
Abstract
Background
Three-port laparoscopic appendectomy (TPLA) has been shown superior to open appendectomy for acute appendicitis (AA); alternatively, single-incision laparoscopic appendectomy (SILA) is gaining popularity. The choice between SILA and traditional TPLA remains controversial. This meta-analysis of high-quality randomized controlled trials (RCTs) aims to compare efficacy and safety of SILA with TPLA for AA.
Methods
We searched MEDLINE, EMBASE, and the Cochrane Library for RCTs comparing SILA with TPLA. Reference lists of relevant articles and reviews, conference proceedings, and ongoing trial databases were also searched. Primary outcomes were operative time, postoperative complications, hospital duration, and days back to normal activities. Meta-analysis was conducted where possible comparing items using weighted mean differences (WMDs) and relative risks (RRs) according to type of data. Methodological quality was evaluated to assess bias risk.
Results
A total of 8 distinct RCTs comparing SILA (n = 616) with TPLA (n = 618) published from 2010 to 2013 were identified in our analysis. SILA took longer to conduct than TPLA (43 vs 38, WMD: 5.96, 95 % CI 2.54–9.38, P = 0.0006). Patients undergoing SILA needed more extra trocars addressed during operation (7 % vs 0 %, RR: 12.36, 95 % CI 3.83–39.90, P < 0.0001), but could return to full activities earlier (6 vs 7, WMD: −0.68, 95 % CI −1.10 to −0.26, P = 0.001). However, these differences were not clinically significant. All other parameters were comparable.
Conclusions
These results provide level 1a support for the clinical similarity that SILA is basically as feasible, effective and safe as TPLA when dealing with AA, although statistically, SILA takes longer to perform, requires more extra trocars, and benefits patients with faster recovery compared with TPLA. Further RCTs are needed to update our finding with advancement of surgical techniques and skills.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Open appendectomy has been considered standard treatment for acute appendicitis (AA) since first described by McBurney [1] in 1894. Recently, meta-analyses based on randomized controlled trials (RCTs) revealed convincingly that laparoscopic appendectomy (LA) which was initially performed by Semm [2] in 1983 and is widespread now has a tendency of replacing the open procedure as a standard treatment for AA with obvious advantages, including earlier bowel function recovery and postoperative oral intake, less invasiveness and postsurgical pain, shorter postoperative hospital stay, earlier return to normal diet, activities and work, lower rates of postoperative complications especially wound infection and mortality, and better cosmesis, despite possibly longer operation time, the difference of which between the two approaches is reducing [3]. There are also evidences sustaining LA for children, obese population, and adults with complicated appendicitis [4]. However, a systematic review based on low-level evidences showed that LA might cause more fetal losses during pregnancy [5].
With the rapid progress of natural orifice translumenal endoscopic surgery, single-incision LA (SILA) emerged as an innovation, which allows minimally invasive surgery to be performed through a single incision, further reducing the trauma, and is gaining widespread acceptance because of its provision of a “scarless” abdominoplasty without increasing hazards [6]. Since the first SILA was conducted for AA by Pelosi [7] in 1992, there have been numerous trials comparing SILA with conventional three-port LA (TPLA). However, claims of reduced pain with improved cosmesis and faster recovery are unsubstantiatedly informed with weak and insufficient evidence [8]. Many other controversies remain, including surgical time, postoperative complications, and hospital duration [6].
Up till now, pooled comparisons [9–13] are mainly based on retrospective and nonrandomized observational trials with few available RCTs. None of them include studies published last year, when 5 novel RCTs with large samples emerged. Gao’s [14] analysis also neglected the fact that St Peter’ and Knott’s results are based on the same population. Therefore, their unconvincing conclusions should be interpreted with caution due to considerable bias.
In this study, potential advantages of each technique were quantified using the meta-analytical method. Meta-analysis reaches the highest level of evidence when pooling data only from randomized trials [15], therefore our study which is carried out according to preferred reporting items for systematic reviews and meta-analysis (PRISMA) [16] guideline and based on intention to treat analysis systematically reviewing all the available high-quality RCTs comparing SILA with TPLA creates the highest level of evidence.
Materials and methods
Literature search
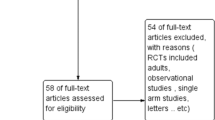
A systematic literature search with search terms “single/one-incision/port/site,” “three-port,” “conventional,” “laparoscopic/laparoendoscopic,” and “appendectomy/appendicectomy/appendicitis” and their combinations as key words was performed in MEDLINE, EMBASE, the Cochrane Library and Springer databases, and Google Scholar (Fig. 1). Special database functions like “related articles” and “explosion” were used to maximize our search, and cross-references, references from relevant articles and reviews were also screened. We also searched conference proceedings and ongoing trial databases. Language restrictions were not applied. The last search was performed on January 12th, 2014.

PRISMA literature selection flow diagram. PRISMA preferred reporting items for systematic reviews and meta-analysis
Inclusion criteria
Titles and abstracts of all identified articles were screened and we selected studies according to the following criteria: population-patients with AA (diagnosed as proposed by Katkhouda [17]) without age, gender, body mass index, and racial limitations; intervention and comparative intervention-clearly documented surgical technique of SILA versus TPLA with curative intent for AA including at least one of the five basic types, regardless of detailed equipment applied, and size and position of the port/incision; outcomes-at least one of the outcome measures reported below; study design-published and unpublished RCTs. If two studies from the same institution were identified, the most recent or the most informative was selected, unless they were reports from different periods or if the data of overlapping patients could be subtracted.
