
Abstract
Background
Although the incidence of perforation after endoscopic procedures of the colon is low, the rising number of diagnostic colonoscopies could pose relevant health problems. Optimizing treatment may reduce the probability of severe complications. This study aimed to determine perforation frequency and the management of perforations that occurred during diagnostic colonoscopy.
Methods
A retrospective review of patient records was performed for all patients with iatrogenic colonic perforations after sigmoidoscopy/colonoscopy from 2000 to 2011 in three institutions of The Catholic University of Korea. The patients’ demographic data, endoscopic procedure information, perforation location, therapy, and outcomes along with different therapeutic strategies were recorded.
Results
In the 12-year period, a total of 115,285 diagnostic sigmoidoscopic/colonoscopic procedures were performed. A total of 27 perforations occurred. Sixteen patients underwent endoscopic clipping, of which three patients failed and were referred for surgery. Fourteen patients in total underwent surgery for perforation. Endoscopic clip closure was successful in 81 % of the patients. No perforation-related major morbidity or mortality occurred.
Conclusion
Endoscopic repair using clips can be effective for the treatment of colon perforations that occur during diagnostic colonoscopy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Iatrogenic perforation resulting from colonoscopic and sigmoidoscopic procedures is a rare but serious complication with high rates of morbidity and mortality. The frequency of perforations from colonoscopy is estimated to be 0.03–0.8 % for diagnostic colonoscopy and 0.15–3 % for therapeutic colonoscopy [1]. With an increasing number of colonoscopies being performed for screening purposes, this small possibility still may cause a high number of clinical problems. The optimal treatment for perforations is controversial because no randomized trial has ever been conducted. Recent studies have acquired evidence for endoscopic clip closure [2–6]. However, most of these studies included perforations mainly from therapeutic procedures and much less from diagnostic procedures. Furthermore, the efficacy and complications of endoscopic clip closure compared to surgery has not been fully elucidated.
Perforation mechanism, size, and location are different between diagnostic colonoscopy-associated perforations and therapeutic colonoscopy-associated perforations [7]. The proper instruments and personnel to perform endoscopic closure of therapeutic colonoscopy-associated perforations may be more readily available than for diagnostic perforations. The prompt and effective choice of a therapeutic closure method may prevent both unnecessary and more invasive surgery, including colon resection with diversion. We therefore investigated the effectiveness of endoscopic clipping for closure of colonic perforations associated with diagnostic colonoscopies compared to surgery.
Materials and methods
A retrospective multicenter review of the records of patients older than 18 years of age who underwent diagnostic colonoscopy/sigmoidoscopy at three teaching hospitals of The Catholic University of Korea from January 2000 to September 2011 was performed. This study protocol was approved by the Institutional Review Board.
All patients who required treatment for an iatrogenic colon perforation during the study period were reviewed. Iatrogenic colon perforation was defined as a perforation that developed during or after diagnostic colonoscopy in the absence of any other definite cause such as abdominal trauma. Perforation was diagnosed by confirming tissue defects involving all four layers of the colon wall during colonoscopy or peritoneal free air detected by plain chest and/or abdominal X-rays after colonoscopy. Perforations that occurred during therapeutic procedures such as endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) and perforations that occurred due to the patient’s underlying disease such as malignancy or diverticulum were excluded from this study.
Medical records, colonoscopy views, and radiologic results were reviewed. Age, sex, history of abdominal operation, size of the defect, and location of the perforation were analyzed. The size of the perforation was based on endoscopic and/or surgical findings. The fasting period, intravenous antibiotics use, and length of hospital stay after the perforation were investigated.
Delayed perforations diagnosed after the colonoscopic/sigmoidoscopic procedure were treated with surgery. Perforations diagnosed immediately during colonoscopy were treated by endoscopic clipping or surgery depending on the endoscopist’s decision. Complete closure of the mucosal defect with endoscopic clipping and improvement of clinical manifestations such as fever, leukocytosis, and signs of peritoneal irritation were regarded as a successful endoscopic closure (Fig. 1).

Colon perforation during diagnostic colonoscopy. a The orifice of the perforated colon is observed. b The perforated orifice has been closed completely with the clips. c Chest X-ray shows a large amount of peritoneal free air
Categorical variables were compared using Fisher’s exact test and numerical variables were compared using the Mann-Whitney test. A P value less than 0.05 was regarded as statistically significant. All analyses were performed using SPSS for Windows ver. 18 (SPSS Inc., Chicago, IL, USA).
