajima T, Matsuda T (2011) Learning curve associated with colorectal endoscopic submucosal dissection for endoscopists experienced in gastric endoscopic submucosal dissection. Dis Colon Rectum 54(10):1307–1312
Saito Y, Uraoka T, Yamaguchi Y, Hotta K, Sakamoto N, Ikematsu H, Fukuzawa M, Kobayashi N, Nasu J, Michida T, Yoshida S, Ikehara H, Otake Y, Nakajima T, Matsuda T, Saito D (2010) A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest Endosc 72(6):1217–1225
Tamegai Y, Saito Y, Masaki N, Hinohara C, Oshima T, Kogure E, Liu Y, Uemura N, Saito K (2007) Endoscopic submucosal dissection: a safe technique for colorectal tumors. Endoscopy 39(5):418–422
Fujishiro M, Yahagi N, Kakushima N, Kodashima S, Muraki Y, Ono S, Yamamichi N, Tateishi A, Oka M, Ogura K, Kawabe T, Ichinose M, Omata M (2007) Outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms in 200 consecutive cases. Clin Gastroenterol Hepatol 5(6):678–683 (quiz 645)
Saito Y, Uraoka T, Matsuda T, Emura F, Ikehara H, Mashimo Y, Kikuchi T, Fu KI, Sano Y, Saito D (2007) Endoscopic treatment of large superficial colorectal tumors: a case series of 200 endoscopic submucosal dissections (with video). Gastrointest Endosc 66(5):966–973
Hurlstone DP, Atkinson R, Sanders DS, Thomson M, Cross SS, Brown S (2007) Achieving R0 resection in the colorectum using endoscopic submucosal dissection. Br J Surg 94(12):1536–1542
Uraoka T, Saito Y, Matsuda T, Ikehara H, Gotoda T, Saito D, Fujii T (2006) Endoscopic indications for endoscopic mucosal resection of laterally spreading tumours in the colorectum. Gut 55(11):1592–1597
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Han Ho Jeon, Hye Sun Lee, Young Hoon Youn, Jae Joon Park and Hyojin Park have no conflicts of interest of financial ties to disclose.
Rights and permissions
About this article

Cite this article
Jeon, H.H., Lee, H.S., Youn, Y.H. et al. Learning curve analysis of colorectal endoscopic submucosal dissection (ESD) for laterally spreading tumors by endoscopists experienced in gastric ESD. Surg Endosc 30, 2422–2430 (2016). https://doi.org/10.1007/s00464-015-4493-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4493-2