Exclusion criteria
Studies were excluded from our analysis if they did not meet the above inclusion criteria, or the study population included diseases other than AA (e.g., appendiceal carcinoid, chronic appendicitis) unless the data were presented separately, or it was impossible to extract or calculate appropriate data from the published results. Abstracts of RCTs were excluded as the surgical technique, methodological quality, and the risk of bias of these studies could not be assessed.
Types of interventions
Any appendectomy performed in the space generated by an insufflated pneumoperitoneum or by a wall lifting method, with visualization of the operative field mainly through a videolaparoscope was included. The technique was referred as SILA if all phases of the operation were performed initially through one incision regardless of incision size. As TPLA, we considered all procedures as “conventional” or “three-port” and performed initially through three abdominal ports. Techniques in which extra incisions or ports were used to facilitate the procedure half-way were not excluded.
Studies that included other types of resections (e.g., open appendectomy) or those that contained multivisceral resections were excluded unless the data were presented separatively.
Outcomes of interest and definitions
Primary outcomes were operating time (min), hospital duration (h), length of postsurgical hospital stay (h), days back to full activities, postsurgical complications, and reoperations. Secondary outcomes included extra trocars and drainages required, hours to regular diet, post-operational pain based on visual analog scale (VAS) [18], and application of analgesics. As described in the included trials, the operative time was recorded as the time from the first incision to the placement of the last suture in the skin. Patients were discharged after clinical examinations, body temperature, and leukocyte count were normal. Postsurgical duration was defined as the number of days in the hospital after the operation day. The days required for a return to work or normal activities were determined by patient follow-up assessment for at least 1 month. Postoperative complications were classified as medical (urinary events, nonsurgical infections, etc.) and surgical, which were further categorized as major (any fistula, any complication that required reoperation, all intra-abdominal collections, etc.) and minor (wound complications, bleeding events, ileus, etc). This classification system of major and minor surgical complications is based on Memorial Sloan-Kettering Cancer Center complication reporting system [19]. Patients’ postoperative pain was scored using a VAS with scores ranging from 1 (absence of pain) to 10 (worst pain possible) [18], and number of patients who required analgesics post-appendectomy.
Data extraction
Titles and abstracts of all retrieved records, and subsequently full-text articles were examined independently by two authors (A.M.X. and L.H.) according to PRISMA [16] guideline. The following data were extracted separately by the same two authors for all included studies: reference of study, study population characteristics, study design, and inclusion and exclusion criteria. For dichotomous outcomes, the number of events was recorded and for continuous outcomes, means, and standard deviations (SDs) were registered. Population characteristics included number of participating subjects, the number and type of procedures performed, age, gender, body mass index, and pathological type of AA. In case of discrepancies, a third author (T.J.L.) was consulted and agreement was reached by consensus.
Missing data were handled by the following methods. Missing SDs were imputed on the basis of ranges when available [20]. If both means and SDs were missing, they were imputed on the basis of the medians and ranges or on the basis of medians and interquartile ranges, according to availability [20]. If neither a range nor any other measure of dispersion was available, then the study data were not applied in meta-analysis.
Risk of bias assessment
Risk of bias was assessed for all articles by individual components using both the Cochrane Collaboration’s tool for assessing risk of bias and the Jadad scoring system [21].
Statistical analysis
This study was carried out in line with the recommendations of the PRISMA [16] statement. Statistical analyses were performed following the recommendations of the Cochrane Collaboration Guidelines [22]. Outcomes reported by 2 or more studies were pooled in meta-analyses. Our study was based on intention to treat analysis.
Dichotomous and continuous outcomes were presented as risk ratios (RRs), rate differences (RDs), and weighted mean differences (WMDs), respectively. Data were pooled using the Mantel–Haenszel and the inverse-variance method for dichotomous and continuous outcomes, respectively. Trials with zero events in both arms were excluded from meta-analysis. Trials with zero events in 1 arm were included in the analysis by adding a continuity correction of 0.5 to all cells in the 2 × 2 table of that study. As a robustness assessment, meta-analyses with RCTs with 0 event in 1 arm were also performed using risk differences in a sensitivity analysis. For all analyses, the 95 % confidence interval (CI) was calculated. Heterogeneity was calculated using Higgins χ 2 test, and inconsistency in study effects was quantified by I 2 values [23]. The fixed-effects model was used if no heterogeneity was present (χ 2 P > 0.100 and I 2 < 50 %). If excessive heterogeneity was present, data were first rechecked and the DerSimonian random-effects model was used when heterogeneity persisted [24]. Funnel plots were used to help identify the presence of publication or other types of bias. Subgroup analysis was planned for studies with and without perforated AA, and pregnacy, and total cases more and less than 150 (cut-off value set in line with the median of the sample size of enrolled RCTs) after the overall analysis. Review Manager software (RevMan© v. 5.0) provided by the Cochrane Collaboration was used for data management and statistical analyses.