Results
Demographics
During the study period, 115,285 diagnostic colonoscopies (20,653 sigmoidoscopies, 94,632 colonoscopies) were performed. A total of 27 iatrogenic colon perforations (incidence of 0.02 %) occurred in 17 women and 10 men. Perforations occurred in 26 colonoscopies (incidence of 0.03 %) and in 1 sigmoidoscopy (incidence of 0.005 %). The mean age of the patients was 67.5 years. The indications for colonoscopy in the 27 patients with perforation were routine screening (n = 15), history of polyps (n = 4), hematochezia (n = 3), abdominal pain (n = 2), diarrhea (n = 1), constipation (n = 1), and anemia (n = 1). In 24 cases (89 %), perforation was noticed by the endoscopist through visualization of extraintestinal tissue during the procedure. In three cases, perforation was diagnosed after completion of the colonoscopy from the existence of pneumoperitoneum at plain chest and/or abdominal X-ray. Eleven patients (8 women and 3 men) had a history of abdominal or pelvic surgery.
Site of perforation
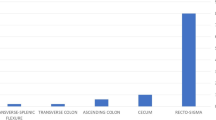
Perforations occurred in the sigmoid colon in 16 cases (59.3 %), the rectum in 8 cases (29.6 %), and the descending colon in 3 cases (11.1 %). Retroflexion was the main cause of perforations in the rectum, while perforation in the sigmoid and descending colons was attributed to excessive pushing of the colonoscopic tip.
Efficacy of endoscopic clip closure compared to surgery
Endoscopic closure of the perforation site was attempted in 16 patients with success in 13 patients (81.3 % of the attempts). Among the three failures, one patient could not have his perforation closed during colonoscopy and was referred for surgery immediately. The other two patients had persistent symptoms of peritoneal irritation after endoscopic closure and were referred for surgery. A total of 14 patients underwent surgery, including the 3 endoscopic closure failure patients. The mean number of clips used was 5.6 (range = 1–18). Perforation size was significantly smaller in the endoscopic closure group (Table 1). However, there were no significant differences in duration of fasting, treatment with intravenous antibiotics, and length of hospital stay between the endoscopic closure group and the surgery group (Table 1). None of the patients who underwent successful endoscopic closure needed further surgical management. For immediate surgical management, laparoscopic wedge resection or primary closure was performed in six patients, segmental resection in two patients, and transanal repair in three patients. No perforation-related major morbidity or mortality occurred.
Discussion
Traditionally, patients with colon perforation have been treated surgically, but recent studies have demonstrated the possibility of endoscopic closure [2–6]. The novel aspect of our study was that we examined the incidence of perforation in diagnostic colonoscopies and excluded those from therapeutic procedures. Although there have been reports demonstrating the feasibility of endoscopic closure of iatrogenic perforations, these reports included mainly perforations from therapeutic procedures such as polypectomy [3, 5, 6]. The mechanisms of perforation for diagnostic procedures and therapeutic procedures are different [8]. Direct pressure to the colonic wall is the main cause of perforations in diagnostic procedures while therapeutic procedures are caused by thermal injury. Perforations in diagnostic colonoscopy are larger than those in therapeutic colonoscopy [6, 7, 9]; thus, immediate diagnosis is more common. Due to this difference, some studies have advocated surgery for diagnostic perforations and a conservative approach to therapeutic perforations [10, 11]. In our study, successful endoscopic closure was possible for 13 (81.3 %) of 16 diagnostic colonoscopy-associated perforation patients. This suggests that immediate endoscopic closure with clips can be attempted for diagnostic perforations as well as therapeutic colonoscopy-associated perforations.
In the current study, the sigmoid colon and rectum were the most common sites of perforation. Iatrogenic colon perforations occur frequently in the sigmoid colon due to its redundancy, luminal narrowing, and adhesions from pelvic operations [8]. Our study confirms the sigmoid colon as the most frequent perforation site and cautious insertion is recommended in patients with severe adhesions due to previous abdominal operations. Perforations occurring at the rectum were due to retroflexion in most cases. Although controversy exists about whether retroflexion increases adenoma and cancer detection in screening colonoscopy [12, 13], it is still a common practice among endoscopists [14]. Our study implies that strenuous attempts of retroflexion should be avoided, especially in patients with a small rectum, since it may be a major cause of iatrogenic perforation.
There was no statistical difference in fasting period, duration of IV antibiotics use, and length of hospital stay between the surgical group and the successful endoscopic clip closure group. However, surgery is associated with significant morbidity and mortality [15]. The high success rate of endoscopic clip closure should make it an attractive treatment option for patients with iatrogenic perforation.