Results
Selected RCTs characteristics
A total of 86 potential relevant publications were identified (Fig. 1). We then identified 34 full-text articles comparing SILA with TPLA and found 24 studies did not randomly allocate patients. One RCT [25] comparing the two methods has been registered, but without any accessible data. One RCT [26] was excluded for duplicate publication based on the same population with St. Peter’s. Finally, eight original RCTs [27–34] comparing SILA with TPLA when treating AA which met the eligibility criteria were identified. Among them 4 publications excluded patients suffering from perforated AA, while the other 4 articles set no special limitations on type of AA.
The 8 included RCTs were published between 2010 and 2013, and conducted between February 2009 and November 2011 with 1 week to 35 months of follow-up. A total of 1234 patients were included in our analysis with 616 undergoing SILA (49.9 %) and 618 (50.1 %) undergoing TPLA (Table 1). LA was performed in all patients, with either 1 incision or 3 ports in abdomen. Patients’ characteristics are listed in Table 2. All patients had proof of AA on symptoms and/or signs and/or preoperative ultrasound/computed tomography and/or laboratory studies (Table 3). Regarding the preoperative clinical criteria used to select patients, four trials included patients with perforated AA for the laparoscopic technique, and these patients showed no difference of characteristics between both arms (Table 4). In total, 1,170 patients (94.8 %) were imperforated. Overall, there were only 2 conversions to OA (0.16 %), related to incomplete repair of appendiceal base during SILA and an identified mass-forming lesion during TPLA, respectively. Matching of demographic factors was almost complete and all studies were adequately matched in all the factors reviewed (Table 1). Before LA, the two groups did not differ significantly in terms of age (Z = 1.29, P = 0.20), gender (Z = 0.20, P = 0.84), weight (Z = 0.15, P = 0.88), body mass index (Z = 1.74, P = 0.08), inflammatory parameters [C-reactive protein (Z = 0.22, P = 0.83) and leukocyte count (Z = 1.72, P = 0.09)], or type of appendicitis [exudative appendicitis (Z = 1.01, P = 0.31), suppurative appendicitis (Z = 1.07, P = 0.28), perforated appendicitis (Z = 0.27, P = 0.79), gangrenous appendicitis (Z = 0.17, P = 0.86), and periappendiceal abscess (Z = 1.46, P = 0.15)] (Tables 2, 4).
Methodological quality assessment
The trials had relatively good methodological quality with a mean Jadad score of 3.125 (range 1–5). However, they mostly suffered from methodologic drawbacks frequently seen in surgical RCTs in general, mainly difficulties in concealing the allocation of patients, the inherent complexity of blinding between two techniques, and small number of patients included in part of the researches. Five trials did not report double blinding and allocation concealment and one did not report loss to follow-up. Six trials reported a sample size calculation. Seven trials had adequate sequence generation (Table 5)
Primary outcomes
Detailed data and analyses by categories are available in Tables 6 and 7.
Operative time
Results were available for all RCTs. There existed significant heterogeneity (χ 2 = 39.76, P < 0.00001, I 2 = 82 %) between two groups, so a randomized-effect model was chosen. Operative time was approximately 5 min longer in the SILA group than in the TPLA group (43 vs 38; WMD: 5.96; 95 % CI 2.54–9.38; P = 0.0006; Fig. 2A). However, two reports [31, 33] comparing 2 techniques dealing with perforated AA separately revealed no significant difference between 2 procedures (46 vs 49; WMD: 4.15; 95 % CI −15.58 to 23.89; P = 0.68), based on a randomized-effect model due to significant heterogeneity (χ 2 = 2.85, P = 0.09, I 2 = 65 %).


A Operative time by SILA and TPLA techniques, showing SILA takes longer to complete. B Hospital duration by SILA and TPLA techniques, showing no difference. C Days needed to return to full activities, showing patients undergoing SILA recovers faster. D Overall complications, E major surgical complications, F minor surgical complications, G medical complications, H ileus, I abdominal infections, and J wound infections, all showing similar results between SILA and TPLA procedures. SILA single-incision laparoscopic appendectomy, TPLA three-port laparoscopic appendectomy
Hospital and postsurgical duration
There being no significant heterogeneity or bias (Fig. 4A), fixed-effect model chosen showed no significant difference in either overall (4 RCTs, 58 vs 59; WMD −0.96; 95 % CI −2.86 to 0.94; P = 0.32; Fig. 2B) or post-LA hospital stay (2 RCTs, 32 vs 32; WMD: 0.48; 95 % CI −0.86 to 1.81; P = 0.48) between 2 procedures.
Return to normal activities
Follow-ups provided by 3 trials supported that SILA group had a significantly earlier return to full activities (6 vs 7; WMD: −0.68; 95 % CI −1.10 to −0.26; P = 0.001; Fig. 2C), without significant heterogeneity, but St. Peter [28] found no significant difference in days to return to school among children patients. Teoh [29] further reported no significant difference in quality-of-life in short-term.
Postoperative complications
The included trials reported no mortality. There were no significant heterogeneities or biases demonstrated by funnel plots for all parameters (Fig. 4B–D), so fixed-effect models were applied. The combined data from all trials showed that the overall (8 vs 8 %; RR: 1.02; 95 % CI 0.71–1.48; P = 0.91; Fig. 2D), surgical [major (2 vs 1 %; RR: 1.40; 95 % CI 0.63–3.11; P = 0.41; Fig. 2E) and minor (5 vs 6 %; RR: 0.97; 95 % CI 0.62–1.54; P = 0.91; Fig. 2F)], and medical (1 vs 1 %; RR: 0.67; 95 % CI 0.19–2.35; P = 0.53, Fig. 2G) complications were all comparable between 2 groups.
Through a subcategory analysis of postoperative complications, we found that rates of ileus (6 RCTs; 1 vs 2 %; RR: 0.71; 95 % CI 0.23–2.22; P = 0.56; Fig. 2H), abdominal (5 RCTs; 2 vs 1 %; RR: 1.80; 95 % CI 0.61–5.31; P = 0.29; Fig. 2I), and wound (7 RCTs; 4 vs 4 %; RR: 0.96; 95 % CI 0.55–1.68; P = 0.88; Fig. 2J) infections were all similar in both groups, all based on fixed-effect model thanks to insignificant heterogeneity or bias (Fig. 4E–G). Reoperation rates were also comparable (3 RCTs [30, 32, 34]; 0 vs 1 %; RR: 0.34; 95 % CI 0.04–3.21; P = 0.34) for both procedures.
Secondary outcomes
Detailed data and analyses by categories are available in Tables 8 and 9.
Extra trocars and drainages
More extra trocars were observed among patients undergoing SILA (6 RCTs; 7 vs 0 %; RR: 12.36; 95 % CI 3.83–39.90; P < 0.0001; Fig. 3A) based on a fixed-effect model due to insignificant heterogeneity and bias (Fig. 4H), and RD was also calculated with a significant difference found (RD: 0.05; 95 % CI 0.01–0.10; P = 0.03; Fig. 3B) using a randomized-effect model due to significant heterogeneity (χ 2 = 21.28, P = 0.0007, I 2 = 77 %), while drainages needed revealed by 3 studies were comparable (8 vs 11 %; RR: 0.77; 95 % CI 0.45–1.33; P = 0.35; Fig. 3C).

A Extra trocars placed during SILA and TPLA techniques, showing higher likelihood of events for SILA. B Extra trocars placed during SILA and TPLA (risk difference calculated). C Drainages inserted during SILA and TPLA, showing comparable requirement. D Time to regular diet post SILA and TPLA, indicating similar results. SILA single-incision laparoscopic appendectomy, TPLA three-port laparoscopic appendectomy


Funnel plots for A hospital duration, B overall complications, C major surgical complications, D minor surgical complications, E ileus, F abdominal infections, G wound infections, and H extra trocars required between two procedures, showing that all parameters are free from significant bias
Postoperative pain
Significant heterogeneities were observed for VAS scores 12 (χ 2 = 8.21, P = 0.004, I 2 = 88 %) and 24 h (χ 2 = 3.14, P = 0.08, I 2 = 68 %) post-LA, so randomized-effect models were used. Results revealed that there were no significant differences in both scores (2 RCTs; 3 vs 3; WMD: −0.51; 95 % CI −1.51 to 0.49; P = 0.32 and 2 RCTs; 3 vs 3; WMD: −0.34; 95 % CI −1.01 to 0.32; P = 0.31). This was accompanied by a comparable prevalence of analgesics use (2 RCTs; 75 vs 88 %; RR: 0.89; 95 % CI 0.76–1.05; P = 0.16). St. Peter [28] also reported similar results as to days and doses of prescribed analgesics after hospital discharge. However, Teoh [29] revealed more severe pain experienced by patients undergoing SILA upon coughing or standing, but with similar pain score at rest.
Time when regular diet began
There existing no significant heterogeneity, a fixed-effect model was applied. No significant discrepancy was found in time to regular diet between 2 approaches (3 RCTs; 22 vs 28; WMD: 0.02; 95 % CI −0.29 to 0.34; P = 0.88; Fig. 3D).
Sensitivity tests
Kye’s data ignored, patients undergoing 2 procedures returned to normal activity after comparable period of time (7 vs 8; WMD: −0.58; 95 % CI −1.42 to 0.27; P = 0.18; Fig. 5A). Either St. Peter’s (5 vs 0 %; RD: 0.04; 95 % CI −0.01 to 0.09; P = 0.08; Fig. 5B) or Lee’s (6 vs 0 %; RD: 0.04; 95 % CI −0.01 to 0.09; P = 0.10; Fig. 5C) study being excluded, extra trocars applied in 2 procedures were comparable when RD was calculated. Sensitivity analyses of all the other primary and secondary outcomes with 0 event in 1 arm yielded similar results. Funnel plots (Fig. 4) and an exhaustive literature search conferred a substantial degree of confidence in our pooled findings.