There are several limitations to our study. First, it was a retrospective study and factors such as bowel preparation, which are important in deciding between endoscopic treatment and surgery, could not be investigated thoroughly due to the retrospective design. However, iatrogenic colon perforations are a rare, catastrophic event and a prospective randomized trial would be unethical and difficult to design. Second, in spite of the large number of colonoscopies investigated, the small number of perforations did not allow us to show statistical significance in fasting period, duration of antibiotics use, and length of hospital stay. Third, the perforation size of the endoscopic closure group was significantly smaller than that of the surgery group. This implies that surgery should still be recommended for large iatrogenic perforations. Despite these limitations, our study suggests that endoscopic closure of iatrogenic perforation may be safely performed with a high success rate. Even until recently, surgical closure of iatrogenic colon perforations was considered the primary approach [16]. Experience and training in perforation closure may be a key skill required for endoscopists in the future.
In summary, endoscopic closure of iatrogenic perforations showed a success rate of 81.7 %. No further surgical management after successful closure was required. These results suggest that endoscopic closure may be an important alternative to surgery in the near future.
References
Wullstein C, Koppen M, Gross E (1999) Laparoscopic treatment of colonic perforations related to colonoscopy. Surg Endosc 13:484–487
Cho SB, Lee WS, Joo YE, Kim HR, Park SW, Park CH, Kim HS, Choi SK, Rew JS (2012) Therapeutic options for iatrogenic colon perforation: feasibility of endoscopic clip closure and predictors of the need for early surgery. Surg Endosc 26:473–479
Jovanovic I, Zimmermann L, Fry LC, Monkemuller K (2011) Feasibility of endoscopic closure of an iatrogenic colon perforation occurring during colonoscopy. Gastrointest Endosc 73:550–555
Katsinelos P, Kountouras J, Chatzimavroudis G, Zavos C, Pilpilidis I, Tzilves D, Paroutoglou G (2009) Endoscopic closure of a large iatrogenic rectal perforation using endoloop/clips technique. Acta Gastroenterol Belg 72:357–359
Magdeburg R, Collet P, Post S, Kaehler G (2008) Endoclipping of iatrogenic colonic perforation to avoid surgery. Surg Endosc 22:1500–1504
Yang DH, Byeon JS, Lee KH, Yoon SM, Kim KJ, Ye BD, Myung SJ, Yang SK, Kim JH (2010) Is endoscopic closure with clips effective for both diagnostic and therapeutic colonoscopy-associated bowel perforation? Surg Endosc 24:1177–1185
Luning TH, Keemers-Gels ME, Barendregt WB, Tan AC, Rosman C (2007) Colonoscopic perforations: a review of 30,366 patients. Surg Endosc 21:994–997
Damore LJ 2nd, Rantis PC, Vernava AM III, Longo WE (1996) Colonoscopic perforations. Etiology, diagnosis, and management. Dis Colon Rectum 39:1308–1314
Cobb WS, Heniford BT, Sigmon LB, Hasan R, Simms C, Kercher KW, Matthews BD (2004) Colonoscopic perforations: incidence, management, and outcomes. Am Surg 70:750–757
Lo AY, Beaton HL (1994) Selective management of colonoscopic perforations. J Am Coll Surg 179:333–337
Avgerinos DV, Llaguna OH, Lo AY, Leitman IM (2008) Evolving management of colonoscopic perforations. J Gastrointest Surg 12:1783–1789
Hanson JM, Atkin WS, Cunliffe WJ, Browell DA, Griffith CD, Varma JS, Plusa SM (2001) Rectal retroflexion: an essential part of lower gastrointestinal endoscopic examination. Dis Colon Rectum 44:1706–1708
Varadarajulu S, Ramsey WH (2001) Utility of retroflexion in lower gastrointestinal endoscopy. J Clin Gastroenterol 32:235–237
Mattar WE, Kumar AS, Olden KW (2011) Perspective on routine rectal retroflexion during screening colonoscopy: a survey of American gastroenterologists. J Gastrointest Liver Dis 20:102–103
Iqbal CW, Cullinane DC, Schiller HJ, Sawyer MD, Zietlow SP, Farley DR (2008) Surgical management and outcomes of 165 colonoscopic perforations from a single institution. Arch Surg 143:701–706
Anderson ML, Pasha TM, Leighton JA (2000) Endoscopic perforation of the colon: lessons from a 10-year study. Am J Gastroenterol 95:3418–3422
Disclosures
Drs. Joon Sung Kim, Byung-Wook Kim, Jin Il Kim, Jeong Ho Kim, Sang Woo Kim, Jeong-Seon Ji, Bo-In Lee, and Hwang Choi have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, J.S., Kim, BW., Kim, J.I. et al. Endoscopic clip closure versus surgery for the treatment of iatrogenic colon perforations developed during diagnostic colonoscopy: a review of 115,285 patients. Surg Endosc 27, 501–504 (2013). https://doi.org/10.1007/s00464-012-2465-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2465-3