A Sensitivity test for days to full activities after SILA and TPLA, showing the difference disappears disregarding Kye’s study. B Extra trocars applied during SILA and TPLA techniques ignoring St. Peter’s result and C Lee’s report, both showing comparative results when risk difference is calculated. SILA single-incision laparoscopic appendectomy, TPLA three-port laparoscopic appendectomy
Subgroup analysis
We divided subgroups according to whether pregnancy or perforation was included and by using a 150 cases cut-point (Table 10). We found differences of surgical duration no longer existed when only considering studies including pregnancy (3RCTs; 37 vs 32; WMD: 5.84; 95 % CI −0.79 to 12.46; P = 0.08; Fig. 6A) and perforation (4RCTs; 36 vs 34; WMD: 4.47; 95 % CI −2.80 to 11.74; P = 0.23; Fig. 6B), and with less than 150 cases (4RCTs; 43 vs 38; WMD: 5.92; 95 % CI −0.97 to 12.82; P = 0.09; Fig. 6C), with significant intergroup heterogeneity observed though. The overall, major and minor surgical complications, and wound infections remained comparable between SILA and TPLA with low heterogeneity for all subgroups evaluated. Discrepancy in extra trocars persisted in both subgroups with pregnancy included and excluded (Fig. 6D), but disappeared when only including perforated cases (2RCTs; 3 vs 0 %; RR: 3.00; 95 % CI 0.32–28.14; P = 0.34; Fig. 6E) and when there were less than 150 cases (3RCTs; 3 vs 0 %; RR: 3.00; 95 % CI 0.48 to 18.58; P = 0.24; Fig. 6F).


A Subgroup analysis for surgical duration according to whether pregnancy or B perforation is included and C by using a 150 cases cut-point, showing difference no longer exists when only considering studies including pregnancy (A) and perforation (B) and with less than 150 cases (C). Subgroup analysis for extra trocars according to whether perforation is included (D) and by using a 150 cases cut-point (E), showing difference disappears when only considering studies including perforation (D) and with less than 150 cases (E)
Sensitivity analysis for subgroups was further conducted, and we found that with Kye’s data excluded, SILA took longer again both when pregnancy was included in calculation (37 vs 40; WMD: 8.78; 95 % CI 2.32–15.25; P = 0.008; Fig. 7A) and when sample size was less than 150 (47 vs 38; WMD: 8.34; 95 % CI 2.00–14.68; P = 0.01; Fig. 7B). Without Lee’s data, two procedures were accompanied with comparable extra trocars addressed when pregnancy (2 vs 0 %; RR: 3.02; 95 % CI 0.49–18.75; P = 0.24; Fig. 7C) was excluded in analysis.

Sensitivity tests for subgroups of operative time according to whether pregnancy is included (A) and by using a 150 cases cut-point (B), showing both differences recur when Kye’s study is excluded in the subgroups including pregnancy (A) and with less than 150 cases (B), respectively. C Sensitivity test for subgroups of extra trocars placed according to whether pregnancy is included, showing difference emerges when Lee’s results is excluded in the subgroups excluding pregnancy
Discussion
LA has been proposed to reduce the invasiveness of appendectomy, and was first applied to cure AA by Schreiber [35] in 1987. Although the open procedure is still used in some medical centers and there may exist conversions during LA, the superior clinical outcomes of LA has been certified by convincing proves, and many surgical institutions are inclined to LA because of availability of whole abdominal cavity profilering especially among fat and pregnant population [3–5]. SILA is developing and gaining popularity rapidly with its unique benefit of concealing surgical wound within the umbilicus [36]. There havve been many trials evaluating this new technique mainly among selective adults and uncomplicated AA sufferers without perforation or abscess and many reported ideal achievements [6, 8]. However, most of reports are limited to nonrandomized retrospective study based on relatively small population and focus on the aspect of operating technique [37].
Six systematic reviews based on mainly non-RCTs concluded that SILA was comparable to TPLA in safety and effectiveness [9–14]. Compared with the previous studies, our analyses share some similarities. But the quality of non-RCTs has a great impact on the accuracy of pooled estimates, and the previous meta-analyses comparing SILA with TPLA may contain duplicate and incomplete studies, thus leading to great bias.
This study summarizes the highest quality data comparing SILA with TPLA. In our analysis, RCTs were all published after 2009, and those published in 2013 constituted most of the studies included, which are not included in most previous meta-analyses. Some of the individual trials were inconclusive as they were underpowered and hence too small to identify significant differences regarding the important determinants of ideal LA. This meta-analysis aims to provide this evidence.
Surgical techniques of the included trials were standardized. Three trials enrolled a comparable number of patients suffering from perforated AA and pregnancy in both arms. Study population was similar between trials in all mentioned aspects.
Researches of different qualities revealed discrepant comparisons of surgical duration between the 2 techniques, and most reported longer operating time during SILA [28]. However, in surgical centers majored in this technique, SILA could consume shorter time; [38] Ding’s [11] pooled result based on mainly retrospective studies showed no difference. Our results showed that operative time increased significantly by approximately 5 min in the SILA group, which is not an appreciable clinical difference though. Although SILA seems more difficult than TPLA to conduct technically with a limited vision [28], it may be more practicable when placing gauzes and cleaning abdominal cavity, and the conflicts of external instruments and limitation of their movements caused by parallel and approaching of apparatus which makes adequate triangulation of traction and counter-traction difficult can be solved by improvement of equipment [6]. With joint efforts of surgeons and academic centers, improvements in instrumentation like angled or flexible endoscopes and in ergonomics, and maturation and modification of the new technique, it is reasonable to believe that conducting SILA may consume less and less time with a wider diffusion of this technique, but may require a long and steep learning curve, and good cooperation of whole therapeutic team [6, 8]. We believe that SILA for AA should be offered only in large specialized centers with experience in SILA procedures and a large number of patients in order to make this learning curve completed more effectively. Several of the studies included in our analysis reported on their initial experience, so some outcomes studied, including operative time may have been influenced by learning curve issues. The technical change from conventional to single-port LA requires a learning curve of at least 10 surgeries for a basic handling of SILA [39]. Unfortunately, most studies did not explicitly describe their previous level of proficiency with the technique, so we were unable to perform a subgroup analysis that directly addressed this matter. As a surrogate, a subgroup analysis was performed using 150 cases as a cut point, but the change of SILA operative time was not significant, and the time was still longer than TPLA. It is likely that we did not observe a more pronounced effect of the number of SILA cases performed because the studies represented, for the large part, the experience of a group of surgeons, whereas the learning curve is an individual achievement. In difficult cases like perforation, TPLA may promise more expeditious and easier dissection and mobilization [28]. We did not found significant difference in surgical time when dealing with pure perforated AA cases, and pooled analysis based on studies in which pregnancy or perforated AA was included revealed similar results between 2 procedures.
Recently, the results of RCTs demonstrated that SILA resulted in similar post-surgical complications compared with TPLA, and trials of larger scale reported no greater complication rates during SILA than those revealed before [40]. The level 1a evidence provided by us showed no significant differences as to overall, surgical (major and minor), and medical complications between 2 techniques, which may be because SILA, although less trocars applied, leads to the same organ and mesoappendix resection as TPLA. SILA with insertion of just 1 trocar in the umbilical area eliminates the possibility of injury to the bladder and the inferior epigastric vessels [8]. Wound complications seem to be common for LA [8, 28], and early reports indicated SILA might be combined with higher incidence of wound infection [8]. According to the best evidence provided by us, there is no significant difference on this issue regardless of specific protection for umbilical skin during appendix division [28], and the discrepancy shown before might be due to diverse surgical techniques and postsurgical management. Theoretically, the larger abdominal incision is, the higher risk of postoperative hernias there will be. Based on the included RCTs, we found basically no existence. Rates of ileus, abdominal infection and reoperation were all similar between SILA and TPLA techniques according to our convincing analysis. Period of post-surgical follow-ups may be a great influential factor impacting complication rates especially the long-terms though. Our study also revealed that SILA significantly required an extra port in only 7 % of cases during surgery, which is not clinically significant though. And in the case of inadequate visualization or mobilization of the appendix, the insertion of additional ports or trocars is not regarded as a shortcoming but is supported to preserve the appropriateness of the operation [40]. We further revealed that during complicated AA managing, comparable trocars were required in both procedures. Our pooled results showed that patients undergoing two procedures required comparable drains at the end of LA, which may be a challenge for SILA because the placement of a drain via the umbilicus may lead to higher risk of wound infection and incisional hernia, and affect cosmetic results [8].
With comparable usage of analgesics and anti-inflammatory drugs, it is believed that the larger the transumbilical fascial incision is and the greater wound irritation there exists due to the insertion of all surgical instruments through only one incision, the more painful patients may experience post-LA [28]. While others demonstrated that postsurgical pain is mainly related to the injury of muscles and parietal peritoneum, regardless of the diameter of the trocar, and that for minimally invasive surgery, the less trocars, the less pain [41]. Patients may suffer from more serious pain post SILA, while other researchers made the converse conclusion [28]. We found that 12 and 24 h VAS scores were comparable post 2 procedures, possibly because there is only 1 trocar during SILA through which all equipment has to be inserted, thus size may not reduce significantly compared with the sum of the 3 trocars when performing TPLA [28]. Researches showed better post-operative recovery results after SILA than those after TPLA [27–34]. Ding [11] revealed shorter length of hospital stay for SILA, but we showed no significant difference on this issue. We also revealed comparable peri-operative recovery parameters between 2 procedures including time to regular diet, and postsurgical hospital stay. Though patients undergoing SILA could return to full activities earlier according to our convincing results, but it is not a clinically distinction actually due to the interval of observation.
The internal validity of this study is high because the analysis was based on high-quality RCTs, with low risk of bias. This analysis is limited by the diverse follow-up period and the fact that not all outcomes of interest are reported by all enrolled studies. One RCT [25] is currently being conducted in England, and it is hoped that it will address questions better.
In conclusion, choice of the technique for AA may be based on patients’ preferences and presence of local expertise [29]. SILA is basically a comparable option for the treatment of AA that compares favorably with TPLA in hospital stay and post-operative complications. Statistically, SILA results in a longer operative duration and require more extra trocars, while patients could return to normal activities earlier post-SILA. However, these differences are not clinically significant, and may be due to learning curve issues. All other indexes are similar. More studies are needed to be carried out in patients suffering from complicated AA and those with higher BMI and associated comorbidities. These results lend level 1a support for the alternative use of SILA for the surgical treatment of AA.
References
McBurney C (1894) IV. The incision made in the abdominal wall in cases of appendicitis, with a description of a new method of operating. Ann Surg 20(1):38–43
Semm K (1983) Endoscopic appendectomy. Endoscopy 15(2):59–64. doi:10.1055/s-2007-1021466
Wei B, Qi CL, Chen TF, Zheng ZH, Huang JL, Hu BG, Wei HB (2011) Laparoscopic versus open appendectomy for acute appendicitis: a metaanalysis. Surg Endosc 25(4):1199–1208. doi:10.1007/s00464-010-1344-z
Tiwari MM, Reynoso JF, Tsang AW, Oleynikov D (2011) Comparison of outcomes of laparoscopic and open appendectomy in management of uncomplicated and complicated appendicitis. Ann Surg 254(6):927–932. doi:10.1097/SLA.0b013e31822aa8ea
Wilasrusmee C, Sukrat B, McEvoy M, Attia J, Thakkinstian A (2012) Systematic review and meta-analysis of safety of laparoscopic versus open appendicectomy for suspected appendicitis in pregnancy. Br J Surg 99(11):1470–1478. doi:10.1002/bjs.8889
Chow A, Purkayastha S, Nehme J, Darzi LA, Paraskeva P (2010) Single incision laparoscopic surgery for appendicectomy: a retrospective comparative analysis. Surg Endosc 24(10):2567–2574. doi:10.1007/s00464-010-1004-3
Pelosi MA, Pelosi MA 3rd (1992) Laparoscopic appendectomy using a single umbilical puncture (minilaparoscopy). J Reprod Med 37(7):588–594
Teoh AY, Chiu PW, Wong TC, Wong SK, Lai PB, Ng EK (2011) A case-controlled comparison of single-site access versus conventional three-port laparoscopic appendectomy. Surg Endosc 25(5):1415–1419. doi:10.1007/s00464-010-1406-2
Gill RS, Shi X, Al-Adra DP, Birch DW, Karmali S (2012) Single-incision appendectomy is comparable to conventional laparoscopic appendectomy: a systematic review and pooled analysis. Surg Laparosc Endosc Percutaneous Tech 22(4):319–327. doi:10.1097/SLE.0b013e31824f2cf8
Pisanu A, Porceddu G, Reccia I, Saba A, Uccheddu A (2013) Meta-analysis of studies comparing single-incision laparoscopic appendectomy and conventional multiport laparoscopic appendectomy. J Surg Res. doi:10.1016/j.jss.2013.03.038
Ding J, Xia Y, Zhang ZM, Liao GQ, Pan Y, Liu S, Zhang Y, Yan Z (2013) Single-incision versus conventional three-incision laparoscopic appendicectomy for appendicitis: a systematic review and meta-analysis. J Pediatr Surg 48(5):1088–1098. doi:10.1016/j.jpedsurg.2013.01.026
Li P, Chen ZH, Li QG, Qiao T, Tian YY, Wang DR (2013) Safety and efficacy of single-incision laparoscopic surgery for appendectomies: a meta-analysis. World J Gastroenterol 19(25):4072–4082. doi:10.3748/wjg.v19.i25.4072
Rehman H, Rao AM, Ahmed I (2011) Single incision versus conventional multi-incision appendicectomy for suspected appendicitis. Cochrane Database Syst Rev 7:CD009022. doi:10.1002/14651858.CD009022.pub2
Gao J, Li P, Li Q, Tang D, Wang DR (2013) Comparison between single-incision and conventional three-port laparoscopic appendectomy: a meta-analysis from eight RCTs. Int J Colorectal Dis. doi:10.1007/s00384-013-1726-5
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 283(15):2008–2012
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535. doi:10.1136/bmj.b2535
Katkhouda N, Mason RJ, Towfigh S, Gevorgyan A, Essani R (2005) Laparoscopic versus open appendectomy: a prospective randomized double-blind study. Ann Surg 242(3):439–448; discussion 448–450
Emshoff R, Bertram S, Emshoff I (2011) Clinically important difference thresholds of the visual analog scale: a conceptual model for identifying meaningful intraindividual changes for pain intensity. Pain 152(10):2277–2282. doi:10.1016/j.pain.2011.06.003
Grobmyer SR, Pieracci FM, Allen PJ, Brennan MF, Jaques DP (2007) Defining morbidity after pancreaticoduodenectomy: use of a prospective complication grading system. J Am Coll Surg 204(3):356–364. doi:10.1016/j.jamcollsurg.2006.11.017
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13. doi:10.1186/1471-2288-5-13
Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, Tugwell P, Klassen TP (1998) Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet 352(9128):609–613. doi:10.1016/S0140-6736(98)01085-X
Clarke M, Horton R (2001) Bringing it all together: Lancet-Cochrane collaborate on systematic reviews. Lancet 357(9270):1728. doi:10.1016/S0140-6736(00)04934-5
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560. doi:10.1136/bmj.327.7414.557
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7(3):177–188
Malik M, McCormack K, Krukowski ZH, McDonald A, McPherson G, Cook JA, Ahmed I, Group SS (2012) Single port/incision laparoscopic surgery compared with standard three-port laparoscopic surgery for appendicectomy: a randomised controlled trial. Trials 13:201. doi:10.1186/1745-6215-13-201
Knott EM, Gasior AC, Holcomb GW 3rd, Ostlie DJ, St Peter SD (2012) Impact of body habitus on single-site laparoscopic appendectomy for nonperforated appendicitis: subset analysis from a prospective, randomized trial. J Laparoendosc Adv Surg Tech A 22(4):404–407. doi:10.1089/lap.2012.0056
Park JH, Hyun KH, Park CH, Choi SY, Choi WH, Kim DJ, Lee S, Kim JS (2010) Laparoscopic vs transumbilical single-port laparoscopic appendectomy; results of prospective randomized trial. J Korean Surg Soc 78(4):213–218
St Peter SD, Adibe OO, Juang D, Sharp SW, Garey CL, Laituri CA, Murphy JP, Andrews WS, Sharp RJ, Snyder CL, Holcomb GW 3rd, Ostlie DJ (2011) Single incision versus standard 3-port laparoscopic appendectomy: a prospective randomized trial. Ann Surg 254(4):586–590. doi:10.1097/SLA.0b013e31823003b5
Teoh AY, Chiu PW, Wong TC, Poon MC, Wong SK, Leong HT, Lai PB, Ng EK (2012) A double-blinded randomized controlled trial of laparoendoscopic single-site access versus conventional 3-port appendectomy. Ann Surg 256(6):909–914. doi:10.1097/SLA.0b013e3182765fcf
Frutos MD, Abrisqueta J, Lujan J, Abellan I, Parrilla P (2013) Randomized prospective study to compare laparoscopic appendectomy versus umbilical single-incision appendectomy. Ann Surg 257(3):413–418. doi:10.1097/SLA.0b013e318278d225
Kye BH, Lee J, Kim W, Kim D, Lee D (2013) Comparative study between single-incision and three-port laparoscopic appendectomy: a prospective randomized trial. J Laparoendosc Adv Surg Tech A 23(5):431–436. doi:10.1089/lap.2012.0284
Lee WS, Choi ST, Lee JN, Kim KK, Park YH, Lee WK, Baek JH, Lee TH (2013) Single-port laparoscopic appendectomy versus conventional laparoscopic appendectomy: a prospective randomized controlled study. Ann Surg 257(2):214–218. doi:10.1097/SLA.0b013e318273bde4
Perez EA, Piper H, Burkhalter LS, Fischer AC (2013) Single-incision laparoscopic surgery in children: a randomized control trial of acute appendicitis. Surg Endosc 27(4):1367–1371. doi:10.1007/s00464-012-2617-5
Sozutek A, Colak T, Dirlik M, Ocal K, Turkmenoglu O, Dag A (2013) A prospective randomized comparison of single-port laparoscopic procedure with open and standard 3-port laparoscopic procedures in the treatment of acute appendicitis. Surg Laparosc Endosc Percutaneous Tech 23(1):74–78. doi:10.1097/SLE.0b013e3182754543
Schreiber JH (1987) Early experience with laparoscopic appendectomy in women. Surg Endosc 1(4):211–216
Ahmed K, Wang TT, Patel VM, Nagpal K, Clark J, Ali M, Deeba S, Ashrafian H, Darzi A, Athanasiou T, Paraskeva P (2011) The role of single-incision laparoscopic surgery in abdominal and pelvic surgery: a systematic review. Surg Endosc 25(2):378–396. doi:10.1007/s00464-010-1208-6
Prasad A (2010) Single incision laparoscopic surgery. World J Gastroenterol 16(21):2705–2706
Muensterer OJ, Puga Nougues C, Adibe OO, Amin SR, Georgeson KE, Harmon CM (2010) Appendectomy using single-incision pediatric endosurgery for acute and perforated appendicitis. Surg Endosc 24(12):3201–3204. doi:10.1007/s00464-010-1115-x
Cho MS, Min BS, Hong YK, Lee WJ (2011) Single-site versus conventional laparoscopic appendectomy: comparison of short-term operative outcomes. Surg Endosc 25(1):36–40. doi:10.1007/s00464-010-1124-9
Vidal O, Valentini M, Ginesta C, Marti J, Espert JJ, Benarroch G, Garcia-Valdecasas JC (2010) Laparoendoscopic single-site surgery appendectomy. Surg Endosc 24(3):686–691. doi:10.1007/s00464-009-0661-6
Goel R, Buhari SA, Foo J, Chung LK, Wen VL, Agarwal A, Lomanto D (2011) Single-incision laparoscopic appendectomy: prospective case series at a single centre in Singapore. Surg Laparosc Endosc Percutaneous Tech 21(5):318–321. doi:10.1097/SLE.0b013e3182311bd9
Acknowledgments
This work was supported by: National Natural Science Foundation of China (81172036), and Foundation of Anhui Science and Technology Agency (12070403061). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. We are grateful to the referees, and Profs. Wen-Xiu Han and Zhi-Jian Wei for critically reviewing this paper. We thank College of Public Hygiene of Anhui Medical University and the Information Center in the First Affiliated Hospital of Anhui Medical University for their contributions to our study.
Disclosures
Drs. A-Man Xu, Lei Huang, and Tuan-Jie Li have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
A-Man Xu and Lei Huang contributed equally to this work.
Rights and permissions
About this article

Cite this article
Xu, AM., Huang, L. & Li, TJ. Single-incision versus three-port laparoscopic appendectomy for acute appendicitis: systematic review and meta-analysis of randomized controlled trials. Surg Endosc 29, 822–843 (2015). https://doi.org/10.1007/s00464-014-3735-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3735-z